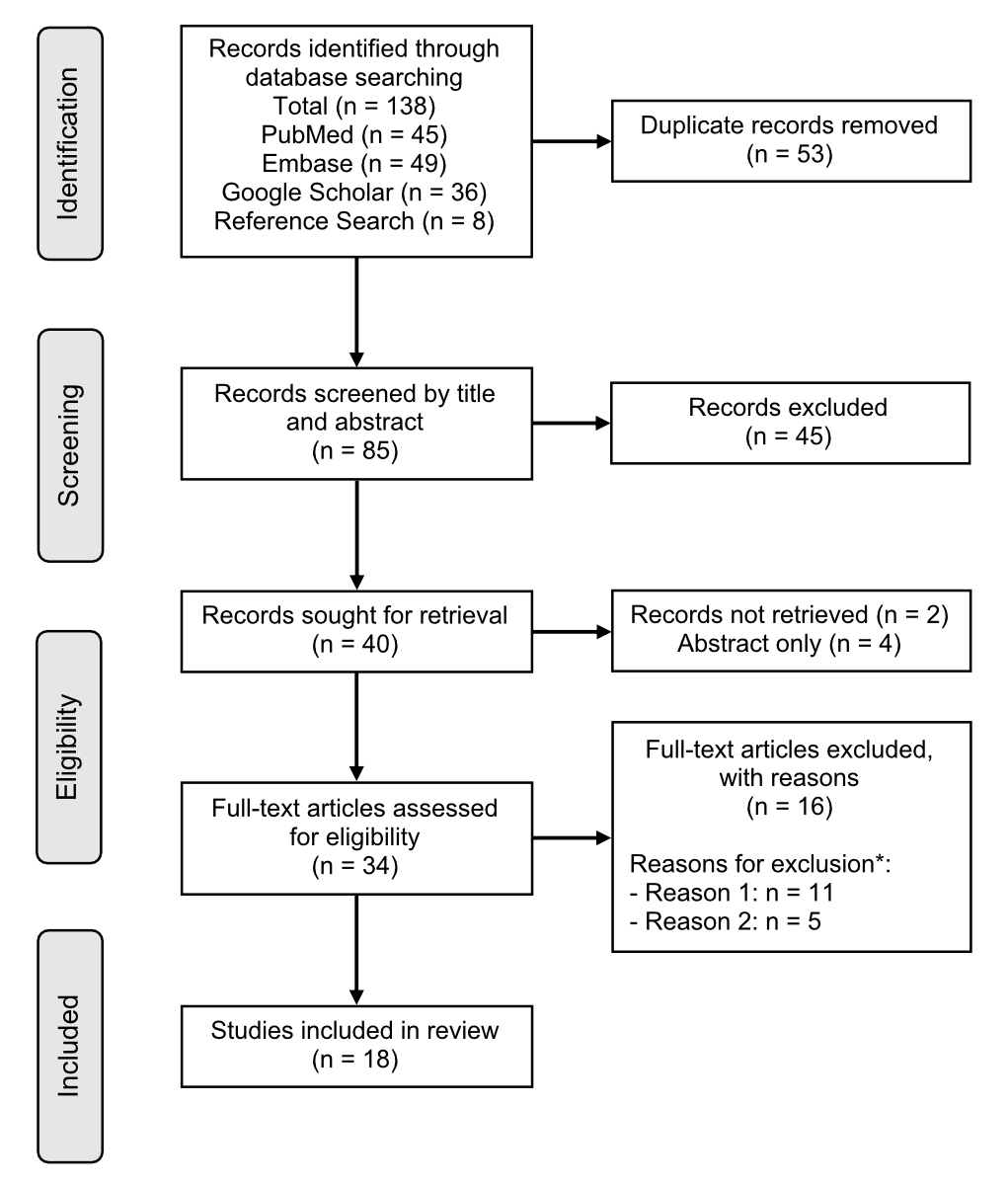
Figure 1PRISMA flow diagram. * Reason 1: article type was literature review; Reason 2: not a direct focus on use or users of image- and performance-enhancing drugs.
DOI: https://doi.org/https://doi.org/10.57187/smw.2023.40080
Body culture has significantly changed over the past decades towards lean and muscular body types, resulting in often unnatural, extreme physiques [1–4]. “Image- and performance-enhancing drugs” (IPEDs) are widely used as a convenient way to rapidly achieve personal image and sports-performance goals, not only by professional bodybuilders and professional athletes, but increasingly by recreational athletes for aesthetic purposes [5]. Image- and performance-enhancing drugs, in the context of sports, or “doping”, are performance-enhancing substances banned by the World Anti-Doping Agency (WADA), as per the prohibited list [6]. IPEDs comprise different groups of substances, with anabolic androgenic steroids being the most frequently used [1]. The use of supraphysiological doses of testosterone and its synthetic derivatives, especially when combined with strength training, leads to increased fat-free muscle mass (lean muscle mass), hypertrophic changes in muscle volume and increased strength; these effects have been described and recognised in the literature for decades [7–10]. Many different IPEDs exist and considering their rising popularity in recent years, the problematic use of these substances now poses a serious risk to individual and public health. The use of anabolic androgenic steroids can lead to many well-established and alarming side effects on various organ systems and functions: the cardiovascular system; the metabolic system; the skin; male-specific or female-specific hormonal changes; the reproductive system, potentially causing subfertility; possible nephrotoxicity, hepatotoxicity, neurotoxicity and mental health problems [1, 7, 11, 12]. Furthermore, a large proportion of anabolic androgenic steroid users develop a substance dependence [7, 17]. Although the use of anabolic androgenic steroids spread throughout the US bodybuilding world and among Olympic athletes from the late 1940s onwards, it was only from the 1980s, when anabolic androgenic steroids started to spread among the general US population, that it became a worldwide substance use problem [2]. In the 21st century, other substances have also received increasing recognition, such as growth hormones, insulin and stimulants (e.g. clenbuterol) to name a few, but anabolic androgenic steroids still form the largest category of IPEDs used [2, 15].
Today, the use of anabolic androgenic steroids and other IPEDs has become widespread throughout the world and represents one of the newest of the world’s major substance use disorders [2]. There is a large and increasing number of individuals who may be exposed to these substances [1]. Unfortunately, international research often does not included research data from Switzerland. For example, in their systematic review of over 180 articles in 2014, Sagoe and colleagues [18] estimated that the global lifetime prevalence of anabolic androgenic steroid use was as high as 3.3% in the general population, but not a single article originated from Switzerland. Research interest in this user population is growing worldwide [2]. International research has revealed that the majority of IPED users are no longer athletes but non-competitive bodybuilders or recreational gym users [1, 10, 19]. The global lifetime prevalence of IPED users in recreational sportspeople and recreational athletes is estimated to be significantly higher than in the general population, with estimates of 18.4% and 13.4%, respectively [18]. Furthermore, the popularity of these substances is reported to have increased significantly over the last decade outside Switzerland [1].
Regarding the growing research interest and use of IPEDs worldwide, we decided to conduct a scoping literature review on evidence of the use of these substances and substance users in Switzerland. We also further elaborate on the implications of our findings for Swiss drug policy.
This scoping review was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) statement [20].
For this scoping literature review, we searched PubMed/Medline, Embase and Google Scholar for peer-reviewed studies and grey literature published before 6 August 2022. The primary objective was to further describe evidence of (1) IPED use, and (2) IPED users in Switzerland.
