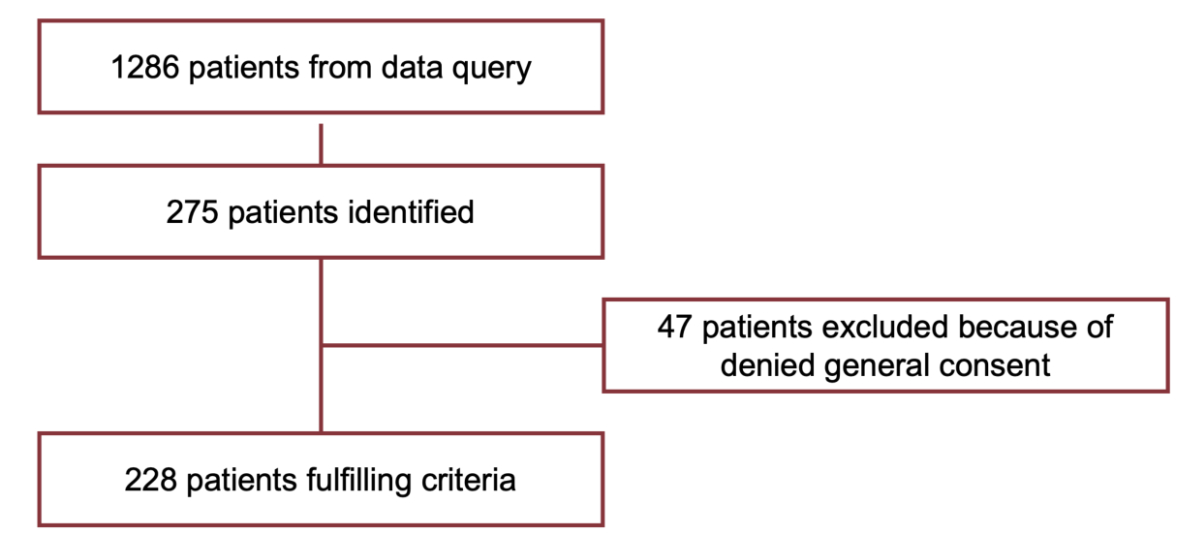
Figure 1 Study flow chart.
DOI: https://doi.org/https://doi.org/10.57187/smw.2023.40077
Travelling to another country for medical treatment is appealing due to the potentially lower costs but when complications arise post-procedure, such “bargains” are not as cost-effective as they first seemed. Patients often require follow-up care once they return home thereby burdening their home country’s healthcare system [1]. In particular, complications such as wound infection or wound healing disorders sometimes require a long period to achieve closure, as well as several visits for outpatient treatment. Over the past decade, patients seeking medical care abroad have been observed in Europe, South America, the USA and Asia [2] with patients attracted by lower costs, the quality of medical care and medical procedures not approved elsewhere [3–5]. Paraskou and George reported patients seeking cross-border reproductive care may be motivated by legislative restrictions on fertility treatment in their home country [6], whereas Bookman et al. reported a financial saving of 40% to 90% for patients for comparable procedures [7]. Regarding cosmetic surgery, a multifaceted project in which patients were accompanied on their travels abroad showed a well-organised market with agents acting as brokers between patients and surgeons [8]. Attractive offers, more affordable procedures and shorter waiting lists seem to deemphasise the client’s risks and concerns [9, 10]. A Canadian study by Penney et al. demonstrated the lack of information on websites regarding procedural and medical risks [11]. Inadequately informed patients are susceptible to falling for the lure and potentially exposing themselves to danger [12, 13]. Consequently, an unknown number of patients seek medical attention in their home countries due to complications. In a time of increasing financial pressure on the national healthcare system, costs resulting from cosmetic surgery tourism may have a considerable impact. Indeed, a recent American study of the expenses of treated complications showed that only 63% of the bill receivables demanded by clinics and 9% demanded by physicians were covered through insurance or the patients themselves [13]. Also, a study at the University Hospital Zurich reported a marginal profit of 3.6% for the treatment of complications from abroad between 2010 to 2014 [1].
This study constitutes a follow-up of a previous study “Complications after cosmetic surgery”, published by our group in 2016 [1]. An exponential trend of treated complications was observed from 2010 to 2014. The present study documented the development of complications resulting from procedures performed abroad and compared them to those performed in Switzerland which were subsequently treated at the University Hospital Zurich between 2015 and 2019.
The Ethics Committee declared that the decision of approval does not fall within its jurisdiction (BASEC-Nr. 2019-02298) and the data usage rights from the general consent of the University Hospital of Zurich are applicable. All patients who did not give consent and individuals younger than 18 years of age were excluded from this study (47 patients). The patients were retrospectively identified based on a data query of the clinical information system (figure 1). The terms for data retrieval were determined by the first two authors and the first author collected the data by revising patients’ records twice. Any irregularities or uncertainties were discussed by the first two authors.
Figure 1 Study flow chart.
Patients treated at the University Hospital Zurich for complications following aesthetic procedures performed domestically or abroad were included in the study. Patients without information regarding the location of performed procedure were excluded from further analysis. The complications included: wound breakdown, infections, hematoma, seroma, tissue necrosis, capsular fibrosis, implant rupture or dislocation, residual thread material, foreign body granuloma, dissatisfaction, pain, or simple postoperative follow-up care. The data collected included patient-related information (age, sex, height, weight, smoking, or diabetes), date of consultation and operation, the procedure performed and the geographical data, as well as consecutive complication and treatment-related information. The procedures performed were breast surgery (augmentation, mastopexy, reduction plasty, change of implants), body contouring (liposuction, abdominoplasty, brachioplasty), facial surgery (otoplasty, blepharoplasty, facelift), injections (botulinum toxin, fillers) and others (e.g., hair transplantation, scar revision). The type of complication according to time of occurrence was classified as follows: early <30 days, midterm 30–180 days and late >180 days. The physiology of the healing process serves as the foundation for this classification and as a matter of comparability, the groups correspond to the previous study by Klein et al [1].
