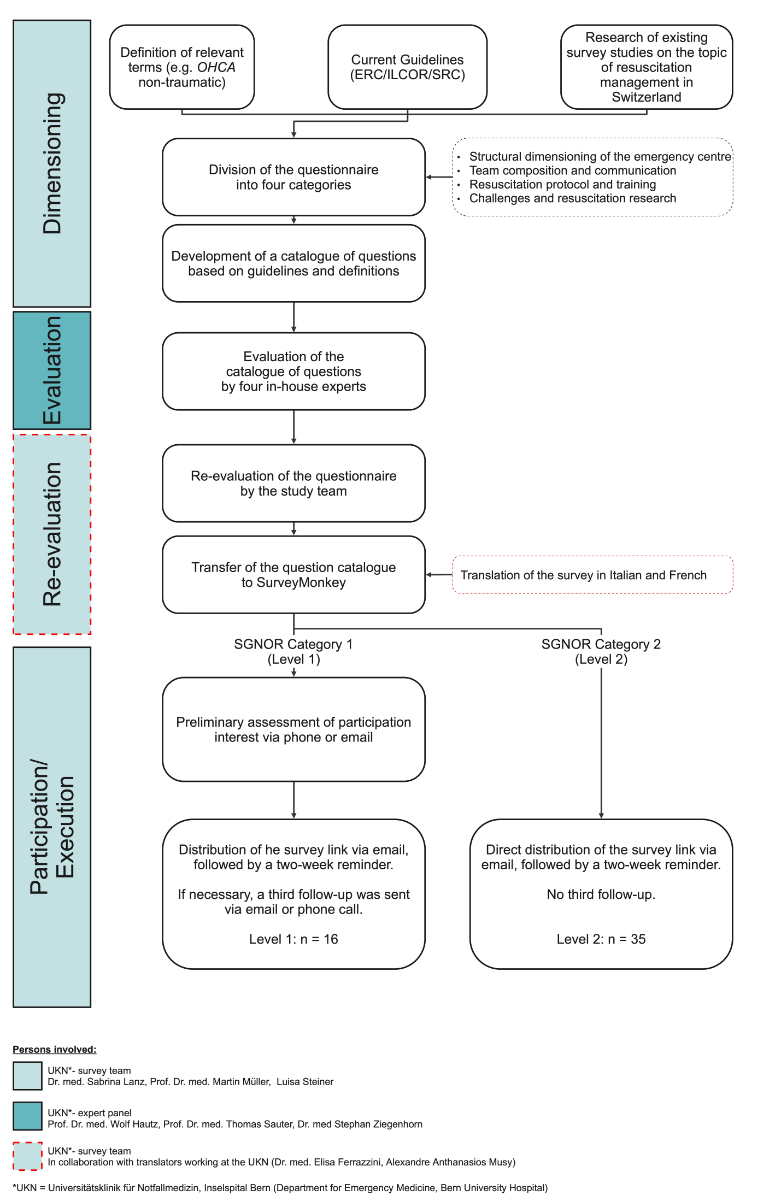
Figure 1Development of the clinical resuscitation management survey.
DOI: https://doi.org/https://doi.org/10.57187/4645
Advanced Cardiac Life Support
American Heart Association
Basic Life Support
CPR: Cardio-Pulmonary Resuscitation
Crisis Resource Management
Extra-Corporeal Membrane Oxygenation
European Resuscitation Council
International Liaison Committee on Resuscitation
Out-of-Hospital Cardiac Arrest
Return Of Spontaneous Circulation
Schweizerische Gesellschaft für Notfall- und Rettungsmedizin (Swiss Society for Emergency and Rescue Medicine)
Standard Operating Procedure
Swiss Resuscitation Council
Effective cardiopulmonary resuscitation (CPR) management is essential for the survival of out-of-hospital cardiac arrest (OHCA) patients as optimising resuscitation quality complements prevention strategies to reduce mortality [1]. The chain of survival, particularly the clinical aspects of CPR management, represents the most actionable area for improving survival rates with favourable neurological outcomes [2]. The Utstein formula of survival with its three components (1) educational efficiency, (2) medical science and (3) local implementation builds the foundation of research in CPR management [3].
Educational efficiency is critical for improving survival rates among patients experiencing OHCA. The American Heart Association (AHA) guidelines on CPR and emergency cardiovascular care highlight the importance of effective training in enhancing both provider performance and patient outcomes [4]. In the European context, ACLS certification generally refers to the Advanced Life Support (ALS) certification provided by the European Resuscitation Council (ERC) [5] rather than the American Heart Association (AHA) ACLS programme [6]. As a foundational step, it is necessary to conduct an evaluation of the training resources and methodologies employed across Swiss emergency centres. Such an analysis would facilitate the identification of existing gaps and inform the development of standardised, evidence-based training protocols.
The quality assurance of CPR management is enhanced through advancements in medical science such as technical procedures like extracorporeal membrane oxygenation (ECMO) [7–10] or vector-change defibrillation [11]. However, a systematic evaluation of current practices in Switzerland and their alignment with the latest evidence has yet to be conducted. Furthermore, the interplay between individual elements of CPR management remains underexplored.
To generate solid data on CPR management and increase knowledge about local implementation, continuous measurement of resuscitation quality and patient outcomes is required [2].
Currently there is a prehospital resuscitation data registry in Switzerland: SWISSRECA. All emergency medical services (EMS) are obliged to enter their data into the SWISSRECA data registry. However, in-hospital and follow-up data remain incomplete, since data registration is not mandatory for Swiss emergency centres [12]. It is therefore crucial to evaluate their current registration methods and identify opportunities for standardisation and implementation of locally tailored resuscitation guidelines.
To address the identified knowledge gaps in the three components of the Utstein formula of survival, we conducted a nationwide survey on CPR management in Swiss level 1 [13] and 2 [14] emergency centres.
This web-based cross-sectional survey incorporates all three factors of the Utstein formula for survival and was developed according to the CROSS reporting criteria [15]. It underwent a single round of Delphi consultation with an expert panel from the Department of Emergency Medicine at Bern University Hospital, Inselspital, in Bern, Switzerland. Experts were selected based on clinical experience in resuscitation, emergency medicine and medical education. Panel members reviewed the draft survey for relevance, clarity and completeness. Final modifications were made according to their consensus feedback. The complete process of survey development is shown in figure 1. The emergency medical services (EMS) system in Switzerland is comprehensively documented through the SWISSRECA registry. Consequently, this survey study prioritises the investigation of intra-hospital management strategies for OHCA patients, excluding EMS data from its scope.
Figure 1Development of the clinical resuscitation management survey.
