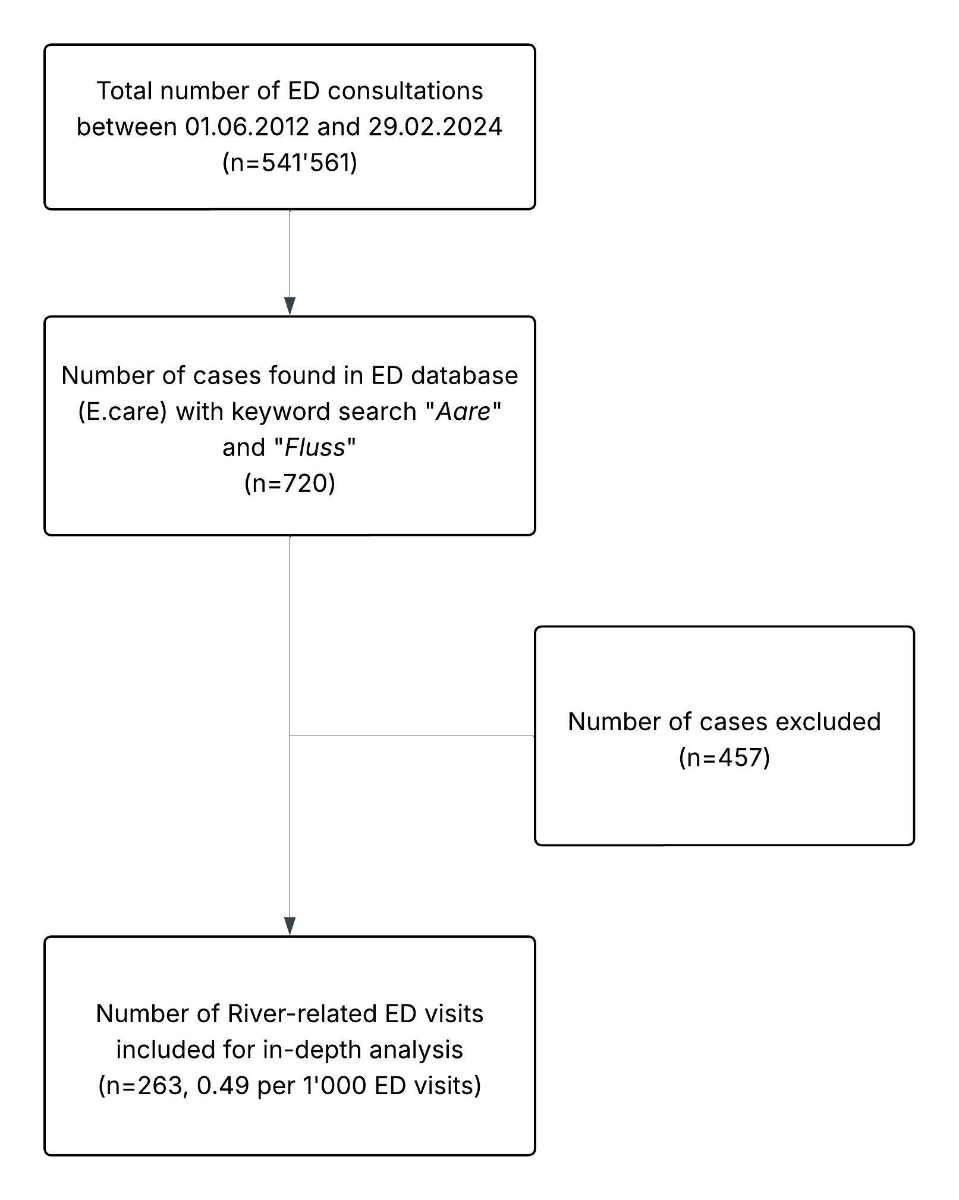
Figure 1Study flowchart. Abbreviations: ED: Emergency Department.
DOI: https://doi.org/https://doi.org/10.57187/4839
Urban swimming is a long-standing cultural tradition in Switzerland, with the Aare River in Bern serving as one of its most iconic locations [1]. Recognised by the Federal Office of Culture as part of Switzerland’s intangible cultural heritage, swimming in the Aare attracts large numbers of participants each year [2]. On hot summer days, up to 30,000 individuals can be seen walking along the river each day, preparing to swim downstream with the current [3]. The river offers a range of activities, including swimming, boating, surfing and bridge jumping, and is a favoured location for sunbathing and relaxation, drawing both locals and tourists.
However, swimming in an unsupervised natural river presents significant hazards. In the section of the Aare River flowing through the city of Bern, the flow velocity typically ranges between 6 and 19 km/h, depending on seasonal variations and discharge levels. Entry into the Aare is advised only for strong swimmers, and participation is at one’s own risk [4].
The river’s unpredictable currents and varying flow conditions pose dangers, especially to those with limited experience. In response to these risks, the City of Bern and the Swiss Lifesaving Society (SLRG; Schweizerische Lebensrettungs-Gesellschaft) have initiated multiple public awareness campaigns (e.g. “Aare you safe?”) aimed at improving safety [5].
Over the past decade, about 50 drowning deaths have been documented annually across Switzerland, with a significant portion attributed to river and lake incidents: in 2023 for instance, 59 individuals lost their lives due to drowning, 71% of whom were adult males. Most of these fatalities occurred in natural bodies of water, including lakes (46%) and rivers (41%) [6].
While fatal drownings remain a tragic and high-profile concern, non-fatal swimming- and bathing-related injuries are also prevalent. According to recent data from SUVA, Switzerland’s largest accident insurer, an average of 5593 swimming- and bathing-related accidents were reported annually between 2017 and 2021, resulting in an average insurance cost of 34.6 million Swiss francs per year [7]. An extrapolated estimate from the Swiss Advisory Centre for Accident Prevention (BFU) suggests that the actual number of incidents may be significantly higher, with an average of 12,160 swimming-related accidents reported annually between 2016 and 2020 [8].
