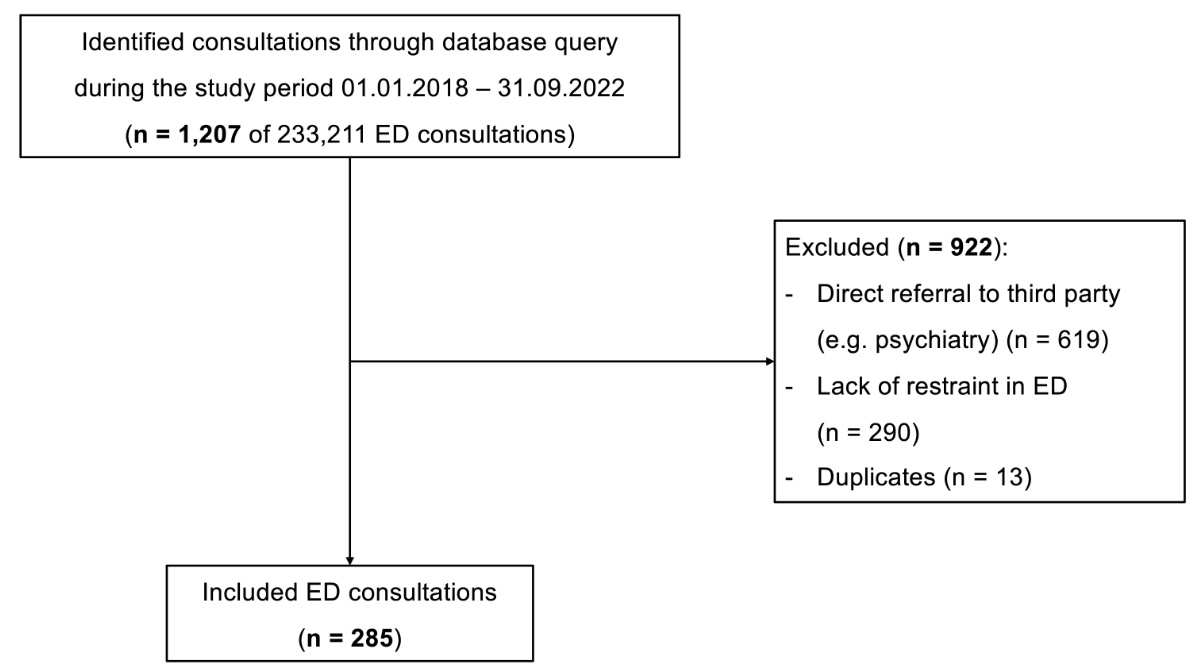
Study flowchart.
DOI: https://doi.org/https://doi.org/10.57187/4566
Coercive measures present an ongoing ethical dilemma for physicians. On the one hand, they conflict with the right to human dignity (Art. 7 of the Federal Constitution of the Swiss Confederation) and the right to personal liberty and physical freedom of movement (Art. 10 of the Federal Constitution of the Swiss Confederation) [1]. On the other hand, ensuring the safety of patients, staff and others in healthcare settings sometimes requires interventions that limit aggressive behaviour, including coercive measures. Each case requires careful individual assessment and prioritisation. The use of coercion can be traumatising for both patients and medical personnel [2]. Therefore, restraints should always be considered a measure of last resort to ensure safety [3, 4]. Due to this inherent ethical conflict, the application of coercive measures in the medical contexts is strictly regulated in Switzerland through various control mechanisms [2, 5, 6].
Although emergency department (ED) staff frequently encounter agitated patients requiring coercive measures, the literature on restraint use in EDs is scarce and often focused exclusively on patients with mental illness [7–10]. Moreover, data are inconsistently reported since “coercive measures” encompass a wide range of interventions, from observation and chemical seclusion to physical or mechanical restraint. Reported incidences vary considerably, ranging from 0.36% to 8.5% of all ED visits [11–15], whereas the 30-day prevalence of restraint use among hospitalised patients ranges from 8.7% to 11.8% [16, 17].
However, comparisons between studies remain difficult, due to differences in legislation, definitions and inclusion criteria.
The aims of the present study were: (1) to determine the incidence of mechanical restraint in a large Swiss university hospital ED, (2) to evaluate whether mechanical restraint is carried out more frequently and differently in specific patient groups (e.g. men vs women, younger vs older adults, and alcohol- vs no alcohol involvement), (3) to describe the triggers that led to aggression/agitation and the characteristics of mechanical restraint usage, particularly the medications used before and during restraint and, (4) to analyse temporal patterns, particularly the impact of the COVID-19 lockdown and pandemic on the number of mechanical restraints.
This study is reported according to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cohort studies to ensure comprehensive reporting [18].
The study was classified as a quality evaluation study by the Ethics Committee of the Canton of Bern, Switzerland. The need for informed consent was waived by the ethics committee (KEK-2019-00416).
This is a retrospective single-centre cohort study of emergency consultations in which patients were subjected to mechanical restraint due to aggressive or agitated behaviour.
The study was conducted between 1 January 2018 and 30 September 2022, in the adult ED of the University Hospital of Bern (Inselspital), a certified level 1 university-affiliated adult trauma centre. It has a catchment population of 1.8 million inhabitants, corresponding to around 20% of the Swiss population, with more than 50,000 emergency consultations each year.
According to the Swiss government, the COVID-19 mitigation period lasted from March 2020 to February 2022 [19].
The medical records of all ED consultations during the study period are stored in digital full text in the clinical database system, E-Care ED v2.1.3.0 (Mesalvo Turnhout BV, Turnhout, Belgium). This medical database enables access to previous diagnostic reports, consultations and other pertinent medical documents. Cases were identified through a comprehensive full-text search algorithm using specific search terms “fixation” (which is the commonly used term in German for restraint), “fix*” and “aggression”. The medical records obtained were extracted and assessed for eligibility, through manual full-text analysis by NH. All patients aged 16 years or older who presented to our ED during the specified period were included if they were initially assessed by an emergency physician (with psychiatric consultation upon request) and underwent mechanical restraint using a 5-point fixation bed for any reason (e.g. aggressive/agitated behaviour) during their ED stay. Patients were excluded if they did not undergo mechanical restraint or were directly assigned to the psychiatric emergency service. Direct referral to the psychiatric emergency service at our institution is determined by a triage nurse and is reserved for patients who do not require urgent pharmacological intervention (e.g. for seclusion), physical examination, laboratory testing, imaging studies and/or mechanical restraint.
Patients subjected to restraint more than once during the study period were listed as separate consultations. At the time of the study, a standard protocol for mechanical restraint was not yet operating at our ED.
Medical reports of the ED, existing preclinical reports and other ED documentation (e.g. nursing notes) were analysed. Data were systematically extracted using a predefined extraction sheet, developed prior and included standardised fields for the following variables:
Intoxication was defined as positive blood alcohol testing (breath alcohol ≥0.05‰, blood alcohol ≥0.62 G/L), positive toxicological urine sampling and/or history positive for current intoxication, and/or clinical judgement/diagnosis by the treating physician. For urine analysis, Quidel Triage® TOX Drug Screen, 94600 (QuidelOrtho Corporation, San Diego, CA, USA) was used.