The costs were analysed by the hospital’s commissioning team with “Tarmed” and “Swiss Diagnosis Related Group (SwissDRG)” codes used for the direct cost analysis of the treatment in respect of outpatients and inpatients [14, 15]. Tarmed is a billing system based on individual services in the outpatient setting [14] and the SwissDRG system is based on flat-rate remuneration for the diseases presented [15]. The total expenses were compared with the contribution margins and the total costs for all treatments were calculated using the exchange rate on 31st August 2021: 1 CHF = 1.09 USD. Data analysis and visualisation were performed with IBM SPSS Statistics Version 27 for Macintosh. Descriptive statistics are presented as count (percentage) for discrete values and mean ± standard deviation (SD) or median [interquartile range (IQR)] for continuous values.
A total of 228 patients were identified from January 2015 to the end of December 2019 including 207 (91%) females and 21 (9%) males. The mean female age was 40.9 ± 12.0 years (range 19–74 years) whereas the male mean age was 34.3 ± 8.9 years (range 21–50 years). At the time of surgery, the mean age of women was 36.1 ± 11.4 years whilst most men were 32.6 ± 8.3 years. Patients younger than 18 years were not presented reflecting the general recommendation to perform aesthetic procedures only in adults.
Of our population, 187 (82%) patients presented secondary to cosmetic procedures abroad and 36 (16%) with complications after cosmetic surgery in Switzerland (figure 2).
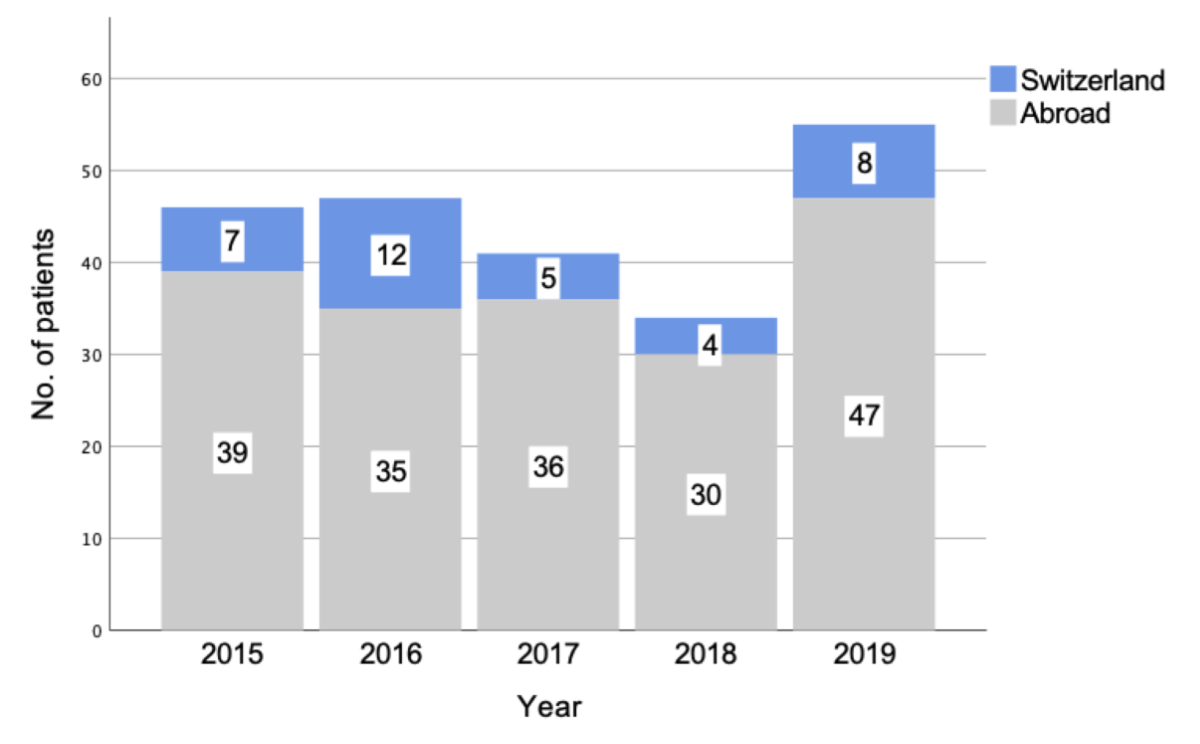
Figure 2 Number of annualy treated complications after cosmetic surgery abroad or in Switzerland.
The primary country where surgery was performed was unknown in 5 (2%) patients, with most procedures performed in Europe (69%) and the most frequently visited countries were Turkey (16%), the Czech Republic (13.4%), Brazil (13.4%) and Germany (11.2%) (table 1).
Table 1Number of performed procedures per country.
| Visited continents | No. of patients | Breast surgery | Body contouring | Facial surgery | Injections | Others | |||||
| Percentage of patients | No. of patients | Percentage of patients | No. of patients | Percentage of patients | No. of patients | Percentage of patients | No. of patients | Percentage of patients | No. of patients | ||
| America | |||||||||||
| Brazil | 25 | 18 | 58.1% | 4 | 50.0% | 1 | 25.0% | 2 | 50.0% | 0 | – |
| Colombia | 8 | 4 | 12.9% | 2 | 25.0% | 1 | 25.0% | 1 | 25.0% | 0 | – |
| Dominican Republic | 6 | 4 | 12.9% | 1 | 12.5% | 0 | – | 1 | 25.0% | 0 | – |
| Ecuador | 1 | 0 | – | 0 | – | 1 | 25.0% | 0 | – | 0 | – |
| Mexico | 1 | 1 | 3.2% | 0 | – | 0 | – | 0 | – | 0 | – |
| Paraguay | 1 | 1 | 3.2% | 0 | – | 0 | – | 0 | – | 0 | – |
| Peru | 1 | 1 | 3.2% | 0 | – | 0 | – | 0 | – | 0 | – |
| United States | 2 | 2 | 6.5% | 0 | – | 0 | – | 0 | – | 0 | – |
| Venezuela | 2 | 0 | – | 1 | 12.5% | 1 | 25.0% | 0 | – | 0 | – |
| Europe | |||||||||||
| Austria | 1 | 1 | 1.1% | 0 | – | 0 | – | 0 | – | 0 | – |
| Belgium | 2 | 1 | 1.1% | 1 | 3.4% | 0 | – | 0 | – | 0 | – |
| Bulgaria | 3 | 1 | 1.1% | 0 | – | 0 | – | 2 | 25.0% | 0 | – |
| Croatia | 4 | 3 | 3.2% | 1 | 3.4% | 0 | – | 0 | – | 0 | – |