The goal of the present study was to analyse river-related emergency department (ED) visits over more than eleven years, with an emphasis on epidemiological patterns, injury mechanisms, triage severity and clinical outcomes, at Switzerland’s largest trauma centre, which records over 50,000 ED visits per year [9]. Particular attention was given to three subgroups relevant for prevention efforts: (1) sex differences, which may reflect varying risk-taking behaviours; (2) non-Swiss nationals, who may be unfamiliar with local river conditions; and (3) younger and older individuals, who may face distinct risk profiles due to activity preferences or physical limitations. By examining these subgroups, the study aims to support targeted prevention strategies and strengthen interdisciplinary approaches to improving river-related safety.
This study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines [10]. According to the local ethics committee (Req-2023-00537), the study was exempt from the Human Research Act and did not require general informed consent. A study plan was submitted to the local ethics committee as part of the mandatory ethics committee responsibility declaration.
This retrospective cross-sectional study utilised ED data collected over a period of eleven years and nine months. To identify and analyse river-related ED visits, all ED data from patients who consulted the study site during the study period (1 June 2012 to 29 February 2024) were examined.
The adult ED at Bern University Hospital, a tertiary care centre, operates as a self-contained, interdisciplinary unit, staffed by approximately 45 emergency physicians (primarily from internal medicine or anaesthesia) and 120 nurses, managing over 50,000 patient visits (age ≥16 years) annually [11]. Major trauma cases are managed in a dedicated shock room under the supervision of an emergency physician, in collaboration with trauma and anaesthesia teams following institutional trauma protocols. Specialty consultations are requested as needed. Children (<16 years) are treated in a paediatric ED nearby.
All ED records are digitally stored in the patient management system (E.care; Mesalvo Turnhout BV, Turnhout, Belgium). A full-text search for the keywords “Aare” and “Fluss” (German for “river”) in the patient’s history was conducted to identify relevant cases. The identified records were manually reviewed using the following exclusion criteria:(1) Situations in which “Aare” or “Fluss” were mentioned in the patient’s history but had no direct connection to the ED visit (e.g. a person who had a heart attack while strolling by the river);(2) Patients aged under 16, who were not included as they received care in the paediatric ED.
All medical records of patients who visited the ED during the study period were screened based on the inclusion criterion that the keyword “Aare” or “Fluss” appeared in the patient’s history at the time of admission. The keywords were used to ensure comprehensive identification of river-related incidents. The term “Fluss” was included to capture all cases referring to any river exposure, while “Aare” was added because the Aare is the most frequently visited river in the Bern region, and is therefore expected to account for most river-related injuries.
A manual review of the data was conducted to evaluate the eligibility criteria.
The data were retrieved from the patient management system through both automated extraction and manual review of medical records. Both steps were performed by one author (T.M.). To ensure data accuracy, 50% of the dataset was independently rechecked by J.H., yielding a concordance rate of 99.7%.
The study made use of factors that were regularly gathered and evaluated at the time of ED admission; these variables were then incorporated directly into a structured dataset for analysis. No separate study database was created. The dataset was reviewed for plausibility and internal consistency by a statistics expert (M.M.) during data analysis. Among the factors were demographics (patient’s age, sex and nationality); consultation information (year, month and weekday of admission); triage classification based on the Swiss Emergency Triage Scale (from non-urgent, 5, to life-threatening, 1).
Additionally, the study authors used free-text analysis of medical records to extract new factors:
All available cases that met the inclusion criteria were included. The study period corresponds to the timeframe during which the patient management software E.care was in use in our emergency department. The system was introduced on 1 June 2012 and remained in use until 29 February 2024.
Stata® 18.1 (StataCorp, College Station, Texas, USA) was used for statistical analysis. While continuous variables, including patient age, were expressed as median with interquartile range (IQR; 25th to 75th percentile), categorical variables were summarised as absolute numbers and percentages. For proportional incidences, 95% confidence intervals (CIs) were calculated. To analyse the number of river-related ED visits over the study period, a two-way fractional polynomial prediction plot with a 95% confidence interval was generated.
Three subgroup analyses were performed comparing i) male vs female, ii) Swiss vs non-Swiss nationality, and iii) younger vs older (≤35 years vs >35 years) ED visits. Age was dichotomised at 35 years, in keeping with established drowning and injury epidemiology strata that distinguish young adults from older adult groups beginning at 35 years [12, 13]. For each subgroup, differences in patient demographics, accident characteristics, consultation characteristics, injury characteristics and discharge outcomes were assessed.
The chi-squared test was used to evaluate group differences for categorical variables, and the Wilcoxon rank-sum test for continuous variables. As this study was primarily exploratory and descriptive, no predefined hypotheses were tested. Instead, a broad range of group comparisons was performed to identify potential patterns and associations. Given the large number of statistical tests conducted, p-values were interpreted descriptively rather than as confirmatory evidence. To adjust for multiple testing, we used a cut-off of p <0.005 as proposed by Ioannidis [14]. All findings should therefore be considered hypothesis-generating and require confirmation in future studies.
The study was conducted in accordance with Swiss law and submitted to the local ethics committee (Req-2023-00537). The committee determined that the study does not fall within the scope of the Human Research Act (Art. 2, Para. 1) and therefore does not require approval. As a retrospective data analysis, no informed consent was necessary.
Over the longer than 11-year study period, a keyword search for “Aare” and “Fluss” in the Emergency Department (ED) database identified 720 patient records. After applying predefined exclusion criteria, 456 cases (63%) were excluded due to the absence of a clear connection between the patient’s interaction with the river and their ED admission. One additional case was excluded because the patient was under 16 years of age (figure 1). This resulted in 263 patient records (36.5%) being included in the final analysis, corresponding to 0.49 (95% CI: 0.43–0.55) river-related ED visits per 1000 ED consultations. Among the 263 cases included in the analysis, the vast majority of incidents (n = 250, 95.1%) occurred in the Aare. Only 13 cases (4.9%) were associated with other rivers. The median age of patients was 31 years (IQR: 24–45), with 34.6% aged over 35 years. Males accounted for 62.7% of cases and females for 37.3%. Swiss nationals comprised 65.4% of the sample, while foreign nationals accounted for 34.6%. The majority of patients (89%) were categorised as at least urgent upon presentation to the ED. Baseline characteristics are shown in table 1.
