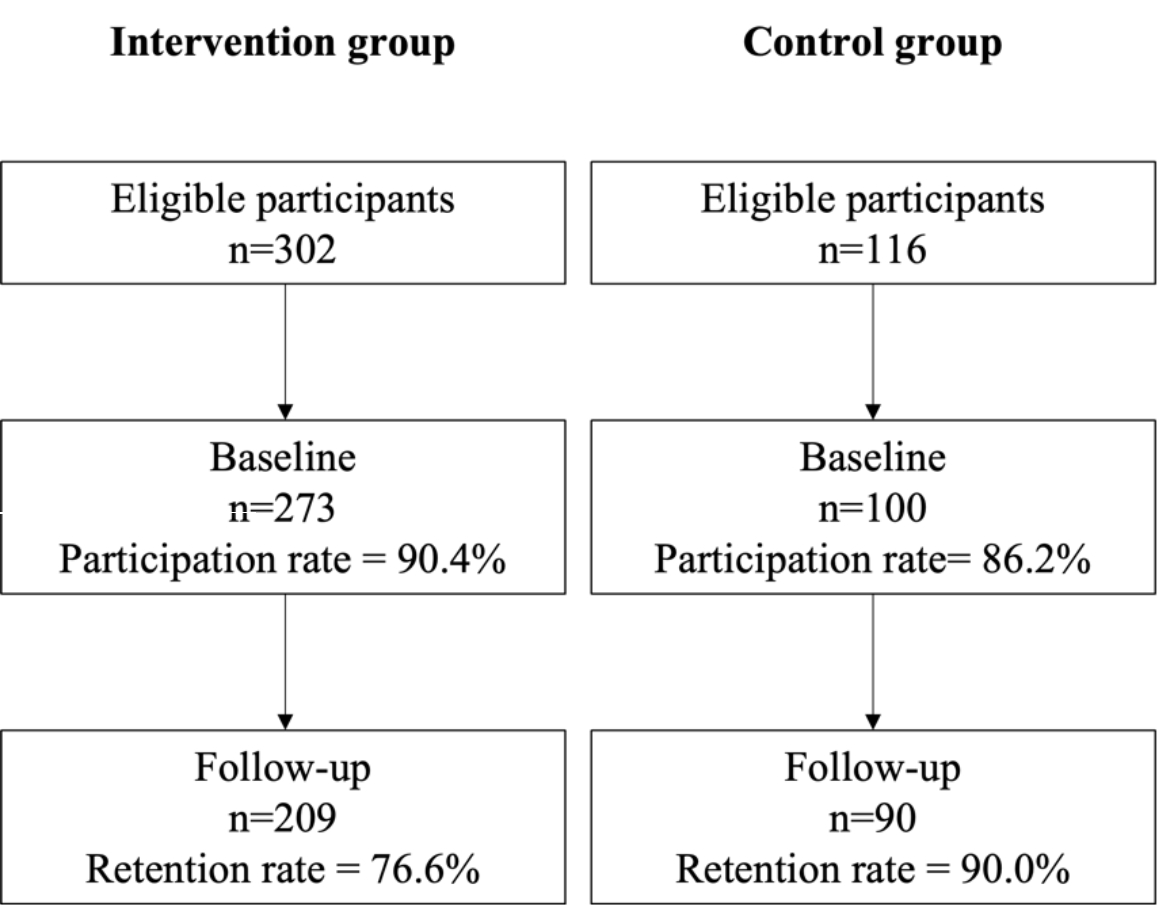
Figure 1 Flow chart.
DOI: https://doi.org/10.4414/SMW.2022.w30207
Suicide is one of the leading causes of death in young people [1]. Preventing suicide is therefore a public health priority in several countries and there is a critical need of effective national prevention strategies. In Switzerland, where this study was conducted, suicide is one of the first causes of death among young people [2]. Few studies have yet evaluated a suicide prevention programme in this country [3], and to our knowledge, there has been no evaluation study focusing on young people. As these programmes should be culturally adapted, research in the Swiss context is needed [4].