The CPR survey comprised 27 questions organised into four categories and referred to the year 2022: i) characteristics of the emergency centre, ii) team and communication, iii) CPR protocol and training, and iv) challenges and resuscitation research. The survey included questions on ACLS certification requirements to assess standardisation across emergency centres. To capture all different certification practices, the survey included an open answer field for respondents to specify other requirements beyond formal ACLS/ALS certification. This distinction is important when interpreting survey results, as terminology varies between regions. The full survey is shown in appendix 1.
The survey was translated into the three most spoken national languages in Switzerland – German, French and Italian [16] – allowing each representative to choose their preferred language when completing it.
For this study, Swiss Society for Emergency and Rescue Medicine (SGNOR) category 1 (n = 16) and 2 (n = 35) training centres were defined as level 1 and level 2 emergency centres, respectively, and the survey was completed by representatives from each centre. Requirements for an SGNOR category 1 emergency training centre comprise 24-hour availability of anaesthesiology, bronchoscopy, interventional radiology and cardiology services as well as stroke centre certification. In contrast, SGNOR category 2 emergency training centres are required to provide extended standard emergency care, including intensive and intermediate care units, but do not offer the specialised treatment options available in category 1 centres [17]. Level 1 emergency centres were selected assuming a high rate of allocation of OHCA cases related to the availability of labour resources and advanced treatment options. Additionally, level 2 emergency centres were included in the survey to reflect broader clinical practice and establish a comparison of CPR management.
The survey was sent to all level 1 and level 2 emergency centres via e-mail, containing the survey link through SurveyMonkey, followed by a two-week reminder. For level 1 centres, a preliminary assessment of participation interest was conducted via phone or e-mail before distributing the survey. If necessary, a third follow-up was sent to level 1 centres via e-mail or phone to increase the response rate. Each emergency centre designated one doctor to complete the survey by retrieving the hospital’s internal data. However, no additional details about the respondents, such as their level of training or professional experience, were collected.
This study followed open-science principles for survey research. As it was a descriptive nationwide survey without patient-level data, no formal registration in a public registry was required. The complete questionnaire, including all survey items, is provided in appendix 1. No protocol deviations occurred during the study.
Given the limited number of participating centres, the survey was analysed descriptively, without conducting inferential statistical analyses. Quantitative responses are presented as means, with standard deviations (SD) provided in brackets. Variables with skewed distributions (e.g. number of OHCA cases per year) are reported as medians with interquartile ranges (IQR). Figures were created using Stata/MP 18.0 for Mac (Apple Silicon).The map of Switzerland was generated using the geoplot command [18], with geographical data sourced from the Swiss Federal Statistical Office [19].
The study was performed in accordance with Swiss law. There was no need for an ethical review for this survey study.
The survey response rate was 94% (15/16) for level 1 and 28% (10/36) for level 2 emergency centres. Table 1 summarises the structural and organisational characteristics of the participating emergency centres. Level 1 centres reported a mean of 31.6 (SD: 9.7) treatment bays compared to 14.3 (SD: 6.0) in level 2 centres. The annual patient volume was more than twice as high in Level 1 centres. Data availability and quality varied considerably, with 40% of Level 1 and 60% of Level 2 centres lacking a structured OHCA database. Research activity was reported in 20% of Level 1 centres, while 93% of them expressed interest in future collaboration (table 1).
Table 1OHCA management infrastructure and research activity in Swiss emergency centres. Percentages refer to all responding centres within each level (Level 1, n = 15; Level 2, n = 10). Variables with skewed distributions (annual OHCA cases and patients arriving under ongoing CPR) are presented as median with interquartile range (IQR).
| Level 1 EC (n = 15) | Level 2 EC (n = 10) | ||
| Infrastructure | Mean number of treatment bays (SD); range. | 31.6 (9.7); 19–50 | 14.3 (6.0); 6–25 |
| Mean annual patient volume (SD); range. | 49,867 (19,272); 24,000–100,000 | 19,600 (10,783); 8000–35,000 | |
| OHCA caseload | OHCA cases in 2022: Median (IQR); range. | 133 (IQR: 63–161); 27–580 | 6.5 (IQR: 4–19); 0–50 |
| Patients arriving under ongoing CPR in 2022: Median (IQR); range. | 28 (IQR: 20–75); 7–305 | 3.5 (IQR: 2–10); 0–30 | |
| Data availability & quality | Centres without structured OHCA database | 40%* | 60%* |
| Centres with structured OHCA database | 60%* | 40%* | |
| German CPR registry | 7%* | 0%* | |
| Hospital-developed database | 20%* | 10%* | |
| SWISSRECA database used | 13%* | 0%* | |
| COPRA patient data management system | 13%* | 0%* | |
| Retrospective case-counting post-survey | 7%* | 20%* | |
| Data from previous research project | 0%* | 10%* | |
| Research engagement & interest | EC actively conducting resuscitation research | 20%* | 0%* |
| EC with interest in future research projects | 93%* | 50%* | |
| Conditions required for future collaboration | Ethical approval, sufficient funding, institutional relevance. | Small-scale studies due to limited resources and personnel availability. | |
* Multiple answers were possible for registry use so totals may exceed 100%.
COPRA: Computer-based Patient Record and Analysis system; CPR: cardiopulmonary resuscitation; EC: emergency centre; IQR: interquartile range; OHCA: out-of-hospital cardiac arrest; SD: standard deviation; SWISSRECA: Swiss Registry of Cardiac Arrest.
Figure 2 illustrates the distribution of emergency centres across Switzerland, along with their survey participation and reported number of OHCA cases treated in 2022.