Figure 1Study flowchart. Abbreviations: ED: Emergency Department.
Table 1Baseline characteristics of the 263 included river-related Emergency Department visits.
| Characteristics | n | % | |
| Age group | 16–25y | 77 | 29.3% |
| >25–35y | 95 | 36.1% | |
| >35–50y | 41 | 15.6% | |
| >50–65y | 32 | 12.2% | |
| >65y | 18 | 6.8% | |
| Sex | Female | 98 | 37.3% |
| Male | 165 | 62.7% | |
| Nationality | Foreign | 91 | 34.6% |
| Swiss | 172 | 65.4% | |
| Accident: month | January | 4 | 1.5% |
| February | 3 | 1.1% | |
| March | 2 | 0.8% | |
| April | 6 | 2.3% | |
| May | 6 | 2.3% | |
| June | 42 | 16% | |
| July | 81 | 30.8% | |
| August | 84 | 31.9% | |
| September | 19 | 7.2% | |
| October | 6 | 2.3% | |
| November | 7 | 2.7% | |
| December | 3 | 1.1% | |
| Accident: day of week | Monday | 31 | 11.8% |
| Tuesday | 33 | 12.5% | |
| Wednesday | 29 | 11.0% | |
| Thursday | 42 | 16.0% | |
| Friday | 30 | 11.4% | |
| Saturday | 51 | 19.4% | |
| Sunday | 47 | 17.9% | |
| Triage | Life-threatening | 33 | 12.5% |
| High-urgent | 63 | 24% | |
| Urgent | 138 | 52.5% | |
| Semi-urgent | 25 | 9.5% | |
| Non-urgent | 4 | 1.5% | |
| Discharge | Home | 197 | 74.9% |
| Medical ward | 7 | 2.7% | |
| Surgical ward | 6 | 2.3% | |
| Operation | 4 | 1.5% | |
| ICU | 17 | 6.5% | |
| Psychiatric clinic | 21 | 8.0% | |
| ED death | 7 | 2.7% | |
| Other | 4 | 1.5% | |
Abbreviations: ED: Emergency Department; ICU: Intensive Care Unit.
The annual frequency of river-related ED visits ranged from a minimum of 9 cases in 2014 to a peak of 40 cases in 2018, with an average of 22.4 cases per year. Figure 2 illustrates the yearly trend in river-related ED visits. The trend shows a stable number of cases over the longer than 11-year study period.
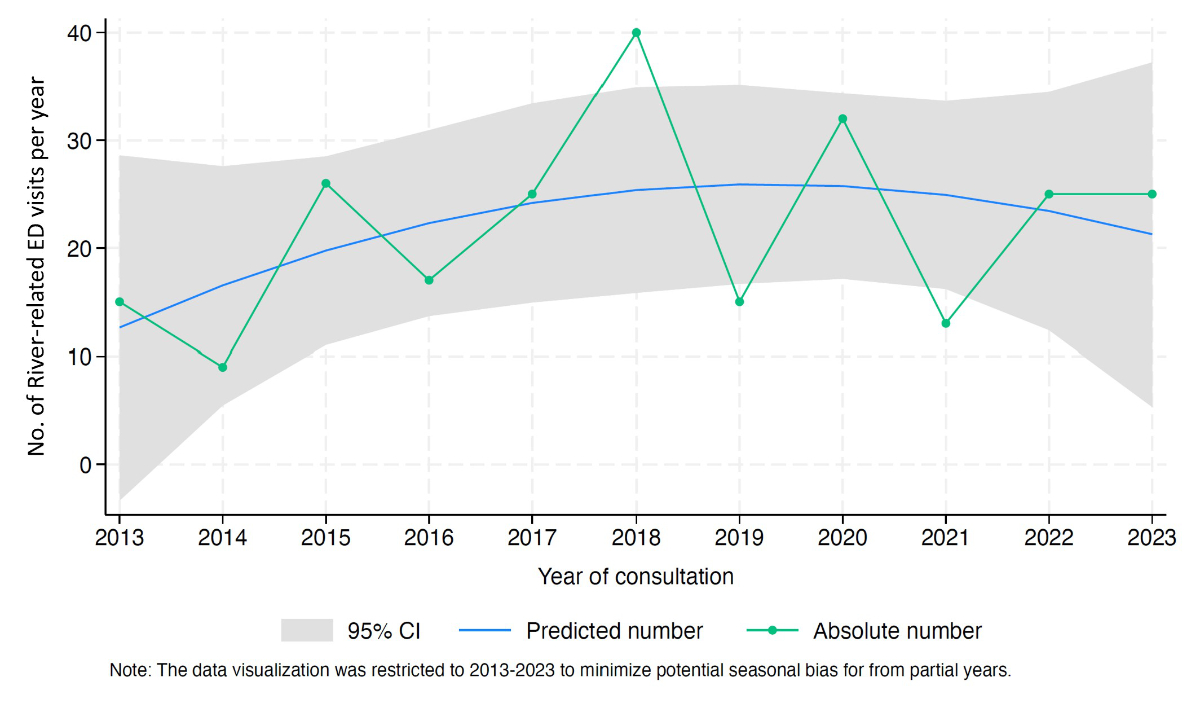
Figure 2Number of river-related ED visits per year over the study period. Note: The green line represents the absolute number of river-related ED visits per year. The blue line represents the predicted trend, with the grey area indicating the 95% confidence interval, based on a fractional polynomial model. Abbreviations: CI: confidence interval; ED: Emergency Department.