The time of patient arrival was categorised based on the type of shift: day shift (07:30–14:00), late shift (14:00–22:30) or night shift (22:30–07:30).
The pre- and post-COVID-19 phases were defined by the beginning of the first lockdown from 1 March 2020 [20] until almost all measures were lifted in February 2022 [21]. Age was treated as a continuous variable for comparisons between two groups. For analysis of sex-specific alcohol consumption, age was additionally dichotomised into young adults (≤40 years) and older adults (>40 years), reflecting changes in physiological, sociocultural and risk behaviour around this age [22]. Furthermore, the duration of mechanical restraint and total ED time were treated as continuous variables.
A comprehensive keyword search was conducted to ensure the identification of all eligible patients and minimise the risk of selection bias. Beside the medical reports, preclinical reports and other digital information (e.g. nurse documentation) were screened to reduce information and reporting bias as far as possible.
No formal study size calculation was performed as all eligible patients up to six months after the COVID-19 restrictions were included.
Data analysis was performed using Stata® 18.1 (StataCorp, The College Station, TX, USA). All categorical variables are reported in percentages and absolute numbers. The distributions of continuous variables are described by the median and the interquartile range (IQR). The 95% confidence interval (CI) of the incidence was calculated for different time groups using Stata’s cii proportion command.
Comparisons of continuous variables between two groups (i.e. young vs older adults, women vs men) or among three/four groups (i.e. different COVID-19 mitigation phases and cause of mechanical restraint) were performed using the Wilcoxon rank-sum test or Kruskal–Wallis test, respectively. Categorical variables were compared by the chi-squared test. The significance level was set at an alpha of 0.01 to adjust for multiple testing.
A fractional-polynomial prediction plot with 95% CI was used to model the course of the absolute number of mechanical restraints per month/quarter over the study period and to describe the impact of COVID-19 mitigations on the course.
We estimated incidence rate ratios of mechanical restraints across the three COVID-19 mitigation phases (pre, during, post) using Poisson regression, with the total number of ED consultations as the exposure.
A study protocol was not prepared in advance. The analytical code can be made available upon reasonable request from the corresponding author.
During the study period, we included 26.6% (n = 285) of all identified consultations through keyword search in the study (figure 1). With 233,211 consultations at our ED during the specified study period, this resulted in an incidence of 1.22 (95% CI: 1.08–1.37) mechanical restraints per 1000 ED consultations.
Study flowchart.
Figure 1The monthly absolute numbers of mechanical restraints increased until the mid-2020, followed by a period of stabilisation then a slight decline over two years (figure 2).
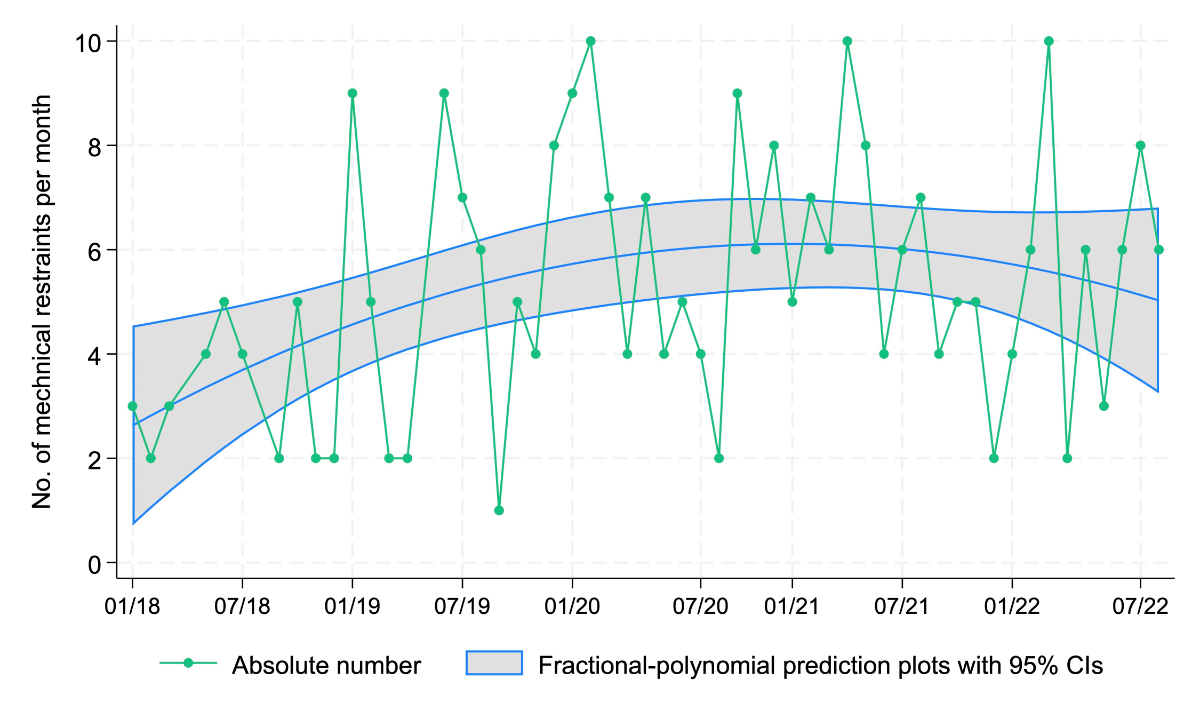
Figure 2Absolute number of restraints per month and year and a fractional-polynomial prediction plot with 95% CI over the course of the study, n = 285.
Most patients were men, young adults and of Swiss nationality, with a median age of 30 years (IQR: 23–41). The majority presented during late or night shifts, were brought in by ambulance or the police service, and had experienced preclinical mechanical restraint. In 62.8% of the consultations, restraint was required following intoxication, most commonly due to alcohol. More than half of the patients were mechanically restrained for ≥4 hours, corresponding to 79% of the total duration of ED stay. Only a minority of patients were discharged as outpatients.