In other countries, universal suicide prevention programmes have been successfully implemented in school settings [5, 6]. Indeed, schools constitute an ideal setting for suicide prevention programmes [7]. However, empirical studies with robust methods are repeatedly called for [5, 6, 8]. Indeed, there is a lack of controlled studies testing the efficacy of suicide prevention programs [9, 10]. This is especially true among school-aged children, as reported in a recent meta-analysis [6]. It identified only 27 controlled studies evaluating universal suicide prevention programmes among school-aged children, mostly focusing on high school students [6]. Furthermore, this meta-analysis pointed out that the effectiveness of suicide prevention programmes on important distal outcomes such as suicidal behaviour/intention and psychological distress are less investigated [6].
In addition to these important limitations, programmes often required multiple sessions and may be not easy to implement in school settings. For example, the well-known Youth Aware of Mental Health Program takes place over 3 weeks (three sessions for a total of 5 hours) [11]. Brief programmes would have a high cost-efficacy and transportability. Unfortunately, the efficacy of brief programmes has been less investigated. In Brann et al. [6], no study focused on brief programmes for school-aged children.
To fill in these research gaps, this study investigated the efficacy and acceptability of a brief universal suicide prevention programme for school-aged youths [12]. It included proximal outcomes (knowledge on suicide, perceived suicide awareness and knowledge of help-seeking resources) and distal outcomes (coping skills, suicide-related behaviours, and psychological distress).
We conducted a non-randomised cluster-controlled trial to compare the intervention group (brief suicide prevention programme) with a control group (no intervention). The study included a baseline measure and a one-month follow-up.
The study took place in the French-speaking part of Switzerland, in the cantons of Geneva and Neuchâtel. The workshops were conducted in secondary schools. Classes were used as clusters. The study was promoted by the association Stop Suicide (https://stopsuicide.ch), which delivers suicide prevention workshops in the French-speaking part of Switzerland in school and community settings and targets young people aged 14–29. Study participation was offered to all schools in which the association Stop Suicide delivers suicide prevention programmes. Two schools participated in the study. Data were collected between December 2019 and November 2020. Data of the intervention group were collected before the SARS-CoV-2 pandemic: baseline on 2 December 2019 in school 1 and 15 January 2020 in school 2; follow-up on 13 January 2019 in school 1 and 19 February 2020 in school 2. Data of the control group were collected in school 1 after the beginning of the pandemic when the schools reopened: baseline on 26 October 2020; follow-up on 23 November 2020. The baseline assessment for the control group took place just before the first lockdown, but the next steps of the study could not take place, so the recruitment of the control group started again after schools reopened. Assignment to groups was based on logistical factors (whether the workshop was planned early or late in the semester).
The study protocol was submitted to the cantonal ethic committee (Geneva, no. 2019-00295). It was considered as falling outside the scope of the Swiss legislation (Federal Act on Research involving Human Beings). Participants nonetheless signed a written informed consent form. The study protocol has been published elsewhere [12]. Deviations from the protocol were due to the SARS-CoV-2 pandemic (i.e., the second follow-up after three months could not take place because schools were closed in March 2020). There was no data registry.
Young people were eligible to participate if they were aged 14 or more and were able to communicate in French. Those who had already participated in the workshop the previous year were excluded. A total of 418 adolescents were eligible for study participation, 373 of whom agreed to participate (response rate 89.7%). Among these, 299 also participated in the follow-up visit (retention rate = 80.2%). Detailed information for each group is described in figure 1. There were 216 participants in the first school, separated in two distinct data collections, before the pandemic (n = 110) and after the beginning of the pandemic (n = 100), and 169 in the second school.
Figure 1 Flow chart.
The groups were not balanced because of the disruption due to the SARS-CoV-2 pandemic (schools’ closure in March 2020). The recruitment after the reopening of schools in September 2020 was difficult because of sanitary restrictions.
The main aim of this universal suicide prevention programme was to raise awareness on suicide and to provide resources to seek for / offer help. The workshop lasted for 90 minutes. It provided general information on suicidal behaviour, helped to identify risk factors and warning signs of suicide intention as well as facts and myths about suicide, and provided information on ways to seek for help and to get support. The workshop included a lecture, group discussions based on case examples, a quiz on myths and facts on suicide, and an illustrated book. The workshop was conducted by a trained staff member of Stop Suicide, with the help of a psychologist. The psychologist was available during and after the workshop if needed.