Most river-related ED visits occurred during the summer months, with 78.7% of cases recorded in June, July or August. Over one-third of patients (n = 98, 37.3%) presented to the ED on a weekend. Among weekdays, Thursday had the highest number of incidents (n = 42, 16%).
Figure 3 presents the distribution of activities associated with river-related ED visits. In more than half of the cases, the incident was triggered by swimming (n = 135, 51.3%). Other popular leisure activities included jumping from a bridge (n = 48, 18.3%) and boating on the river (n = 22, 8.4%). The third most common cause overall was entering a river in the context of a suicide attempt (n = 25, 9.5%).
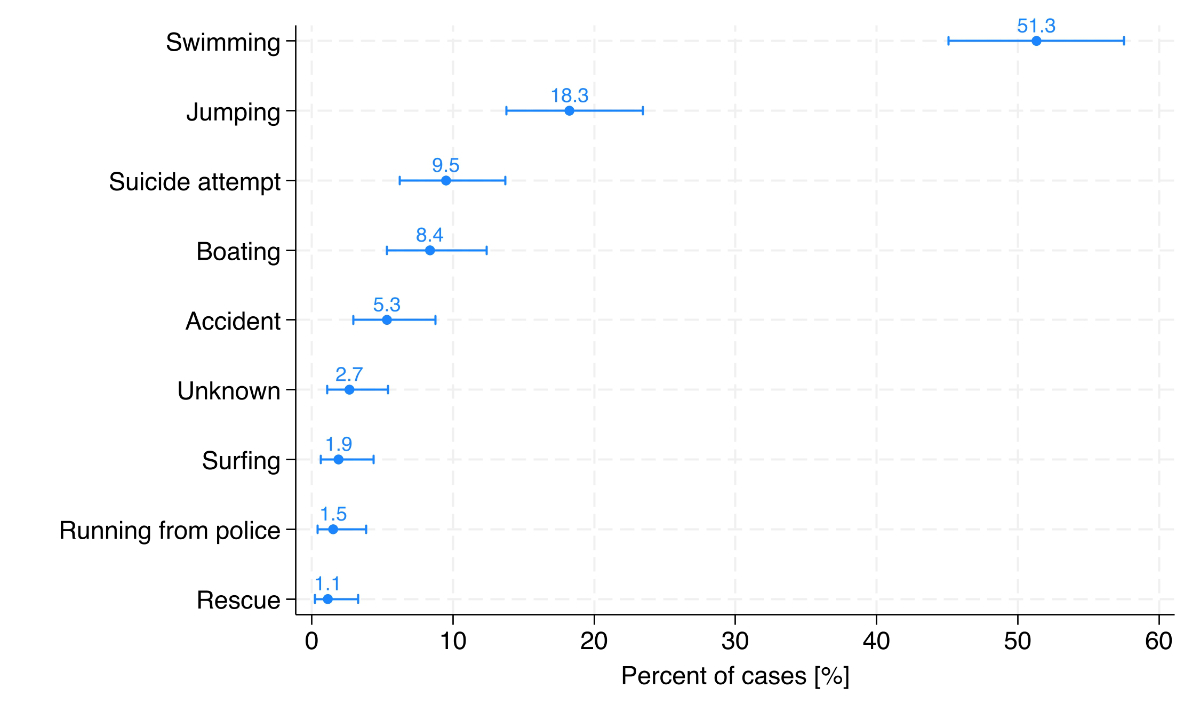
Figure 3Activities related to the 263 river-related Emergency Department visits, shown as percentages with 95% confidence intervals and ordered by frequency. Abbreviations: ED: Emergency Department.
In total, 63.1% of river-related visits were classified as trauma cases based on the main diagnosis, with nearly one-third of these involving injuries to the lower extremities (figure 4).
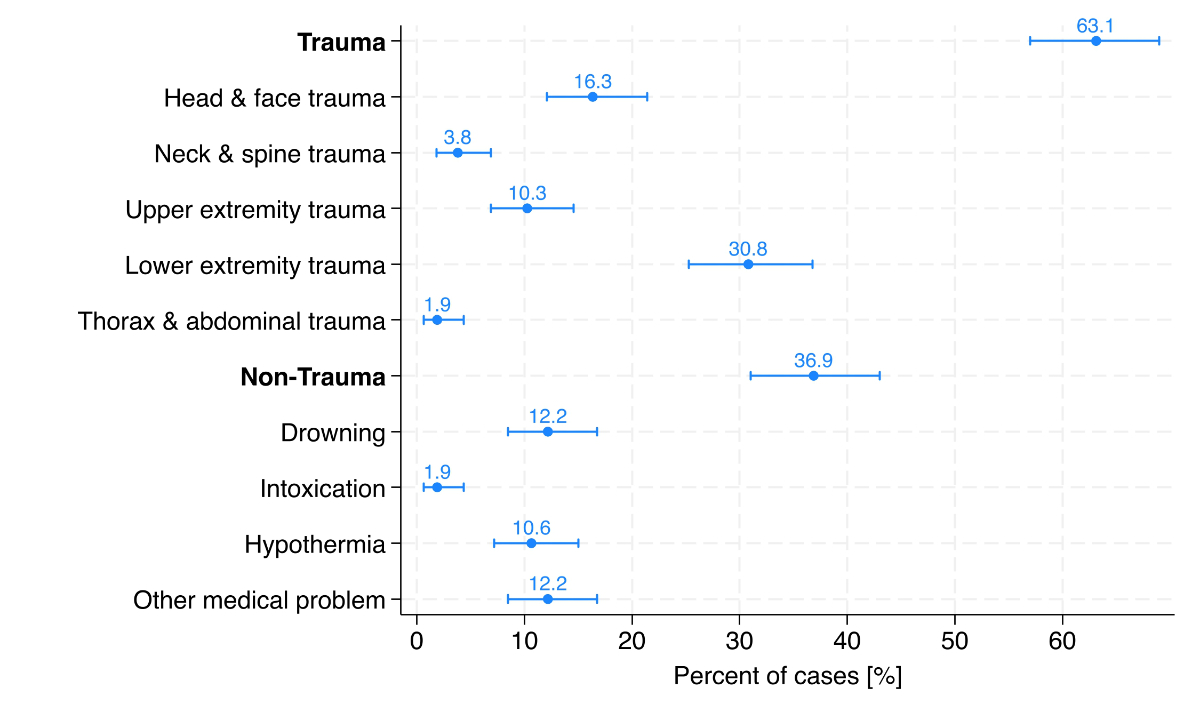
Figure 4Main diagnosis group related to the 263 river-related Emergency Department visits, shown as percentages with 95% confidence intervals. Abbreviations: CI: confidence interval; ED: Emergency Department.