We used the following search strategy with Boolean operators: “(Doping) AND (Switzerland)”, “(AAS) AND (Switzerland)”, “(Anabolic steroids) AND (Switzerland)”, “(Image- and performance-enhancing drug) AND (Switzerland)”, “(Performance-enhancing drug) AND (Switzerland)”, “(Doping) AND (Swiss)”. For Google Scholar the search term “Doping Switzerland” was used. The search terms were translated and used in comparable expressions in German, Italian and French, which are the national languages of Switzerland. In addition, relevant article references were manually tracked in order to identify sources in obscure locations – the so-called snowball method [21]. Each study was screened by title, abstract, and full-text based on predefined eligibility criteria (table 1).
Table 1Inclusion and exclusion criteria.
| Inclusion criteria |
| Peer-reviewed original article; full text available |
| Non-peer-reviewed original article; full text available (grey literature) |
| Conducted in Switzerland |
| None for study period |
| Article in English, German, French or Italian |
| None for study design |
| None for study population or sex |
| Article that presents evidence on use or users of IPEDs |
| Exclusion criteria |
| Abstract-only article (e.g. conference proceedings), editorial, correspondence, thesis, book |
| Non-original article, e.g. review article |
| Article without full text available |
| Article that does not discuss direct or indirect evidence on use or users of IPEDs. Examples of excluded articles: those discussing attitudes towards IPEDs; policy papers |
Two reviewers (MK/RM) performed the database search and extracted articles separately. Both reviewers removed duplicate records and screened each study by title and abstract. Full texts of eligible studies were screened and reviewed by both reviewers (MK/RM) for data extraction. Disagreements in study eligibility were resolved by consensus between all reviewers (MK/RM/PB).
Once the articles were selected, the following data were recorded in an extraction table: author, year of publication, geographical area of Switzerland, study design, study period (if applicable), peer-review status, study objective, sample size, study population with sports classification, outcome and outcome measure, evidence of IPED use or users, key findings. Three team members (MK/RM/PB) reviewed all data to ensure accuracy before analysis. Disagreements in data extraction were resolved by consensus between the three reviewers (MK/RM/PB).
No formal study quality assessment was done for this literature review as it is not a prerequisite for scoping reviews. We used a narrative synthesis approach for data analysis. Outcome measures were not pre-specified, but continuously added throughout data extraction to ensure that all relevant outcomes were captured. Data was summarised by outcome table and text.
For the classification of prohibited substances, articles commonly referred to the world anti-doping agency (WADA) prohibited list, which can be viewed in table 2 (updated version as of 01 January 2021) [6].
Table 2Classification of prohibited substances coded according to the World Anti-Doping Agency prohibited list (updated version as of 01 January 2021) [6].
| WADA Class | Compound class | Examples of compounds |
| S0 | Non-approved substances | Specified substances, e.g. drugs under preclinical or clinical development or discontinued, designer drugs, substances approved only for veterinary use |
| S1 | Anabolic agents | E.g. anabolic androgenic steroids, other anabolic agents such as clenbuterol and selective androgen receptor modulators |
| S2 | Peptide hormones, growth factors, related substances and mimetics | E.g. erythropoietin and agents affecting erythropoiesis, chorionic gonadotropin, luteinising hormone and growth hormone, growth factors and growth factor modulators |
| S3 | Beta-2 agonists | E.g. fenoterol, salbutamol and salmeterol |
| S4 | Hormone and metabolic modulators | E.g. aromatase inhibitors, antioestrogenic substances, agents preventing activin receptor IIB activation (such as myostatin inhibitors), metabolic modulators (such as insulins) |
| S5 | Diuretics and masking agents | E.g. desmopressin and acetazolamide |
| S6 | Stimulants | E.g. ephedrine, cocaine, methylenedioxymethamphetamine (MDMA / “ecstasy”) |
| S7 | Narcotics | E.g. diamorphine (heroin), fentanyl, oxycodone |
| S8 | Cannabinoids | E.g. in cannabis (hashish, marijuana), natural and synthetic tetrahydrocannabinols (THCs) |
| S9 | Glucocorticoids | E.g. cortisone, prednisolone |
People participating in sports were classified into “athletes”, “recreational gym users” and “bodybuilders”. “Athlete” refers to “a person who competes in one or more sports that involve physical strength, speed or endurance”. Based on their level of participation, athletes were professionals or amateurs [22]. “Recreational gym user” refers to a person who uses the gym for leisure. “Bodybuilder” refers to a person who uses resistance training for building muscle via muscle hypertrophy. Bodybuilders are professionals if they participate in competitions and recreational if they do not.
Figure 1 shows the process used to identify and select studies. The predefined search strategy, involving three electronic databases, yielded 138 records (PubMed: 45, Embase: 49, Google Scholar: 36, reference search: 8). After removing 53 duplicates, we screened 85 records, first by title then by abstract. Of the 40 records we marked for retrieval, we retrieved 34 full-text articles; we could not obtain 2 records in full-text format and 4 were abstracts only and hence excluded. The full-text screening stage of 34 articles yielded 18 articles relevant to this scoping review. Additional articles were excluded after full-text assessment for the reasons mentioned in the flow chart.
Figure 1PRISMA flow diagram. * Reason 1: article type was literature review; Reason 2: not a direct focus on use or users of image- and performance-enhancing drugs.
Table 3Characteristics of n = 18 published studies presenting data on image- and performance-enhancing drug users and use in Switzerland.
| Characteristic | Proportion of articles | |
| Year of publication (mean) | 1998 to 2022 (2011) | |
| Published within last 5 years | 3 (17%) | |
| Published within last 10 years | 7 (39%) | |
| Peer-reviewed | Yes | 15 (83%) |
| No | 3 (17%) | |
| Sample information (total included n, range) | Survey participants | 11,401 (147 to 2500) |
| Interview participants | 140 (8 to 70) | |
| Chemically analysed samples | 1368 (75 to 1190) | |
| Study design | Non-clinical in vitro toxicological analysis | 3 (17%) |
| Observational | 1 (6%) | |
| Semi-structured interviews | 4 (22%) | |
| Survey | 9 (50%) | |
| Mixed | 1 (6%) | |
| No (of total n = 14) of included studies involving: | Professional athletes | 6 (43%) |
| Amateur athletes | 5 (36%) | |
| Mixed | 3 (21%) | |
| No (of total n = 14) of articles originating from different areas of Switzerland | French-speaking area | 8 (57%) |
| German-speaking area | 1 (7%) | |
| Italian-speaking area | 0 (0%) | |
| Mixed | 5 (36%) | |
| Articles involving as outcome | Use of IPEDs | 4 (22%) |
| Users of IPEDs | 0 (0%) | |
| Both | 14 (78%) | |
IPEDs: image- and performance-enhancing drugs
All study characteristics can be viewed in detail in table 3. The peer-reviewed literature on IPED use and users has not increased considerably in the last few years. Among the included articles, a minority (17%) were published within the 5-year period (2018–2022) preceding the present review and less than half (39%) within the preceding 10-year period (2013–2022). The mean year of publication of the studies included was 2011. Most of the studies included were peer-reviewed (83%). Among the included articles, a cumulative total of 11,401 participants were surveyed and 140 people were interviewed. Importantly, among the interviewees, eight of the professional cyclists were interviewed in three different articles. Among the toxicological articles included, 1368 substances overall were chemically analysed.
Among the different study designs included, the most frequent (50%) was survey. Other designs were semi-structured interview (22%), non-clinical in vitro toxicological analysis (17%), observational study (6%) and mixed study design (6%).