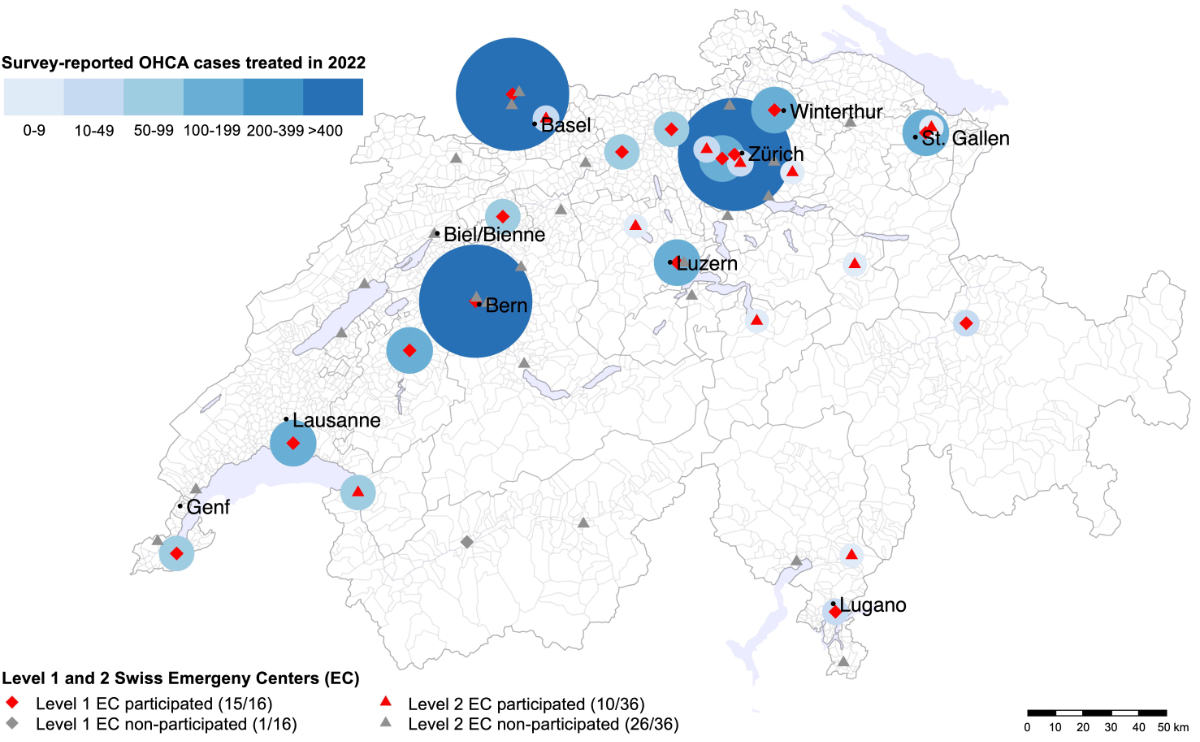
Figure 2Geographical distribution of participating and non-participating emergency centres and survey-reported OHCA cases treated in 2022 (the size and colour of the circles around a centre correspond to the number of cases).
The main barriers to effective OHCA management differed between Levels, but several themes were consistent across institutions. Leadership challenges in Level 1 centres were primarily related to managing multidisciplinary teams, whereas Level 2 centres reported staff shortages and coordination difficulties. Shared challenges included maintaining training continuity and protocol adherence despite rotating staffing (table 2).
Table 2Key challenges in local implementation and standardisation of resuscitation management in Swiss emergency centres. Responses were summarised qualitatively and grouped thematically according to the most frequently reported challenges. Each theme includes representative examples provided by emergency centres (ECs) of both Levels. Multiple responses per centre were possible.
| Challenge | Level 1 EC (n = 15) | Level 2 EC (n = 10) | Shared and General Challenges |
| Leadership & Coordination | Managing diverse, multidisciplinary teams with variable experience levels | Coordination difficulties due to limited personnel and constrained resources | Ensuring leadership continuity throughout resuscitation |
| Training & Education | Variability in staff qualifications and training frequency | Limited access to structured training due to staff turnover | Maintaining regular resuscitation training despite rotating staff |
| Resources & Staffing | Sufficient but unevenly distributed expertise | Overall shortage of staff and limited resources for continuous improvement | Frequent staffing changes hinder consistent training and protocol adherence |
| Standardisation & Protocols | Difficulties implementing uniform procedures across shifts | Adapting standardised protocols to local resource constraints | Ensuring protocol compliance amid alternating personnel |
Simulation-based training was conducted in almost all centres, with ACLS certification being mandatory in 73% of Level 1 but only 20% of Level 2 centres. Table 3 details the scope of ACLS certification requirements and outlines team composition, communication strategies and debriefing practices. Structured debriefing frameworks were reported in 33% of Level 1 and 40% of Level 2 centres (table 3).
Table 3Training, team composition and resuscitation protocols. The denominator used for percentages is the number of responding centres of each Level (15 for Level 1, 10 for Level 2). Percentages below 10% are rounded to one decimal for clarity. Multiple answers were possible for handover methods so totals may exceed 100%.
| Level 1 EC (n = 15) | Level 2 EC (n = 10) | ||
| Training and certification | Simulation-based resuscitation training conducted | 87% | 100% |
| ACLS certification mandatory | 73% | 20% | |
| ACLS required for all team members | 53% | 0% | |
| ACLS required for senior physician and higher ranks | 13% | 20% | |
| ACLS required for all permanent emergency bay staff | 7% | 0% | |
| Biennial ACLS refresher mandatory | 45% (of those with mandatory ACLS) | 100% (of those with mandatory ACLS) | |
| Team composition | Team size (day shift): mean (SD); range. | 7.4 (1.7); 5–10 | 7.3 (1.6); 5–10 |
| Team size (night shift): mean (SD); range. | 6.9 (1.9); 5–10 | 5.2 (1.0); 4–7 | |
| Nº of specialties per team: mean (SD). | 4.2 (1.4) | 3.5 (1.3) | |
| Common medical specialisations | EM: 87%, Anaesth: 80%, ICM: 27%, IM: 27% | EM: 80%, Anaesth: 60%, Cardio: 10%, ICM: 10% | |
| Leadership | Primary leadership specialisation | EM: 60% | EM: 50% |
| Dual specialisation leadership (EM + Anaesth) | 20% | 20% | |
| Other single specialties | IM: 7%, ICM: 7% | Anaesth: 10%, IM: 10% | |
| Leadership rotation by shift* | 0% | 10% | |
| Communication and handover strategies | Structured handover process present | 67% | 50% |
| … cABCDE | 67% | 50% | |
| … SAMPLE | 47% | 50% | |
| … SBAR | 27% | 20% | |
| … ATMIST | 13% | 10% | |
| No formal handover protocol | 7% | 10% | |
| Debriefing practices | EC with structured debriefing concept | 33% | 40% |
| … CRM-based debriefing | 13% | 0% | |
| … Hot-debriefing model# | 7% | 0% | |
| … STOP debriefing model | 7% | 0% | |
| … PEARLS debriefing model | 0% | 10% | |
| Institutionally developed debriefing framework | 0% | 10% | |
| Debriefing integrated into resuscitation protocol | 0% | 10% | |
| Leadership-dependent debriefing | 0% | 10% | |
| Debriefing framework in development | 7% | 0% | |
* Day shift: EM; Night shift: Anaesth or IM. Hot-debriefing: Immediate feedback round after resuscitation.