All ED diagnoses (main and secondary diagnoses) are summarised in table 2. The most common diagnosis was lower extremity trauma, accounting for 30.8% of cases. Among these, contusions of the ankle and foot (8.7%) and open wounds of the ankle and foot (9.1%) were the most frequently observed injuries. Head and face trauma was the second most frequent category, accounting for 16.3% of cases. Within this group, open wounds of the head (8.0%), traumatic rupture of the ear drum (4.2%) and ear barotrauma (3.4%) were the most frequently reported injuries. Upper extremity trauma was diagnosed in 10.3% of cases, with dislocation of the shoulder (3.4%) being the most prevalent injury in this category. Drowning incidents made up 12.2% of cases, with 9.9 % classified as nonfatal and 1.9% as fatal. Hypothermia was documented in 10.6% of cases.
Table 2Main and secondary detailed diagnoses of river-related Emergency Department visits: (A) Trauma diagnosis, (B) Non-trauma diagnosis; n = 263 patients (100%).
| Diagnoses of river-related ED visits | n* | %** | |
| Trauma diagnosis | |||
| Head and face trauma | Open wound of head | 21 | 8.0% |
| Fracture of skull | 4 | 1.5% | |
| Sprain of jaw | 1 | 0.5% | |
| Concussion | 8 | 3.2% | |
| Traumatic rupture of ear drum | 11 | 4.3% | |
| Ear barotrauma | 9 | 2.7% | |
| Dissection of vertebral artery | 2 | 0.8% | |
| Neck and spine trauma | Fracture of neck | 3 | 1.1% |
| Sprain of neck | 1 | 0.4% | |
| Fracture of thoracic spine | 4 | 1.5% | |
| Upper back pain | 1 | 0.4% | |
| Fracture of lumbar spine | 4 | 1.5% | |
| Lower back pain | 2 | 0.8% | |
| Upper extremity trauma | Fracture of humerus | 1 | 0.4% |
| Dislocation of shoulder | 9 | 3.4% | |
| Contusion of elbow and forearm | 3 | 1.1% | |
| Open wound of forearm | 7 | 2.7% | |
| Contusion of wrist and hand | 6 | 2.3% | |
| Open wound of wrist and hand | 7 | 2.7% | |
| Fracture of wrist and hand | 1 | 0.4% | |
| Thorax and abdominal trauma | Contusion of thorax | 9 | 3.4% |
| Lung injury | 5 | 1.9% | |
| Open wound of abdomen | 1 | 0.4% | |
| Drowning | Nonfatal drowning | 26 | 9.9% |
| Fatal drowning | 5 | 1.9% | |
| Drowning following fall | 2 | 0.8% | |
| Lower extremity trauma | Contusion of hip and thigh | 4 | 1.5% |
| Open wound of hip and thigh | 2 | 0.8% | |
| Injury of muscle or tendon of hip | 1 | 0.4% | |
| Contusion of knee and lower leg | 7 | 2.7% | |
| Open wound of knee and lower leg | 11 | 4.2% | |
| Injury of knee joint | 4 | 1.5% | |
| Ankle fracture | 3 | 1.1% | |
| Contusion of ankle and foot | 23 | 8.7% | |
| Open wound of ankle and foot | 24 | 9.1% | |
| Foot fracture | 7 | 2.7% | |
| Injury of ankle | 3 | 1.1% | |
| Puncture wound | 7 | 2.7% | |
| Non-trauma diagnosis | |||
| Intoxication | Behavioural disorder, alcohol | 8 | 3.0% |
| Behavioural disorder, multiple drugs | 6 | 2.3% | |
| Alcohol intoxication | 17 | 6.4% | |
| Amphetamine intoxication | 3 | 1.1% | |
| Hypothermia | 28 | 10.6% | |
| Other medical problem | Acute stress reaction | 3 | 1.1% |
| Arthritis | 1 | 0.4% | |
| Cardiac arrest | 13 | 4.9% | |
| Cerumen impaction | 5 | 1.9% | |
| Dissociative disorder | 2 | 0.8% | |
| Erysipelas | 1 | 0.4% | |
| Foreign body in oesophagus | 1 | 0.4% | |
| Foreign body in eye | 1 | 0.4% | |
| Intentional self-harm by jump | 3 | 1.1% | |
| Otitis externa | 8 | 3.0% | |
| Pulmonary oedema | 1 | 0.4% | |
| Syncope | 1 | 0.4% | |
| Urticaria | 4 | 1.5% | |
* n includes all 355 diagnoses of 263 patients (63 patients had two diagnoses, 7 patients had three and 5 patients had four).
** The total number of patients (n = 263) is used as the denominator.
Among non-trauma diagnoses, intoxication was reported in 1.9% of cases, including behavioural disorders related to alcohol (3%) and multiple drug use (2.3%). “Other” medical problems accounted for 12.2% of cases, with cardiac arrest (4.9%) and otitis externa (3%) being the most common within this category.
Most patients (74.9%) were discharged home (n = 197). Hospital admissions were relatively uncommon, with 7 patients (2.7%) admitted to a medical ward and 6 patients (2.3%) to a surgical ward. Additionally, 4 patients (1.5%) underwent an immediate operation.