With regard to different types of athletes, 43% of the obtained data was derived from studies with professional athletes, 36% from studies with amateur athletes. In 21% (n = 3), the data was mixed; this data included articles that did not focus on athletes, such as surveys of the general population, comparison between sporty and non-sporty adolescents and IPED importers [23–25].
With regard to articles that conducted interviews and surveys, most originated from the French-speaking part of Switzerland (57%), whereas 7% originated from the German-speaking part. The origin was not clear in four studies, and one study was conducted in both French- and German-speaking parts of Switzerland [23, 25–28].
Among the 18 included studies, only 11 different first authors conducted the research. Three of these studies were based on interviews with professional cyclists and their environment, with eight cyclists repeatedly interviewed in all three studies.
The full extraction form can be viewed in table S1 in the appendix. Regarding the primary outcomes, most (78%) of the included articles focused on both outcomes. Table 4 shows outcome measures that were extracted from available literature per primary outcome.
Table 4Outcome measures.
| Outcome | Outcome measure | N° of articles measuring the outcome |
| Users of IPEDs | Epidemiology | 6 |
| Motivators of IPED use | 8 | |
| Affected sports disciplines | 5 | |
| Knowledge about IPED use | 8 | |
| Use of performance-enhancing drugs among athletes | 5 | |
| Perception of IPEDs | 3 | |
| Use of IPEDs | Diversity of substances used | 13 |
| Chemical quality of substances | 3 | |
| Access to banned substances | 7 | |
| Information on IPED use | 7 |
IPEDs: image- and performance-enhancing drugs
Epidemiology
Some authors have analysed the prevalence of IPED use in sports in Switzerland. The prevalence of IPED use among amateur athletes and sporty active adolescents was estimated to be between 2% and 3.7%, according to survey data [24, 29, 30]. These estimates come with some caveats. Different questionnaires used different types of question: open-ended questions, closed-ended questions or lists of substances. Furthermore, definitions of performance-enhancing drugs varied, not always being consistent with the World Anti-Doping Agency (WADA) anti-doping list (table 2); thus the prevalence of performance-enhancing drug use among athletes could range from 1.3% to 39.2% according to survey data [29, 30]. Nocelli and colleagues additionally concluded that the prevalence of performance-enhancing drug use in sports is perceived to be high among the Swiss population in general [23]. Importantly, the surveys demonstrated the non-trivial proportion of non-users (8.6%) and of adolescents (7.4%) who intended to use performance-enhancing drugs in the future [24, 29].
Lentillon and colleagues further investigated the frequency of performance-enhancing drug use among users and demonstrated that the majority of users (60.9%) only used them sometimes, while a minority used them regularly (25.9%) or even daily (13.2%) [29]. Furthermore, Bélanger and colleagues demonstrated that the percentage of sporty and non-sporty adolescents who reported knowing peers using performance-enhancing drugs was as high as 14% and 9%, respectively [24].
Use of IPEDs is not confined to athletes; the general population in Switzerland also seems highly affected [25]. Although survey data on recreational bodybuilders and gym users in Switzerland was not found in the literature search, the analysis of importers of IPED packages seized by Swiss border authorities gives more insight on the whole spectrum of IPED users in Switzerland. Only 1% of a total of 696 importers of IPEDs in 2013/2014 were athletes subject to anti-doping regulations of the Antidoping Switzerland (ADCH) Foundation, and hence liable to disciplinary action [31]. In the vast majority of cases, users did not belong to any active sports organisation and were partaking in recreational bodybuilding or staying fit [31].
Weber and colleagues identified common traits of Swiss IPED importers and users [25]. Typical IPED importers are well-educated, employed, non-competing males in their 20s to 40s. Furthermore, sex differences exist with the overwhelming majority (82%) of the importers investigated being male and the minority (15%) female [31]. This data was confirmed by Lentillon and colleagues who showed that males had a higher prevalence of IPED use [30]. Furthermore, a higher frequency of training was also associated with a higher level of IPED misuse [23, 28, 30].
Motivation for using IPEDs
The most frequently cited reasons for IPED use were performance enhancement and muscle building [25, 27, 28, 32]. Among IPED importers, it could be shown that the motivation to use these substances differed according to age and sex [25]. While men aimed to increase their muscle mass and improve athletic performance, women focused on weight loss [25]. For both men and women, however, appearance seemed to play an important role in IPED use, with men and women importing IPEDs for image reasons [25]. While the vast majority of young people under the age of 20 aimed to improve their athletic performance, the aim of those over the age of 50 was for medical, health or other reasons [25]. Other motivators were: to prevent injuries; pain relief; regeneration; the feeling of strength; and overall wellbeing [28, 33]. It was demonstrated that bodybuilders started using IPEDs through contact with more experienced peers [33]. Among professional cyclists, reasons for the use of performance-enhancing drugs varied, but they were primarily for short-term performance improvements, e.g. to win a race, to achieve personal goals or to overcome insecurities especially in the absence of adequate support [32, 34, 35]. Living in a city was another risk factor for the use of IPEDs among adolescents [24]. In professional sports, the main risk factor for the use of performance-enhancing drugs was the pressure exerted on the athlete by the family, team members and staff or managers [34].
Affected sports disciplines
According to survey data and interviews with coaches, the general population and bodybuilders, it was demonstrated that IPED use appears to be common among power sports, i.e. bodybuilding and fitness in general, but also among endurance sports [25]. Among bodybuilders, the use of IPEDs appears to be particularly common and widespread [23, 33]. Among professional sports, disciplines that were perceived to have high proportions of performance-enhancing drug use included swimming, track and field, cycling and Nordic walking [23, 26]. Comparable results were also found in a survey of young Swiss amateur athletes, which showed that IPEDs are most used in outdoor sports and team sports, with sports such as martial arts (e.g. judo), ice hockey and cycling being the most frequently mentioned [30].
Knowledge about IPEDs
There appears to be a lack of knowledge about the type of IPEDs used, the import of IPEDs into Switzerland and their side effects. It was demonstrated that the vast majority of amateur athletes lacked knowledge about performance-enhancing drugs that appear on the WADA anti-doping list; therefore on some occasions athletes did not have the intention of using performance-enhancing drugs or were not aware of even taking banned substances [29, 30]. Regarding the import of IPEDs, only a minority of importers was aware that the import of these substances into Switzerland was prohibited and that they were at risk of legal action [25]. Regarding the awareness of side effects, a higher proportion of bodybuilders were aware of the side effects and dangers of IPEDs than professional athletes, e.g. professional cyclists, who either hardly recognised or trivialised side effects and potential harm to health [32–34]. The use of performance-enhancing drugs under medical supervision was perceived as health protection by interviewees [36]. Regarding supplements, survey data also confirmed a lack of knowledge among adolescent professional athletes and amateur athletes, as supplements were often taken inappropriately and consumers did not know whether the substances contained in the supplements were on the WADA anti-doping list [27, 28].