Table 1Sociodemographic, mechanical restraint and consultation characteristics, with subgroup analysis for sex, age and alcohol involvement in 285 ED patients undergoing mechanical restraint.
| Variable | Total | Sex | p-value | Age | p-value | Alcohol involvement | p-value | |||
| Women | Men | ≤40y | >40y | No | Yes | |||||
| Sociodemographic | ||||||||||
| Sex | ||||||||||
| Women | 93 (32.6%) | 93 (100.0%) | 0 | 76 (35.7%) | 17 (23.6%) | 50 (43.5%) | 43 (25.3%) | |||
| Men | 192 (67.4%) | 0 | 192 (100%) | <0.001 | 137 (64.3%) | 55 (76.4%) | 0.059 | 65 (56.5%) | 127 (74.7%) | 0.001 |
| Age in years | 30 (23–41) | 28 (23–36) | 32 (25–43) | 0.035 | 27 (22–32) | 50 (45–58) | <0.001 | 29 (23–39) | 31 (24–42) | 0.287 |
| Nationality | ||||||||||
| Non-Swiss | 117 (41.1%) | 19 (20.4%) | 98 (51.0%) | 87 (40.8%) | 30 (41.7%) | 34 (29.6%) | 83 (48.8%) | |||
| Swiss | 168 (58.9%) | 74 (79.6%) | 94 (49.0%) | <0.001 | 126 (59.2%) | 42 (58.3%) | 0.902 | 81 (70.4%) | 87 (51.2%) | 0.001 |
| Consultation | ||||||||||
| Shift | ||||||||||
| Day shift | 43 (15.1%) | 13 (14.0%) | 30 (15.6%) | 0.716 | 29 (13.6%) | 14 (19.4%) | 0.232 | 25 (21.7%) | 18 (10.6%) | 0.010 |
| Late shift | 131 (46.0%) | 54 (58.1%) | 77 (40.1%) | 0.004 | 98 (46.0%) | 33 (45.8%) | 0.979 | 60 (52.2%) | 71 (41.8%) | 0.084 |
| Night shift | 111 (38.9%) | 26 (28.0%) | 85 (44.3%) | 0.008 | 86 (40.4%) | 25 (34.7%) | 0.395 | 30 (26.1%) | 81 (47.6%) | <0.001 |
| Overall | 0.012 | 0.437 | <0.001 | |||||||
| Discharge | ||||||||||
| Outpatient | 102 (35.8%) | 20 (21.5%) | 82 (42.7%) | <0.001 | 75 (35.2%) | 27 (37.5%) | 0.726 | 11 (9.6%) | 91 (53.5%) | <0.001 |
| Inpatient psychiatric | 117 (41.1%) | 59 (63.4%) | 58 (30.2%) | <0.001 | 82 (38.5%) | 35 (48.6%) | 0.132 | 66 (57.4%) | 51 (30.0%) | <0.001 |
| Inpatient medicine | 3 (1.1%) | 2 (2.2%) | 1 (0.5%) | 0.206 | 0 | 3 (4.2%) | 0.003 | 2 (1.7%) | 1 (0.6%) | 0.350 |
| Inpatient prison | 32 (11.2%) | 0 | 32 (16.7%) | <0.001 | 31 (14.6%) | 1 (1.4%) | 0.002 | 17 (14.8%) | 15 (8.8%) | 0.118 |
| Inpatient intensive care | 31 (10.9%) | 12 (12.9%) | 19 (9.9%) | 0.445 | 25 (11.7%) | 6 (8.3%) | 0.423 | 19 (16.5%) | 12 (7.1%) | 0.012 |
| Overall | <0.001 | 0.001 | <0.001 | |||||||
| Duration of treatment in min | 425 (278–577) | 370 (258–498) | 456 (282–623) | 0.019 | 417 (267–560) | 443 (308–676) | 0.064 | 320 (223–526) | 472 (348–603) | <0.001 |
| Mechanical restraint | ||||||||||
| Assignments | ||||||||||
| Police | 68 (23.9%) | 16 (17.2%) | 52 (27.1%) | 0.067 | 54 (25.4%) | 14 (19.4%) | 0.309 | 30 (26.1%) | 38 (22.4%) | 0.468 |
| Ambulance | 68 (23.9%) | 32 (34.4%) | 36 (18.8%) | 0.004 | 52 (24.4%) | 16 (22.2%) | 0.706 | 36 (31.3%) | 32 (18.8%) | 0.015 |
| Both | 146 (51.2%) | 43 (46.2%) | 103 (53.6%) | 0.241 | 104 (48.8%) | 42 (58.3%) | 0.163 | 47 (40.9%) | 99 (58.2%) | 0.004 |
| Self-briefing | 3 (1.1%) | 2 (2.2%) | 1 (0.5%) | 0.206 | 3 (1.4%) | 0 | 0.311 | 2 (1.7%) | 1 (0.6%) | 0.350 |
| Overall | 0.010 | 0.414 | 0.021 | |||||||
| Acute risk of harm to self or others | ||||||||||
| Self | 24 (8.4%) | 15 (16.1%) | 9 (4.7%) | 0.001 | 21 (9.9%) | 3 (4.2%) | 0.133 | 21 (18.3%) | 3 (1.8%) | <0.001 |
| Others | 179 (62.8%) | 49 (52.7%) | 130 (67.7%) | 0.014 | 133 (62.4%) | 46 (63.9%) | 0.826 | 54 (47.0%) | 125 (73.5%) | <0.001 |
| Both | 82 (28.8%) | 29 (31.2%) | 53 (27.6%) | 0.532 | 59 (27.7%) | 23 (31.9%) | 0.492 | 40 (34.8%) | 42 (24.7%) | 0.065 |
| Overall | 0.002 | 0.297 | <0.001 | |||||||
| Preclinical mechanical restraint | ||||||||||
| No | 55 (19.3%) | 28 (30.1%) | 27 (14.1%) | 0.001 | 41 (19.2%) | 14 (19.4%) | 0.971 | 30 (26.1%) | 25 (14.7%) | 0.017 |
| Yes | 156 (54.7%) | 41 (44.1%) | 115 (59.9%) | 0.012 | 117 (54.9%) | 39 (54.2%) | 0.910 | 57 (49.6%) | 99 (58.2%) | 0.149 |
| Unknown | 74 (26.0%) | 24 (25.8%) | 50 (26.0%) | 0.966 | 55 (25.8%) | 19 (26.4%) | 0.924 | 28 (24.3%) | 46 (27.1%) | 0.609 |
| Overall | 0.004 | 0.993 | 0.057 | |||||||
| Diagnosis | ||||||||||
| Alcohol | 101 (35.4%) | 28 (30.1%) | 73 (38.0%) | 0.190 | 63 (29.6%) | 38 (52.8%) | <0.001 | 0 | 101 (59.4%) | <0.001 |
| Drugs | 9 (3.2%) | 2 (2.2%) | 7 (3.6%) | 0.499 | 8 (3.8%) | 1 (1.4%) | 0.321 | 9 (7.8%) | 0 | <0.001 |
| Mixed | 69 (24.2%) | 15 (16.1%) | 54 (28.1%) | 0.027 | 60 (28.2%) | 9 (12.5%) | 0.007 | 0 | 69 (40.6%) | <0.001 |
| Psychiatric comorbidity | 79 (27.7%) | 40 (43.0%) | 39 (20.3%) | <0.001 | 68 (31.9%) | 11 (15.3%) | 0.006 | 79 (68.7%) | 0 | <0.001 |
| Other | 27 (9.5%) | 8 (8.6%) | 19 (9.9%) | 0.727 | 14 (6.6%) | 13 (18.1%) | 0.004 | 27 (23.5%) | 0 | <0.001 |
| Overall | 0.002 | <0.001 | <0.001 | |||||||
| Psychiatric comorbidity | ||||||||||
| None | 113 (39.6%) | 15 (16.1%) | 98 (51.0%) | <0.001 | 84 (39.4%) | 29 (40.3%) | 0.900 | 26 (22.6%) | 87 (51.2%) | <0.001 |
| Borderline, PTSD, personality disorder | 60 (21.1%) | 44 (47.3%) | 16 (8.3%) | <0.001 | 58 (27.2%) | 2 (2.8%) | <0.001 | 47 (40.9%) | 13 (7.6%) | <0.001 |
| Schizophrenia | 17 (6.0%) | 6 (6.5%) | 11 (5.7%) | 0.809 | 12 (5.6%) | 5 (6.9%) | 0.685 | 15 (13.0%) | 2 (1.2%) | <0.001 |
| Autism | 6 (2.1%) | 1 (1.1%) | 5 (2.6%) | 0.399 | 4 (1.9%) | 2 (2.8%) | 0.646 | 6 (5.2%) | 0 | 0.003 |
| Addiction | 89 (31.2%) | 27 (29.0%) | 62 (32.3%) | 0.578 | 55 (25.8%) | 34 (47.2%) | 0.001 | 21 (18.3%) | 68 (40.0%) | <0.001 |
| Overall | <0.001 | <0.001 | <0.001 | |||||||
| Duration of restraint in min | 258 (160–400) | 240 (149–341) | 284 (168–423) | 0.045 | 255 (148–400) | 262 (180–394) | 0.583 | 223 (121–329) | 291 (189–419) | 0.001 |
| % mechanical restraint during ED stay | 79 (43–100) | 79 (39–100) | 79 (45–100) | 0.971 | 82 (44–100) | 64 (39–100) | 0.097 | 100 (41–100) | 72 (43–100) | 0.015 |
ED: emergency department; PTSD: post-traumatic stress disorder. Notes: Continuous variables are described with median (interquartile range), while categorical variables are shown with number (%) in each category.
