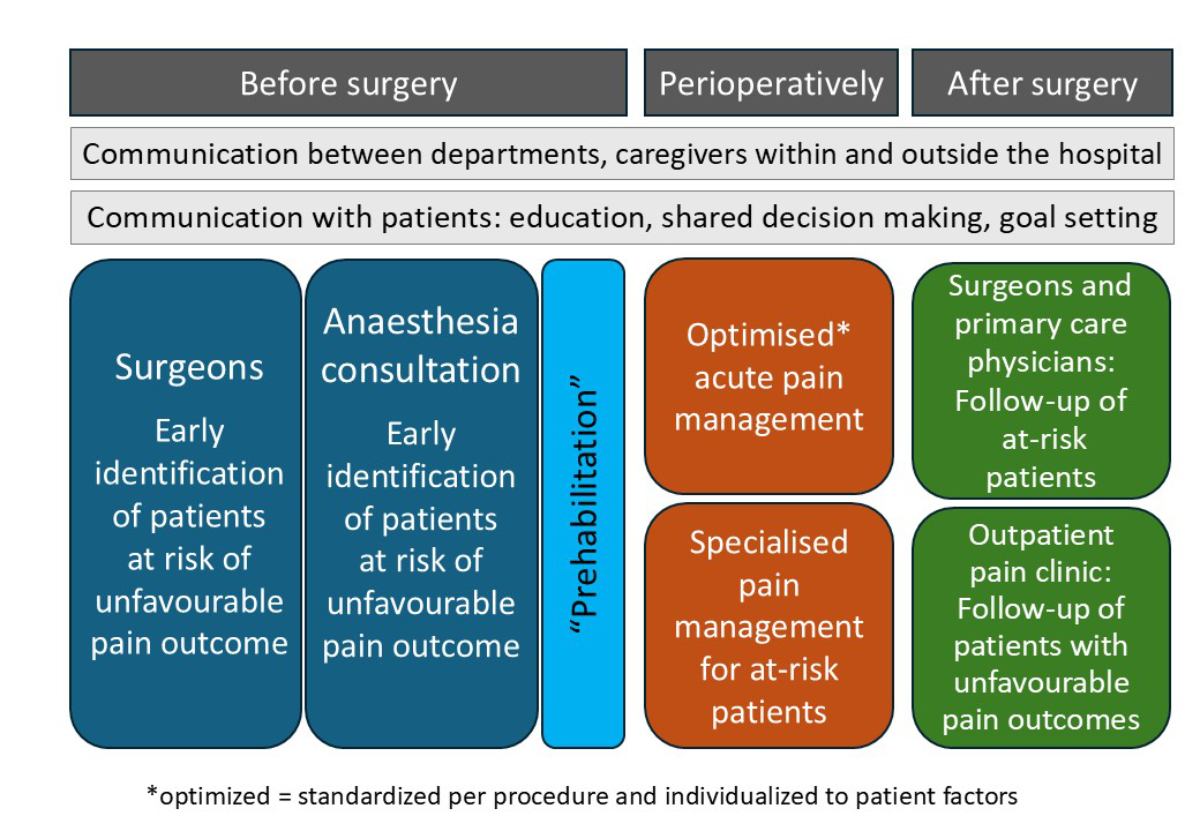
Figure 1The continuum of care in perioperative pain management.
DOI: https://doi.org/https://doi.org/10.57187/4797
As early as 40 years ago, it was recognised that despite the introduction of new analgesic drugs and techniques, postoperative pain management had not substantially improved for many patients due to the lack of adequate organisational structures [1]. Various studies have shown that the percentage of patients with severe postoperative pain remains high [2]. In addition, focusing on pain intensity alone has been shown to be insufficient for adequate postoperative pain management [3–5]. Insufficient postoperative pain control was considered to be due to a lack of experience, time, and staffing required to care for patients with pain. Furthermore, there was often no competent surgeon available on the ward for back-up or to prescribe the necessary medication [6].
In 1985, departments of anaesthesiology first introduced Acute Pain Services (APS) into patient care; these services were welcomed enthusiastically and considered an exciting new opportunity [7, 8]. Many institutions have followed and implemented APS, in most cases by anaesthesiologists with an interest and expertise in the field. However, only a minority of patients were cared for by APS teams, as they focused on major surgical procedures for which more sophisticated analgesic techniques, such as PCA and neuraxial or peripheral regional analgesia, were provided [5, 9–13].
Considerable variation in the availability, function, and quality of APS has been reported, and patient care varies among different health care systems, hospital sizes and structures, the surgical spectrum, and, not least, economic constraints [5, 9–13]. Thus, overall improvement in the quality of pain management has been questioned or has been less than anticipated [14, 15]. APS has often been only a self-defined label, with no standardised criteria that have to be met.