Image- and performance-enhancing drug use among professional athletes
A number of interviews with professional cyclists further explored the role of performance-enhancing drug use in professional sports and revealed that interest in using them still persists, as the majority of interviewees were tempted by performance-enhancing drugs [32, 34, 36]. In the past, it was demonstrated that at the professional level there was extensive pressure to start using performance-enhancing drugs, which manifested as, for example, exclusion from the team, bullying or being forced to end one’s career [32, 36]. Furthermore, the use of performance-enhancing drugs under medical supervision was common practice at international professional level [36]. As a result of several performance-enhancing drug scandals, however, the use of performance-enhancing drugs in professional cycling has changed [32]. Nowadays, performance-enhancing drug use in professional cycling is less common and more individual [32]. Associated health risks are also considered more dangerous since these substances must be obtained from the Internet and are less easily available from doctors [32]. This has led to some rejection among athletes, as the clandestine market over the Internet does not guarantee good-quality substances and there is a risk of possible anti-doping checks [32]. Following several performance-enhancing drug scandals, the external pressure on professional cyclists has decreased and it is possible nowadays to avoid the use of performance-enhancing drugs, according to interviewees [32]. However, the interest of professional cyclists in performance-enhancing drug use can also be seen indirectly nowadays, as six of the eight respondents intentionally chose a sports doctor who supports performance-enhancing drug use rather than a doctor who is against their use, a finding that is also evident from interviews with professional cyclists conducted by Brissonneau and colleagues [32, 35].
Mettler and colleagues demonstrated in a recent user survey that supplement use was widespread among adolescent professional athletes of various sports disciplines, with only 3% of all respondents not taking any supplements [27]. Substantial proportions (30%) of the substances were intentionally used to enhance performance, in addition to the main motivators of improving regeneration (40%) and supporting health (39%) [27]. Overall, a small proportion (2.8%) of all respondents was willing or somewhat willing to use illegal IPEDs if no-one would ever find out [27]. Importantly, this group also uses supplements more often to improve performance than those who would never use banned IPEDs [27].
Perception about IPED use
Surveys among the general population conducted in 1995 already suggested that there was a problem of performance-enhancing drug use in sport, as performance-enhancing drug use in professional sports was considered a serious problem by most of the Swiss general population; in contrast, in amateur sports, performance-enhancing drug use was assumed to be a less severe problem [23]. Up until today, large proportions of athletes and trainers have stated that they perceived performance-enhancing drug use to be a serious problem in their sport, according to survey data [23]. However, among professional cyclists, performance-enhancing drug use was not only perceived as a problem in sport, but much more as a social phenomenon, as nowadays performance-enhancing drugs are used in many areas of life and have been trivialised [34].
Diversity of used substances
Some authors assessed the variety of different substances that are used by the Swiss population. Among 1190 IPEDs seized at the Swiss border in 2013/2014, by far the most common substance group seized was anabolic agents, most frequently anabolic androgenic steroids (75%), with testosterone and its esters (27.3%; 213/779) among many other synthetic derivatives [37]. Other substance groups that were commonly seized were peptide hormones or growth factors and mimetics, e.g. human chorionic gonadotropin (hCG), human growth hormone (hGH), insulin-like growth factor 1 (IGF-1), and antioestrogens, e.g. aromatase inhibitors, or other metabolic modulators, e.g. clomiphene, tamoxifen, anastrozole [37].
The type of substances used varied by age, motivation, sex and sports discipline. Among young adolescents, the most commonly used illegal substances were analgesics (11.3%), alcohol (5.1%) and cannabis (3.4%) according to survey data [24]. There is a higher prevalence of IPED use among users of recreational drugs, e.g. cannabis, than in non-users (2.3% vs 0.1%); in the same survey, approximately 32% of all cannabis users also used IPEDs with the aim of improving athletic performance [24]. Other substances mentioned in that user survey were human growth hormone and cocaine use among the sporty adolescents, as well as erythropoietin (EPO) and anabolic androgenic steroids among the non-sporty adolescents [24]. Furthermore, substances such as methylphenidate (neurodoping) and corticosteroids were identified [24]. The products most frequently used by adolescents to improve performance included caffeinated products such as energy drinks, sports drinks or other supplements [24].
Regarding the motivation of IPED importers, this depended on the prospective use of the different substances. In order to improve athletic performance, supplements were mainly used, whereas for increasing muscle mass, anabolic androgenic steroids and supplements were preferred [25]. Regarding sex, it was demonstrated that for men, anabolic androgenic steroids and supplements were the most popular, while women preferred human chorionic gonadotropin, testosterone and clenbuterol [25, 31].
Regarding the different sports disciplines, Weber and colleagues demonstrated that athletes imported significantly more anabolic androgenic steroids than non-athletes [25]. According to user survey data, the most commonly used performance-enhancing drugs in recreational athletes were alcohol, marijuana and drugs for asthma [29, 30]. Less frequently, other substances were also listed such as anabolic androgenic steroids, amphetamines, beta-blockers or beta-2 agonists, cocaine, corticosteroids, diuretics, ecstasy, ephedrine, erythropoietin, growth hormone, heroin, local anaesthetics, morphine, methylphenidate [28–30].
Interviews among professional cyclists demonstrated that all interviewees (n = 8) were taking nutritional supplements [34]. Corticosteroids were the substances most frequently misused, due to anti-doping regulations with a Therapeutic Use Exemption, and often formed the entry point for IPED abuse among cyclists [34, 35]. The use of other banned substances was widespread in professional cycling, e.g. erythropoietin, human growth hormone and blood transfusions, which are more expensive but also more difficult to obtain and apply and therefore only used at professional level [32, 34, 36]. Regarding methods of using IPEDs, injected substances appear not to be used in amateur cycling but are more common among professional cyclists [34, 35].
Chemical quality of substances from unregulated online markets
In order to further determine the proportions of fake IPEDs among the compounds seized at the Swiss border, chemical analyses of these substances were carried out. It was demonstrated that the majority, over 80%, of all analysed products either did not contain the labelled substance or the substance was not present at the anticipated concentration [37]. The authors demonstrated that these fake products might contain no active ingredient, or contain it but in an amount other than that labelled; contain a wrong active ingredient; or contain none, all or more active ingredients than those labelled [37]. Interestingly, the proportion of fake substances varied by substance group, e.g. anabolic androgenic steroids were most commonly fake whereas antioestrogens, i.e. aromatase inhibitors, were of original quality throughout [37].
Additionally, the problem of fake products obtained via unregulated channels was not confined to pharmaceutical compounds but affected supplements too. Kamber and colleagues as well as Baume and colleagues demonstrated that major proportions of supplements might be mislabelled or adulterated, most frequently with testosterone and its derivatives, whereby their intake would even result in a positive doping test [38, 39].
Access to banned substances
It was demonstrated that by far the most frequent access route to substances was via the Internet or the black market, but other suppliers were also used, such as friends, other athletes, physicians, pharmacies, gyms, and coaches or trainers [23–25].
Regarding imported black-market products seized at the Swiss border, Weber and colleagues demonstrated that shipments originated from many manufacturers, ranging from well-known pharmaceutical companies to underground laboratories, and that these were sent to Switzerland mostly from Asian countries or China, mostly via south-east European countries [31]. Importantly, the vast majority of these seized shipments were sent with the final destination being Switzerland [31]. In particular, the biggest proportion was sent to the canton of Zurich [31]. Other frequent destinations in Switzerland were Geneva, Lausanne, Bern, Basel and St. Gallen [31]. The imported IPEDs were mostly for personal use and on some occasions consumers ordered more than once [25, 31]. Importantly, the import of these substances appears to be a multimillion CHF business. The 960 packages seized had an estimated value of 1,114,311 CHF, and these seized packages represent only a fraction of all packages that are actually imported; the exact number of imports remains unknown [31].