| Czech Republic | 25 | 21 | 22.3% | 2 | 6.9% | 2 | 9.1% | 0 | – | 0 | – |
| France | 5 | 5 | 5.3% | 0 | – | 0 | – | 0 | – | 0 | – |
| Germany | 21 | 10 | 10.6% | 6 | 20.7% | 3 | 13.6% | 1 | 12.5% | 1 | 25.0% |
| Hungary | 6 | 5 | 5.3% | 1 | 3.4% | 0 | – | 0 | – | 0 | – |
| Italy | 3 | 1 | 1.1% | 0 | – | 1 | 4.5% | 1 | 12.5% | 0 | – |
| Lichtenstein | 1 | 1 | 1.1% | 0 | – | 0 | – | 0 | – | 0 | – |
| Poland | 1 | 1 | 1.1% | 0 | – | 0 | – | 0 | – | 0 | – |
| Portugal | 4 | 3 | 3.2% | 0 | – | 1 | 4.5% | 0 | – | 0 | – |
| Serbia | 10 | 6 | 6.4% | 3 | 10.3% | 1 | 4.5% | 0 | – | 0 | – |
| Spain | 4 | 4 | 4.3% | 0 | – | 0 | – | 0 | – | 0 | – |
| Switzerland | 36 | 17 | 18.1% | 3 | 10.3% | 11 | 50.0% | 3 | 37.5% | 2 | 50.0% |
| Turkey | 30 | 14 | 14.9% | 12 | 41.4% | 2 | 9.1% | 1 | 12.5% | 1 | 25.0% |
| United Kingdom | 1 | 0 | – | 0 | – | 1 | 4.5% | 0 | – | 0 | – |
| Asia | |||||||||||
| Azerbaijan | 1 | 0 | – | 0 | – | 1 | 33.3% | 0 | – | 0 | – |
| China | 2 | 0 | – | 1 | 100.0% | 0 | – | 1 | 20.0% | 0 | – |
| Thailand | 10 | 4 | 100.0% | 0 | – | 2 | 66.7% | 4 | 80.0% | 0 | – |
| Africa | |||||||||||
| Morocco | 2 | 1 | 25.0% | 0 | – | 0 | – | 1 | 50.0% | 0 | – |
| Tunisia | 4 | 3 | 75.0% | 0 | – | 0 | – | 1 | 50.0% | 0 | – |
| NA | |||||||||||
| NA | 5 | 3 | – | 0 | – | 0 | – | 2 | 100.0% | 0 | – |
The most frequently performed procedure in Switzerland and abroad was breast surgery (n = 17, 47% and n = 116, 62%). The second most common operation in Switzerland was facial surgery (n = 11, 31%), followed by body contouring and injections (n = 3, 8% and n = 3, 8%). Four of those who underwent facial surgery were male and one male in each group underwent body contouring and injections. The second most common operation abroad was body contouring (n = 35, 19%) followed by facial surgery and injections (n = 18, 10% and n = 16, 9%) (figure 3). Of those who underwent body contouring, six were male, three of which underwent facial procedures, four males had injections and one had a hair transplant.
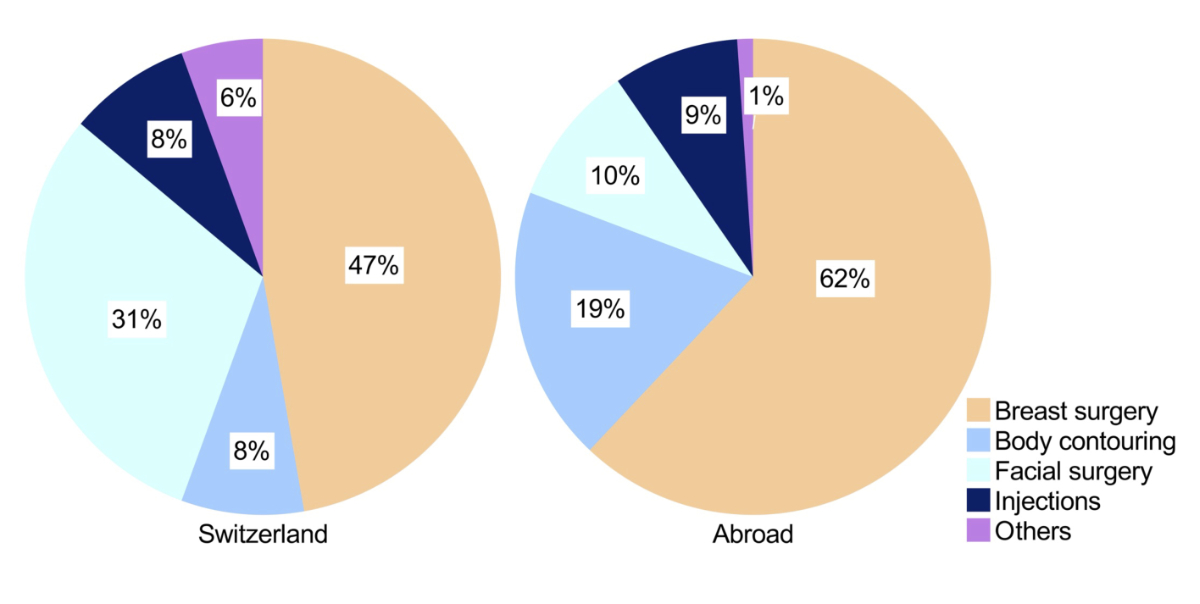
Figure 3 Percentage of performed procedures.
Of all patients who underwent cosmetic surgery abroad, most patients (n = 129, 69%) presented with a delayed complication such as persistent pain and discomfort (n = 36, 19%), dissatisfaction (n = 33, 18%), capsular fibrosis (n = 20, 11%), implant rupture or dislocation (n = 17, 9%) or due to other complications such as disturbing suture remnants, granulomas, bullous reaction, or nonspecific swelling (n = 23, 12%). Acute complications occurred in fewer patients (n = 58, 31%) with infection in 20 patients (11%), wound breakdown in 27 patients (14%), 7 patients suffered seroma (4%) and 4 patients presented with hematoma (2%).
Analogically, a similar trend was observed in the group with domestic complications, whereby most patients presented due to a non-acute complication (86%) such as dissatisfaction (n = 20, 65%), capsular contracture (n = 8, 26%), pain or discomfort (n = 2, 6%) and a bullous skin reaction after several months (n = 1, 3%). Acute complications were observed in 14% (n = 5) with infection in 2 patients and wound breakdown in 3 patients (figure 4).