The study included two visits. During the first visit, participants received information on the study and provided written consent. After that, they completed the baseline assessment (about 20 minutes). The suicide prevention workshop was immediately delivered to the intervention group (90 minutes). The same questionnaire was used for the one-month follow-up, except for sociodemographic variables (not assessed at follow-up) and questions on acceptability for the intervention group. When the study was finished, the control group participated in the workshop. Measures were administered through paper-and-pencil.
Three tools were used to assess the primary outcome, namely the efficacy of the intervention at baseline and follow-up.
We used items from the French version of the Literacy of Suicide Scale (LOSS), developed to test suicide knowledge and awareness of suicidal risks [13]. We used seven relevant items from the original 12-item scales (other items were not discussed in the workshop). A total score of correct responses (0–7) was computed.
We used subscales derived from a previous study on suicide prevention to assess suicide awareness [14]. It included perceived knowledge of suicide and help-seeking (five items), willingness to talk about suicide and to seek for help (three items), confidence to talk about suicide and to seek for help (five items), and intention to seek for help (one item). Items were assessed on a five-point scale and a mean score was computed (ranging from 0 = totally disagree to 4 = totally agree).
We self-developed a scale to assess perceived knowledge of help-seeking resources (six items). Items were also assessed on a five-point scale and a mean score was computed (ranging from 0 = totally disagree to 4 = totally agree).
One tool was used to assess the secondary outcome acceptability at follow-up (only for the intervention group):
We used the six items from the same previous suicide prevention study to test whether the intervention was enjoyable and useful [14]. Items were assessed on a five-point scale (ranging from 0 = totally disagree to 4 = totally agree).
We translated the scales related to suicide awareness, knowledge of help-seeking resources, and acceptability into French using back translation and pre-testing the scales.
Exploratory secondary outcomes were assessed using three tools at baseline and follow-up.
Three subscales from the French version of the COPE inventory were used to assess coping skills: Planning, seeking of instrumental social support, and seeking of emotional social support [15]. Other coping skills were not assessed because they were not relevant for the study. Each subscale has four items assessed on a four-point scale. A mean score for each subscale was computed (ranging from 0 = totally disagree to 3 = totally agree).
The presence of suicidal ideation was tested using two items from the French version of the Columbia-Suicide Severity Rating scale (C-SSRS, [16]). The previous-month screen of suicidal thoughts was used to test the efficacy of the intervention. The lifetime version was used to describe groups at baseline. The presence of any suicidal thoughts was assessed using the endorsement of any of the two items of the C-SSRS (wish to be dead and non-specific suicide thoughts).
The French version of the Kessler Psychological Distress scale (K-6) was used to assess global psychological distress over the previous four weeks [17, 18]. This six-item scale is assessed on a five-point scale. A sum score ranging from 0 to 24 was computed, with a score of 13 or more indicating a severe psychological distress.
Sociodemographic variables included age, gender, type of school (secondary I or II) and parental level of education (primary or secondary versus tertiary).
A total of 95 participants in each group were required to detect a statistically significant difference between groups, with alpha = 5%, power = 80%, expected mean differences between groups for the primary outcomes (suicide knowledge, suicide awareness and knowledge of help-seeking resources) = 1, variance = 6. Estimates for mean differences and variances are based on findings of Bailey et al. [14].
We first ran descriptive statistics for both groups and all variables using means and percentages. We then compared groups at baseline to see whether they were comparable using mixed-effect models (linear or logistic according to the type of variables). Participants were nested into classes. We also compared completers and dropouts at baseline using mixed-effect models.