Meanwhile, the original concept of APS providing postoperative analgesia has been expanded. It is well recognised that multidisciplinary approaches – involving all health care providers, physicians, nurses, and physiotherapists on the ward, and, if available, specialised pain services – are essential to improve outcomes for patients, specifically among those at risk of poorly controlled perioperative pain. This implies that caregivers outside the department of anaesthesiology must have sufficient knowledge not only of analgesic therapy for acute postoperative pain but also of the risk of developing chronic pain after surgery. The overall management of pain before and after surgery is referred to as “perioperative pain medicine”.
To enhance awareness outside the field of anaesthesiology, this article summarises and comments on the current recommendations on perioperative pain management as one key factor in the emerging field of perioperative medicine. The recommendations were developed by a Swiss expert group of anaesthesiologists, pain specialists, and pain nurses [16].
The organisation of perioperative pain management requires an adequate structural foundation as well as appropriate processes, and recommendations have been made for both. The recommendations were developed by a group of 16 experts in perioperative pain medicine who were members of the Acute Pain Interest Group and the Commission for Pain Medicine and Palliative Care of the Swiss Society of Anaesthesiology and Perioperative Medicine (SSAPM) on behalf of the SSAPM board. The reporting of the recommendations followed the RIGHT statement for reporting items for practice guidelines in health care [17]. Items were selected based on existing evidence, guidelines, and recent publications, such as those of other European countries [6, 9, 18–21]. No new systematic review was carried out. For the structural recommendations, a two-round Delphi process was used. The experts voted on the strength of each recommendation:
A “strong recommendation” (or “must”) indicates that at least 75% of the experts voted for a strong recommendation.
A “recommendation” (or “should”) indicates that more than 25% but less than 75% of the experts voted for a strong recommendation.
An “open recommendation” (or “can”) means that less than 25% of the experts voted for a strong recommendation.
In the text that follows, the strength of the recommendation is indicated by the following wording: strong recommendation, or “must”; recommendation, or “should”; and open recommendation, or “can”, all marked in bold.
The process recommendations were adapted from the pre-existing literature without defining a strength of recommendation, as optimising processes is independent of the size and resource availability of individual institutions. The final structural and procedural recommendations were subsequently reviewed and endorsed by the board of the SSAPM before publication on the SSAPM website [16].
The recommendations emphasise the necessity of interdisciplinary and interprofessional cooperation for perioperative pain management, including all departments and health care professionals involved (physicians, nurses, andphysiotherapists).
The majority of patients experiencing postoperative pain are cared for by the staff of the surgical wards, while only a minority receive care from a dedicated pain service. However, surgeons and ward nurses have limited resources for pain management. As a consequence, it is strongly recommended to establish jointly developed, written and signed agreements between surgical departments and the pain service that detail responsibilities of all partners to avoid conflicts and gaps in therapy. Furthermore, it is strongly recommended that all hospitals implement common written standard operating procedures (SOPs) for pain management, developed jointly by health care providers from the surgical and anaesthesia departments. These should be founded on evidence-based international recommendations [22, 23] and adapted to local conditions.
To provide adequate perioperative pain management, qualified personnel are required. Thus, a strong recommendation was made for the availability of designated qualified medical and nursing staff with reserved time contingents for perioperative pain management. The consensus was that the head of the perioperative pain service should be well trained in pain medicine. A strong recommendation was made that the position be held by a consultant board-certified anaesthesiologist who has at least basic training in pain medicine, such as the SPS pain specialist certificate issued by the Swiss Pain Society (SPS). In large (A1) hospitals, the equivalent of the SSIPM certificate issued by the Swiss Society of Interventional Pain Medicine (SSIPM) is recommended. It was also specified that the head of the perioperative pain service must have overall responsibility to ensure that the pain service has a clear organisational structure.
For the nursing personnel of the perioperative pain service, training as either an anaesthesia or pain nurse is strongly recommended. If nurses are not trained as pain nurses, they should have at least basic training in pain medicine, such as the SPS pain specialist certificate (or equivalent). In larger hospitals, the employment of an advanced practice nurse (APN) may also facilitate the coordination of organisational tasks and perioperative management for patients with a complex pain history, severe comorbidity, or the need for long-term hospitalisation with pain as a leading symptom.
A strong recommendation was made for regular (at least weekly) meetings of the pain service team to discuss and communicate patient-related problems. Furthermore, regular (at least monthly) meetings of the pain service are recommended to discuss organisational problems.
Patients with acute pain must be cared for around the clock. Physicians and nurses of other disciplines must know how to reach the perioperative pain service at any time. Therefore, it is strongly recommended that a reference person for pain management is available 24/7 and has dedicated contact information that is visible to all disciplines and professions within the hospital. The experts suggested that, outside of working hours, a board-certified anaesthesiologist be responsible for pain management and that at least one physician with specialist training in pain medicine be available either as an in-house or on-call physician. However, the panel acknowledged that not enough physicians with training in pain medicine are currently available in Switzerland. Therefore, the strength of this recommendation was left open. Nonetheless, it is recommended that any physician responsible for the perioperative pain service during on-call hours should have undergone at least a 2-month rotation in a perioperative pain service. Consequently, all anaesthesiologists in training should have a scheduled rotation in a perioperative pain service.