The most frequently used intra- and peri-restraint medications were benzodiazepines administered intravenously. Haloperidol, given either intravenously or intramuscularly, was also commonly used. Neither alcohol intoxication nor mixed intoxication influenced the choice of seclusion drug (see appendix).
Compared to men, women were generally younger, more likely to be Swiss nationals, more frequently presented during the late shift and arrived more often by ambulance, whereas men were more likely to present during the night shift. Women also had a higher incidence of psychiatric comorbidities and were more likely to undergo compulsory admission for acute risk of self-harm without concurrent risk of harm to others. Furthermore, women had fewer documented preclinical restraints.
Regarding discharge outcomes, women were more often admitted to psychiatric inpatient care, whereas men were more frequently discharged to inpatient prison.
The older age group (>40 years) demonstrated a higher incidence of alcohol-involved intoxications and addiction. In contrast, the younger age group (≤40 years) showed a higher prevalence of psychiatric disorders, particularly borderline, PTSD and other personality disorders, and were more frequently discharged to prison. No significant differences were found regarding intra-/peri-restraint drugs or other characteristics.
Besides identifying as men and non-Swiss nationality, alcohol-involvement presentations were significantly associated with acute risk of harm to others, night shift, addiction problems and longer mechanical restraint times as well as ED treatment duration and outpatient treatment.
Table 2Intra- and peri-restraint medication usage and routes of administration in 285 ED patients undergoing mechanical restraint.
| Intra- and peri-restraint drugs | Total | |
| Benzodiazepine | 223 (78.2%) | |
| Admission benzodiazepine | None | 62 (21.8%) |
| i.v. | 94 (33.0%) | |
| i.m. | 9 (3.2%) | |
| Nasal | 32 (11.2%) | |
| p.o. | 12 (4.2%) | |
| i.v. and nasal | 50 (17.5%) | |
| i.v. and sublingual | 11 (3.9%) | |
| i.m. and nasal | 2 (0.7%) | |
| i.m. and sublingual | 1 (0.4%) | |
| i.v. and i.m. | 4 (1.4%) | |
| Nasal and sublingual | 4 (1.4%) | |
| i.v., i.m. and sublingual | 1 (0.4%) | |
| i.v., i.m. and nasal | 2 (0.7%) | |
| i.v., p.o. and nasal | 1 (0.4%) | |
| Haloperidol | 135 (47.4%) | |
| Admission haloperidol | None | 150 (52.6%) |
| i.v. | 59 (20.7%) | |
| i.m. | 52 (18.2%) | |
| p.o. | 11 (3.9%) | |
| i.v. and sublingual | 1 (0.4%) | |
| i.m. and sublingual | 4 (1.4%) | |
| i.v. and i.m. | 8 (2.8%) | |
| Other medication | None | 242 (84.9%) |
| Morphine | 2 (0.7%) | |
| Quetiapine | 4 (1.4%) | |
| Ketamine | 3 (1.1%) | |
| Methadone | 1 (0.4%) | |
| Others | 33 (11.6%) | |
ED: emergency department; i.m.: intramuscular; i.v.: intravenous; p.o.: per os (oral). Notes: Categorical variables are shown with count (%) in each category.
Alcohol involvement was documented in 59.6% of restraint cases. Young men under the influence of alcohol (31.6%) constituted the largest subgroup, followed by young men without alcohol involvement (16.5%). Among cases involving alcohol, the men-to-women ratio was approximately 3:1 in young adults and 3.7:1 in older adults. In contrast, among cases without alcohol involvement, the corresponding ratios were lower (young adults 1:1, older adults 2.5:1).
Table 3Breakdown of subgroup sizes by alcohol involvement, age group and sex.
| Variables | Sex | ||
| Women | Men | ||
| Alcohol involvement | ≤40 years | 33 (19.4%) | 90 (52.9%) |
| >40 years | 10 (5.9%) | 37 (21.8%) | |
| No alcohol involvement | ≤40 years | 43 (37.4%) | 47 (40.9%) |
| >40 years | 7 (6.1%) | 18 (15.7%) | |
Categorical variables are shown with count (%) in each category.
The number of mechanical restraints followed a circadian pattern: 15.1% of the restraints took place during the day shift (07:30–14:00), 46% during the late shift (14:00–22:30) and 38.9% during the night shift (22:30–07:30 (figure 3).