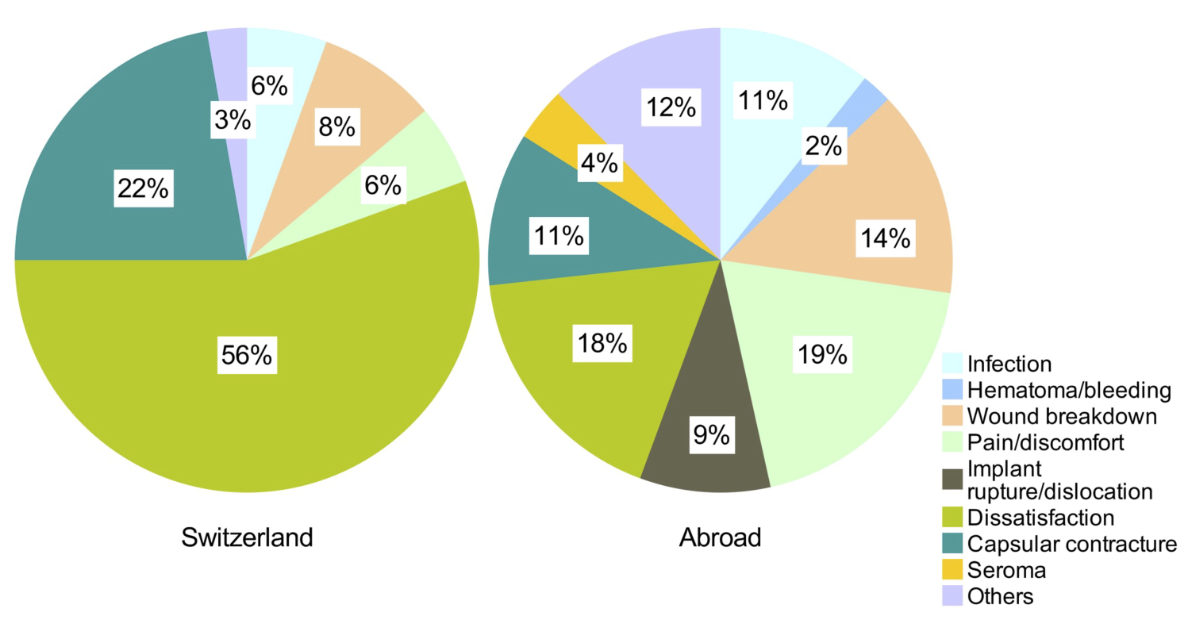
Figure 4 Percentage of presented domestic and abroad complications.
Staphylococcus aureus was the source of most infections in patients with domestic and foreign complications, with one case of ESBL microbes (Extended Spectrum Beta-Lactamase) and multi-resistant gram-negative bacteria (MRGN) in the foreign procedures group. Mycoplasma was not reported in any bacteriological samples.
The median follow-up time for complications after cosmetic surgery abroad was 566 days (IQR 2304 days), 672 days (IQR 2583 days) in Switzerland. Most patients in both groups (118, 28 respectively) presented with late complications (>180 days) with a median follow-up time of 1767 days (IQR 2890 days) after surgery abroad and 751 days (IQR 3017 days) after domestic surgery. Thirty-nine patients presented with midterm complications (30−180 days) after surgery abroad with a median follow-up time of 76 days (IQR 72 days). One patient presented with midterm complications after undergoing surgery in Switzerland after 78 days. The least frequent were patients (30 and 3 patients, respectively) with early complications (<30 days) such as infection, wound breakdown, and pain who presented with a median follow-up time of 14 days after surgery abroad and 22 days after a procedure in Switzerland (IQR 13 and 5 days).
Of the total 228 patients treated at University Hospital Zurich, 43 patients (18.9%) presented to the emergency department with a complication from abroad and one patient with a domestic complication. None of the patients was in critical condition or required intensive care.
In total, 80.2% of the patients with complications after surgery abroad were treated as outpatients, 18.2% as inpatients and 1.6% were treated as outpatients and subsequently as inpatients. Of the domestic complications, 72.2% were treated in an outpatient setting and 27.8% as inpatients. Admission was due to a need for intravenous antibiotic therapy (3 patients), surgical debridement and intravenous antibiotic therapy (3 patients), surgical debridement (4 patients), hematoma evacuation (1 patient), or elective surgery (35 patients). Figure 5 outlines the percentage of patients receiving therapy according to the treatment setting excluding patients who presented only for a single outpatient visit and figure 6 presents the required treatments.
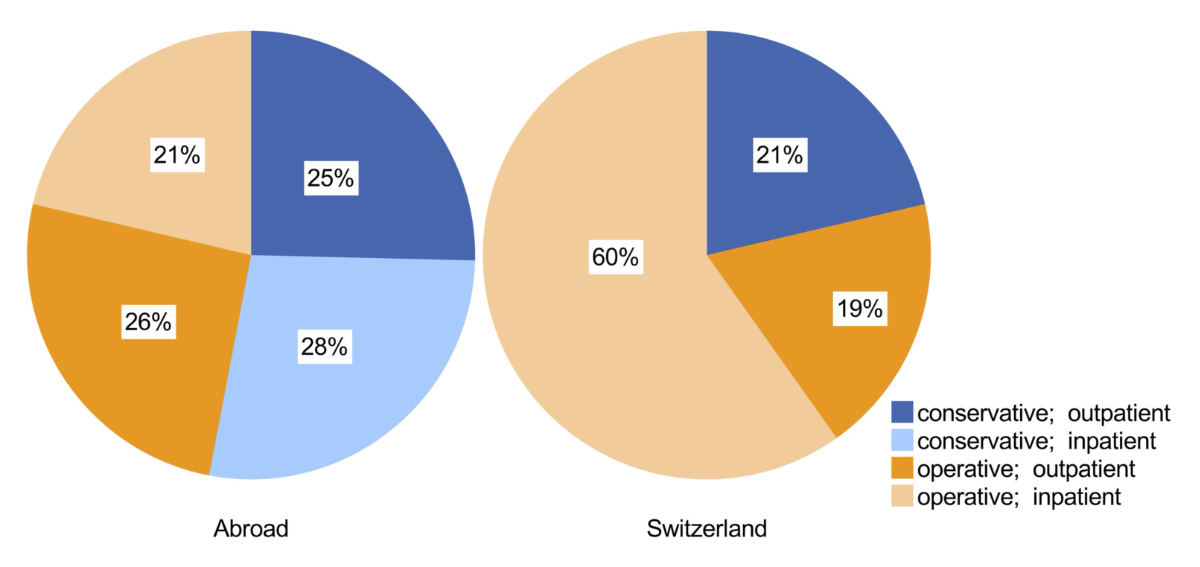
Figure 5 Percentage of received therapy according to treatment setting, excluding patients who presented only for consultation.