Information on IPED use
Among IPED importers, the Internet appears to be the channel most frequently used to obtain information about the quality of substances [25]. In professional sports, information about performance-enhancing drugs is commonly obtained from Antidoping Switzerland (ADCH), trainers and staff, experienced peers, federations and clubs, doctors, articles or books about performance-enhancing drug scandals, as well as via the Internet [26, 32, 34–36]. Moreover, adolescent professional athletes mostly obtained information about supplements from those who recommended the substances, but also from the Internet and supplement suppliers, so the information they received is considered low-quality [27]. According to survey data, professional athletes commonly felt sufficiently informed about performance-enhancing drugs, but their coaches wished to be better informed [26].
Our scoping literature review included 18 articles from the published literature that provided evidence on use and users of IPEDs in Switzerland. A diversity of study designs and a variety of sports areas were assessed. Results were derived from a total of 11,401 survey participants and 140 interviewees, as well as toxicological results of 1368 chemically analysed substances.
We have demonstrated that there is a lack of studies and a lack of diversity within the different research groups that are conducting research on IPED use and users in Switzerland. Less than half of the studies were conducted within the past ten years and only eleven different first authors of these 18 articles were responsible for the articles included. Furthermore, the geographical scope was limited as most studies originated from the French-speaking area of Switzerland, but the diversity of sports fields was also disproportionate, as most studies were conducted among professional athletes. We have demonstrated that most imported substances seized at the Swiss border were from non-athletes [25], which is in line with the literature outside of Switzerland [1, 7, 10, 19, 40–43]. It is of great importance that more research will be done on this possibly growing user population in Switzerland, and particularly among recreational gym users and bodybuilders, as they represent most users.
Few authors have provided data on IPED users. Due to a lack of reporting, precise prevalence and demographic data about these users are scarce and, due to methodological challenges, this data must be interpreted with caution. Use of these substances among professional and amateur athletes appears to be prevalent. Prevalence of performance-enhancing drug use among amateur athletes was estimated to be between 2% and 3.7% according to survey data in Switzerland, although the prevalence of performance-enhancing drug use among athletes ranged from 1.3% to 39.2% [24, 29, 30]. It has been demonstrated that many more intend to use IPEDs in the future or knew someone who was also using IPEDs. This is in line with a systematic review that estimated a global lifetime prevalence of anabolic androgenic steroids users in athletes of up to 13.4% in 2014 [18]. In this scoping review, we did not find any evidence for prevalence among non-athletes. The analysis of IPED importers supports the hypothesis that most users are non-athletes as it was demonstrated that only 1% of Swiss IPED importers via online sources were athletes, whereas the rest were non-athletes [31]. Some common traits of these importers or users were identified: importers were well-educated, employed, non-competing males in their 20s to 40s [25]. This is in line with epidemiological data from IPED users from other countries outside Switzerland [1, 7]. The most common reasons for use were image enhancement, i.e. muscle growth, although athletes were motivated by the performance-enhancing effect. Other motivators exist depending on age, sports field, sex and other sociodemographic factors. Furthermore, the type of substances used could also vary by age, motivation, sex and sports discipline. More epidemiological data on this user population is of great importance to further understand this threat to individual and public health in Switzerland.
We have demonstrated that substantial proportions of IPEDs found on the black market and seized at the Swiss border are fake and of a substandard drug purity that leaves users in Switzerland with unpredictable risks [37]. Fake products were a problem affecting almost all imported substances, although differences exist between substance groups. These findings are in line with data from outside Switzerland [14]. These fake products can lead to unexpected adverse events in addition to the already well-established side effects of IPEDs, as well as additional unexpected drug-drug interactions as this user population is inclined to polydrug use [1, 40, 44]. These substances commonly originated from many different manufacturers and were sent to Switzerland from Asian countries, mostly via south-east European countries. Users in Switzerland need to be protected from these fraudulent substances. There is nothing that would suggest that the use and import of these substances will decline in the foreseeable future as we also provide further evidence that the amount of seized or confiscated compounds increased over the observation period in Switzerland, and that the illegal import of these substances is also estimated to be a multimillion CHF business [37].
Besides fake IPEDs from the black market, we have also demonstrated that sports supplements from online markets may be adulterated and possibly contain testosterone and synthetic derivatives [38, 39]. Supplements are very widely used by non-athletes, athletes and bodybuilders [24, 25, 27, 33, 34, 38, 39]. This is particularly concerning as these users do not intend to use anabolic androgenic steroids and may possibly suffer from unexpected effects, as well as adverse events and unexpected positive doping tests from unintentional intake of these substances. These products are widely unregulated, do not go through any drug approval process and thus lack the necessary quality control. It is of importance that prevention strategies incorporate the use of these non-regulated supplements.
Image- and performance-enhancing drug use has become widespread throughout the world and represents one of the newest of the world’s major substance abuse disorders [2]. According to international data, there appears to be a large and increasing number of individuals who encounter these substances [18, 45]. With this scoping literature review, we have presented some evidence that the use of these substances is also prevalent in Switzerland, although we have not presented any conclusive evidence on prevalence, side effects or long-term implications of use in Switzerland. We have demonstrated that the quality and quantity of research relevant to Switzerland is limited and further research with robust methodologies is needed, particularly as IPED use is becoming an aesthetic tool across the general population. At this point, we can only surmise that use of these substances and motivations for use by Swiss users will follow international trends. In neighbouring Germany, the Epidemiological Survey of Substance Abuse (ESA) estimated the 12-month prevalence of anabolic use in the general population to be 0.7% in 2018, which has increased over the observation period [46]. In a systematic review and meta-analysis by Sagoe and colleagues, the global lifetime prevalence of anabolic androgenic steroids use in the general population was estimated to be 3.3%, which would suggest that over 200,000 people have used anabolic androgenic steroids in Switzerland [18].
Clinicians should become aware of the considerable individual and public health threat that anabolic androgenic steroids and other IPEDs pose in Switzerland and worldwide, given the significant negative long-term health effects of IPED use. Importantly, anabolic androgenic steroid dependence among substance users is common and is described in 25–40% of anabolic androgenic steroid users according to literature [1, 7, 19, 47]. Other relevant risks regarding addiction medicine that should be mentioned are the concurrent use of other psychotropic substances that appears to be common, as well as the risk of infection by blood-borne viruses from injection practices and sexual behaviours [48, 49]. Swiss drug policy aims to reduce drug use and its negative consequences for users and society [50]. The revised Narcotics Act (NarcA) of 2008 implemented a four-pillar drug policy into law, comprising prevention, harm reduction, therapy and repression. Unfortunately, IPED use as substance use disorder is currently a widely neglected area in the field of medicine; prevention and harm-reduction strategies, as well as medical programmes barely exist in Switzerland and should be further explored and evaluated for this user population.
Prevention strategies often do not reach this hard-to-reach user population. According to survey data in Switzerland, most anabolic androgenic steroid users demonstrate inadequate knowledge about the harmful effects of these substances, the WADA anti-doping list and the law surrounding import, as demonstrated in this review [24–26, 28–30, 32, 34]. Tailored prevention strategies are needed to accurately inform this hard-to-reach user community.