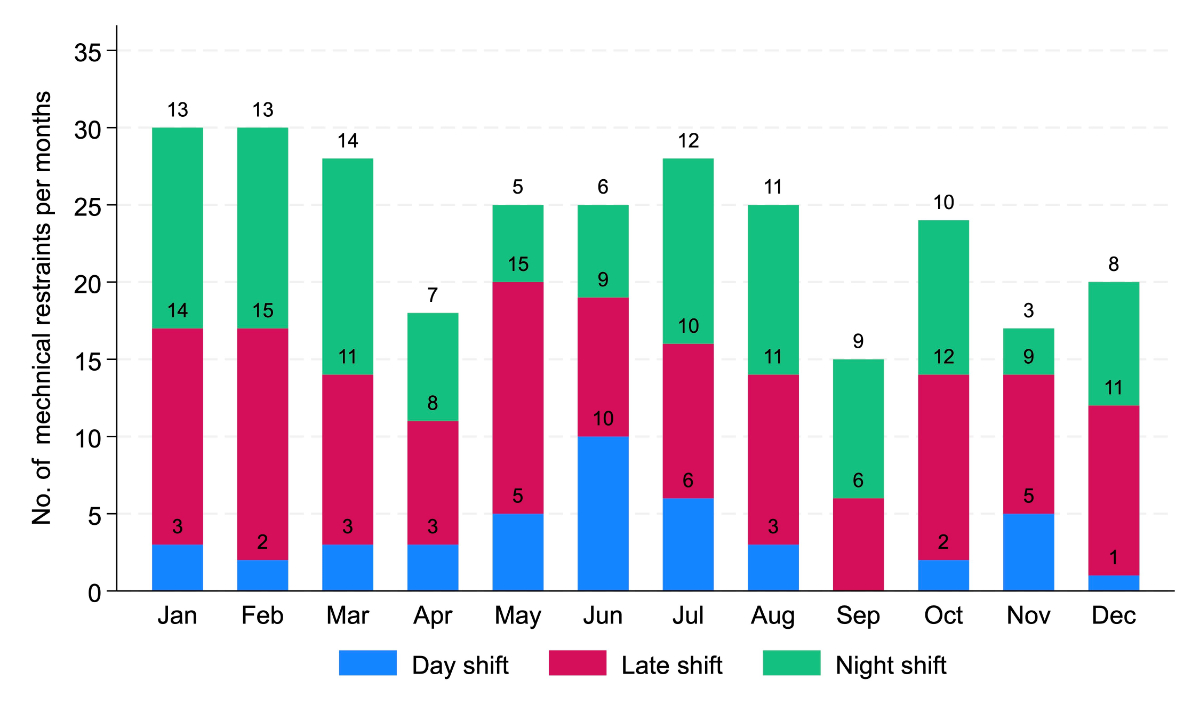
Figure 3Mechanical restraint distribution over shifts, n = 285.
Table 4Absolute numbers of patients and mechanical restraints, proportional incidence and incidence rate ratios in the three groups pre-, peri- and post-COVID-19 mitigations.
| N of ED patients | N of mechanical restraints | Proportional incidence (95% CI) per 1000 ED consultations* | IRR with 95% CI and p-value** | ||
| Pre | 107,091 | 109 | 1.02 (0.84–1.23) | 0.71 (0.55–0.91) | 0.008 |
| Peri | 94,196 | 135 | 1.43 (1.20–1.70) | 1.00 (Baseline) | – |
| Post | 31,934 | 41 | 1.28 (0.92–1.74) | 0.90 (0.63–1.27) | 0.537 |
| Total | 233,221 | 285 | 1.22 (1.08–1.37) | ||
* Obtained by Stata’s cii proportion command. ** Incidence Rate Ratios (IRR) with 95% CI and p-values were obtained by Poisson regression.
The incidence was higher during COVID-19 mitigations with 1.43 (95% CI: 1.20–1.70) mechanical restraints per 1000 ED consultations vs pre-COVID-19: 1.02 (95% CI: 0.84–1.23) per 1000 ED consultations; the incidence rate ratios differed significantly (p = 0.008). No significant differences (p = 0.205) were observed comparing the incidence rate ratio during and after COVID-19 mitigations with an incidence post-COVID-19 of 1.28 (95% CI: 0.92–1.74) per 1000 ED consultations.
The temporal trend of mechanical restraints in the ED is presented in figure 4.
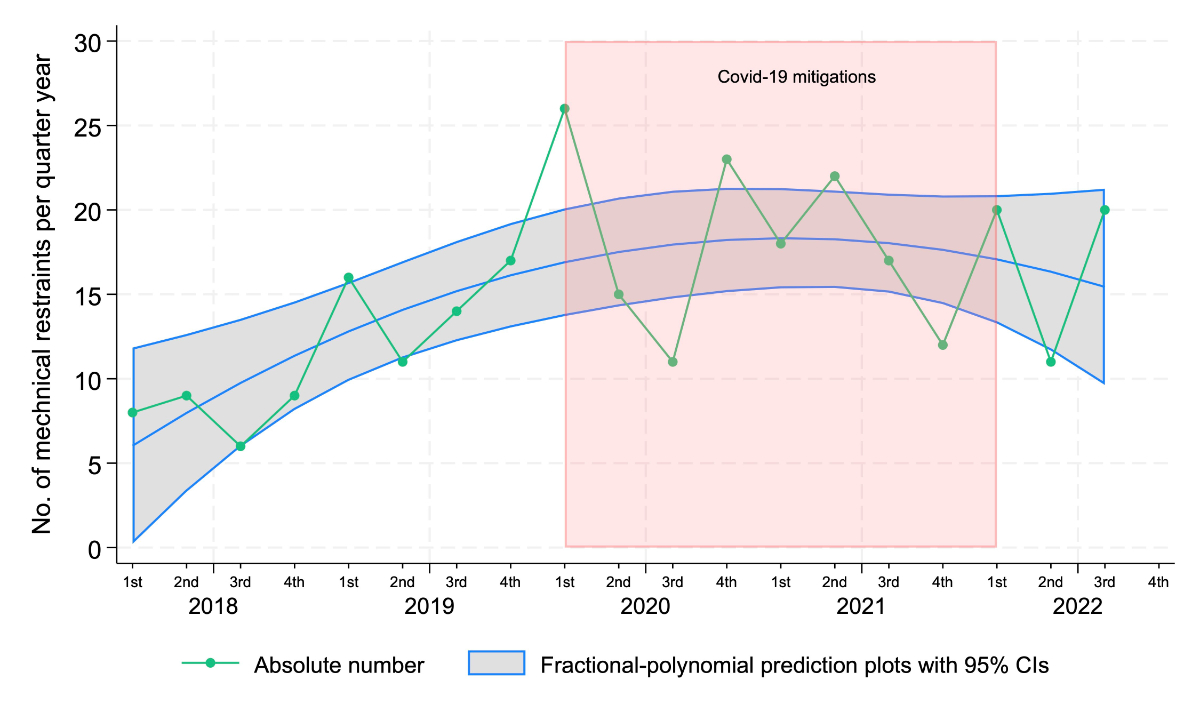
Figure 4Mechanical restraints per quarter and the impact of COVID-19 mitigations, n = 285.
Overall, the number of restraints per quarter showed a steady increase from 2018 to 2020, followed by more marked fluctuations during the COVID-19 mitigation period in 2020 and 2021. The absolute number of restraints rose progressively, peaking in the 2nd and 3rd quarters of 2020, during the early phases of the pandemic response.