ACLS: Advanced Cardiac Life Support; Anaesth: Anaesthesia; ATMIST: Age Time Mechanism Injuries Symptoms Treatment; cABCDE: critical bleeding Airway Breathing Circulation Disability Environment; Cardio: Cardiology; CRM: Crisis Resource Management; EM: Emergency Medicine; ICM: Intensive Care Medicine; IM: Internal Medicine; PEARLS: Promoting Excellence and Reflective Learning in Simulation; SAMPLE: Symptoms Allergies Medication Last Oral Intake Exposure; SBAR: Situation Background Assessments Recommendation; STOP: Summarise Things that went well Opportunities to improve Points to action and responsibilities.
A notable trend was observed in centres with higher OHCA case volumes, which reported lower overall debriefing rates. However, debriefing frequency differed across institutions, with 70% of Level 2 centres reporting debriefing rates above 25%, and 20% conducting debriefings after every resuscitation (figure 3).
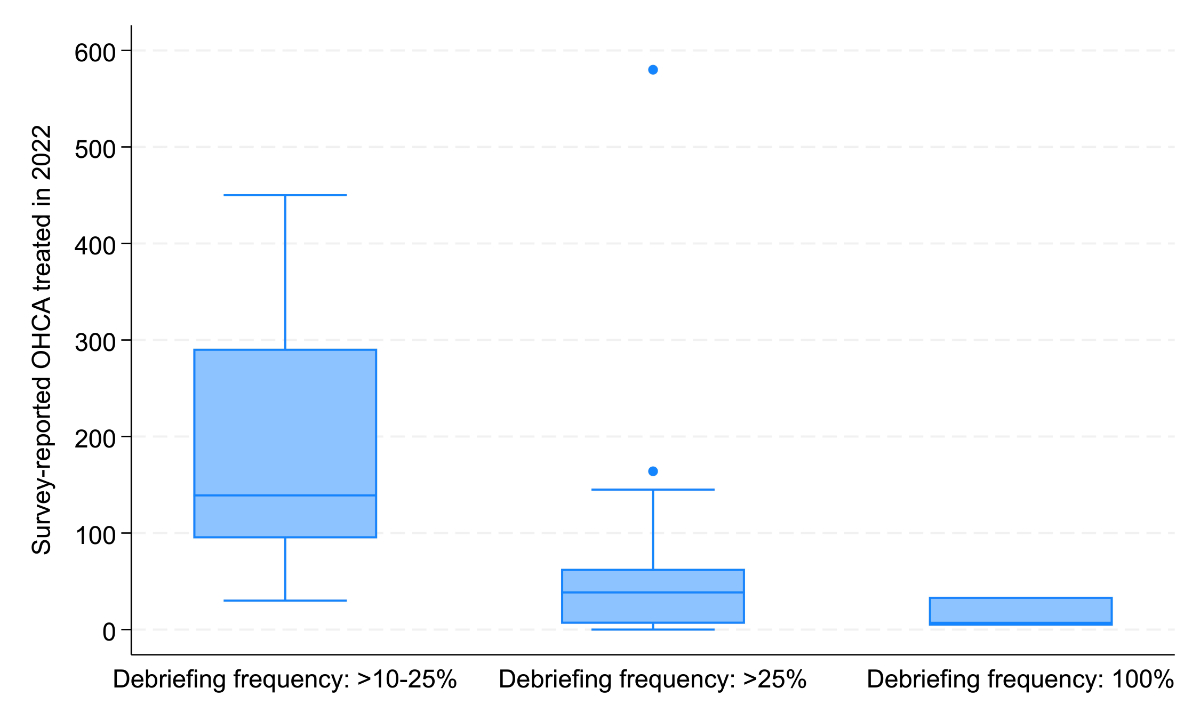
Figure 3Box plot diagram of survey-reported OHCA cases treated in 2022 stratified by debriefing frequency (10–25%, >25%, 100%).Boxes show interquartile range (IQR), the horizontal line indicates the median, whiskers denote 1.5 x IQR and dots represent outliers.
Table 4 provides an overview of technical and procedural resources available across emergency centres. Most Level 1 centres (73%) had a written standard operating procedure (SOP) for resuscitation, compared with 80% of Level 2 centres. Mechanical chest compression devices were available in 80% of Level 1 and 30% of Level 2 centres, with the LUCAS device being most frequently used. ECMO capability was reported by 73% of Level 1 centres and 10% of Level 2 centres.
Table 4Clinical and technical resources for OHCA management in Swiss emergency centres. The denominator used for percentages is the number of responding centres of each Level (15 for Level 1, 10 for Level 2). The table summarises clinical management strategies and availability of technical resources related to out-of-hospital cardiac arrest (OHCA) care in Swiss emergency centres. Reported difficulty values reflect institutional self-assessment based on current practices and infrastructure.
| Level 1 EC (n = 15) | Level 2 EC (n = 10) | ||
| Resuscitation protocol | SOP for resuscitation available | 73% | 80% |
| Primary reference sources for SOP | Resuscitation guidelines, EM congresses | Resuscitation guidelines, EM congresses | |
| Authorised representative for SOP updates | 53% | 50% | |
| In-house ACLS-certified expert managing SOP | 13% | 0% | |
| Mechanical chest compression devices | Device available | 80% | 30% |
| Most frequently used device | LUCAS (47%) | LUCAS (30%) | |
| Other devices used | AutoPulse (27%), Corpuls (7%) | AutoPulse (10%) | |
| Use only in specific scenarios* | 13% | ||
| Extracorporeal Membrane Oxygenation | ECMO insertion capability | 73% | 10% |
| Written SOP for ECMO decision-making | 67% | 10% | |
| Defibrillation strategies | Integration of DSD and/or VCD concepts | 47% | 40% |
| Focus on ventilation optimisation | 7% | 0% | |
| Challenges in medical decision-making | Key difficulties identified | TOR decisions, interdisciplinary communication, cause and prognosis assessment, post-resuscitation phase. | TOR decisions, interdisciplinary communication, cause and prognosis assessment, post-resuscitation phase. |
* Scenarios e.g. prolonged CPR, hypothermia. # Isolated initiative in one centre. ACLS: Advanced Cardiovascular Life Support; CPR: Cardiopulmonary Resuscitation; DSD: Double Sequential Defibrillation; ECMO: Extracorporeal Membrane Oxygenation; EM: Emergency Medicine; SOP: Standard Operating Procedure; TOR: Termination of Resuscitation; VCD: Vector-Change Defibrillation.
This survey is the first to detail CPR management in Swiss emergency centres, identifying system gaps and practice variation. The results revealed substantial variability in resuscitation training, team structures, communication strategies, protocol adherence and data collection across emergency centres. Advanced measures such as ECMO and mechanical chest compression devices are primarily available in Level 1 centres, whereas Level 2 centres report more frequent staff shortages and coordination challenges. These differences depict the heterogeneity in organisational structures, resource allocation and educational practices, indicating a need for standardised national strategies in CPR management. To better interpret the implications of these findings and to identify opportunities for optimisation, the following discussion will explore the key aspects of CPR management in Swiss emergency centres, highlighting strengths, gaps and potential areas for improvement.