The perioperative pain service must collaborate with all surgical departments, and all information about patients should be shared with other departments. The assessment of pain severity must consider the multidimensionality of pain to reflect the now well-established biopsychosocial contribution to the phenomenon of pain. Thus, focusing solely on pain intensity is no longer sufficient. Pain-related physical (surgery-specific) and affective interference are important variables that influence recovery after surgery and must be measured and documented (strong recommendation). These pain-related patient-reported outcomes (PROs) and their measures (PROMs) as well as possible treatment-related side effects must be assessed at least once per shift (strong recommendation). In patients with insufficient analgesia and/or with changed analgesic treatment, additional assessment may be necessary depending on the patient’s status.
The documentation must include the patient’s diagnosis and current therapy, basic analgesics prescribed, including rescue medication, as well as pain intensity at rest and during activity (movement). In case of additional intravenous, peripheral, or neuraxial regional techniques, pump settings, patient-controlled analgesia (PCA) parameters, the number of PCA demands and delivered boluses, as well as total 24 h consumption and additional rescue medication must be documented.
It is strongly recommended that hospitals have an electronic documentation system in place, with information accessible to all disciplines and professions.
Hospitals should implement regular training courses in pain management for surgical teams (surgeons, nurses,and physiotherapists). These should be institutionalised and made mandatory on a regular basis (recommendation). Anaesthesiologists involved in pain therapy should cooperate in providing such education.
Furthermore, the panel strongly recommended that personnel of the pain service participate in at least 3 hours of continuing medical education related to pain management each year.
Whereas structures describe the environment in which care is delivered (including personnel, organisational characteristics, and resources), processes describe how care is provided to patients in daily clinical routine, how personnel interact with patients, and how the cooperation of different disciplines and professions works.
Pain management is a multidisciplinary, multiprofessional approach that must be regularly reinforced and updated. Only a well-coordinated interplay between structures and processes can lead to overall favourable patient outcomes and positively impact population health. For patients at risk of chronic postsurgical pain, it is especially important to ensure a continuum between inpatient and postoperative outpatient pain management. Clearly defined processes between institutions and primary care providers are mandatory to prevent the transition to chronic pain.
The published recommendations do not specify the internal organisation of the perioperative pain service. Depending on the size and organisation of the hospital, rounds may be performed by nurses only or may be supervised by a pain physician or a dedicated physician. By contrast, the recommendations focus on interdisciplinary collaboration within and outside the hospital to guarantee a continuum of care concerning pain management.
Similarly, surgeons and anaesthesiologists should cooperate in the follow-up of patients at risk using surgery-specific functional recovery protocols and multidimensional pain evaluations. This collaboration can be organised, for example, as regular interdisciplinary meetings and case discussions.
Collaboration, of course, is not limited to surgeons and anaesthesiologists. Often, a continuum of care is absent between inpatient and outpatient pain management. However, such a continuum of care is crucial for the follow-up of patients at risk of chronic pain and should include the primary care provider (family physician) and – depending on the patient’s needs – an outpatient pain specialist, physiotherapist, and psychologist. To enhance this collaboration between caregivers inside and outside the hospital, the development of common pathways in the prevention, documentation, and treatment of pain is proposed [26].
As mentioned above, preoperative contacts with the patients by surgeons and anaesthesiologists should be used to provide information regarding analgesic treatment options, including non-pharmacological treatment approaches, and possible adverse events and risks. This includes patient education on the goals of analgesic therapy, assessment of pain and function, and the setting of realistic treatment expectations. Discussion with the patient should encourage self-efficacy and be based on shared decision-making.
Unfavourable pain-related outcomes after surgery include severe acute pain with difficult postoperative pain management, delayed patient mobilisation, insufficient compliance with physiotherapy, and, in the long run, chronic post-surgical pain (CPSP) or other chronic pain [27]. Patients at risk of an abnormal pain trajectory must be identified, ideally before surgery, closely monitored perioperatively, and followed up after discharge (table 1).
Table 1Risk factors for problematic pain management and unfavourable pain outcomes after surgery – either problematic acute pain (A), chronic pain after surgery (B), or prolonged opioid use after surgery (C) [28–33].