The fractional-polynomial prediction plot with 95% CI showed a similar trend, with an increase in mechanical restraints up until 2020, followed by a stabilisation or slight decrease in the subsequent years.
The characteristics of the three subgroups (before, during and after the COVID-19 mitigations) are shown in supplement 4. There was a significant association with compulsory admission due to acute risk of self-harm and risk of harm to others, with the latter being more prevalent during (71.2%), respectively post (65.9%) COVID-19 mitigations compared to the pre-mitigation period (51.4%). Additionally, there were fewer concomitant risks of harm during (23%) and post (19.5%) COVID-19 mitigation period, compared to the pre-mitigation phase (39.4%). Furthermore, significantly fewer cases of borderline personality disorders, PTSD and other personality disorders were found during the post-COVID-19 mitigation phase (4.9%) compared to the during (20.7%) and pre-mitigation (27.5%) phases.
No other relevant differences were found regarding sociodemographic or consultation characteristics other than the presenting shift between the different mitigation phases.
During the study period (January 2018 – September 2022), a total of 285 patients were mechanically restrained. This corresponds to an incidence of 1.22 per 1000 consultations, which is substantially lower than previously reported in Lausanne, Switzerland [23]. We identified several possible factors that might explain the difference. First, in our institution, we almost exclusively use 5-point mechanical restraint. We generally refrain from partial mechanical restraint, opting instead for supervision by security personnel when necessary. In Lausanne, by contrast, partial mechanical restraint is used and was included in the analysis of Beysard et al. Second, the rate of violent offences is markedly higher in Lausanne, which could contribute to more presentations involving risk of harm to others [24]. Finally, violations of the Narcotics Act are more common in Lausanne than in our region, which may result in a greater number of presentations with aggressive behaviour, often associated with illicit drug use [25].
Due to variations in legal and practical definitions of mechanical restraints, as well as differences in healthcare organisation, comparing incidences across different countries is difficult. Nevertheless, our reported incidence is very low compared with published data of EDs in other countries. Krueger et al. reported that 12 per 100 patients were subject to at least one physical restraint. However, if restrictive bedrails were excluded, only 2 per 100 patients underwent restrictive measures [17]. In the state of Victoria in Australia, a multicentre retrospective analysis found that at least one restrictive intervention (physical restraint, mechanical restraint and/or chemical restraint) was applied in 0.36% of cases [13]. In contrast, a single-centre retrospective analysis in Brisbane reported a significantly higher rate of 2.5%, despite the presence of a round-the-clock, nurse-led team responding to occupational violence emergencies [14]. In Boston, Hayek and colleagues reported a rate of 1.4% 4-point mechanical restraints among all patients presenting to the ED [15].
These considerable differences may, at least partially, be explained by structural factors such as infrastructure specifically designed for aggressive patients, staff training in communication skills and the presence of dedicated security personnel in the ED.
The duration of mechanical restraint is reported inconsistently, making direct comparisons challenging, also due to differences in how healthcare systems are organised. However, our data show significantly longer restraint durations (258 minutes) compared to Australian data (180 minutes) [13]. Furthermore, the duration of ED stays in our population (425 min) was nearly twice as long as previously reported (232 min) [14], despite similar lengths of stay in EDs reported for Switzerland [26] and Australia [27].
Notably, patients intoxicated with alcohol were subject to the longest durations of mechanical restraint, but were also significantly more often managed as outpatients, likely due to the decrease in aggression levels as blood alcohol concentration declines.
We found significant demographic and clinical differences among patients who underwent mechanical restraint. Most restrained patients were young men (67.4%) and intoxication was common (62.8%), consistent with previous studies [13–15]. In contrast, Hayek et al. reported predominantly elderly patients, while Knott et al. found few intoxicated patients, but most cases related to mental illness [13, 15]. In our cohort, the majority of restrained patients were Swiss nationals (58.9%).
Throughout the study period, most intoxicated patients were men, aligning with evidence that men consume more alcohol and experience more related harms [28–32]. This higher consumption is associated with increased aggression [33], similar to patterns observed with illicit drug use [25]. Even without intoxication, men generally display higher aggression levels, contributing to greater involvement in violent crime and overrepresentation in correctional settings [34–37]. This disparity likely reflects social and behavioural factors, including deficits in social interaction and socialisation [38]. Hormonal factors such as elevated testosterone levels have not shown associations with aggression [39]. Additionally, the perception of men as more threatening may partly explain their higher exposure to mechanical restraints [40, 41].
Furthermore, significantly more women presented with diagnosed psychiatric conditions, consistent with epidemiological data [42]. This difference may reflect a gender gap in mental health service utilisation and the underdiagnosis of psychiatric disorders in men [43, 44].
In Switzerland, 26.6% of the population lacks Swiss citizenship [45]. This group was overrepresented in our cohort, particularly among young men. Contributing factors include experiences of discrimination and racism, which increase vulnerability to substance use and aggressive behaviour [46], the heightened risk of behavioural issues among young refugees [47] and the impact of insecure residency status on aggression [48]. Furthermore, racial bias among healthcare staff may influence clinical decision-making, potentially leading to disproportionate use of mechanical restraint in minority groups [49].
The vast majority of patients were secluded with benzodiazepines, followed by haloperidol. No significant differences were observed in the choice of drugs used for coercive parenteral administration concerning the present intoxication. According to the recommendations by Hirsch et al., drugs with potential respiratory depressant effects should not be used in patients intoxicated with alcohol [50]. This discrepancy with internationally published guidelines may be partially attributed to the absence of standardised protocols for coercive measures, including specific guidelines for seclusion medication, at our institution during the study period. Another contributing factor could be the lack of standardised and/or continuous staff training.
Implementing standardised protocols in institutions regularly managing aggressive patient behaviour should be prioritised, not only to enhance adherence to international guidelines but also to reduce stress and traumatic experiences for both caregivers and patients [51]. These protocols should also include regular, critical reviews of the necessity of restraining measures and standardised documentation, such as the SOAS-R [52]. Future efforts should therefore focus on developing and evaluating institution-specific restraint protocols and structured staff training programmes to ensure both patient safety and ethical practice.
We observed a significant increase in the incidence rate ratios of mechanical restraints, as well as point estimates from the fractional polynomial regression that significantly differed from zero, during the period of COVID-19 mitigation measures compared to the pre-COVID-19 period. This finding is consistent with other published data that also showed a rise of restrictive measures and seclusions during COVID-19 [53]. The significant increase in the subgroup of patients presenting with a risk of harm to others as the reason for mechanical restraint might be associated with increased alcohol consumption and generally increased aggression [54] during the COVID-19 mitigation phase [55–57]. Unexpectedly, there was no significant decrease in mechanical restraints after COVID-19 mitigations ended. However, we only analysed data for six months after the COVID-19 pandemic, which limits the scope of interpretation. Furthermore, a longer observation period is likely required for the normalisation of the mentioned effects and consequently the return to the baseline incidence of mechanical restraints as observed prior to the COVID-19 mitigation efforts.
