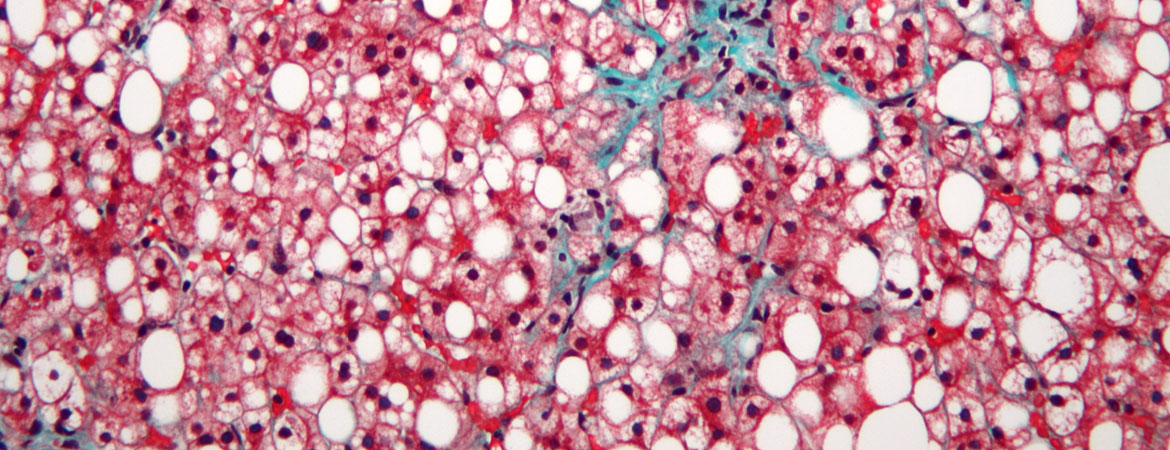
Stephan Baumeler, Wolfram Jochum, Jörg Neuweiler, Irina Bergamin, David Semela (Author) Controlled attenuation parameter for the assessment of liver steatosis in comparison with liver histology: a single-centre real life experience Fulltext PDF Fulltext HTML
Véronique Andrey, Pierre-Alex Crisinel, Guy Prod’hom, Antony Croxatto, Jean-Marc Joseph (Author) Impact of co-amoxicillin-resistant Escherichia coli and Pseudomonas aeruginosa on the rate of infectious complications in paediatric complicated appendicitis Fulltext PDF Fulltext HTML
Rahul Gupta, Daniele R. Nolan, Donald A. Bux, Andres R. Schneeberger (Author) Is it the moon? Effects of the lunar cycle on psychiatric admissions, discharges and length of stay Fulltext PDF Fulltext HTML
Julia Notter, Andrea Bregenzer, Pietro Vernazza, Christian R. Kahlert (Author) Nevirapine in HIV maintenance therapy – can “old drugs” survive in current HIV management? Fulltext PDF Fulltext HTML
Boris Cheval, Stéphane Cullati, Denis Mongin, Ralph E. Schmidt, Kim Lauper, Jesper Pihl-Thingvad, Pierre Chopard, Delphine S. Courvoisier (Author) Associations of regrets and coping strategies with job satisfaction and turnover intention: international prospective cohort study of novice healthcare professionals Fulltext PDF Fulltext HTML