| Patient-related risk factors (can be assessed preoperatively) | For outcome | |
| Patient-related factors | Younger (adult) age | A, B, C |
| Female sex | A, B | |
| Pre-existing chronic pain (surgical site or elsewhere) | A, B, C | |
| Opioid medication before admission | A, B | |
| History of substance use disorder | C | |
| Sleep disturbance | B | |
| Low socioeconomic status | B | |
| Psychological factors | Pain catastrophising, | A, B |
| Low self-efficacy/helplessness | A, B | |
| Expected pain | A, B | |
| State and trait anxiety | A, B | |
| Depression | A, B, C | |
| Intraoperative risk factors | ||
| Type of surgery (already known before surgery) | Limb amputation | B |
| Spine surgery | ||
| Arthroplasty | ||
| Mastectomy | ||
| Thoracotomy | ||
| Trauma surgery | ||
| Open abdominal surgery | ||
| Hernia surgery | ||
| Surgery-related risk factors | Extended, traumatic surgery | B |
| Revision surgery, repeated surgery | ||
| Intraoperative nerve injury | ||
| Postoperative risk factors | ||
| Patient-related | High analgesic demands | B |
| Severe pain on mobilisation | ||
| Disease-related risk factors | Examples: adjuvant cancer therapy (radiation, chemotherapy) | B |
After surgery, an abnormal pain trajectory indicating a potential chronification may be signalled by several parameters, which should be monitored manually (by chart review and patient visits in cooperation with surgeons, ward nurses, and physiotherapists) or automatically (by alerts in an electronic patient data management system):
Chronic pain is associated with increased pain-related physical and affective interference, discomfort, and distress. With the launch of the 11th version of the International Classification of Diseases (ICD-11) by the World Health Organisation in 2022, chronic pain is now recognised as a disease rather than merely a symptom [34]. The ICD-11 emphasises the multifactorial dimensions of chronic pain, with biological, psychosocial, and social factors contributing (Box 1). This also involves a multidimensional assessment of pain, which is not limited to pain scores but also covers pain-related physical and psychological impairment as well as psychosocial factors [27]. In the past, definitions of chronic postsurgical pain were heterogeneous, and many previous studies did not clearly differentiate between different types of chronic pain after surgery [27]. The ICD-11 now provides a clear-cut definition of CPSP that enables improved communication and more targeted pain management (Box 1). It is discussed as a major health care problem significantly influencing patients’ quality of life. Preventive measures of CPSP are being discussed; however, a general recommendation for prophylaxis is not possible at the moment, with the exception that an excellent perioperative multimodal analgesia and a regional technique, when indicated, should be performed [33]. However, early detection of an unfavourable pain trajectory in the subacute phase or new (neuropathic) pain in the surgical area and/or associated dermatomes should be cause for re-evaluation and consistent multidisciplinary treatment, preferably by pain specialists at a pain centre or a transitional pain service [9, 33].
In a third coding level of the ICD-11, one can distinguish between CPSP after herniotomy, amputation, mastectomy, thoracotomy, hysterectomy, arthroplasty, and spinal surgery. Here, it is mentioned that if the pain continues from a preoperative condition, either the intensity or the pain characteristics must be different from the preoperative status.
A postoperative gradual reduction in the opioid dose used for postoperative analgesia should be started as early as possible to prevent long-term opioid medication with possible related harm [36]. The general aim is patient discharge without any opioid medication. In the case of discharge with opioids, it is recommended that written and oral patient information on how to taper analgesics be given and explained to the patient. In addition, written recommendations on dosing and tapering of analgesics and co-analgesics should be provided to the general practitioners or doctors responsible for further care.
Patients receiving preoperative opioid therapy highlight the importance of interdisciplinary collaboration, as they are at increased risk of adverse postoperative outcomes [37]. There is consensus that opioid tapering must be started well before surgery, although optimal timing remains undefined [38].
In patients in whom preoperative opioid tapering is not possible, special attention is required to avoid accidental interruption of therapy and possible opioid withdrawal during the hospital stay. Independent of a pre-existing long-term opioid medication, additional postoperative analgesia must be carefully planned and should be non-opioid-based analgesia (e.g. regional analgesic technique) whenever possible. Written SOPs should be in place to manage these patients.
New long-term opioid medication due to chronic pain after surgery is discussed as one reason for the North American opioid crisis, with prescription practices of physicians contributing considerably. In Europe, opioid prescriptions in general have also increased; however, an opioid epidemic specifically induced by long-term opioid use due to CPSP has not been substantiated in Switzerland to date [39, 40].
The recommendations emphasise that hospital-specific standards (SOP/guidelines for perioperative pain management) should be jointly developed and implemented by all disciplines and professions. These should include standards for pain management based on a multimodal analgesic concept (see table 2 as an example) based on up-to-date guidelines (e.g. those of ANZCA [22] and ESRA - PROSPECT [23]).
Table 2Multimodal perioperative analgesia. Contraindications of the drugs and possible drug interactions should always be considered. (i.v.: intravenous).
