Antoine Flahault, Antoine Geissbuhler, Idris Guessous, Philippe J Guérin, Isabelle Bolon, Marcel Salathé, Gérard Escher (Author) Precision global health in the digital age Fulltext PDF Fulltext HTML
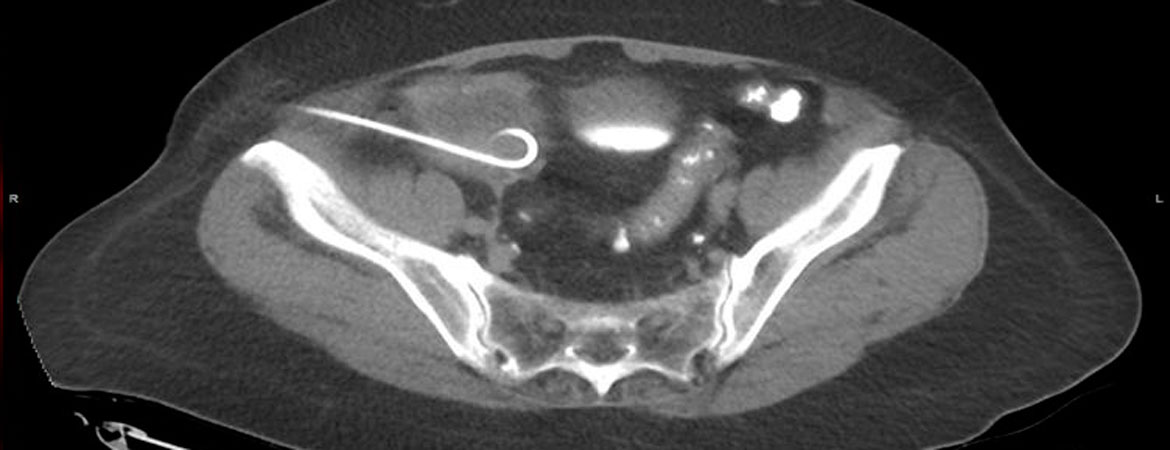
Almir Miftaroski, Ulf Kessler, Etienne Monnard, Bernhard Egger (Author) Two-step procedure for complicated appendicitis with perityphlitic abscess formation Fulltext PDF Fulltext HTML
Corina Metaxas, Deborah Mathis, Cyrill Jeger, Kurt E. Hersberger, Isabelle Arnet, Philipp Walter (Author) Early biomarker response and patient preferences to oral and intramuscular vitamin B12 substitution in primary care: a randomised parallel-group trial Fulltext PDF Fulltext HTML
Carl Chrobak, Jan A. Sidler, Alix O'Meara, Sabine Schädelin, Balthasar L. Hug (Author) Iron homeostasis in inflammation: a single centre prospective observational study in medical inpatients Fulltext PDF Fulltext HTML