The SWISSRECA registry provides essential prehospital OHCA data in Switzerland, maintained through mandatory reporting by certified EMS providers [16]. However, hospital-based and outcome data are incomplete, with inconsistent participation by emergency centres. This study found that 47% of Level 1 and 80% of Level 2 centres lack structured OHCA databases, often relying on retrospective counts or estimations.
This highlights the need for an integrated system linking prehospital, in-hospital and outcome data. Although SWISSRECA contributes to the EuReCa THREE study led by the ERC [20–22], the registry currently covers only the prehospital phase. Without standardised hospital-level documentation, national resuscitation data remain fragmented, limiting benchmarking and quality improvement [23]. A standardised OHCA data registration system across all hospitals and emergency services could identify disparities of outcomes based on demographics [24], enable benchmarking and ultimately improve patient outcomes. Germany’s German Cardiac Arrest Registry (G-CAR) could serve as a useful model as it prospectively integrates all phases of OHCA care and links them to certified Cardiac Arrest Centres (CAC) [25, 26]. CAC certification mandates the availability of ECMO and therefore improves neurological outcomes, although current evidence shows no significant increase in survival to discharge after CAC certification [27, 28]. These findings indicate a need for further research in Switzerland, particularly in relation to regional variability in OHCA outcomes.
Beyond data registration, a standardised protocol – mandatory in CAC-certified centres – could improve both educational efficiency and patient outcomes. Bern University Hospital exemplifies how structured SOPs provide a framework for standardised decision-making (appendix 2). Regular feedback loops and inter-institutional benchmarking, as emphasised in the Utstein formula of survival, would be crucial for optimising OHCA management in Switzerland.
Lower reported OHCA numbers in Western Switzerland may be due to stricter termination-of-resuscitation (TOR) protocols. Emergency physicians dispatched to suspected OHCA cases may decide against initiating or continuing resuscitation based on futility, leading to more selective transport strategies [29–31].
Another contextual factor is the demography of some urban regions in Western Switzerland, where a younger population might contribute to a lower overall incidence of OHCA [32]. Finally, variation in documentation practices – especially in centres without databases – may also influence reported case numbers.
The survey examined whether OHCA patients arrived with Return Of Spontaneous Circulation (ROSC) or under ongoing CPR. A higher proportion of patients arrived under CPR in Level 2 centres, raising questions about prehospital triage and alignment with hospital resources. While Level 1 centres treat more OHCA cases and offer advanced therapies like ECMO, current routing does not always reflect this capacity. A centralised triage approach could improve outcomes by directing refractory OHCA cases to high-volume centres with ECMO availability.
A meta-analysis showed that CPR quality during transport is more critical than transport itself, with no survival or neurological benefit for immediate transport compared with on-scene resuscitation [33]. Data from Bern University Hospital showed higher mortality in patients transported under CPR (69.8%) than in those with ROSC (5.7%). Within the ROSC group, age and female sex were associated with worse outcomes [34]. Differences may reflect varying cardiac-arrest circumstances and hospital management strategies, as suggested by the Targeted Temperature Management study [35]. Although patient outcome data were not collected in this survey, external findings highlight the relevance of prehospital decision-making. International Liaison Committee on Resuscitation (ILCOR) consensus papers from 2020 and 2022 recommend on-scene CPR over transport CPR unless ECMO is available, as CPR quality deteriorates in transit and increases paramedic injury risk [36, 37].
These findings highlight the importance of aligning transport destinations with available hospital resources. Despite 73% of Level 1 centres offering ECMO compared with only 10% of Level 2 centres, more patients were transported under CPR to the latter. Evidence from SAVE-J III (Japan) [38] and Tonna et al. [39] shows that higher ECMO case volumes correlate with better survival and fewer complications. Implementing structured triage protocols could ensure that eligible patients are routed to adequately equipped centres. Further research should evaluate existing triage pathways and regional variability in transport decisions.
Debriefing practices after resuscitation varied considerably across centres, and only a few used structured models such as CRM, STOP or PEARLS. While CRM training has shown benefits in team communication during crises, there is limited research evaluating STOP or PEARLS models specifically [40, 41]. Nonetheless, a structured debriefing is consistently associated with better teamwork, leadership and patient safety [42]. Virtual reality-based training may further enhance learning through immersive, reproducible and engaging feedback sessions [43].
Interestingly, centres with fewer OHCA cases conducted debriefings more frequently, possibly to compensate for limited exposure and to strengthen team reflection. In high-volume centres, targeted debriefings after critical cases may be more efficient, suggesting that debriefing strategies should be adapted to the institutional context [44].
Structured handovers represent another critical aspect of team communication. While most centres use a structured handover process, the methods differ. Many rely on cABCDE for clinical prioritisation, while tools like SBAR or ATMIST are less common. This may reflect a tendency to focus on clinical assessment rather than communication standardisation. However, standardised handover tools improve interdisciplinary coordination and reduce information loss during transitions [45, 46]. Simulation-based training could therefore strengthen consistency and efficiency across resuscitation teams.
According to the 2022 ILCOR consensus, mechanical chest compression devices should be considered for CPR during transport [37]. In this survey, 80% of Level 1 and 30% of Level 2 centres reported using such devices. Among Level 1 centres, 13% used them only for specific indications like hypothermia or prolonged resuscitation. These devices also serve to reduce workload and enhance safety in emergency settings.
Evidence on outcome benefits remains mixed. While adequate cerebral perfusion is associated with higher ROSC rates[47], a porcine model showed better circulation but no mortality benefit [48]. A meta-analysis found more CPR-related injuries under mechanical compression, though life-threatening events were comparable [49]. Thus, mechanical CPR seems most useful in transport or when manpower is limited, while manual CPR remains appropriate otherwise.
ECMO availability differed markedly, reported in 73% of Level 1 and 10% of Level 2 centres, with 93% of ECMO-capable centres having written SOPs.
The 2021 ERC guidelines support eCPR for specific cases, e.g. short downtime, high-quality prehospital CPR and shockable rhythms [49–51]. The Swiss Academy of Medical Sciences (SAMS) guidelines further highlight consideration of patient preferences [49], and the German S3 guidelines of 2021 recommend local, written SOPs [52]. The high adherence among Swiss centres indicates strong alignment with international standards.
The survey showed that Level 1 centres had an average team size of 7.4 (SD: 1.7) during the day shift and 6.9 (SD: 1.9) at night. In Level 2 centres, the night shift reduction was more pronounced, which may impact response time and decision-making in resuscitation.
