Daniel Scheidegger (Author) More practice - better results: applicable even in visceral surgery Fulltext PDF Fulltext HTML
Angelos G. Kolias, Ellie Edlmann, Peter J. Hutchinson (Author) The role of pharmacotherapy in the management of chronic subdural haematoma Fulltext PDF Fulltext HTML
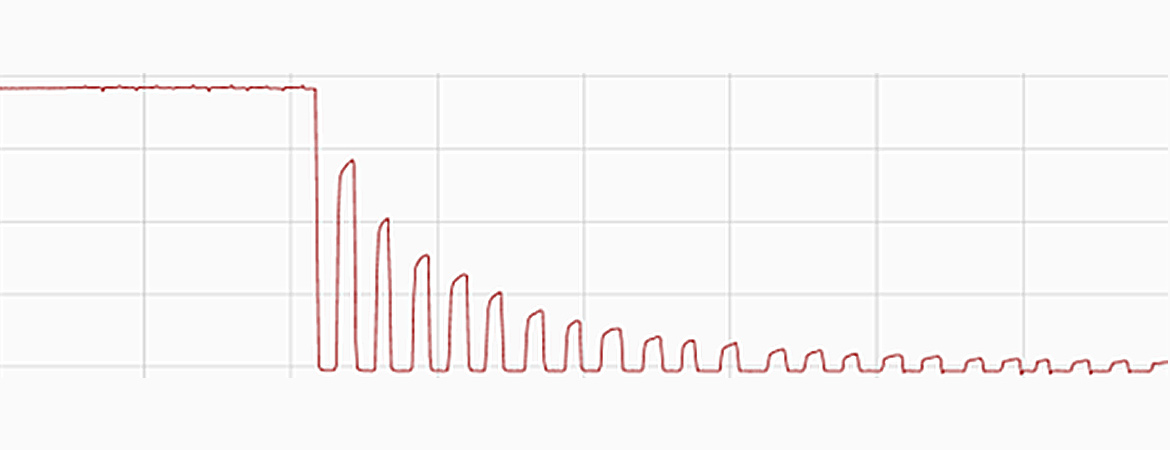
Hyunseok Jee, Jong-Hee Kim (Author) A mini-overview of single muscle fibre mechanics: the effects of age, inactivity and exercise in animals and humans Fulltext PDF Fulltext HTML
Jakob Usemann, Sophie Yammine, Florian Singer, Philipp Latzin (Author) Inert gas washout: background and application in various lung diseases Fulltext PDF Fulltext HTML
Joanna Gawinecka, Felix Schönrath, Arnold von Eckardstein (Author) Acute aortic dissection: pathogenesis, risk factors and diagnosis Fulltext PDF Fulltext HTML
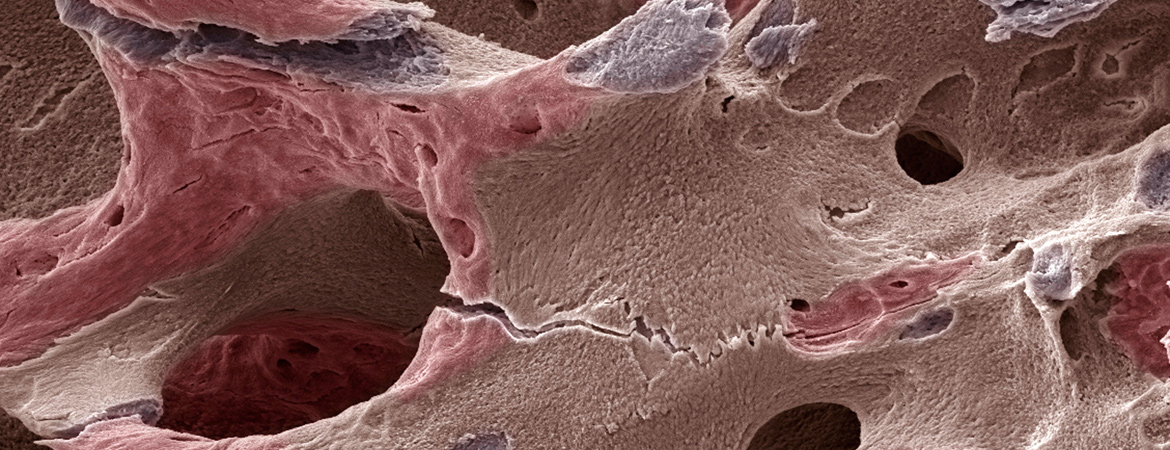
Christian Meier, Brigitte Uebelhart, Bérengère Aubry-Rozier, Martin Birkhäuser, Heike A. Bischoff-Ferrari, Diana Frey, Reto W. Kressig, Olivier Lamy, Kurt Lippuner, Petra Stute, Norbert Suhm, Serge Ferrari (Author) Osteoporosis drug treatment: duration and management after discontinuation. A position statement from the Swiss Association against Osteoporosis (SVGO/ASCO) Fulltext PDF Fulltext HTML