A notable proportion of patients required intensive care or psychiatric treatment, with 17 patients (6.5%) admitted to the ICU and another 21 patients (8%) transferred to a psychiatric clinic. A total of 7 patients (2.7%) succumbed to their injuries and were classified as ED death. Four patients (1.5%) were discharged to other destinations.
The time-trend analysis demonstrated a stable pattern in both absolute and relative values across all subgroups over the study period. Individuals aged ≤35 years, males as well as Swiss nationals consistently showed higher incidence rates. During the COVID-19 year with mitigation measures in place (2020), the number of cases involving foreign nationals was low, whereas the number of river-related presentations among Swiss nationals reached its peak (figure S1 in the appendix).
Accident characteristics showed statistically significant differences between males and females (p <0.001), with suicide attempts (20.4% vs 3%) and boating-related incidents (11.2% vs 6.7%) more common in females and jumping-related incidents more frequent in males (22.4% vs 11.2%). In contrast, no significant differences were observed between sexes in demographic, consultation, injury or procedure characteristics (table S1 in the appendix).
Compared to younger patients (≤35 years), those aged >35 years were significantly more likely to present with hypothermia (19.8% vs 5.8%; p <0.001), be triaged as life-threatening (22% vs 7.6%; p <0.001), report intentions other than swimming (notably more suicide attempts and accidents; p <0.001), and have higher rates of ICU admission and psychiatric or surgical interventions at discharge (p <0.001) (table S2 in the appendix).
Hypothermia was significantly more common among non-Swiss nationals (18.7%) compared to Swiss nationals (6.4%) (p = 0.002) with no other significant differences found (table S3 in the appendix).
This cross-sectional study analysed 263 ED visits related to recreational use of rivers over a period of 11 years and 9 months. While all river-related ED visits were included, 95.1% involved the Aare, underscoring its central role as the region’s most accessible and commonly used river. For this reason, the discussion predominantly addresses Aare-related incidents, as the small number of cases from other rivers precludes meaningful comparisons.
Young adults, particularly males, were the most affected group, with swimming, bridge jumping and boating identified as the leading causes. Most incidents occurred during summer weekends, and trauma was the predominant clinical category. We will now discuss these findings in relation to existing literature, with a focus on risk profiles, injury mechanisms, mental health and clinical outcomes.
The predominance of male patients in this cohort (62.7%) is consistent with existing literature, which reports higher rates of water-related injuries and drowning among males across all age groups [15–17]. Several factors may contribute to this overrepresentation, including greater exposure to open-water environments, higher participation in risk-prone activities such as bridge jumping and a general propensity for risk-taking behaviour in males. Such behavioural tendencies may explain both incidence and injury severity. The sex disparity observed in the present data thus mirrors international findings but also underscores the importance of targeted prevention strategies addressing risk perception and behaviour, particularly among young men engaging in recreational river activities. Notably, most cases occurred during summer months and on weekends, with an additional peak on Thursdays, likely reflecting increased river exposure during leisure time, after-work activities and pre-weekend social gatherings.
Previous studies reported a general decline in leisure and traffic accidents during the COVID-19 pandemic, accompanied by a rise in domestic injuries and mental health emergencies [18, 19]. In contrast, the number of river-related ED visits among Swiss nationals increased in 2020 in this cohort, possibly reflecting intensified use of local recreational spaces due to restricted travel and limited leisure alternatives.
More than half of the injury events in our cohort were triggered by swimming (51.3%), followed by bridge jumping (18.3%) and boating (8.4%). These findings likely reflect the specific recreational culture surrounding rivers such as the Aare, where swimming long distances downstream is a long-standing seasonal practice, particularly in the city of Bern [1, 2]. The high accessibility of the river, combined with minimal barriers to entry and limited formal supervision, may increase exposure and the likelihood of adverse events during swimming.
Bridge jumping, although less frequent (18.3%), represents a high-risk activity, primarily among males in this cohort. Previous studies have documented severe trauma, spinal injuries and drowning following jumps from medium-height bridges [20, 21]. Fatal outcomes often result from drowning rather than impact trauma, illustrating the interaction of kinetic trauma and immersion risk.
Notably, 9.5% of incidents in our cohort were classified as suicide attempts. These were significantly more common in women, contrasting with the overall male predominance in injury events. This aligns with previous research from coastal regions in Australia and urban rivers in Shanghai, where drowning and jumping into water were common suicide methods, especially among female patients, often associated with psychiatric illness, prior suicidal behaviour and seasonal patterns [22, 23]. These observations highlight the need for integrated prevention strategies that include mental health support and surveillance.
Trauma represents the predominant risk associated with urban swimming. In the present dataset, 63.1% of river-related incidents (166 of 263 cases) were traumatic in nature, highlighting the hazardous conditions of natural urban waterways. Fast-moving currents, submerged obstacles and uneven riverbeds contribute significantly to injury risk.
Lower extremity trauma, particularly ankle contusions and lacerations, was frequent and often caused by unstable or rocky riverbeds. Head and facial trauma was also common, comprising 16.3% of cases. Injuries included lacerations, concussions and tympanic membrane ruptures, primarily in younger individuals following high-velocity bridge jumps. Bridge jumping also contributed to shoulder dislocations, spinal and internal injuries.
Collisions with submerged structures were a frequent mechanism, especially following unintended or misjudged entries. Puncture wounds and lacerations were frequently linked to debris, such as fishing hooks, nails or glass fragments. These accounted for a substantial proportion of non-blunt injuries. The observed injury pattern contrasts with data from the US National Electronic Injury Surveillance System (NEISS), where head and neck trauma was most frequent (37%) and lower extremity injuries ranked second (33%) [16]. The reversed pattern in our cohort may reflect river-specific mechanisms, such as impacts with submerged rocks or unstable riverbeds.