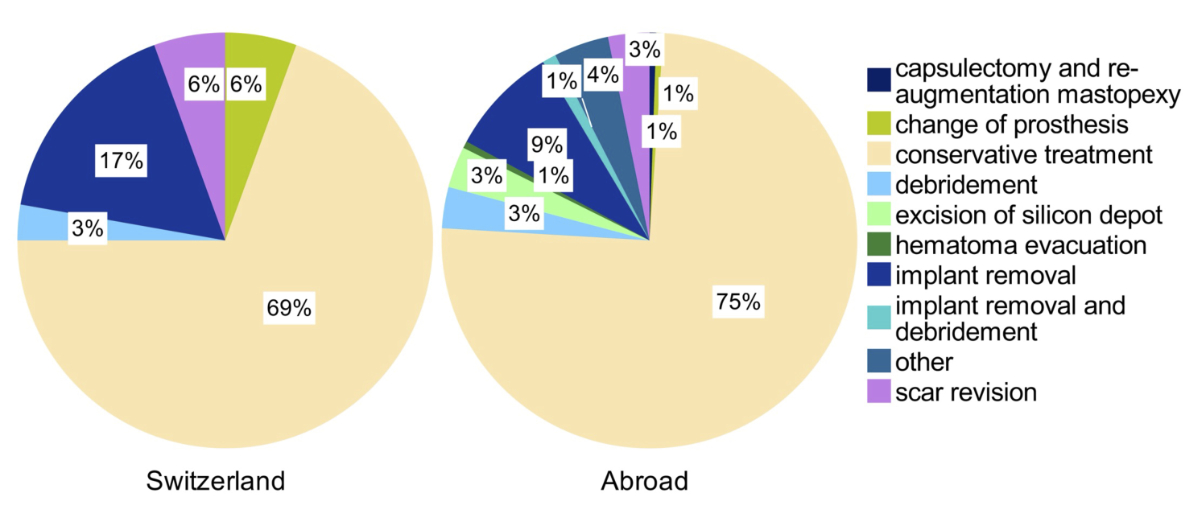
Figure 6 Received treatment.
The treatment costs of the 187 treated complications after surgery abroad amounted to $ 578,238, while the overall reimbursement was $ 610,297 resulting in a financial gain of $ 32,059 for the hospital (table 2).
Table 2Average and total costs of cases from Switzerland and abroad.
| Switzerland | Abroad | |||
| Average costs per patient | Total | Average costs per patient | Total | |
| Arising costs | $ 3538 | $ 127,358 | $ 3092 | $ 578,238 |
| Reimbursement | $ 5147 | $ 185,277 | $ 3264 | $ 610,297 |
| Revenue | $ 1609 | $ 57,919 | $ 171 | $ 32,059 |
The average cost per patient was $ 3092 for the group who had surgery abroad, with an average cost per patient who presented to the emergency department of $ 4219 compared to $ 2756 per patient presenting to the outpatient clinic (table 3).
Table 3Average costs of cases presented through emergency department and at our outpatient clinic.
| Switzerland | Abroad | |||||||
| Emergency department | Emergency department | |||||||
| Yes | No | Yes | No | |||||
| Average costs per patient | Total | Average costs per patient | Total | Average costs per patient | Total | Average costs per patient | Total | |
| Arising costs | $ 21,138 | $ 21,138 | $ 3035 | $ 106,220 | $ 4219 | $ 181,417 | $ 2756 | $ 396,821 |
| Reimbursement | $ 39,537 | $ 39,537 | $ 4164 | $ 145,740 | $ 3442 | $ 147,994 | $ 3210 | $ 462,303 |
| Revenue | $ 18,399 | $ 18,399 | $ 1129 | $ 39,520 | -$ 777 | -$ 33,423 | $ 455 | $ 65,482 |
There was a financial gain of $ 1484 per inpatient and a loss of $ 114 per outpatient (table 4).
Table 4Average costs of complications treated surgically and conservative.
| Switzerland | Abroad | |||||||||
| Treatment setting | Treatment setting | |||||||||
| Outpatient | Inpatient | Outpatient | Inpatient | Outpatient, subsequently inpatient | ||||||
| Average costs per patient | Total | Average costs per patient | Total | Average costs per patient | Total | Average costs per patient | Total | Average costs per patient | Total | |
| Arising costs | $ 825 | $ 21,461 | $ 10,590 | $ 105,897 | $ 811 | $ 121,624 | $ 12,960 | $ 440,655 | $ 5320 | $ 15,959 |
| Reimbursement | $ 537 | $ 13,956 | $ 17,132 | $ 171,321 | $ 697 | $ 104,584 | $ 14,445 | $ 491,118 | $ 4865 | $ 14,596 |
| Revenue | -$ 289 | -$ 7505 | $ 6542 | $ 65,425 | -$ 114 | -$ 17,040 | $ 1484 | $ 50,462 | -$ 455 | -$ 1364 |
Furthermore, the average duration of hospitalisation for inpatient treatment of foreign complications was 3 days (IQR 2 days, range 1−36 days). In the surgically treated group, the mean hospitalisation time was 3 days (range 1−36 days), compared to 5 days (range 2−7 days) in the conservatively treated group of inpatients.
For comparison, the treatment expenses of the 36 domestic complications reached $ 127,358, of which, $ 185,277 was refunded by health insurance, resulting in a financial gain of $ 57,919 for the hospital (table 2). The average cost per patient was $ 3538, with a financial gain of $ 6542 per inpatient and a loss of $ 289 per outpatient (table 4). Since only one patient presented to the emergency department, there was no calculation conducted for comparison. The average duration of hospitalisation was 2 days (IQR 1 day, range 1−3 days), where every inpatient was treated surgically.