Participants were analysed in their original group (intention to treat), regardless of involvement in the workshop. No per protocol analyses were conducted. We used three-level mixed-effect (linear or logistic) models, with measures nested into participants and participants into classes. A two-level logistic mixed-effect model was used for suicidal ideation because there was no convergence when the level of the class was taken into account. There was evidence for moderate to large intraclass correlation (ranging between 0.47 and 0.75). The effect of the intervention was tested using the interaction between group and time. We included group and time as main effects, and the interaction term group × time. We ran analyses adjusted for baseline sociodemographic variables: age, gender, and parental level of education. For acceptability, means along with 95% confidence intervals (CIs) were used. We used listwise deletion to handle missing data. No replacement was used.
Statistical analyses were conducted with R version 4.1.2 (package lme4 version 1.1–27.1).
Descriptive statistics and comparisons between groups at baseline are reported in table 1. Participants were on average 15.28 years old, 55.8% were girls, and 44.4% had parents with a tertiary level of education. A total of 56.1% of participants were enrolled in secondary I education. Regarding study outcomes, participants had a good suicide-related knowledge (mean score = 5.44 on a 0–7 scale). They had a moderate level of perceived knowledge, willingness and confidence to talk about suicide / seek for help (mean scores between 2.32 and 2.44). Help-seeking questions (intention to seek help and perceived knowledge of help-seeking resources) were lower (1.55–1.75). Participants had a moderate level of coping skills (1.26–1.61) and psychological distress (mean score = 8.12, with a score of 12 indicating severe psychological distress). A notable proportion had suicidal ideation, both in the previous 12 months (45.4%) and previous month (17.5%).
Table 1Descriptive statistics and comparisons between groups at baseline.
| Total | Groups | Comparisons | Missing values | ||||
| Intervention | Control | ||||||
| n = 373 | n = 273 | n = 100 | Coef. | p-value | |||
| Sociodemographic variables | Age (mean) | 15.28 | 15.62 | 14.34 | 1.20 | 0.001 | 1 |
| Gender (%) | |||||||
| Girls | 55.8 | 56.8 | 53.0 | –0.15 | 0.503 | 0 | |
| Boys | 44.1 | 43.2 | 47.0 | ||||
| Parental level of education (%) | |||||||
| Primary/secondary | 55.6 | 53.0 | 62.9 | 0.43 | 0.175 | 8 | |
| Tertiary | 44.4 | 47.0 | 37.1 | ||||
| Type of school (%) | |||||||
| Secondary I | 56.1 | 40.3 | 100 | – | – | 0 | |
| Secondary II | 43.9 | 59.7 | 0.0 | ||||
| Efficacy outcomes | Suicide-related knowledge (0–7) | 5.44 | 5.44 | 5.44 | –0.01 | 0.978 | 0 |
| Perceived knowledge (0–4) | 2.37 | 2.33 | 2.48 | –0.15 | 0.051 | 1 | |
| Willingness to talk/seek help (0–4) | 2.44 | 2.39 | 2.59 | –0.20 | 0.066 | 1 | |
| Confidence to talk/seek help (0–4) | 2.34 | 2.26 | 2.55 | –0.29 | 0.001 | 1 | |
| Intention to seek help (0–4) | 1.75 | 2.72 | 2.84 | –0.12 | 0.364 | 2 | |
| Knowledge help-seeking resources (0–4) | 1.55 | 2.50 | 2.69 | –0.19 | 0.040 | 1 | |
| Coping skills | Planning (0–3) | 1.61 | 1.63 | 1.56 | 0.78 | 0.334 | 5 |
| Instrumental social support (0–3) | 1.26 | 1.28 | 1.23 | 0.04 | 0.645 | 5 | |
| Emotional social support (0–3) | 1.60 | 1.56 | 1.69 | –0.15 | 0.129 | 5 | |
| Psychological variables | Lifetime suicidal ideation (%) | 45.4 | 44.6 | 47.5 | –0.13 | 0.623 | 5 |
| Previous month suicidal ideation (%) | 17.5 | 16.4 | 21.2 | –0.33 | 0.301 | 4 | |
| Psychological distress (0–24) | 8.12 | 7.93 | 8.63 | –0.70 | 0.222 | 6 | |
Comparisons were performed using mixed-effect linear or logistic models.