However, increasing team size does not automatically enhance CPR effectiveness. A simulation study comparing 2-, 3- and 4-person paramedic crews found no significant differences in performance [53]. Most Level 1 centres had emergency medicine specialists leading resuscitation teams, ensuring consistent decision-making, whereas some Level 2 centres used a shift-dependent leadership model, potentially affecting coordination.
Leadership is a critical factor in team performance. Studies show that poor leadership behaviours negatively impact CPR quality [59,60]. Leaders adopting a “hands-off” approach – focusing on oversight rather than direct intervention – have been associated with improved team structure and cooperation during resuscitation [56]. Promoting such leadership behaviours and structured training may strengthen performance across emergency centres, regardless of the leader’s specialty background.
This study has some limitations. First, as an online survey, there was no control over who completed it at each emergency centre or how accurately the data were retrieved. Moreover, the survey format did not allow for clarification or follow-up questions. To address this, open-response fields were included to enable additional comments [57]. However, such fields also pose challenges – they are time-consuming and may result in data that are harder to interpret and less suitable for robust analysis [58]. Second, the Delphi consultation used to test the questionnaire involved a single-centre expert panel. This could have introduced institutional bias, as the reviewers may have been influenced by their own centre’s resuscitation practices. Involving a multicentre panel might have reduced this risk and improved objectivity [59]. Lastly, the more intensive follow-up process for Level 1 centres – through prior contact and multiple reminders – may have influenced participation rates and skewed the sample towards higher-volume institutions. However, given their greater experience with OHCA cases, this targeted approach may be justified to ensure that the study captured insights from the most relevant centres.
This study provides the first comprehensive assessment of CPR management in Swiss emergency centres, highlighting significant heterogeneity in CPR management and data collection. While resuscitation training and ACLS certification are widely implemented, their standardisation remains inconsistent, particularly in level 2 centres. Differences in team composition, leadership and communication strategies further emphasise the need for structured training programmes and clear protocols.
Despite the availability of ECMO and mechanical chest compression devices in some centres, allocation of OHCA patients under ongoing CPR or ROSC remains uneven, potentially affecting patient outcomes. Decision-making challenges related to termination of resuscitation, interdisciplinary coordination and post-resuscitation care persist, underscoring the importance of guideline development and training. A nationally standardised OHCA data registry is crucial for improving patient outcomes, enabling benchmarking and ensuring evidence-based optimisation of emergency care. The findings support efforts to align Swiss CPR management with international best practices and emphasise the need for further research and collaboration to enhance patient survival and neurological recovery.
The dataset supporting the conclusions of this study consists of aggregated, anonymised survey results and does not include any identifiable personal or institutional data. Deidentified data elements and the survey instrument are available from the corresponding author upon reasonable request for research purposes related to emergency medicine, resuscitation management or health services research. No data dictionary or additional documents will be publicly deposited, as the dataset contains information that could indirectly identify participating centres. Data will remain accessible for a period of five years after publication.
We would like to extend our gratitude to all participating SGNOR emergency centres for completing the survey. We thank Prof. Dr med. Wolf Hautz, Prof. Dr med. Thomas Sauter, Dr med. Stephan Ziegenhorn (all UKN) and PD Dr med. Jonas Lanz (Department of Cardiology, Inselspital) for the critical review of the survey. We also thank Dr med. Elisa Ferrazzini and Mr Alexandre Athanasios Musy for their assistance in translating the survey. Furthermore, we thank Mr André Willmes (Swiss Association of Rescue Services) for his insights into the SWISSRECA database.
Author contributions: Prof. Dr med. Martin Müller, Dr med. Sabrina Lanz and Luisa Steiner conceptualised the study and designed the methodology. Luisa Steiner collected data, managed data curation and prepared the original draft of the manuscript. Prof. Dr med. Martin Müller supervised the research process, while Prof. Dr med. Aristomenis Exadaktylos and Dr med. Beat Lehmann provided project supervision. Dr med. Manuela Iten provided Cardiac Arrest Centre SOP figures. All authors contributed to the revision of the manuscript and approved the final version.
This study received no external funding.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest related to the content of this manuscript was disclosed.
1. Myat A, Song KJ, Rea T. Out-of-hospital cardiac arrest: current concepts. Lancet. 2018 Mar;391(10124):970–9.
2. Baldi E, Contri E, Burkart R, Bywater D, Duschl M. The three dimension model of the out-of-hospital cardiac arrest. Resuscitation. 2019 May;138:44–5.
3. Perkins GD, Jacobs IG, Nadkarni VM, Berg RA, Bhanji F, Biarent D, et al.; Utstein Collaborators. Cardiac Arrest and Cardiopulmonary Resuscitation Outcome Reports: Update of the Utstein Resuscitation Registry Templates for Out-of-Hospital Cardiac Arrest: A Statement for Healthcare Professionals From a Task Force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Resuscitation. 2015 Nov;96:328–40.
4. Cheng A, Magid DJ, Auerbach M, Bhanji F, Bigham BL, Blewer AL, et al. Part 6: Resuscitation Education Science: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020 Oct;142 16_suppl_2:S551–79.
5. European Resuscitation Council. ERC Course Rules. Version 2022-08-24 European Resuscitation Council; 2022. Available from: https://www.erc.edu/assets/documents/ERC_Course_Rules_Version_20220824.pdf accessed March 10 2025.
6. American Heart Association. Advanced Cardiovascular Life Support Provider Manual. 2020 Dallas (TX): American Heart Association; 2020. Available from: https://ebooks.heart.org/product/acls-provider-manual-ebook-collection50044713 accessed March 10 2025.
7. Gandhi KD, Moras EC, Niroula S, Lopez PD, Aggarwal D, Bhatia K, et al. Left Ventricular Unloading With Impella Versus IABP in Patients With VA-ECMO: A Systematic Review and Meta-Analysis. Am J Cardiol. 2023 Dec;208:53–9.
8. Bhatia K, Jain V, Hendrickson MJ, Aggarwal D, Aguilar-Gallardo JS, Lopez PD, et al. Meta-Analysis Comparing Venoarterial Extracorporeal Membrane Oxygenation With or Without Impella in Patients With Cardiogenic Shock. Am J Cardiol. 2022 Oct;181:94–101.
9 Tonna JE, Abrams D, Brodie D, Greenwood JC, Rubio Mateo-Sidron JA, Usman A, et al. Management of Adult Patients Supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): Guideline from the Extracorporeal Life Support Organization (ELSO). ASAIO J Am Soc Artif Intern Organs 1992 2021;67:601–10. https://doi.org/.