| Loco-regional anaesthesia: use whenever possible! | Neuraxial analgesia, particularly epidural catheters for extended abdominal/thoracic surgery |
| Truncal blocks such as TAP-block, PEC-block, paravertebral block | |
| Peripheral nerve blocks (“single shot”) | |
| In select cases, peripheral nerve or plexus catheters with continuous administration | |
| Wound infiltration if no block is indicated or possible | |
| Systemic analgesia | Basic analgesia with one to two different groups of non-opioid analgesics in sufficient daily doses: NSAIDs or Cox2-inhibitors, metamizole, paracetamol |
| If indicated: short-acting opioids, including oral patient-controlled analgesia (PCA) or, in cases of contraindications to the oral route, i.v. PCA | |
| Co-analgesics – cave: use only for specific indications, the evidence is weak for most types of surgery! | Intraoperative i.v. dexamethasone as antiemetic and co-analgesic (for analgesic effects, at least 8 mg i.v. given in a timely manner for a delayed effect) |
| i.v. ketamine (intraoperatively or by acute pain service) | |
| i.v. lidocaine (intraoperatively or by acute pain service) | |
| Others (e.g. gabapentinoids, antidepressants, α2-agonists) | |
| Physical treatments | Early mobilisation/ambulation |
| Physiotherapy | |
| Physical measures such as cold packs and positioning | |
| Acupuncture, either for treatment of pain or for PONV | |
| TENS | |
| Psychological interventions – note: should start preoperatively whenever possible | Patient education (ideally for all patients) |
| Reduction of fear and anxiety (e.g. by hypnosis) | |
| Specific short interventions for patients with pain catastrophising, low self-efficacy | |
| Treatment of depression |
Non-opioid analgesics should be the basis of analgesic therapy. They should be given at regular time intervals and in sufficient daily doses (table 3). The analgesic potency of NSAIDs/Cox-2 inhibitors and metamizole is considered to be higher than that of paracetamol, which, by contrast, probably has the lowest risk of severe side effects, as long as it is not overdosed.
A combination of two different classes of non-opioid analgesics, such as an NSAID/COX2 inhibitor (e.g. ibuprofen, ketorolac, or celecoxib) with metamizole or paracetamol, is recommended in cases of moderate to severe pain. Non-steroidal analgesics should be used with caution in patients with renal impairment, severe cardiopathy, or gastrointestinal ulcers (reduce dose or avoid). In cases of risk of gastrointestinal ulcers, COX2 inhibitors are preferable, and/or a proton pump inhibitor such as omeprazole.
Doses of non-opioid analgesics should be reduced in patients with comorbidities, older age, and a body weight of <50 kg (refer to specific drug information). Whenever possible, the oral route should be preferred. For tapering of analgesics, opioids should be reduced and discontinued first, followed by non-opioid analgesics.
Table 3Examples of non-opioid analgesic regimens. General recommendation: treatment should be administered at the lowest effective dose and for the shortest duration possible, tailored to the individual needs of the patient.
| Substance | Initial dose (mg) | Dosing interval (hours) | Maximum daily dose (mg) | Maximum duration of use (from manufacturers’ instructions) |
| Oral administration | ||||
| Paracetamol | 1000 | 6 | 4000 | |
| Ibuprofen | 400-800 | 6-8 | 2400 | |
| Celecoxib | 200 | 12 | 400 | Shortest time possible |
| Diclofenac | 50-100 | 12 | 150 | |
| Metamizole | 1000 | 4-6 | 4000 | Depending on type and severity of disease |
| Etoricoxib | 60-90 (1 mg/kg) | 24 | 60-120 | Shortest time possible |
| i.v. administration | ||||
| Ketorolac i.v. | 10-30 | 8 | 90 | 2 days |
| Dexketoprofen i.v. | 50 | (6) 8-12 | 150 | Short term, no longer than 2 days |
| Ibuprofen i.v. | 400-600 | 6-8 | 1200 | Shortest time possible, no longer than 3 days |
| Metamizole i.v. | 1000 | 4-6 | 5000 | Depending on the type and severity of the disease |
| Paracetamol i.v. | 1000 | 6 | 4000 | Short term |
Patients are often followed up after hospital discharge by surgeons but not by anaesthesiologists. In addition, if the hospital’s acute pain service and outpatient pain clinic are separate entities, there is often no continuum of care between inpatient and outpatient pain management. However, such a continuum of care is crucial for the follow-up of patients at risk of persistent postoperative pain and should also include the primary care provider (family physician).
Clearly defined pathways and structured communication within the health care institution (including surgeons, inpatient and outpatient pain specialists, and physiotherapists) and between the institution and primary care providers are essential to provide effective discharge management and potentially also prevent the transition to chronic pain.
To facilitate the transition from inpatient to outpatient pain management, some institutions may choose to create specialised teams, as has been discussed and published by teams from several hospitals, such as those in Toronto (Transitional Pain Service, TPS), Belgium (Chronic Postsurgical Pain Service), Helsinki (Acute Pain Outpatient Clinic), and the USA (Perioperative CPSP Home, PSH) [33, 42–45]. Preoperative group interventions, so-called preoperative surgery schools designed to enhance patients’ treatment participation and self-efficacy, have also been implemented [46]. No recommendations have been made to create a specialised team, and the organisation will depend on the individual characteristics of each hospital.
In contrast to previous guidelines [21, 23, 47], which focus on purely medical recommendations, these new guidelines emphasise organisational requirements to improve perioperative pain management. Key elements of these recommendations include interdisciplinary cooperation within a hospital as well as cooperation with caregivers outside hospitals, who follow the patient after discharge. This continuum of care in perioperative pain management is summarised in figure 1. It is clear that the implementation of this continuum of care requires adequate structural resources and dedicated processes (i.e. organisational arrangements) to be successful.