Cosmetic surgery tourism has become a frequent topic of discussion due to its increasing popularity. Our study indicates an ongoing trend but contrary to our previous study, there was no exponential increase observed in both groups [1]. Thacoor et al. identified 24 patients in England between 2006 and 2018 who needed surgical revision after surgery abroad, 63% of whom were registered during the last 5 years of their study [16]. Although their study was small, the trend supports our findings.
The International Society of Aesthetic and Plastic Surgery (ISAPS) annual survey of 2019 recorded a total number of 11,363,569 performed surgical and non-surgical aesthetic procedures worldwide [2]. The survey collected data about the most popular countries for cosmetic tourism and their visitors’ nationality, showing that between 2016 and 2019, the most frequently visited countries by Swiss residents were Germany, France, Italy and Turkey [17, 18]. Interestingly, Germany and Turkey were two of the countries where most complications were observed. In our present population, more patients visited Europe compared to America compared to a previous study by Klein et al. [1]. Thus, our results show the increasing popularity of European countries among patients undergoing cosmetic surgery abroad.
In contrast to the study published by Klein et al., this was the first time that men with complications after aesthetic surgery were observed [1]. The American Society of Plastic surgeon report in 2018 recorded a 29% growth in procedures in men since 2000 [19], with the most popular surgical procedure among men being eyelid surgery followed by gynecomastia [20]. According to ISAPS 2019 statistics, the percentage of women and men undergoing cosmetic procedures remained stable since 2013, so we assume the trend of cosmetic surgery among Swiss men has increased [21–23], possibly due to increased social and cultural pressure [24]. The increased social media presence has resulted in an increased emphasis on physical appearance in society, consequently the pressure to look their best and resort to cosmetic procedures [25].
Most patients treated at the University Hospital Zurich between 2010 to 2014 presented with infections, followed by wound dehiscence, pain and discomfort [1] in line with many other studies [13, 12, 26, 27], whereas Miyagi et al. reported aesthetic dissatisfaction as one of the most frequent complications besides infection or dehiscence [28]. Similarly, our data showed aesthetic dissatisfaction as the major concern after pain and discomfort.
Compared to our previous study, there were almost three times as many patients with capsular contracture over the past five years than during 2010−2014 [1]. Importantly, the treatment of capsular fibrosis and postoperative complications, in general, is covered by health insurance in Switzerland. Swiss people pay monthly health insurance premiums for mandatory insurance and an annual franchise, with the insurance paying for required treatments if a disease value is presented, sometimes requiring cost approval from the insurance. Financially, it is not attractive for patients to travel abroad because of such a complication, rather they place a burden on the national healthcare system. Usually, this does not include the insertion of new implants or mastopexy when capsule/implant removal is performed. The aesthetic part of the surgery must be paid for by the patient, which is why some patients seek surgery abroad after consultation at our department.
More foreign complications were treated as outpatients than as inpatients, with a shorter mean hospitalisation time than in our previous study [1]. This may reflect the current development in our healthcare system forcing hospitals to reduce inpatient stays [29]. The mean hospital stay for conservatively treated infections was remarkably shorter compared to the average length of hospital stay of the conservatively treated group in the study of Adabi et al. (5 vs. 13 days) [30]. They compared the length of hospital stay and arising costs according to early surgical management of infection. Of the twenty patients with infection, three were admitted for inpatient conservative management and eleven patients were treated conservatively but not as inpatients, with six patients treated surgically as inpatients (n = 4) and outpatients (n = 2). In contrast to Adabi et al., we did not evaluate the severity of the infection, therefore, we cannot assume that our efficient management of infection is mainly due to outpatient care or early surgical management.
Considering that treatment in the emergency department causes higher treatment costs, it is part of a cost-efficient treatment to refer the patients to the outpatient clinic whenever medically justifiable. Even though just 2.8% of the patients with complications arising from domestic surgery presented to the emergency department, the average cost per patient of the domestic group was higher compared to the abroad group. This is explained by complications arising after inland surgery encompassing fewer acute cases, resulting in treatment by elective surgery with a regulated SwissDRG-related reimbursement [15]. The calculated rate does not cover the costs completely in all cases, so the expenses must be covered by the hospital. In countries without compulsory health insurance, unlike Switzerland, hospitals bear much more of the incurred costs [31].
Travel has serious effects on colonisation with uncommon bacteria. As observed in other studies, many patients presenting with infection have uncommon or multidrug-resistant bacteria [32, 13]. Khawaja et al. investigated the colonisation rate of travellers with multidrug-resistant bacteria and their origin, showing higher rates of multidrug-resistant bacteria carriers among travellers to (sub)tropical countries [33]. In contrast to our previous study [1], there was no evidence of mycobacteria in the present study. The absolute number of patients travelling to South America was higher in the current study but fewer infections originated from South America (3 vs. 9 patients, respectively) [1], indicating that a higher hygienic standard has been established in South America, resulting in fewer surgical site infections. Since infection with uncommon bacteria is more often observed in those who have travelled to low-income and developing countries [33], domestic clinicians must still hold a low threshold to test for these bacteria when it comes to postoperative infections from abroad [33]. Targeted antibiotic treatments are essential, as well as the prevention of further resistance [32, 34].
Both surgical and inpatient treatments are associated with higher costs but also lead to more reimbursement from health insurance based on the performance-related “flat rates” (SwissDRG-System) [29, 15]. A slightly higher proportion of the domestic group was treated surgically (31% vs. 26%), but interestingly, the total financial gain per inpatient of the domestic group was significantly higher than for the abroad group ($ 6542 vs. $ 1484). We assume that Swiss patients who can afford cosmetic surgery in Switzerland are additionally covered by non-mandatory supplementary insurance for which they pay a surcharge. In return, hospitals receive more reimbursement for the treatment of additionally insured patients, with a significant portion of hospital costs covered by patients holding private health insurance [35].
Overall, there was a similar gain per patient, comparing the previous and the present study, while the loss per outpatient was less. The total gain for the treatment of 187 patients was $ 32,059 in the present study and $ 20,000 for 105 patients in the previous period, resulting in a 60% increase. Over the observed period from 2015 to the end of 2019, there was a diminished loss per treated outpatient and a slightly higher gain in total, indicating an improved cost-efficient treatment. From a global perspective, it should be mentioned that if a hospital does not record any losses, the treatment of complications still places a significant burden on the national healthcare system by straining the health insurance companies. In addition, patients who presented due to dissatisfaction with the aesthetic results were treated on a self-pay basis, as these treatments were not covered by health insurance.