Harm reduction addresses people who use IPEDs, those who cannot or do not want to discontinue their use, to reduce risks wherever possible. Different, established harm-reduction strategies that are already implemented for different areas of addiction medicine in Switzerland should be further explored and could be implemented to reduce risks of IPED use. Such strategies could entail the controlled use and availability of these substances through healthcare providers, such as the medical prescription of opioids (opioid agonist therapy), needle and syringe programmes (NSP) and promotion of safer-use practices [51]. The authors would like to highlight the findings of Weber and colleagues, who demonstrated the high levels of counterfeiting and mismatches between listed and contained ingredients in IPED samples shipped through Switzerland and seized by Swiss border authorities [37]. International data demonstrates that this trend is similar across various countries and settings [14]. Many who use IPEDs such as anabolic androgenic steroids for non-medical purposes report coming into contact with counterfeit substances and experiencing harm as a result [52]. Furthermore, some IPED users try taking steps to limit coming into contact with counterfeit products, though recognise that many of these methods have limitations (e.g. appearance of packaging or content) [52]. The implementation of drug safety checking services with accompanying counselling could provide IPED users with an opportunity for more informed decision-making when taking these substances. This harm-reduction strategy has already been successfully implemented for other illicit drugs in Switzerland and worldwide [53]. People using this service submit samples for chemical analysis and receive feedback on the composition of their samples prior to use [54]. Drug-checking services in Switzerland have existed since the 1990s and they are central elements in the Swiss drug policy that aims to reduce drug use and its negative consequences for users and society. Evidence on the positive impact of drug-testing services on substance user behaviour and individual health has been described in the literature [55–58]. To our knowledge, there is currently no published evidence on drug-checking services for IPEDs. Existing drug-checking guidelines should be reviewed to further explore the potential role in engaging people who use IPEDs within their services, given significant health effects of its use.
For IPED users who develop side effects and dependency, there are some guidelines in the literature on treatment recommendations [10, 16, 47, 59]. A few so-called “steroid clinics”, specialised clinics for IPED users, have already been successfully implemented and established in the recent past in a few countries [60]. Previous positive experiences in the field of addiction medicine with patient groups that are difficult to reach, such as recreational substance users, give hope that with adapted treatment concepts, stable contacts can also be established with this user population and that these patients can be persuaded to accept further offers of help [61, 62]. Despite the global rise of IPED use, only a minority of IPED users seek support from medical professionals in case of questions or adverse events [63]. In practice, the medical approach includes the principles of harm reduction and adheres to medical guidelines regarding optimal treatment for a patient. For the treatment of IPED users, these guidelines often suggest the prescription of a few substances prohibited under anti-doping regulations in order to treat adverse events. In Switzerland, by virtue of the Sports Promotion Act, healthcare professionals could be held criminally liable for providing care or prescribing treatment with these substances, leaving non-athlete IPED users in Switzerland untreated when it comes to medical problems [64]. Principles of medical care that apply to patients consuming other illegal substances in unregulated drug markets, such as heroin and other opioids, do not apply to IPED users, not even for non-competing, recreational gym users. Under current legislation, the Sports Promotion Act, providing care to non-athlete IPED users may lead to imprisonment of the treating doctor. Unfortunately, as demonstrated, regulations and legislation surrounding these substances currently still represent the biggest hurdle in providing prevention and medical care to IPED users and in reducing the related public health burden. There are substantial efforts to conduct doping tests among athletes and efforts to stop their use in competing athletes. Importantly, these efforts only affect a minority of users as most individuals using these substances appear to be non-athletes. The current anti-doping legislation does not seem to be preventing the number of non-athlete IPED users from growing, but it is actively hindering adequate medical care for these individuals and contradicts Switzerland’s established drug policy for other illegal substances.
This research has some limitations. The evidence base for this research area is very limited due to the paucity of Swiss studies and there are many variables in this study that may lead to bias of the studies included and the conclusions drawn. The use of self-reporting, possibly poor interviewing techniques, inclusion of outdated studies, use of grey literature, use of multiple data sources and possible misclassification of doping substances in the respective studies may have led to inaccurately measured study variables and thus influenced the results and conclusions of this review, as well as led to over- or underestimation of prevalence data (information bias). More studies with robust methodologies undergoing peer-review are needed. Furthermore, the use of interviews and self-reports may have led to interviewer bias, as well as response bias, particularly as the consumption of doping substances is illegal (social desirability bias) and may have led to inaccurate responses among interviewees and thus impacted the data synthesis of this review. Lastly, interviews of professional athletes consisted almost entirely of cyclists (selection bias), and we demonstrated a misrepresentation of user populations (most perspectives were from athletes, the minority of IPED users), a misrepresentation of regions in Switzerland (most articles derived from the French-speaking area), small sample sizes and involvement of the same interviewees across different articles (sampling bias). This may have led to a one-sided perspective and influenced the generalisability of results and conclusions of this review. Future studies should involve a greater variety of IPED users, including non-athletes, as well as represent all areas of Switzerland.
In this scoping literature review on IPED use and users among Swiss sportspeople, we have demonstrated that the use of these substances is prevalent among athletes, recreational bodybuilders and gym users. Many different substances are used in that context. The major method of obtaining information about these substances and obtaining the substances themselves appears to be the Internet. We have demonstrated that substantial proportions of these substances may be fake and as such they put the user at unpredictable risk when consuming them. The individual and public health impact of IPEDs among this growing, often insufficiently informed, and hard-to-reach user community in Switzerland may be substantial. There is considerable need and opportunity for future prevention, harm reduction and treatment programmes for this growing and hard- to-reach user community. The use of anabolic androgenic steroids and other IPEDs affect tens of millions of individuals worldwide and their use belongs to the newest of the world’s major substance use disorders. Image- and performance-enhancing drug use as substance use disorder is currently a widely neglected area in medicine in Switzerland and worldwide. Current Swiss doping policies should be critically reviewed, as simple medical care and evidence-based treatment for non-athlete IPED users is excessively criminalised under current legislation, leaving possibly over 200,000 IPED users in Switzerland with inadequate medical care. Furthermore, the policies do not appear to prevent the number of non-athlete IPED users from growing, but actively hinder adequate medical care for these individuals, contradicting the established Swiss drug policy for other illegal substances.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest was disclosed.
1. Mullen C, Whalley BJ, Schifano F, Baker JS. Anabolic androgenic steroid abuse in the United Kingdom: an update. Br J Pharmacol. 2020 May;():2180–98. 10.1111/bph.14995
2. Kanayama G, Pope HG Jr. History and epidemiology of anabolic androgens in athletes and non-athletes. Mol Cell Endocrinol. 2018 Mar;:4–13. 10.1016/j.mce.2017.02.039
3. Hilkens L, Cruyff M, Woertman L, Benjamins J, Evers C. Social Media, Body Image and Resistance Training: Creating the Perfect ‘Me’ with Dietary Supplements, Anabolic Steroids and SARM’s. Sports Med Open. 2021 Nov;():81. 10.1186/s40798-021-00371-1
4. Piacentino D, Kotzalidis GD, Del Casale A, Aromatario MR, Pomara C, Girardi P, et al. Anabolic-androgenic steroid use and psychopathology in athletes. A systematic review. Curr Neuropharmacol. 2015 Jan;():101–21. 10.2174/1570159X13666141210222725
5. Ip EJ, Lu DH, Barnett MJ, Tenerowicz MJ, Vo JC, Perry PJ. Psychological and physical impact of anabolic-androgenic steroid dependence. Pharmacotherapy. 2012 Oct;():910–9. 10.1002/j.1875-9114.2012.01123
6. World Anti-Doping Agency (WADA). Prohibited List 2021. Internet: https://www.wada-ama.org/sites/default/files/resources/files/2021list_en.pdf (Accessed: 30.12.2022).