There were few significant differences between groups at baseline. Participants in the intervention group were significantly older than the control group (p = 0.001). Participants in the intervention group were recruited in secondary I and II, whereas participants in the control group were recruited only in secondary I. Confidence to talk about suicide / seek for help and perceived knowledge of help-seeking resources were higher in the control group compared with the intervention group (p = 0.001 and p = 0.040). Perceived knowledge was almost significant (p = 0.051), with the intervention group having a slightly lower mean score than the control group. Differences for confidence and perceived knowledge of help-seeking resources remained significant with controlling for sociodemographic variables (p = 0.002 and p = 0.015, not reported in table 1). There were no significant differences for coping skills and psychological variables.
Comparisons between completers and dropouts are reported in table 2. There was a significant difference in study participation at follow-up between groups (p = 0.005). Participants from the intervention group were more likely to drop out from the study. One comparison was almost significant, previous-month suicidal ideation (p = 0.051). A marginally significant lower percentage of completers had suicidal ideation. With controlling for sociodemographic variables, the association was no longer significant (p = 0.147, not reported in table 2).
Table 2Comparisons between completers and dropouts at baseline.
| Completers | Dropouts | Comparisons | ||||
| n = 299 | n = 74 | Coef. | p-value | |||
| Sociodemographic variables | Age (mean) | 15.24 | 15.45 | 0.01 | 0.888 | |
| Gender (% | Girls | 53.9 | 63.5 | -0.40 | 0.135 | |
| Boys | 46.1 | 36.5 | ||||
| Parental level of education (%) | Primary/secondary | 55.7 | 55.1 | 0.02 | 0.949 | |
| Tertiary | 44.3 | 44.9 | ||||
| Type of school (%) | Secondary I | 58.2 | 48.7 | 0.39 | 0.140 | |
| Secondary II | 41.8 | 51.3 | ||||
| Group (%) | Intervention | 69.9 | 86.5 | 1.01 | 0.005 | |
| Control | 30.1 | 13.5 | ||||
| Efficacy outcomes | Suicide-related knowledge (0–7) | 5.49 | 5.24 | –0.25 | 0.096 | |
| Perceived knowledge (0–4) | 2.36 | 2.40 | 0.04 | 0.616 | ||
| Willingness to talk/seek help (0–4) | 2.44 | 2.43 | 0.02 | 0.869 | ||
| Confidence to talk/seek help (0–4) | 2.34 | 2.33 | –0.01 | 0.976 | ||
| Intention to seek help (0–4) | 2.75 | 2.78 | 0.04 | 0.796 | ||
| Knowledge help-seeking resources (0–4) | 2.55 | 2.56 | 0.01 | 0.941 | ||
| Coping skills | Planning (0–3) | 1.60 | 1.67 | 0.08 | 0.407 | |
| Instrumental social support (0–3) | 1.25 | 1.32 | 0.07 | 0.540 | ||
| Emotional social support (0–3) | 1.61 | 1.54 | –0.07 | 0.511 | ||
| Psychological variables | Lifetime suicidal ideation (%) | 44.0 | 51.4 | 0.31 | 0.257 | |
| Previous month suicidal ideation (%) | 15.8 | 25.7 | 0.63 | 0.051 | ||
| Psychological distress (0–24) | 7.91 | 5.46 | 1.09 | 0.089 | ||
Comparisons were performed using mixed-effect linear or logistic models.
The main results are reported in tables 3, 4, and 5. For efficacy outcomes (table 3), there was an interaction effect between group and time for perceived knowledge about suicide / help seeking (b = –0.20, 95% CI –0.33; –0.07, p = 0.002), willingness to talk about suicide / help seeking (b = –0.27, 95% CI –0.43; –0.11, p = 0.001), confidence to talk about suicide / help seeking (b = –0.36, 95% CI –0.50; –0.21, p <0.001), intention to seek help (b = –0.29, 95% CI –0.50; –0.07, p = 0.010), and perceived knowledge of help-seeking resources (b = –0.39, 95% CI –0.58; –0.30, p <0.001). The difference was in favour of the intervention group, whose outcomes improved over time compared with the control group (interaction plots are reported in supplementary figures S1 to S6 in the appendix). For perceived knowledge of suicide and help-seeking resources, both groups improved over time (main effect of time: p = 0.006 and p = 0.001), but the improvement was greater in the intervention group. There was no significant interaction effect for suicide-related knowledge (b = –0.14, 95% CI –0.41; 0.13, p = 0.312).