Felix Burkhalter, Uyen Huynh-Do, Karine Hadaya, Marice Matter, Thomas F. Mueller, Isabelle Binet, Christa Nolte, Juerg Steiger (Author) Early complications after living donor nephrectomy: analysis of the Swiss Organ Living Donor Health Registry Fulltext PDF Fulltext HTML Appendix
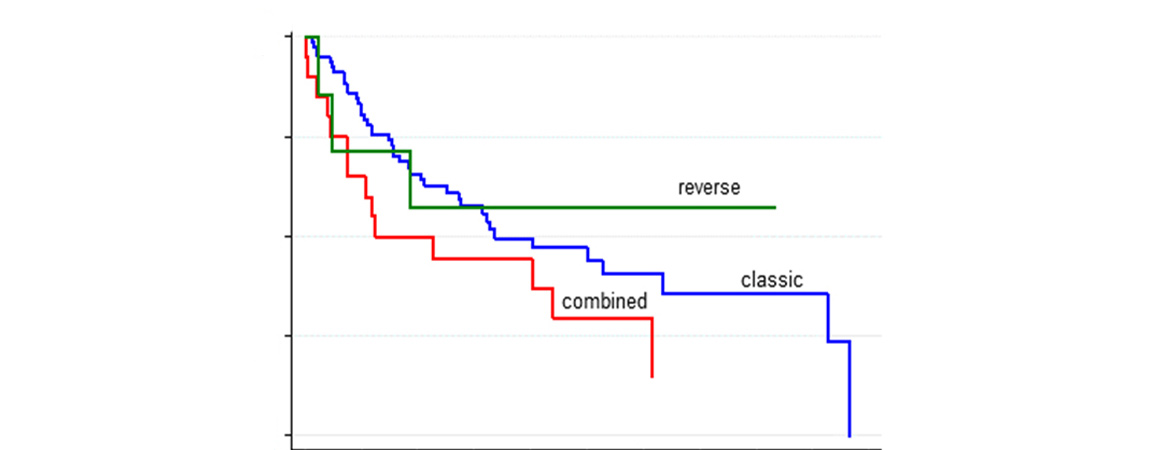
Maria J. Schaumeier, Alexandra Nagy, Salome Dell-Kuster, Rachel Rosenthal, Stefan Schaub, Michael Dickenmann, Lorenz Gurke, Thomas Wolff (Author) Right retroperitoneoscopic living donor nephrectomy does not increase surgical complications in the recipient and leads to excellent long-term outcome Fulltext PDF Fulltext HTML
Daniel Reding, Bernhard C. Pestalozzi, Stefan Breitenstein, Roger Stupp, Pierre-Alain Clavien, Ksenija Slankamenac, Panagiotis Samaras (Author) Treatment strategies and outcome of surgery for synchronous colorectal liver metastases Fulltext PDF Fulltext HTML
Beatrice Mosimann, Chantal Pfiffner, Sofia Amylidi-Mohr, Lorenz Risch, Daniel Surbek, Luigi Raio (Author) First trimester combined screening for preeclampsia and small for gestational age – a single centre experience and validation of the FMF screening algorithm Fulltext PDF Fulltext HTML
Swiss Society of Rheumatology (Author) Supplementum 224: Annual Meeting of the Swiss Society of Rheumatology (SGR) (Interlaken, Switzerland, September 7-8, 2017) Fulltext PDF