Drowning was documented in 12.2% of cases, including both fatal and non-fatal outcomes, while hypothermia occurred in 10.6% of patients. These findings reflect the inherent risks of swimming in dynamic, cold-water environments such as the Aare, where strong currents, fluctuating temperatures and physical exhaustion may contribute to rapid deterioration. Hypothermia and severe outcomes were more frequently observed in older individuals (>35 years) and non-Swiss nationals, underlining the physiological vulnerability of these groups. Although medical comorbidities were not assessed in this dataset, previous studies have identified them as important modifiers of drowning risk. A Canadian study showed that seizure disorders and ischaemic heart disease significantly increase the likelihood of fatal drowning [24]. Global data further point to alcohol use and occupational exposure as key contributors to drowning-related burden, particularly among men [25]. Taken together, these findings underscore the complex interplay of environmental stressors and individual vulnerability, and highlight the need for prevention strategies that go beyond behavioural education to also address physiological and situational risk factors.
In the present cohort, 74.9% of patients were discharged home, whereas 6.5% required intensive care and another 8% psychiatric treatment. The discharge rate is lower than in the NEISS dataset [16], in which 94.5% of patients were treated and released from the ED, indicating a higher clinical complexity of river-related injuries. This difference may be explained by the setting: while NEISS injuries occurred predominantly in or around swimming pools (87%), this study focused exclusively on an urban river environment, characterised by uncontrolled currents, variable depths and limited supervision. Among older patients (>35 years), triage as life-threatening and the need for ICU care or psychiatric/surgical interventions were significantly more common, indicating both clinical severity and resource intensity in this subgroup.
The findings point to several relevant implications for prevention and health system preparedness. Risk communication should particularly address young males and non-Swiss nationals, who represented key risk groups. Multilingual information campaigns, visible signage at river access points and seasonal lifeguard presence might help reduce acute incidents.
The notable share of suicide attempts, particularly among female patients, highlights the role of rivers as a site of psychiatric crisis. Mental health considerations should therefore be integrated into water safety strategies, including early detection, outreach and coordination with crisis services.
Lower extremity trauma was common, often resulting from contact with uneven riverbeds, rocks or debris. Preventive measures could include improved riverbed maintenance and awareness regarding protective footwear or safe entry techniques.
Hypothermia occurred in a substantial proportion of cases, even during warmer months. This underlines the need for public education on cold-water risks and the importance of timely rescue. Older adults and non-Swiss nationals were disproportionately affected and may benefit from targeted communication strategies.
To support effective interventions, continued surveillance of river-related injuries and coordination between healthcare providers, local authorities and community organisations are essential.
When evaluating the results, it is important to consider the limitations of this study.
Selection bias is a significant drawback given that only patients who visited the University ED were included in this single-centre study. Even though this hospital has the largest ED in the Canton of Bern, it mostly handles moderate-to-severe cases, so minor injuries treated by general practitioners, walk-in clinics or smaller EDs were not taken into account and hence are likely to be underrepresented. This likely resulted in an overestimation of the severity of injuries and an underestimation of the actual number of river-related occurrences.
Furthermore, the relatively small number of cases (n = 263) limits the generalisability of these findings. However, this number reflects the true burden of river-related emergencies at Switzerland’s largest tertiary trauma centre.
The absence of visiting data, which makes it impossible to calculate incidence rates accurately, is another drawback. It is impossible to calculate the actual risk of harm in relation to exposure without knowing the entire number of people who swam in rivers like the Aare throughout the study period. Furthermore, it is challenging to evaluate risk variables and make inferences regarding relative risk and possible protective treatments due to the lack of a control group of swimmers who are not harmed.
Additionally, this study only included patients who were admitted to the ED; hence, the dataset did not include individuals who were found dead at the scene and not transported to the hospital. This ‘forgotten cohort’ represents an important patient group that is often overlooked, as they are frequently excluded from analysed datasets [26]. Furthermore, the vulnerable subgroup of children was not assessed.
Lastly, because the research is based on pre-existing medical data, which could have inconsistent or insufficient documentation, the retrospective study design raises the risk of information bias, regarding the documentation of the river name in the medical report. Some river-related cases may have been missed if neither the river name “Aare” nor the word “Fluss” was explicitly documented in the clinical records, potentially leading to an underestimation of the true number of cases. Furthermore, the accuracy of the data may be impacted by factors like the precise circumstances of occurrences, drug or alcohol use, and pre-existing medical issues that may not have been accurately documented.
River-related ED visits are a seasonal issue that primarily affects young males who participate in dangerous activities. Trauma, especially involving head and lower extremities, predominated over drowning incidents. Numerous injuries were caused by collisions with submerged items or jumping from bridges, underscoring the risks involved with urban river swimming.
The proportion of non-Swiss nationalities was notably high. This finding suggests that visitors and foreign residents are less knowledgeable about the river’s currents, exits and possible hazards such as hypothermia. This implies that to guarantee water safety for all swimmers, multilingual safety information and focused preventive initiatives should be initiated.
Although public safety campaigns along the Aare have been in place for several years, systematic data on injury characteristics and clinical outcomes have been limited. This study provides an evidence-based overview that can inform and refine ongoing prevention strategies, serving as a basis for evaluating their future impact.
Prevention measures should therefore focus on: i) Educating the public, particularly young adults, about the risks associated with river swimming, ii) Enhancing warnings and signs at high-risk areas, such as river entry points and bridge jumping points, and iii) Improving emergency readiness by guaranteeing prompt rescue operations and first aid supplies along rivers. By addressing the unique risks and challenges associated with urban swimming, public health campaigns can help create a safer environment for both locals and visitors while preserving this iconic Swiss tradition.
The dataset supporting the conclusions of this study is not publicly available due to institutional and legal data protection regulations. Deidentified data may be made available from the corresponding author upon reasonable request.
Custom code was developed for data cleaning and analysis and is available from the corresponding author upon reasonable request.
Author contributions: Martin Müller, Sabrina Jegerlehner and Thomas Maurer conceptualised the study and designed the methodology. Thomas Maurer conducted data collection and managed data curation. Martin Müller performed the data analysis. Julius Husarek, Thomas Maurer and Martin Müller prepared the original draft of the manuscript. Karsten Klingberg, Sabrina Jegerlehner and Aristomenis Exadaktylos edited the manuscript. All authors contributed to the revision of the manuscript and approved the final version.