Table 3Mixed-effect models for efficacy outcomes.
| Suicide-related knowledge | Perceived knowledge | Willingness | Confidence | Intention help-seeking | Knowledge help-seeking | |||||||
| Coef. | p -value | Coef. | p -value | Coef. | p -value | Coef. | p-value | Coef. | p-value | Coef. | p | |
| Group | –0.19 | 0.217 | 0.07 | 0.425 | 0.12 | 0.276 | 0.09 | 0.384 | 0.21 | 0.151 | 0.14 | 0.191 |
| Time | –0.04 | 0.721 | 0.15 | 0.006 | –0.03 | 0.622 | –0.08 | 0.196 | –0.12 | 0.195 | 0.27 | 0.001 |
| Interaction group x time | –0.14 | 0.312 | –0.20 | 0.002 | –0.27 | 0.001 | –0.36 | <0.001 | –0.29 | 0.010 | –0.39 | <0.001 |
| Age | 0.15 | 0.003 | –0.02 | 0.472 | –0.05 | 0.241 | –0.02 | 0.603 | –0.02 | 0.734 | 0.03 | 0.479 |
| Gender | –0.57 | <0.001 | 0.02 | 0.804 | 0.03 | 0.691 | 0.05 | 0.512 | 0.20 | 0.045 | –0.14 | -0.044 |
| Parental level of education | 0.06 | 0.533 | 0.12 | 0.050 | 0.10 | 0.196 | 0.11 | 0.131 | 0.07 | 0.075 | 0.01 | 0.868 |
Three-level linear mixed-effect models were run.
Acceptability outcomes are reported in table 4 (n = 201 participants from the intervention group at follow-up). On the five-point scale (0–4), participants found the workshop enjoyable, not upsetting, and worthwhile, with mean scores about 3. CIs for these questions did not overlap with the other questions (equipped for help and recommendation).
Table 4Descriptive statistics and 95% confidence intervals (CIs) for acceptability outcomes.
| Questions | Mean | 95% CI |
| Mean score acceptability | 2.76 | 2.67–2.84 |
| Q1. Did you enjoy the training? | 2.94 | 2.82–3.06 |
| Q2. Did you find the training upsetting? (reversed question) | 3.00 | 2.85–3.14 |
| Q3. How well are you equipped to help your friends and close relatives? | 2.61 | 2.49–2.74 |
| Q4. How well equipped are your friends to help you? | 2.46 | 2.35–2.57 |
| Q5. How worthwhile was the training for students? | 2.91 | 2.79–3.03 |
| Q6. Would you recommend the training to a friend? | 2.65 | 2.51–2.78 |
For exploratory outcomes (table 5), there were significant differences for planning coping skills (b = –0.16, 95% CI –0.31; –0.01, p = 0.038), psychological distress (b = 1.04, 95% CI 0.22; 1.85, p = 0.012), and suicidal ideation (b = –2.32, 95% CI –4.25; –0.39, p = 0.019). Again, outcomes improved over time (or deteriorated less) for the intervention group compared with the control group (see interaction plots in supplementary figures S7 to S11 in the appendix). For psychological distress and suicidal ideation, the control group had a deterioration over time (higher score or rate), whereas the score/rate remained stable or even decreased a little in the intervention group. There were no significant differences for the coping skills instrumental social support (b = –0.05, 95% CI –0.24; 0.13, p = 0.587) and emotional social support (b = –0.07, 95% CI –0.22; 0.09, p = 0.388).