The retrospective nature of this study, the small sample size and the heterogeneous subgroups are the main limitations of this study. Data extraction was performed by a single author (NH), introducing a potential risk for observer bias, as interrater reliability could not be assessed. Furthermore, standardised protocols were not available during the study period at our institution; they were implemented only later. Since coercive measures including mechanical restraint were subject to the individual discretion of the supervising physician (e.g. different perception of threat level), case comparability might not always have been given. Lastly, as mentioned above, the observation period after the implemented COVID-19 mitigations was short and numbers of mechanical restraints per quarter were small and confidence intervals wide, which leads to limited comparability of the periods before and during COVID-19 mitigations and may introduce bias.
In our study cohort, mostly young, intoxicated men were subject to mechanical restraint. However, it is crucial to recognise the complexity of socially based stressors that contribute to aggressive behaviour. Women who underwent mechanical restraint predominantly presented with psychiatric comorbidities and were more likely to be at risk of self-harm rather than harm to others. During the period of COVID-19 mitigation measures, the incidence of mechanical restraint increased; however, the causality of this phenomenon is not yet fully understood.
Implementing standardised protocols in institutions managing aggressive patient behaviour is key to improving guideline adherence and reducing stress for both patients and staff.
Individual participant data that underlie the results reported in this article, after deidentification, will be available from the corresponding author, Basil Ryser, upon reasonable request, within five years of article publication.
Many thanks to Sabina Utiger and Jolanta Klukowska-Rötzler (both Department of Emergency Medicine, Inselspital, University Hospital, University of Bern, Switzerland) for their support in data collection and the collaboration with the Cantonal Ethics Committee as well as to Rodney Yeates, PhD, UK Medical Writing, for English-language editing.
No external funding was received for this study.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest related to the content of this manuscript was disclosed.
1. Federal Constitution of 18 April 1999 of the Swiss Confederation. https://www.fedlex.admin.ch/eli/cc/1999/404/de (accessed 27 September 2024)
2. Klein G, König D. Zwangsmassnahmen in der Psychiatrie: klinische Perspektive. Swiss Medical Forum ‒ Schweizerisches Medizin-Forum. 2016;16. doi:
3. Overview | Violence and aggression: short-term management in mental health, health and community settings | Guidance | NICE. 2015. https://www.nice.org.uk/guidance/ng10 (accessed 26 March 2025)
4. American College of Emergency Physicians (ACEP). Use of patient restraints. Policy statement. Ann Emerg Med. 2014 Nov;64(5):574.
5. Swiss Civil Code of 10 December 1907. https://www.fedlex.admin.ch/eli/cc/24/233_245_233/en (accessed 27 September 2024)
6. Swiss Academy of Medical Sciences. Coercive measures in medicine. https://www.samw.ch (accessed 27 September 2024)
7. Huf G, Coutinho ES, Adams CE; TREC-SAVE Collaborative Group. Physical restraints versus seclusion room for management of people with acute aggression or agitation due to psychotic illness (TREC-SAVE): a randomized trial. Psychol Med. 2012 Nov;42(11):2265–73. doi: https://doi.org/10.1017/S0033291712000372
8. Simpson SA, Joesch JM, West II, Pasic J. Risk for physical restraint or seclusion in the psychiatric emergency service (PES). Gen Hosp Psychiatry. 2014;36(1):113–8.
9. Knutzen M, Bjørkly S, Eidhammer G, Lorentzen S, Helen Mjøsund N, Opjordsmoen S, et al. Mechanical and pharmacological restraints in acute psychiatric wards—why and how are they used? Psychiatry Res. 2013 Aug;209(1):91–7.
10. Zun LS. A prospective study of the complication rate of use of patient restraint in the emergency department. J Emerg Med. 2003 Feb;24(2):119–24. doi: https://doi.org/10.1016/S0736-4679(02)00738-2
11. Lavoie FW. Consent, involuntary treatment, and the use of force in an urban emergency department. Ann Emerg Med. 1992 Jan;21(1):25–32. doi: https://doi.org/10.1016/S0196-0644(05)82232-2
12. Beysard N, Yersin B, Carron PN. Mechanical restraint in an emergency department: a consecutive series of 593 cases. Intern Emerg Med. 2018 Jun;13(4):575–83.
13. Knott J, Gerdtz M, Dobson S, Daniel C, Graudins A, Mitra B, et al. Restrictive interventions in Victorian emergency departments: A study of current clinical practice. Emerg Med Australas. 2020 Jun;32(3):393–400.
14. Tosswill H, Cabilan CJ, Learmont B, Taurima K. A descriptive study on the use of restrictive interventions for potentially or actually violent patients in the emergency department. Australas Emerg Care. 2023 Mar;26(1):7–12.
15. Hayek W, Oblath R, Bryant V, Duncan A. Risk management or racial Bias? The disparate use of restraints in the Emergency Department of an Urban Safety-Net Hospital. Gen Hosp Psychiatry. 2024;90:56–61.
16 . Thomann S, Hahn S, Bauer S, et al. Does Restraint Use Depend on the Hospital? A Multilevel Analysis of Multicentre Prevalence Measurements. 2021.
17. Krüger C, Mayer H, Haastert B, Meyer G. Use of physical restraints in acute hospitals in Germany: a multi-centre cross-sectional study. Int J Nurs Stud. 2013 Dec;50(12):1599–606.
18. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014 Dec;12(12):1495–9.
19. Coronavirus: Wichtige Entscheide des Bundesrats. 2025. https://www.uvek.admin.ch/de/coronavirus-wichtige-entscheide-des-bundesrats (accessed 13 September 2025)
20. Anwander H, Klingberg K, Gerber J, Bednarski P, Exadaktylos A, Müller M. Major trauma during COVID-19 in a level 1 trauma centre in Switzerland - a cohort study comparing the years 2020 and 2019. Swiss Med Wkly. 2021 Aug;151(33-34):w30010.
21. Coronavirus: Federal Council to lift measures – mask requirement on public transport and in healthcare institutions and isolation in the event of illness to remain until end of March. https://www.admin.ch/gov/en/start/documentation/media-releases/media-releases-federal-council.msg-id-87216.html (accessed 27 September 2024)
22. Kelly S, Martin S, Kuhn I, Cowan A, Brayne C, Lafortune L. Barriers and Facilitators to the Uptake and Maintenance of Healthy Behaviours by People at Mid-Life: A Rapid Systematic Review. PLoS One. 2016 Jan;11(1):e0145074.
23. Beysard N, Yersin B, Carron PN. Mechanical restraint in an emergency department: a consecutive series of 593 cases. Intern Emerg Med. 2018 Jun;13(4):575–83.