7. Bonnecaze AK, O’Connor T, Aloi JA. Characteristics and Attitudes of Men Using Anabolic Androgenic Steroids (AAS): A Survey of 2385 Men. Am J Men Health. 2020;():1557988320966536. 10.1177/1557988320966536
8. Bhasin S, Storer TW, Berman N, Callegari C, Clevenger B, Phillips J, et al. The effects of supraphysiologic doses of testosterone on muscle size and strength in normal men. N Engl J Med. 1996 Jul;():1–7. 10.1056/NEJM199607043350101
9. Storer TW, Magliano L, Woodhouse L, Lee ML, Dzekov C, Dzekov J, et al. Testosterone dose-dependently increases maximal voluntary strength and leg power, but does not affect fatigability or specific tension. J Clin Endocrinol Metab. 2003 Apr;():1478–85. 10.1210/jc.2002-021231
10. Rahnema CD, Lipshultz LI, Crosnoe LE, Kovac JR, Kim ED. Anabolic steroid-induced hypogonadism: diagnosis and treatment. Fertil Steril. 2014 May;():1271–9. 10.1016/j.fertnstert.2014.02.002
11. Nieschlag E, Vorona E. Doping with anabolic androgenic steroids (AAS): adverse effects on non-reproductive organs and functions. Rev Endocr Metab Disord. 2015 Sep;():199–211. 10.1007/s11154-015-9320-5
12. Christou MA, Christou PA, Markozannes G, Tsatsoulis A, Mastorakos G, Tigas S. Effects of Anabolic Androgenic Steroids on the Reproductive System of Athletes and Recreational Users: A Systematic Review and Meta-Analysis. Sports Med. 2017 Sep;():1869–83. 10.1007/s40279-017-0709-z
13. Fink J, Schoenfeld BJ, Hackney AC, Matsumoto M, Maekawa T, Nakazato K, et al. Anabolic-androgenic steroids: procurement and administration practices of doping athletes. Phys Sportsmed. 2019 Feb;():10–4. 10.1080/00913847.2018.1526626
14. Magnolini R, Falcato L, Cremonesi A, Schori D, Bruggmann P. Fake anabolic androgenic steroids on the black market - a systematic review and meta-analysis on qualitative and quantitative analytical results found within the literature. BMC Public Health. 2022 Jul;():1371. 10.1186/s12889-022-13734-4
15. Sagoe D, McVeigh J, Bjørnebekk A, Essilfie MS, Andreassen CS, Pallesen S. Polypharmacy among anabolic-androgenic steroid users: a descriptive metasynthesis. Subst Abuse Treat Prev Policy. 2015 Mar;():12. 10.1186/s13011-015-0006-5
16. Iff S, Butzke I, Zitzmann M, Schneiter R, Hunziker M, Quednow BB, et al. [IPED Use in Recreational Sports]. Praxis (Bern 1994). 2022;111(6):345-9.
17. Pope HG Jr, Kanayama G, Athey A, Ryan E, Hudson JI, Baggish A. The lifetime prevalence of anabolic-androgenic steroid use and dependence in Americans: current best estimates. Am J Addict. 2014;():371–7. 10.1111/j.1521-0391.2013.12118.x
18. Sagoe D, Molde H, Andreassen CS, Torsheim T, Pallesen S. The global epidemiology of anabolic-androgenic steroid use: a meta-analysis and meta-regression analysis. Ann Epidemiol. 2014 May;():383–98. 10.1016/j.annepidem.2014.01.009
19. McBride JA, Carson CC 3rd, Coward RM. The Availability and Acquisition of Illicit Anabolic Androgenic Steroids and Testosterone Preparations on the Internet. Am J Men Health. 2018 Sep;():1352–7. 10.1177/1557988316648704
20. Andrea C. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation . Ann Intern Med. 2018 ; 169 : 467-473 . [Epub ahead of print 4 September 2018]. doi:
21. Greenhalgh T, Peacock R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sources. BMJ. 2005 Nov;():1064–5. 10.1136/bmj.38636.593461.68
22. Wikipedia contributors. (2022, December 6). Athlete. In Wikipedia, The Free Encyclopedia. Retrieved 09:24, January 14, 2023, from https://en.wikipedia.org/w/index.php?title=Athlete&oldid=1125863214
23. Nocelli L, Kamber M, François Y, Gmel G, Marti B. Discordant public perception of doping in elite versus recreational sport in Switzerland. Clin J Sport Med. 1998 Jul;():195–200. 10.1097/00042752-199807000-00006
24. Bélanger RE, Ohl F, Berchtold A, Lentillon-Kaestner V, Suris JC. Substance use among adolescents in the French-speaking part of Switzerland. Lausanne: IUMSP; 2010. 51 pp.
25. Weber C, Kamber M, Lentillon-Kaestner V. Are doping substances imported into Switzerland mainly to increase athletic performance. Perform Enhanc Health. 2016;():66–76. 10.1016/j.peh.2016.06.001
26. Gebert A, Stamm H, Kamber M, Lamprecht M. The fight against doping from the perspective of Swiss athletes and coaches. Schweizerische Zeitschrift für Sportmedizin & Sporttraumatologie. 2019;():50–6.
27. Mettler S, Lehner G, Morgan G. Widespread Supplement Intake and Use of Poor Quality Information in Elite Adolescent Swiss Athletes. Int J Sport Nutr Exerc Metab. 2022 Jan;():41–8. 10.1123/ijsnem.2021-0043
28. Stamm H, Stahlberger M, Gebert A, Lamprecht M, Kamber M. Supplemente, Medikamente und Doping im Freizeitsport. Schweizerische Zeitschrift für. Sportmedizin und Sporttraumatologie. 2011;():122–6.
29. Lentillon-Kaestner V, Ohl F. Can we measure accurately the prevalence of doping? Scand J Med Sci Sports. 2011 Dec;():e132–42. 10.1111/j.1600-0838.2010.01199.x
30. Lentillon-Kaestner V, Becholey S, Romand P, Ohl F. Pratique sportive et conduites dopantes chez les jeunes Suisses romands. 2009; Internet: https://serval.unil.ch/resource/serval:BIB_8E0FDC205961.P001/REF (Accessed: 14.01.2023)
31. Weber C, Kamber M, Lentillon-Kaestner V, Krug O, Thevis M. Seizures of doping substances at the Swiss Border—a descriptive investigation. Forensic Sci Int. 2015 Dec;:359–68. 10.1016/j.forsciint.2015.10.001
32. Lentillon-Kaestner V, Hagger MS, Hardcastle S. Health and doping in elite-level cycling. Scand J Med Sci Sports. 2012 Oct;():596–606. 10.1111/j.1600-0838.2010.01281.x
33. Coquet R, Roussel P, Ohl F. Understanding the Paths to Appearance- and Performance-Enhancing Drug Use in Bodybuilding. Front Psychol. 2018 Aug;:1431. 10.3389/fpsyg.2018.01431
34. Lentillon-Kaestner V, Carstairs C. Doping use among young elite cyclists: a qualitative psychosociological approach. Scand J Med Sci Sports. 2010 Apr;():336–45. 10.1111/j.1600-0838.2009.00885.x
35. Brissonneau C, Defrance J, Fincoeur B, Lentillon‐Kaestner V, Ohl F. Carrière sportive et socialisation secondaire en cyclisme sur route: les cas de la Belgique, la France et la Suisse. 2009. 132, Université de Lausanne, ISSUL- Faculté des SSP. Internet: https://www.wada-ama.org/sites/default/files/resources/files/wada_cyclisme_suisse-belgique-france_ohl_rapport_final.pdf (Accessed: 14.01.2023).