Table 5Mixed-effect models for exploratory outcomes.
| Coping skills | Psychological variables | |||||||||
| Planning | Instrumental | Emotional | Psychological distress | Suicidal ideation | ||||||
| Coef. | p -value | Coef. | p -value | Coef. | p -value | Coef. | p value | Coef. | p- value | |
| Group | –0.06 | 0.517 | –0.04 | 0.692 | –0.15 | 0.175 | –1.00 | 0.115 | 0.04 | 0.969 |
| Time | 0.15 | 0.001 | 0.11 | 0.029 | 0.03 | 0.536 | –0.30 | 0.191 | 0.95 | 0.210 |
| Interaction group x time | -0.16 | 0.038 | -0.05 | 0.587 | –0.07 | 0.388 | 1.04 | 0.012 | -2.32 | 0.019 |
| Age | 0.09 | 0.005 | 0.05 | 0.237 | –0.02 | 0.621 | 0.12 | 0.607 | 0.15 | 0.705 |
| Gender | 0.11 | 0.093 | -0.18 | 0.014 | –0.43 | <0.001 | –3.17 | <0.001 | –1.32 | 0.108 |
| Parental level of education | 0.11 | 0.102 | 0.13 | 0.088 | 0.05 | 0.547 | 0.11 | 0.824 | 0.09 | 0.910 |
Three-level linear mixed-effect models were run for coping skills and psychological distress. A two-level logistic mixed-effect model was ran for suicidal ideation (no convergence when the level of the class was taken into account).
This study investigated the efficacy and acceptability of a brief universal suicide prevention programme for school-aged youths. Findings highlighted potential positive results in four main areas.
First, the intervention seemed to increase perceived suicide awareness and knowledge of help-seeking resources. Suicide awareness and helping skills are the main outcomes for suicide prevention programmes [6] and were also key features of the programme delivered by Stop Suicide in Switzerland. In previous studies, the main effects of intervention programmes dealt with these outcomes [6]. Our findings showed that a brief programme (90 minutes) might also have significant benefits on these important proximal outcomes. On the contrary, there was no significant benefit of the intervention on suicide-related knowledge, and thus no increased awareness on myths and facts about suicide. At baseline, youths already had a good knowledge (mean score of 5.44 on a 0–7 scale), which meant that there was not great room for improvement.
Second, the intervention was evaluated as being enjoyable, not upsetting, and worthwhile. It suggests that there was a high acceptability for this brief suicide prevention programme. This result is in line with previous research showing a large acceptability of longer universal suicide prevention programmes [14, 19]. This was an important finding, as such programmes should not increase youths’ distress.
Third, the intervention also seemed to have benefits on important distal outcomes. Participants in the intervention group showed improvement of a specific kind of coping skills, planning, compared with the control group. This is a problem-solving strategy, which consists of thinking about action strategies and steps to deal with the problem [15]. Other coping skills related to support seeking (seeking social support for instrumental and emotional reasons) did not change (e.g., talking about the situation, about emotions). Coping planning was probably enhanced because the workshop focused on identification of help-seeking resources and ways to behave in the case of suicidal thoughts (for oneself or others). Another explanation for these results is that there are developmental-graded ways to cope with problems [20]. Support seeking is more common in childhood, whereas problem solving strategies increase over time [20]. The intervention might have improved the most commonly used coping skills in adolescence. Coping skills are a protective factor against suicide [21] and therefore could be an interesting psychological mechanism for suicide prevention programmes. Besides, previous studies concluded that universal suicide prevention programmes did not change coping skills [22] and that these programmes worked whatever the prevailing coping skills used [21].
Fourth, the study also highlighted potential benefits of the intervention on psychological outcomes. More precisely, psychological distress and suicidal ideation increased in the control group whereas they remained stable or even decreased in the intervention group. As previous studies reported modest or even null effects of suicide prevention programmes on these critical distal outcomes [6], these findings might be important. The deteriorated psychological outcomes in the control group were probably not due to the questions on psychological distress and suicidal ideation, as previous studies reported that screening for such sensitive topics did not worsen distress [14, 23].
This study suggested that a brief suicide prevention programme could lead to beneficial effects, providing further empirical evidence on brief programmes.