The most predominant limitation of our study is the single-centre design providing data from one plastic surgery unit followed by the retrospective nature. Despite the limitation of our data, the analysis is a very important component for the early identification of a potentially dangerous trend and from external validity. We strongly recommend that every plastic surgery unit observes this population of patients over the years. There is a lack of methods to record all patients travelling for cosmetic tourism, as there is no law obligating patients to report their venture. Forty-seven patients with complications after cosmetic surgery were excluded because they did not provide consent. While severe cases might be those who did not provide consent, more cases were handled externally leading to an unknown number of complications. Switzerland lists 290 hospitals, of which, 37% are for primary care and 63% are specialised clinics such as psychiatric wards or rehabilitation clinics [36]. Despite representing one of the largest plastic surgery units in Switzerland, there are many other hospitals besides the University Hospital Zurich treating complications after cosmetic surgery tourism and not reporting them, therefore only a national reporting system could reveal the actual number of complications after cosmetic surgery abroad.
In conclusion, the number of complications as a result of cosmetic surgery tourism has remained steady over the last five years, potentially due to ameliorated patient care with higher hygienic standards abroad leading to fewer acute complications. For the first time, a remarkable number of men with complications from cosmetic procedures was observed. Pain and discomfort as well as dissatisfaction with aesthetic results or wound breakdown remain the main complaints, with cost-efficient treatment achieved if emergency admission is avoided.
Presented at the Annual Congress of the Swiss Society for Plastic, Reconstructive, and Aesthetic Surgery (SGPRAC) in Lausanne, Switzerland in September 2020.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. Nicole Lindenblatt acts as scientific advisor and symposium speaker for Medical Microinstruments (MMI). No other potential conflict of interest was disclosed.
1. Klein HJ , Simic D , Fuchs N , Schweizer R , Mehra T , Giovanoli P , et al. Complications After Cosmetic Surgery Tourism. Aesthet Surg J. 2017 Apr;37(4):474–82. https://doi.org/10.1093/asj/sjw198
2. Global-Survey-2019.pdf. Accessed March 31, 2021. https://www.isaps.org/wp-content/uploads/2020/12/Global-Survey-2019.pdf
3. Hanefeld J , Lunt N , Smith R , Horsfall D . Why do medical tourists travel to where they do? The role of networks in determining medical travel. Soc Sci Med. 2015 Jan;124:356–63. https://doi.org/10.1016/j.socscimed.2014.05.016
4. Chen LH , Wilson ME . The globalization of healthcare: implications of medical tourism for the infectious disease clinician. Clin Infect Dis. 2013 Dec;57(12):1752–9. https://doi.org/10.1093/cid/cit540
5. Foley BM , Haglin JM , Tanzer JR , Eltorai AE . Patient care without borders: a systematic review of medical and surgical tourism. J Travel Med. 2019 Sep;26(6):taz049. https://doi.org/10.1093/jtm/taz049
6. Paraskou A , George BP . The market for reproductive tourism: an analysis with special reference to Greece. Glob Health Res Policy. 2017 Jun;2(1):16. https://doi.org/10.1186/s41256-017-0037-8
7. Bookman MZ , Bookman KR . Medical Tourism in Developing Countries. Palgrave Macmillan, US; 2007. https://doi.org/10.1057/9780230605657
8. Sun-Sea-Final-Report.pdf. Accessed July 30, 2020. http://1n1xkd2j1u702vcxsr1pe3h6.wpengine.netdna-cdn.com/files/2012/11/Sun-Sea-Final-Report.pdf
9. Eissler LA , Casken J . Seeking health care through international medical tourism. J Nurs Scholarsh. 2013 Jun;45(2):177–84. https://doi.org/10.1111/jnu.12014
10. Alleman BW , Luger T , Reisinger HS , Martin R , Horowitz MD , Cram P . Medical tourism services available to residents of the United States. J Gen Intern Med. 2011 May;26(5):492–7. https://doi.org/10.1007/s11606-010-1582-8
11. Penney K , Snyder J , Crooks VA , Johnston R . Risk communication and informed consent in the medical tourism industry: a thematic content analysis of Canadian broker websites. BMC Med Ethics. 2011 Sep;12(1):17. https://doi.org/10.1186/1472-6939-12-17
12. Melendez MM , Alizadeh K . Complications from international surgery tourism. Aesthet Surg J. 2011 Aug;31(6):694–7. https://doi.org/10.1177/1090820X11415977
13. Venditto C , Gallagher M , Hettinger P , Havlik R , Zarb R , Argenta A , et al. Complications of Cosmetic Surgery Tourism: Case Series and Cost Analysis. Aesthet Surg J. 2021 Apr;41(5):627–34. https://doi.org/10.1093/asj/sjaa092
14. BAG B für G. Tarifsystem TARMED . Accessed January 9, 2022. https://www.bag.admin.ch/bag/de/home/versicherungen/krankenversicherung/krankenversicherung-leistungen-tarife/Aerztliche-Leistungen-in-der-Krankenversicherung/Tarifsystem-Tarmed.html
15. BAG B für G. Tarifsystem SwissDRG . Accessed May 9, 2021. https://www.bag.admin.ch/bag/de/home/versicherungen/krankenversicherung/krankenversicherung-leistungen-tarife/Spitalbehandlung/Tarifsystem-SwissDRG.html
16. Thacoor A , van den Bosch P , Akhavani MA . Surgical Management of Cosmetic Surgery Tourism-Related Complications: Current Trends and Cost Analysis Study of the Financial Impact on the UK National Health Service (NHS). Aesthet Surg J. 2019 Jun;39(7):786–91. https://doi.org/10.1093/asj/sjy338