In summary, these recommendations aim to standardise and define perioperative pain management as a core element of modern perioperative medicine.
Figure 1The continuum of care in perioperative pain management.
The recommendations can be downloaded in English, German, Italian, and French from the SSAPM website: https://www.ssapm.ch/spezialgebiete/schmerzmedizin.
We would like to thank the authors of the SSAPM recommendations for perioperative pain medicine for their work: Andrea Berendes, St. Gallen; Mirko Binda, Lugano; Severin Burki, Stans; Sibylle Chettata, Basel; Renate Gerber-Herren, Winterthur; Michael Harnik, Bern; Katrin Meyer, Luzern; Wilhelm Ruppen, Basel; Jürg Schliessbach, Zürich; Susanne Schwarz, St. Gallen; Konrad Streitberger, Bern; Luzia Vetter, Luzern.
We thank the speaker of the SSAPM acute pain group, Joachim Dias (Luzern), for helpful discussions and comments on the manuscript.
The recommendations can be downloaded in English, German, Italian, and French from the SSAPM website: https://www.ssapm.ch/spezialgebiete/schmerzmedizin.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest related to the content of this manuscript was disclosed.
1. Rawal N, Berggren L. Organization of acute pain services: a low-cost model. Pain. 1994 Apr;57(1):117–23. doi: https://doi.org/10.1016/0304-3959(94)90115-5
2. Small C, Laycock H. Acute postoperative pain management [British Journal of Surgery]. Br J Surg. 2020 Jan;107(2):e70–80. doi: https://doi.org/10.1002/bjs.11477
3. Baamer RM, Iqbal A, Lobo DN, Knaggs RD, Levy NA, Toh LS. Utility of unidimensional and functional pain assessment tools in adult postoperative patients: a systematic review. Br J Anaesth. 2022 May;128(5):874–88. doi: https://doi.org/10.1016/j.bja.2021.11.032
4. van Boekel RL, Vissers KC, van der Sande R, Bronkhorst E, Lerou JG, Steegers MA. Moving beyond pain scores: multidimensional pain assessment is essential for adequate pain management after surgery. PLoS One. 2017 May;12(5):e0177345. doi: https://doi.org/10.1371/journal.pone.0177345
5. Erlenwein J, Koschwitz R, Pauli-Magnus D, Quintel M, Meißner W, Petzke F, et al. A follow-up on Acute Pain Services in Germany compared to international survey data. Eur J Pain. 2016 Jul;20(6):874–83. doi: https://doi.org/10.1002/ejp.812
6. Rawal N. Current issues in postoperative pain management. Eur J Anaesthesiol. 2016 Mar;33(3):160–71. doi: https://doi.org/10.1097/EJA.0000000000000366
7. Ready LB, Oden R, Chadwick HS, Benedetti C, Rooke GA, Caplan R, et al. Development of an anesthesiology-based postoperative pain management service. Anesthesiology. 1988 Jan;68(1):100–6. doi: https://doi.org/10.1097/00000542-198801000-00016
8. Saidman LJ. The anesthesiologist outside the operating room: a new and exciting opportunity. Anesthesiology. 1988 Jan;68(1):1–2. doi: https://doi.org/10.1097/00000542-198801000-00001
9. Stamer UM, Liguori GA, Rawal N. Thirty-five Years of Acute Pain Services: Where Do We Go From Here? Anesth Analg. 2020 Aug;131(2):650–6. doi: https://doi.org/10.1213/ANE.0000000000004655
10. Benhamou D, Viel E, Berti M, Brodner G, De Andres J, Draisci G, et al. [PATHOS study on postoperative pain management in Europe: french data]. Ann Fr Anesth Réanim. 2008 Sep;27(9):664–78. doi: https://doi.org/10.1016/j.annfar.2008.07.092
11. Rawal N. Organization, function, and implementation of acute pain service. Anesthesiol Clin North America. 2005 Mar;23(1):211–25. doi: https://doi.org/10.1016/j.atc.2004.11.012
12. Montes A, Aguilar JL, Benito MC, Caba F, Margarit C; Acute Pain Group of the Spanish Pain Society (SED). Management of postoperative pain in Spain: a nationwide survey of practice. Acta Anaesthesiol Scand. 2017 May;61(5):480–91. doi: https://doi.org/10.1111/aas.12876
13. Nasir D, Howard JE, Joshi GP, Hill GE. A survey of acute pain service structure and function in United States hospitals. Pain Res Treat. 2011;2011:934932. doi: https://doi.org/10.1155/2011/934932
14. White PF, Kehlet H. Improving postoperative pain management: what are the unresolved issues? Anesthesiology. 2010 Jan;112(1):220–5. doi: https://doi.org/10.1097/ALN.0b013e3181c6316e
15. Meissner W, Huygen F, Neugebauer EA, Osterbrink J, Benhamou D, Betteridge N, et al. Management of acute pain in the postoperative setting: the importance of quality indicators. Curr Med Res Opin. 2018 Jan;34(1):187–96. doi: https://doi.org/10.1080/03007995.2017.1391081
16. Swiss Society for Anaesthesiology and Perioperative Medicine - SSAPM. [cited 2025 Apr 22]. Available from: https://www.ssapm.ch/spezialgebiete/schmerzmedizin
17. Chen Y, Yang K, Marušic A, Qaseem A, Meerpohl JJ, Flottorp S, et al.; RIGHT (Reporting Items for Practice Guidelines in Healthcare) Working Group. A Reporting Tool for Practice Guidelines in Health Care: the RIGHT Statement. Ann Intern Med. 2017 Jan;166(2):128–32. doi: https://doi.org/10.7326/M16-1565
18. van den Heuvel SA, van Boekel RL, Cox FJ, Ferré F, Minville V, Stamer UM, et al. Perioperative pain management models in four European countries: A narrative review of differences, similarities and future directions. Eur J Anaesthesiol. 2024 Mar;41(3):188–98. doi: https://doi.org/10.1097/EJA.0000000000001919
19. Brunsmann F, Stamer U, Meissner W. Akutschmerz-Management: Aufgabe für Team und Leitung. Dtsch Arztebl 2021; 118 (6): A 301–2.