10. Dalle Ave AL, Shaw DM, Gardiner D. Extracorporeal membrane oxygenation (ECMO) assisted cardiopulmonary resuscitation or uncontrolled donation after the circulatory determination of death following out-of-hospital refractory cardiac arrest-An ethical analysis of an unresolved clinical dilemma. Resuscitation. 2016 Nov;108:87–94.
11. Abuelazm MT, Ghanem A, Katamesh BE, Hassan AR, Abdalshafy H, Seri AR, et al. Defibrillation strategies for refractory ventricular fibrillation out-of-hospital cardiac arrest: A systematic review and network meta-analysis. Ann Noninvasive Electrocardiol. 2023 Sep;28(5):e13075.
12. Interverband für Rettungswesen (IVR). SWISSRECA Jahresbericht 2022 Aarau: IVR; 2022. Available from: https://www.144.ch/wp-content/uploads/2023/10/SWISSSRECA-Jahresbericht-2022.pdf accessed October 24th 2023. German
13. Schweizerische Gesellschaft für Notfall- und Rettungsmedizin (SGNOR). Weiterbildungsstätten klinische Notfallmedizin Kategorie 1 SGNOR; 2023. Available from: https://www.sgnor.ch/fileadmin/user_upload/ISP_KNM/Weiterbildungsstaetten_klinische_Notfallmedizin_SGNOR_kategorie1.pdf accessed October 20th 2023. German.
14. Schweizerische Gesellschaft für Notfall- und Rettungsmedizin (SGNOR). Weiterbildungsstätten klinische Notfallmedizin Kategorie 2 SGNOR; 2024. Available from: https://www.sgnor.ch/fileadmin/user_upload/ISP_KNM/Weiterbildungsstaetten_klinische_Notfallmedizin_SGNOR_kategorie2b.pdf accessed September 23rd 2024. German.
15. Sharma A, Minh Duc NT, Luu Lam Thang T, Nam NH, Ng SJ, Abbas KS, et al. A Consensus-Based Checklist for Reporting of Survey Studies (CROSS). J Gen Intern Med. 2021 Oct;36(10):3179–87.
16. Eidgenössisches Departement für auswärtige Angelegenheiten. About Switzerland: Sprachen cited 2025 Mar 10. Available from: https://www.aboutswitzerland.eda.admin.ch/de/sprachen
17. Schweizerische Gesellschaft für Notfall- und Rettungsmedizin (SGNOR). Anerkennung der Weiterbildungsstätte SGNOR; 2018. Available from: https://www.sgnor.ch/fileadmin/user_upload/knm_antrag_wb_staetten_2021_d.pdf accessed November 1st 2023. German.
18. Jann B. 2023. “GEOPLOT: Stata module to draw maps,” Statistical Software Components S459211, Boston College Department of Economics, revised 19 Sep 2024. n.d.
19. Federal Statistical Office (BFS). Basisgeometrien – Bundesamt für Statistik. Swiss Federal Statistical Office; cited 2025 Mar 6. Available from: Kartengeometrien ThemaKart - Set 2024 Kt n.d. https://www.bfs.admin.ch/asset/de/30566934 (accessed March 6, 2025).
20. Gräsner JT, Wnent J, Herlitz J, Perkins GD, Lefering R, Tjelmeland I, et al. Survival after out-of-hospital cardiac arrest in Europe - Results of the EuReCa TWO study. Resuscitation. 2020 Mar;148:218–26.
21. Gräsner JT, Lefering R, Koster RW, Masterson S, Böttiger BW, Herlitz J, et al.; EuReCa ONE Collaborators. EuReCa ONE-27 Nations, ONE Europe, ONE Registry: A prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe. Resuscitation. 2016 Aug;105:188–95.
22. Wnent J, Masterson S, Maurer H, Tjelmeland I, Herlitz J, Rosell Ortiz F, et al. European Registry of Cardiac Arrest - Study-THREE (EuReCa THREE) - An international, prospective, multi-centre, three-month survey of epidemiology, treatment and outcome of patients with out-of-hospital cardiac arrest in Europe - The study protocol. Resusc Plus. 2022 Oct;12:100314.
23. Suppan L, Burkart R; Swiss Resuscitation Council. Unrealistic expectations or hopeless actions: the importance of a comprehensive survival strategy to improve cardiac arrest outcomes. Resusc Plus. 2023 Jun;14:100408.
24. Uzendu A, Girotra S, Chan PS. What cardiac arrest registries can tell us about health differences and disparities. Resusc Plus. 2024 Mar;18:100614.
25. Pöss J, Sinning C, Schreiner I, Apfelbacher C, Drewitz KP, Hösler N, et al.; G-CAR Investigators. German Cardiac Arrest Registry: rationale and design of G-CAR. Clin Res Cardiol. 2023 Apr;112(4):455–63.
26. Pöss J, Sinning C, Roßberg M, Hösler N, Ouarrak T, Böttiger BW, et al.; G-CAR Investigators. German Cardiac Arrest Registry (G-CAR)-results of the pilot phase. Clin Res Cardiol. 2025 Oct;114(10):1270–9.
27. Rott N, Scholz KH, Busch HJ, Frey N, Kelm M, Thiele H, et al. Criteria for the certification of Cardiac Arrest Centers in Germany. Resuscitation. 2021 Dec;169:1–3.
28. Voß F, Thevathasan T, Scholz KH, Böttiger BW, Scheiber D, Kabiri P, et al. Accredited cardiac arrest centers facilitate eCPR and improve neurological outcome. Resuscitation. 2024 Jan;194:110069.
29. Morrison LJ, Verbeek PR, Zhan C, Kiss A, Allan KS. Validation of a universal prehospital termination of resuscitation clinical prediction rule for advanced and basic life support providers. Resuscitation. 2009 Mar;80(3):324–8.
30. Yates EJ, Schmidbauer S, Smyth AM, Ward M, Dorrian S, Siriwardena AN, et al. Out-of-hospital cardiac arrest termination of resuscitation with ongoing CPR: an observational study. Resuscitation. 2018 Sep;130:21–7.
31. Smits RL, Sødergren ST, van Schuppen H, Folke F, Ringh M, Jonsson M, et al. Termination of resuscitation in out-of-hospital cardiac arrest in women and men: an ESCAPE-NET project. Resuscitation. 2023 Apr;185:109721.
32. Swiss Federal Statistical Office. Demographic aging in Switzerland Internet. 2020 cited 2025 Apr 9. Available from: https://www.swissstats.bfs.admin.ch/data/webviewer/appId/ch.admin.bfs.swissstat/article/issue22014792000-10/package
33. Burns B, Hsu HR, Keech A, Huang Y, Tian DH, Coggins A, et al. Expedited transport versus continued on-scene resuscitation for refractory out-of-hospital cardiac arrest: A systematic review and meta-analysis. Resusc Plus. 2023 Oct;16:100482.