17. GlobalStatistics2016-1.pdf. Accessed March 31, 2021. https://www.isaps.org/wp-content/uploads/2017/10/GlobalStatistics2016-1.pdf
18. 2016-ISAPS-Results-1.pdf. Accessed March 31, 2021. https://www.isaps.org/wp-content/uploads/2017/10/2016-ISAPS-Results-1.pdf
19. Wednesday J . 12, MoreAddThis28 ASB to F to T to L to. More Men Undergo Plastic Surgery as the Daddy-Do-Over Trend Rises in Popularity. American Society of Plastic Surgeons. Accessed May 9, 2021. https://www.plasticsurgery.org/news/press-releases/more-men-undergo-plastic-surgery-as-the-daddy-do-over-trend-rises-in-popularity
20. isaps-global-survey_2021.pdf. Accessed February 1, 2023. https://www.isaps.org/media/vdpdanke/isaps-global-survey_2021.pdf
21. ISAPS-Global-Survey-Results-2018-1.pdf. Accessed March 31, 2021. https://www.isaps.org/wp-content/uploads/2020/10/ISAPS-Global-Survey-Results-2018-1.pdf
22. 2014-ISAPS-Results-3-1.pdf. Accessed March 31, 2021. https://www.isaps.org/wp-content/uploads/2017/10/2014-ISAPS-Results-3-1.pdf
23. ISAPS_2017_International_Study_Cosmetic_Procedures_NEW.pdf. Accessed September 18, 2019. https://www.isaps.org/wp-content/uploads/2019/03/ISAPS_2017_International_Study_Cosmetic_Procedures_NEW.pdf
24. Cosmetic surgery in men. doi:https://doi.org/10.1002/tre.761
25. Hopkins ZH , Moreno C , Secrest AM . Influence of Social Media on Cosmetic Procedure Interest. J Clin Aesthet Dermatol. 2020 Jan;13(1):28–31. [cited 2023 Jan 29] Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7028372/
26. Brightman L , Ng S , Ahern S , Cooter R , Hopper I . Cosmetic tourism for breast augmentation: a systematic review. ANZ J Surg. 2018 Sep;88(9):842–7. https://doi.org/10.1111/ans.14326
27. Pereira RT , Malone CM , Flaherty GT . Aesthetic journeys: a review of cosmetic surgery tourism. J Travel Med. 2018 Jun;25(1): https://doi.org/10.1093/jtm/tay042
28. Miyagi K , Auberson D , Patel AJ , Malata CM . The unwritten price of cosmetic tourism: an observational study and cost analysis. J Plast Reconstr Aesthet Surg. 2012 Jan;65(1):22–8. https://doi.org/10.1016/j.bjps.2011.07.027
29. BAG B für G. Ambulant vor Stationär. Accessed May 9, 2021. https://www.bag.admin.ch/bag/de/home/versicherungen/krankenversicherung/krankenversicherung-leistungen-tarife/Aerztliche-Leistungen-in-der-Krankenversicherung/ambulant-vor-stationaer.html
30. Adabi K , Stern CS , Kinkhabwala CM , Weichman KE , Garfein ES , Tepper OM , et al. Early Surgical Management of Medical Tourism Complications Improves Patient Outcomes. Plast Reconstr Surg. 2020 May;145(5):1147–54. https://doi.org/10.1097/PRS.0000000000006728
31. Livingston R , Berlund P , Eccles-Smith J , Sawhney R . The Real Cost of “Cosmetic Tourism” Cost Analysis Study of “Cosmetic Tourism” Complications Presenting to a Public Hospital. Eplasty. 2015 Jul;15:e34. [cited 2022 May 19] Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4522144/
32. Schwartz KL , Morris SK . Travel and the Spread of Drug-Resistant Bacteria. Curr Infect Dis Rep. 2018 Jun;20(9):29. https://doi.org/10.1007/s11908-018-0634-9
33. Khawaja T , Kirveskari J , Johansson S , Väisänen J , Djupsjöbacka A , Nevalainen A , et al. Patients hospitalized abroad as importers of multiresistant bacteria-a cross-sectional study. Clin Microbiol Infect. 2017 Sep;23(9):673.e1–8. https://doi.org/10.1016/j.cmi.2017.02.003
34. Cusumano LR , Tran V , Tlamsa A , Chung P , Grossberg R , Weston G , et al. Rapidly growing Mycobacterium infections after cosmetic surgery in medical tourists: the Bronx experience and a review of the literature. Int J Infect Dis. 2017 Oct;63:1–6. https://doi.org/10.1016/j.ijid.2017.07.022
35. Spitalfinanzierung. Kanton Zürich. Accessed September 5, 2021. https://www.zh.ch/de/gesundheit/spitaeler-kliniken/spitalfinanzierung.html
36. Statistik B für . Spitäler. Accessed May 19, 2021. https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/gesundheitswesen/spitaeler.html
The following terms were used for data retrieval from the patient records:
Abdominoplastik, Antibiotika, Asymmetrie, asymmetrisch, Augmentationsplastik, Augmentationsmastopexie, Blutung, Body contouring, Botox, Brustchirurgie, Brustaugmentation, Brustvergrösserung, Brustverkleinerung, Débridement, Dermolipektomie, Dislokation, Eiter, Facelift, Fieber, Filler, Gesichtschirurgie, Hämatom, Implantatwechsel, Implantatruptur, Implantatdislokation, Infekt, Infektion, Infektsanierung, Injektion, Kapselfibrose, Komplikation, Körperkonturierung, Lipomodelling, Liposuction, Mammaaugmentation, Mammareduktionsplastik, Mastopexie, Oberarmstraffung, Oberschenkelstraffung, Rötung, Schwellung, Schmerzen, Silikon, Silikonimplantationen, Silikoninjektionen, Wunddehiszenz, Wundheilungsstörung, Unbehagen, unzufrieden, ästhetisch, ästhetischen, Silikonom, Paraffinom, Haartransplantation, zufrieden, unzufriedenstellend, unzufriedenstellendes, Afrika, Amerika, Asien, Ausland, Australien, Barcelona, Belgien, Berlin, Brasilien, Budapest, Bulgarien, Deutschland, Dominikanische Republik, Ecuador, England, Frankreich, Ferner Osten, Indien, Istanbul, Italien, Jordanen, Kolumbien, Kroatien, Libanon, Lissabon, London, Marokko, Mazedonien, Mitteleuropa, Mittlerer Osten, Naher Osten, Nordafrika, Nordamerika, Nordeuropa, Österreich, Paris, Peru, Polen, Portugal, Prag, Rumänien, Serbien, Slowenien, Spanien, Südafrika, Südamerika, Südeuropa, Südosteuropa, Thailand, Tschechien, Tunesien, Türkei, Ungarn, USA, Venezuela, Vereinigte Arabische Emirate, Warschau, Westeuropa, extern.