20. Erlenwein J, Meißner W, Petzke F, Pogatzki-Zahn E, Stamer U, Koppert W. Personelle und organisatorische Voraussetzungen für Schmerzdienste in Krankenhäusern : Empfehlung der Deutschen Gesellschaft für Anästhesiologie und Intensivmedizin e. V. Anaesthesist. 2019 May;68(5):317–24. doi: https://doi.org/10.1007/s00101-019-0589-8
21. Aubrun F, Nouette-Gaulain K, Fletcher D, Belbachir A, Beloeil H, Carles M, et al. Revision of expert panel’s guidelines on postoperative pain management. Anaesth Crit Care Pain Med. 2019 Aug;38(4):405–11. doi: https://doi.org/10.1016/j.accpm.2019.02.011
22. Schug S, Palmer G, Scott D, Alcock M, Halliwell R, Mott J, et al. Acute Pain Management: Scientific Evidence. 5th ed. Melbourne: ANZCA & FPM; 2020. Available from: https://www.anzca.edu.au/resources/college-publications/acute-pain-management/apmse5.pdf
23. The European Society of Regional Anaesthesia and Pain Therapy. Prospect (procedure specific postoperative pain management). [cited 2025 Apr 22]. Available from: https://esraeurope.org/pain-management/
24. Papadomanolakis-Pakis N, Uhrbrand P, Haroutounian S, Nikolajsen L. Prognostic prediction models for chronic postsurgical pain in adults: a systematic review. Pain. 2021 Nov;162(11):2644–57. doi: https://doi.org/10.1097/j.pain.0000000000002261
25. Papadomanolakis-Pakis N, Haroutounian S, Sørensen JK, Runge C, Brix LD, Christiansen CF, et al. Development and internal validation of a clinical risk tool to predict chronic postsurgical pain in adults: a prospective multicentre cohort study. Pain. 2025 Mar;166(3):667–79. doi: https://doi.org/10.1097/j.pain.0000000000003405
26. AlGhamdi SS, Aljohani DM, Adam R, Forget P. Acute Pain Management at the Intersection of Primary and Secondary Care: Insights from Recent Literature. J Clin Med. 2025 Oct;14(21):7732. doi: https://doi.org/10.3390/jcm14217732
27. Stamer UM, Lavand’homme P, Hofer DM, Barke A, Korwisi B. Chronic postsurgical pain in the ICD-11: implications for anaesthesiology and pain medicine. Br J Anaesth. 2025 Mar 14;S0007-0912(25)00094-7.