34. Sauter TC, Iten N, Schwab PR, Hautz WE, Ricklin ME, Exadaktylos AK. Out-of-hospital cardiac arrests in Switzerland: predictors for emergency department mortality in patients with ROSC or on-going CPR on admission to the emergency department. PLoS One. 2017 Nov;12(11):e0188180.
35. Winther-Jensen M, Kjaergaard J, Wanscher M, Nielsen N, Wetterslev J, Cronberg T, et al. No difference in mortality between men and women after out-of-hospital cardiac arrest. Resuscitation. 2015 Nov;96:78–84.
36. Summary E. International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. 2020;(d):
37. Wyckoff MH, Greif R, Morley PT, Ng KC, Olasveengen TM, Singletary EM, et al.; Collaborators. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Resuscitation. 2022 Dec;181:208–88.
38. Misumi K, Hagiwara Y, Kimura T, Hifumi T, Inoue A, Sakamoto T, et al.; SAVE-J II. study group. Impact of center volume on in-hospital mortality in adult patients with out‑of‑hospital cardiac arrest resuscitated using extracorporeal cardiopulmonary resuscitation: a secondary analysis of the SAVE-J II study. Sci Rep. 2024 Apr;14(1):8309.
39. Tonna JE, Selzman CH, Bartos JA, Presson AP, Ou Z, Jo Y, et al. The Association of Modifiable Postresuscitation Management and Annual Case Volume With Survival After Extracorporeal Cardiopulmonary Resuscitation. Crit Care Explor. 2022 Jul;4(7):e0733.
40. Jankouskas TS, Haidet KK, Hupcey JE, Kolanowski A, Murray WB. Targeted crisis resource management training improves performance among randomized nursing and medical students. Simul Healthc. 2011 Dec;6(6):316–26.
41. Petrosoniak A, Hicks CM. Beyond crisis resource management: new frontiers in human factors training for acute care medicine. Curr Opin Anaesthesiol. 2013 Dec;26(6):699–706.
42. Anderson TM, Secrest K, Krein SL, Schildhouse R, Guetterman TC, Harrod M, et al. Best Practices for Education and Training of Resuscitation Teams for In-Hospital Cardiac Arrest. Circ Cardiovasc Qual Outcomes. 2021 Dec;14(12):e008587.
43. Neher AN, Wespi R, Rapphold BD, Sauter TC, Kämmer JE, Birrenbach T. Interprofessional Team Training With Virtual Reality: Acceptance, Learning Outcome, and Feasibility Evaluation Study. JMIR Serious Games. 2024 Nov;12:e57117.
44. Toews AJ, Martin DE, Chernomas WM. Clinical debriefing: A concept analysis. J Clin Nurs. 2021 Jun;30(11-12):1491–501.
45. Lee DH, Lim EJ. Effect of a Simulation-Based Handover Education Program for Nursing Students: A Quasi-Experimental Design. Int J Environ Res Public Health. 2021 May;18(11):5821.
46. Müller M, Jürgens J, Redaèlli M, Klingberg K, Hautz WE, Stock S. Impact of the communication and patient hand-off tool SBAR on patient safety: a systematic review. BMJ Open. 2018 Aug;8(8):e022202.
47. Sanfilippo F, Serena G, Corredor C, Benedetto U, Maybauer MO, Al-Subaie N, et al. Cerebral oximetry and return of spontaneous circulation after cardiac arrest: A systematic review and meta-analysis. Resuscitation. 2015 Sep;94:67–72.
48. Magliocca A, Olivari D, De Giorgio D, Zani D, Manfredi M, Boccardo A, et al. LUCAS Versus Manual Chest Compression During Ambulance Transport: A Hemodynamic Study in a Porcine Model of Cardiac Arrest. J Am Heart Assoc. 2019 Jan;8(1):e011189.
49. Swiss Academy of Medical Sciences (SAMS). Medizin-ethische Richtlinien: Reanimationsentscheidungen SAMW; 2024. Available from: https://www.samw.ch cited March 3rd 2024. German.
50. Perkins GD, Graesner JT, Semeraro F, Olasveengen T, Soar J, Lott C, et al.; European Resuscitation Council Guideline Collaborators. European Resuscitation Council Guidelines 2021: executive summary. Resuscitation. 2021 Apr;161:1–60.
51. Hutin A, Abu-Habsa M, Burns B, Bernard S, Bellezzo J, Shinar Z, et al. Early ECPR for out-of-hospital cardiac arrest: best practice in 2018. Resuscitation. 2018 Sep;130:44–8.
52. Michels G, Wengenmayer T, Hagl C, Dohmen C, Böttiger BW, Bauersachs J, et al. Recommendations for extracorporeal cardiopulmonary resuscitation (eCPR): consensus statement of DGIIN, DGK, DGTHG, DGfK, DGNI, DGAI, DIVI and GRC. Clin Res Cardiol. 2019 May;108(5):455–64.
53. Martin-Gill C, Guyette FX, Rittenberger JC. Effect of crew size on objective measures of resuscitation for out-of-hospital cardiac arrest. Prehosp Emerg Care. 2010;14(2):229–34.
54. Rosenman ED, Branzetti JB, Fernandez R. Assessing Team Leadership in Emergency Medicine: The Milestones and Beyond. J Grad Med Educ. 2016 Jul;8(3):332–40.
55. Hunziker S, Johansson AC, Tschan F, Semmer NK, Rock L, Howell MD, et al. Teamwork and leadership in cardiopulmonary resuscitation. J Am Coll Cardiol. 2011 Jun;57(24):2381–8.
56. Kern P, Tschan F, Semmer NK, Marsch S. Effects of team leaders’ position in cardiopulmonary resuscitation teams on leadership behavior and team performance: A prospective randomized interventional cross-over simulation-based trial. Medicine (Baltimore). 2023 Jul;102(27):e34235.
57. Thomas SL, Pitt H, McCarthy S, Arnot G, Hennessy M. Methodological and practical guidance for designing and conducting online qualitative surveys in public health. Health Promot Int. 2024 Jun;39(3):daae061.
58. Zimba O, Gasparyan AY. Designing, Conducting, and Reporting Survey Studies: A Primer for Researchers. J Korean Med Sci. 2023 Dec;38(48):e403.
59. Winkler J, Moser R. Biases in future-oriented Delphi studies: A cognitive perspective. Technol Forecast Soc Change. 2016;105:63–76.
The appendix is available in the pdf version of the article at https://doi.org/10.57187/4645.