36. Lentillon-Kaestner V. Doping use and deviance in Swiss n ational and international elite cycling. Perform Enhanc Health. 2014;():167–74. 10.1016/j.peh.2015.09.004
37. Weber C, Krug O, Kamber M, Thevis M. Qualitative and Semiquantitative Analysis of Doping Products Seized at the Swiss Border. Subst Use Misuse. 2017 May;():742–53. 10.1080/10826084.2016.1263665
38. Kamber M, Baume N, Saugy M, Rivier L. Nutritional supplements as a source for positive doping cases? Int J Sport Nutr Exerc Metab. 2001 Jun;():258–63. 10.1123/ijsnem.11.2.258
39. Baume N, Mahler N, Kamber M, Mangin P, Saugy M. Research of stimulants and anabolic steroids in dietary supplements. Scand J Med Sci Sports. 2006 Feb;():41–8. 10.1111/j.1600-0838.2005.00442.x
40. Bates G. Image and Performance Enhancing Drugs 2015 Survey Results. In: Mcveigh J, editor. 2016.
41. Leone JE, Sedory EJ, Gray KA. Recognition and treatment of muscle dysmorphia and related body image disorders. J Athl Train. 2005;():352–9.
42. Cerea S, Bottesi G, Pacelli QF, Paoli A, Ghisi M. Muscle Dysmorphia and its Associated Psychological Features in Three Groups of Recreational Athletes. Sci Rep. 2018 Jun;():8877. 10.1038/s41598-018-27176-9
43. Halioua R, Deutschmann M, Vetter S, Jäger M, Seifritz E, Claussen MC. Muskeldysmorphie. Swiss Med Forum. 2019;19(0910):153-158.
44. Solimini R, Rotolo MC, Mastrobattista L, Mortali C, Minutillo A, Pichini S, et al. Hepatotoxicity associated with illicit use of anabolic androgenic steroids in doping. Eur Rev Med Pharmacol Sci. 2017 Mar;( Suppl):7–16.
45. Anawalt BD. Diagnosis and Management of Anabolic Androgenic Steroid Use. J Clin Endocrinol Metab. 2019 Jul;():2490–500. 10.1210/jc.2018-01882
46. Seitz NN, John L, Atzendorf J, Rauschert C, Kraus L. Kurzbericht Epidemio- logischer Suchtsurvey 2018. Tabellenband: Medikamenteneinnahme und Hinweise Kon- sumabhängigkeit und -missbrauch nach Geschlecht und Alter im Jahr 2018. München: IFT Institut für Therapieforschung; 2019.
47. Bates G, Van Hout MC, Teck JT, McVeigh J. Treatments for people who use anabolic androgenic steroids: a scoping review. Harm Reduct J. 2019 Dec;():75. 10.1186/s12954-019-0343-1
48. Hope VD, McVeigh J, Marongiu A, Evans-Brown M, Smith J, Kimergård A, et al. Prevalence of, and risk factors for, HIV, hepatitis B and C infections among men who inject image and performance enhancing drugs: a cross-sectional study. BMJ Open. 2013 Sep;():e003207. 10.1136/bmjopen-2013-003207
49. Hope VD, McVeigh J, Marongiu A, Evans-Brown M, Smith J, Kimergård A, et al. Injection site infections and injuries in men who inject image- and performance-enhancing drugs: prevalence, risks factors, and healthcare seeking. Epidemiol Infect. 2015 Jan;():132–40. 10.1017/S0950268814000727
50. Federal Office of Public Health (FOPH). National Strategy on Addiction. Internet: https://www.bag.admin.ch/bag/en/home/strategie-und-politik/nationale-gesundheitsstrategien/strategie-sucht.html (Accessed 07.01.2023).
51. Santo T Jr, Clark B, Hickman M, Grebely J, Campbell G, Sordo L, et al. Association of Opioid Agonist Treatment With All-Cause Mortality and Specific Causes of Death Among People With Opioid Dependence: A Systematic Review and Meta-analysis. JAMA Psychiatry. 2021 Sep;():979–93. 10.1001/jamapsychiatry.2021.0976
52. Frude E, McKay FH, Dunn M. A focused netnographic study exploring experiences associated with counterfeit and contaminated anabolic-androgenic steroids. Harm Reduct J. 2020 Jun;():42. 10.1186/s12954-020-00387-y
53. Maghsoudi N, Tanguay J, Scarfone K, Rammohan I, Ziegler C, Werb D, et al. Drug checking services for people who use drugs: a systematic review. Addiction. 2022 Mar;():532–44. 10.1111/add.15734
54. Butterfield RJ, Barratt MJ, Ezard N, Day RO. Drug checking to improve monitoring of new psychoactive substances in Australia. Med J Aust. 2016 Mar;():144–5. 10.5694/mja15.01058
55. Measham FC. Drug safety testing, disposals and dealing in an English field: exploring the operational and behavioural outcomes of the UK’s first onsite ‘drug checking’ service. Int J Drug Policy. 2019 May;:102–7. 10.1016/j.drugpo.2018.11.001
56. Hungerbuehler I, Buecheli A, Schaub M. Drug Checking: A prevention measure for a heterogeneous group with high consumption frequency and polydrug use - evaluation of zurich’s drug checking services. Harm Reduct J. 2011 Jun;():16. 10.1186/1477-7517-8-16
57. Korf D, Benschop A, Rabes M. Pill testing, ecstasy and prevention: a scientific evaluation in three European cities. Amsterdam: Rozenberg; 2002.
58. La Mantia A, Oechslin L, Duarte M, Laubereau B, Fabian C. Studie zu den Effekten der Drug-Checking-Angebote in der Schweiz. Bericht zuhanden des Bundesamts für Gesundheit (BAG). Luzern, Muttenz: Interface Politikstudien Forschung Beratung und Fachhochschule Nordwestschweiz FHNW; 2020.
59. Bonnecaze AK, O’Connor T, Burns CA. Harm Reduction in Male Patients Actively Using Anabolic Androgenic Steroids (AAS) and Performance-Enhancing Drugs (PEDs): a Review. J Gen Intern Med. 2021 Jul;():2055–64. 10.1007/s11606-021-06751-3
60. Smit DL, de Ronde W. Outpatient clinic for users of anabolic androgenic steroids: an overview. Neth J Med. 2018 May;():167.
61. Iff S, Butzke I, Quednow B, Gupta R, Imboden C, Claussen M. (2021). «Image and performance enhancing drugs» im Freizeitsport. Swiss Medical Forum, 21:843-847.
62. Butzke I, Iff S, Zitzmann M, Quednow BB, Claussen MC. Interdisciplinary and Psychiatric Treatment of Anabolic Androgenic Steroids Users. Praxis (Bern 1994). 2022;111(6):e339-e44. 10.1024/1661-8157/a003868
63. Amaral JM, Kimergård A, Deluca P. Prevalence of anabolic steroid users seeking support from physicians: a systematic review and meta-analysis. BMJ Open. 2022 Jul;():e056445. 10.1136/bmjopen-2021-056445
64. Diethelm D, Ege G, Claussen MC, Iff S. The criminal liability of health care professionals treating anabolic steroid users under the SpoPA. Sports Psychiatry [Internet]. 2022 Nov;():157–66. [cited 2022 Nov 19]. 10.1024/2674-0052/a000029
65. Kamber M, Alampi G, Marti B. Arzneimittelgebrauch im Breitensport: vergleich von Ausdauersportlern und beruflich körperlich Aktiven. Schweizerische Zeitschrift für Sportmedizin und Sporttraumatologie. 2000;:76–9.
The appendix is available in the pdf version of the article.