28. Sydora BC, Whelan LJ, Abelseth B, Brar G, Idris S, Zhao R, et al. Identification of Presurgical Risk Factors for the Development of Chronic Postsurgical Pain in Adults: A Comprehensive Umbrella Review. J Pain Res. 2024 Jul;17:2511–30. doi: https://doi.org/10.2147/JPR.S466731
29. Andreoletti H, Dereu D, Combescure C, Rehberg B. A systematic review and meta-analysis of three risk factors for chronic postsurgical pain: age, sex and preoperative pain. Minerva Anestesiol. 2022 Oct;88(10):827–41. doi: https://doi.org/10.23736/S0375-9393.22.16489-8
30. Ramo S, Frangakis S, Waljee JF, Bicket MC. Risk factors for persistent postoperative opioid use: an entity distinct from chronic postsurgical pain. Reg Anesth Pain Med. 2025 Feb;50(2):121–8. doi: https://doi.org/10.1136/rapm-2024-105599
31. Varallo G, Giusti EM, Manna C, Castelnuovo G, Pizza F, Franceschini C, et al. Sleep disturbances and sleep disorders as risk factors for chronic postsurgical pain: A systematic review and meta-analysis. Sleep Med Rev. 2022 Jun;63:101630. doi: https://doi.org/10.1016/j.smrv.2022.101630
32. Rosenberger DC, Pogatzki-Zahn EM. Chronic post-surgical pain - update on incidence, risk factors and preventive treatment options. BJA Educ. 2022 May;22(5):190–6. doi: https://doi.org/10.1016/j.bjae.2021.11.008
33. Moka E, Aguirre JA, Sauter AR, Lavand’homme P; European Society of Regional Anaesthesia and Pain Therapy (ESRA). Chronic postsurgical pain and transitional pain services: a narrative review highlighting European perspectives. Reg Anesth Pain Med. 2025 Feb;50(2):205–12. doi: https://doi.org/10.1136/rapm-2024-105614
34. Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019 Jan;160(1):19–27. doi: https://doi.org/10.1097/j.pain.0000000000001384
35. ICD-11 Coding Tool Mortality and Morbidity Statistics (MMS). [cited 2025 Apr 21]. Available from: https://icd.who.int/ct/icd11_mms/en/release
36. Levy N, Quinlan J, El-Boghdadly K, Fawcett WJ, Agarwal V, Bastable RB, et al. An international multidisciplinary consensus statement on the prevention of opioid-related harm in adult surgical patients. Anaesthesia. 2021 Apr;76(4):520–36. doi: https://doi.org/10.1111/anae.15262
37. Frangakis SG, Kavalakatt B, Gunaseelan V, Lai Y, Waljee J, Englesbe M, et al. The Association of Preoperative Opioid Use with Postdischarge Outcomes: A Cohort Study of the Michigan Surgical Quality Collaborative. Ann Surg. 2025 Aug;282(2):234–41. doi: https://doi.org/10.1097/SLA.0000000000006265
38. Edwards DA, Hedrick TL, Jayaram J, Argoff C, Gulur P, Holubar SD, et al.; POQI-4 Working Group. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on Perioperative Management of Patients on Preoperative Opioid Therapy. Anesth Analg. 2019 Aug;129(2):553–66. doi: https://doi.org/10.1213/ANE.0000000000004018
39. Sitter T, Forget P. Persistent postoperative opioid use in Europe: A systematic review. Eur J Anaesthesiol. 2021 May;38(5):505–11. doi: https://doi.org/10.1097/EJA.0000000000001346
40. Hofer DM, Harnik M, Lehmann T, Stüber F, Baumbach P, Dreiling J, et al. Trajectories of pain and opioid use up to one year after surgery: analysis of a European registry. Br J Anaesth. 2024 Mar;132(3):588–98. doi: https://doi.org/10.1016/j.bja.2023.12.002
41. Schug SA, Lavand’homme P, Barke A, Korwisi B, Rief W, Treede RD; IASP Taskforce for the Classification of Chronic Pain. The IASP classification of chronic pain for ICD-11: chronic postsurgical or posttraumatic pain. Pain. 2019 Jan;160(1):45–52. doi: https://doi.org/10.1097/j.pain.0000000000001413
42. De Kock M. Expanding our horizons: transition of acute postoperative pain to persistent pain and establishment of chronic postsurgical pain services. Anesthesiology. 2009 Sep;111(3):461–3. doi: https://doi.org/10.1097/ALN.0b013e3181afde28
43. Tiippana E, Hamunen K, Heiskanen T, Nieminen T, Kalso E, Kontinen VK. New approach for treatment of prolonged postoperative pain: APS Out-Patient Clinic. Scand J Pain. 2016 Jul;12(1):19–24. doi: https://doi.org/10.1016/j.sjpain.2016.02.008
44. Vetter TR, Kain ZN. Role of the Perioperative Surgical Home in Optimizing the Perioperative Use of Opioids. Anesth Analg. 2017 Nov;125(5):1653–7. doi: https://doi.org/10.1213/ANE.0000000000002280
45. Clarke H, Poon M, Weinrib A, Katznelson R, Wentlandt K, Katz J. Preventive analgesia and novel strategies for the prevention of chronic post-surgical pain. Drugs. 2015 Mar;75(4):339–51. doi: https://doi.org/10.1007/s40265-015-0365-2
46. Fecher-Jones I, Ainsworth B, Gan TJ, Moonesinghe SR, Shaw AD, Grocott MP, et al.; Perioperative Quality Initiative Surgery School Consensus Group. Perioperative Quality Initiative consensus statement recommendations on the definition, development, implementation and outcomes of pre-operative surgery schools. Anaesthesia. 2025 Sep;80(9):1115–33. doi: https://doi.org/10.1111/anae.16648
47. AWMF S3 Leitlinie Akutschmerz. 2021 [cited 2023 Feb 11]. Available from: https://register.awmf.org/de/leitlinien/detail/001-025