This study received no external funding.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest related to the content of this manuscript was disclosed.
1. Hoffmeyer V. Nager en eaux vives, une spécialité des villes suisses: Le temps 2020. https://www.letemps.ch/societe/nager-eaux-vives-une-specialite-villes-suisses (accessed March 3, 2024).
2. Rederer K. Aareschwimmen in Bern n.d. https://www.lebendige-traditionen.ch/tradition/de/home/traditionen/aareschwimmen-in-bern.html (accessed March 3, 2024).
3. City of Bern. Badi-Bilanz 2023: Wechselhafte Saison mit Rekordtagen 2023. https://www.bern.ch/mediencenter/medienmitteilungen/aktuell_ptk/badi-bilanz-2023-wechselhafte-saison-mit-rekordtagen?searchterm=Badi (accessed March 3, 2024).
4. Schweizerische Lebensrettungs-Gesellschaft S. Flussregeln n.d. https://www.slrg.ch/de/praevention/slrg-regeln/flussregeln (accessed March 3, 2024).
5. City of Bern. Kampagne «Aare You Safe?» n.d. https://www.bern.ch/themen/sicherheit/pravention/aare-you-safe/projekt (accessed March 3, 2024).
6. Schweizerische Lebensrettungs-Gesellschaft S. Ertrinkungsstatistik 2023 n.d. https://www.slrg.ch/de/ueber-uns/publikationen/ertrinkungsstatistik (accessed March 3, 2024).
7. Schweizerische Unfallversicherungsanstalt (SUVA). Unfallstatistik 2024 n.d. https://www.suva.ch/de-ch/unfall/unfallstatistik-schweiz-und-uvg (accessed March 3, 2024).
8. Beratungsstelle für Unfallverhütung (BFU). Unfallverhütung 2023. https://www.bfu.ch/de (accessed March 3, 2024).
9. Department of Emergency Medicine BUH. Zahlen und Fakten Universitätsklinik für Notfallmedizin - Jahresbericht 2023 n.d. https://notfallmedizin.insel.ch/de/ueber-uns/ueber-die-klinik/zahlen-und-fakten (accessed March 3, 2024).
10. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007 Oct;335(7624):806–8.
11. Birrenbach T, Hoffmann M, Hautz SC, Kämmer JE, Exadaktylos AK, Sauter TC, et al. Frequency and predictors of unspecific medical diagnoses in the emergency department: a prospective observational study. BMC Emerg Med. 2022 Jun;22(1):109.
12. Canadian Drowning Report 2016. https://www.lifesavingsociety.com/media/241812/canadiandrowningreport_english_web.pdf
13. Quan L, Cummings P. Characteristics of drowning by different age groups. Inj Prev. 2003 Jun;9(2):163–8.
14. Ioannidis JP. The Proposal to Lower P Value Thresholds to. 005. JAMA. 2018 Apr;319(14):1429–30.
15. Henderson H, Wilson RC. Water incident related hospital activity across England between 1997/8 and 2003/4: a retrospective descriptive study. BMC Public Health. 2006 Aug;6(1):210.
16. Pollard KA, Gottesman BL, Rochette LM, Smith GA. Swimming injuries treated in US EDs: 1990 to 2008. Am J Emerg Med. 2013 May;31(5):803–9.
17. Ryan KM, Dugas J, Pina T, Maksimenko Y, Liu J. Drowning injuries in the United States: patient characteristics, mortality risk, and associated primary diagnoses. Injury. 2020 Nov;51(11):2560–4.
18. Flury T, Gerber J, Anwander H, Müller M, Jakob DA, Exadaktylos A, et al. Who was at risk of trauma-related injuries during the COVID-19 pandemic? A retrospective study from a level 1 trauma centre in Switzerland. Swiss Med Wkly. 2024 Jan;154(1):3539.
19. Anwander H, Klingberg K, Gerber J, Bednarski P, Exadaktylos A, Müller M. Major trauma during COVID-19 in a level 1 trauma centre in Switzerland - a cohort study comparing the years 2020 and 2019. Swiss Med Wkly. 2021 Aug;151(33-34):w30010.
20. Heming N, Serve E, Weiss N, Imbert A, Ducharne G, Diehl JL, et al. Drowning after falling from a medium-height bridge: multiple trauma victims. Prehosp Emerg Care. 2012;16(3):356–60.
21. Kikuike K, Uemura S, Miyamoto K, Horiya Y, Shimizu K. Upper lumbar burst fracture due to recreational high jumping into a river: report of five cases. Arch Orthop Trauma Surg. 2009 Jan;129(1):87–90.
22. Fang YX, He M, Lin JY, Ma KJ, Zhao H, Hong Z, et al. Suicidal drownings with psychiatric disorders in Shanghai: a retrospective study from 2010.1 to 2014.6. PLoS One. 2015 Apr;10(4):e0121050.
23. Lawes JC, Peden AE, Bugeja L, Strasiotto L, Daw S, Franklin RC. Suicide along the Australian coast: exploring the epidemiology and risk factors. PLoS One. 2021 May;16(5):e0251938.
24. Dunne CL, Sweet J, Clemens T. The link between medical conditions and fatal drownings in Canada: a 10-year cross-sectional analysis. CMAJ. 2022 May;194(18):E637–44.
25. Xie Z, Huang Z, Ran Q, Luo W, Du W. Global burden of drowning and risk factors across 204 countries from 1990 to 2021. Sci Rep. 2025 Mar;15(1):10916.
26. Jakob DA, Müller M, Jud S, Albrecht R, Hautz W, Pietsch U. The forgotten cohort-lessons learned from prehospital trauma death: a retrospective cohort study. Scand J Trauma Resusc Emerg Med. 2023 Aug;31(1):37.
The appendix is available in the pdf version of the article at https://doi.org/10.57187/4839.