24. Strafgesetzbuch: Auswahl von Straftaten, nach Kanton - 2009-2024 | Tabelle. Bundesamt für Statistik. 2025. https://www.bfs.admin.ch/asset/de/34387269 (accessed 16 September 2025)
25. Schmitt J, Lamers C, Kuypers K, et al. Performance And Behavioral Effects Of Illicit Drugs. Medical legal aspects of drugs. Lawyers & Judges; 2006. pp. 71–90.
26. Bosia T, Malinovska A, Weigel K, Schmid F, Nickel CH, Bingisser R. Risk of adverse outcome in patients referred by emergency medical services in Switzerland. Swiss Med Wkly. 2017 Nov;147(4748):w14554.
27. Emergency department care access. Australian Institute of Health and Welfare. 2023. https://www.aihw.gov.au/reports-data/myhospitals/intersection/access/ed? (accessed 25 March 2025)
28. Bundesamt für Statistik. Betäubungsmittelgesetz (BetmG): Beschuldigte Personen nach Geschlecht. Alter, Aufenthaltsstatus und Nationalität; 2024.
29. Alcohol. https://www.who.int/news-room/fact-sheets/detail/alcohol (accessed 26 March 2025)
30. Wilsnack RW, Wilsnack SC, Kristjanson AF, Vogeltanz-Holm ND, Gmel G. Gender and alcohol consumption: patterns from the multinational GENACIS project. Addiction. 2009 Sep;104(9):1487–500.
31 . White A. Gender Differences in the Epidemiology of Alcohol Use and Related Harms in the United States. ARCR. 2020;40:01. doi:
32. Erol A, Karpyak VM. Sex and gender-related differences in alcohol use and its consequences: contemporary knowledge and future research considerations. Drug Alcohol Depend. 2015 Nov;156:1–13.
33. Beck A, Heinz A. Alcohol-related aggression-social and neurobiological factors. Dtsch Arztebl Int. 2013 Oct;110(42):711–5.
34. Bundesamt für Statistik. Strafgesetzbuch (StGB): Beschuldigte Personen nach Geschlecht. Alter, Aufenthaltsstatus und Nationalität; 2024.
35 . Bundesamt für Statistik. Sexualisierte Gewalt: Straftaten und beschuldigte Personen.
36 . Bundesamt für Statistik. Häusliche Gewalt: Beschuldigte Personen von vollendeten Tötungsdelikten nach Beziehung, Geschlecht und Alter.
37 . Bundesamt für Statistik. Freiheitsentzug, Insassenbestand am Stichtag. 2024.
38. AM M-L. Psychosoziale Determinanten männlicher Aggression und Gewalt. J Neurol Neurochir Psychiatr. 2010;11:70–7.
39. Geniole SN, Bird BM, McVittie JS, Purcell RB, Archer J, Carré JM. Is testosterone linked to human aggression? A meta-analytic examination of the relationship between baseline, dynamic, and manipulated testosterone on human aggression. Horm Behav. 2020 Jul;123:104644.
40 . Stevens D, Bulmer S, Banducci S, et al. Male warriors and worried women? Understanding gender and perceptions of security threats. Eur j of int secur. 2021;6:44–65. doi:
41. Harris CR, Jenkins M. Gender Differences in Risk Assessment: Why do Women Take Fewer Risks than Men? Judgm Decis Mak. 2006;1(1):48–63. doi: https://doi.org/10.1017/S1930297500000346
42 . Bundesamt für Statistik (BFS). Schweizerische Gesundheitsbefragung 2022. 2023.
43. Pattyn E, Verhaeghe M, Bracke P. The gender gap in mental health service use. Soc Psychiatry Psychiatr Epidemiol. 2015 Jul;50(7):1089–95.
44. Maestre-Miquel C, López-de-Andrés A, Ji Z, de Miguel-Diez J, Brocate A, Sanz-Rojo S, et al. Gender Differences in the Prevalence of Mental Health, Psychological Distress and Psychotropic Medication Consumption in Spain: A Nationwide Population-Based Study. Int J Environ Res Public Health. 2021 Jun;18(12):6350.
45. Bevölkerung nach Migrationsstatus. https://www.bfs.admin.ch/content/bfs/de/home/statistiken/bevoelkerung/migration-integration/nach-migrationsstatuts.html (accessed 26 March 2025)
46. Amaro H, Sanchez M, Bautista T, Cox R. Social vulnerabilities for substance use: Stressors, socially toxic environments, and discrimination and racism. Neuropharmacology. 2021 May;188:108518.
47. Begemann M, Seidel J, Poustka L, Ehrenreich H. Accumulated environmental risk in young refugees - A prospective evaluation. EClinicalMedicine. 2020 May;22:100345.
48. Eder LL, Martin A, Hapfelmeier G, Walg M. Perspectives Matter: Insecure Residency Status Accounts for Aggressive Emotions in Adolescent Refugees. Adolescents. 2024;4(1):28–40.
49. Hamed S, Bradby H, Ahlberg BM, Thapar-Björkert S. Racism in healthcare: a scoping review. BMC Public Health. 2022 May;22(1):988.
50. Hirsch S, Steinert T. The Use of Rapid Tranquilization in Aggressive Behavior. Dtsch Arztebl Int. 2019 Jun;116(26):445–52.
51. Soravia LM, Schwab S, Walther S, Müller T. Rescuers at Risk: Posttraumatic Stress Symptoms Among Police Officers, Fire Fighters, Ambulance Personnel, and Emergency and Psychiatric Nurses. Front Psychiatry. 2021 Jan;11:602064–602064.
52. Morken T, Baste V, Johnsen GE, Rypdal K, Palmstierna T, Johansen IH. The Staff Observation Aggression Scale - Revised (SOAS-R) - adjustment and validation for emergency primary health care. BMC Health Serv Res. 2018 May;18(1):335–335.
53. Goulet MH, Cassivi C, Hupé C, Jean-Baptiste F, Dumais A. Seclusion and mechanical restraint in the wake of the COVID-19 pandemic: an increased use in mental health settings. Front Psychiatry. 2024 Oct;15:1428599.
54. Killgore WD, Cloonan SA, Taylor EC, Anlap I, Dailey NS. Increasing aggression during the COVID-19 lockdowns. J Affect Disord Rep. 2021 Jul;5:100163.
55. Schmidt RA, Genois R, Jin J, Vigo D, Rehm J, Rush B. The early impact of COVID-19 on the incidence, prevalence, and severity of alcohol use and other drugs: A systematic review. Drug Alcohol Depend. 2021 Nov;228:109065.
56. Rodriguez LM, Litt DM, Stewart SH. Drinking to cope with the pandemic: the unique associations of COVID-19-related perceived threat and psychological distress to drinking behaviors in American men and women. Addict Behav. 2020 Nov;110:106532.
57. McPhee MD, Keough MT, Rundle S, Heath LM, Wardell JD, Hendershot CS. Depression, Environmental Reward, Coping Motives and Alcohol Consumption During the COVID-19 Pandemic. Front Psychiatry. 2020 Oct;11:574676.
The appendix is available in the PDF version of the article at https://doi.org/10.57187/4566