This study has some important limitations. First, it was not a randomised controlled trial and therefore a bias in the group attribution cannot be excluded. Even if baseline differences were small and models controlled for sociodemographic variables, conclusions should be interpreted cautiously. More specifically, participants in the intervention group were older than participants in the control group, because they were recruited in secondary I and II whereas participants in the control group were recruited only in secondary I. As we did not use a probabilistic sampling strategy, the representativeness of our sample should be considered carefully, even if the response rate was very high. In addition, the recruitment period was not the same for the two groups, as the study was interrupted because of the SARS-CoV-2 pandemic. We should keep in mind that data from the control group were collected after the pandemic started and after months of school closure. It was not possible to control for the effect of the pandemic, as this variable was collinear with the groups. There were no significant differences between groups at baseline, but the context of the SARS-CoV-2 has impacted young people’s mental health [24] and results should therefore be interpreted carefully. The difference in the attrition rate was also a study limitation. The retention rate was lower in the intervention group because of a logistic issue (an outdoor activity was planned for a subgroup of youths who therefore could not attend the follow-up assessment). However, the fact that dropouts were marginally more likely to have suicidal ideation was an important study shortcoming and findings should be interpreted considering this limitation. It could mean that young people concerned by suicidal ideation and/or affected by the intervention tended to drop out. Other limitations included the short-term follow-up, non-inclusion of potential confounders (e.g., family factors, mental health variables), and focus on youths involved in schools. Future studies should include long-term follow-ups, a larger range of variables, and youths not enrolled in school (e.g., apprenticeship). Our study did not include per protocol analyses, meaning that findings might be conservative. Further studies should also include per protocol analyses to provide a full overview of the benefits of universal suicide prevention. Finally, some tools were not available in French (suicide awareness, knowledge of help-seeking resources, and acceptability) and further validation of these scales are needed.
Overall, our study showed that the brief universal suicide prevention programme conducted by Stop Suicide seemed beneficial and safe for school-aged youths. Suicide prevention programmes are important among school-aged youths because it is a vulnerable developmental phase, in which psychological distress is likely to peak. In addition to increasing suicide awareness and helping skills and resources, universal suicide prevention programmes could also contribute to develop healthy pathways to deal with adversity by enhancing coping skills. Further randomieed controlled trials with longer follow-up would be needed to achieve a better understanding of the benefits of this promising brief universal suicide prevention programme. Future studies should also focus on vulnerable youths (e.g., with high psychological distress, mental health problems, deprived background, migration background).
Anonymised data and statistical code are available on reasonable request to the corresponding author.
The work was supported by Promotion Santé Suisse.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest was disclosed.
1. WHO . Suicide worldwide in 2019 - Global health estimates. World Health Organization; 2021.
2. OFS . Statistique des causes de décès 2018. Federal Office of Statistics; 2020.
3. Saillant S , Michaud L , Besson J , Dorogi Y . Programme sentinelle : exemple de prévention du suicide auprès d’une population agricole en Suisse. Encephale. 2020 Aug;46(4):258–63. https://doi.org/10.1016/j.encep.2019.10.008
4. Trageser J , Petry C , von Stokar T , Reisch T . Bilan intermédiaire de la mise en oeuvre du plan d’action national pour la prévention du suicide - Synthèse. INFRAS; 2021.
5. Robinson J , Calear AL , Bailey E . Suicide prevention in educational settings: a review. Australas Psychiatry. 2018 Apr;26(2):132–40. https://doi.org/10.1177/1039856218759406
6. Brann KL , Baker D , Smith-Millman MK , Watt SJ , DiOrio C . A meta-analysis of suicide prevention programs for school-aged youth. Child Youth Serv Rev. 2021;121:105826. https://doi.org/10.1016/j.childyouth.2020.105826
7. Singer JB , Erbacher TA , Rosen P . School-based suicide prevention: A framework for evidence-based practice. School Ment Health. 2019;11(1):54–71. https://doi.org/10.1007/s12310-018-9245-8
8. Katz C , Bolton SL , Katz LY , Isaak C , Tilston-Jones T , Sareen J ; Swampy Cree Suicide Prevention Team . A systematic review of school-based suicide prevention programs. Depress Anxiety. 2013 Oct;30(10):1030–45. https://doi.org/10.1002/da.22114
9. Robinson J , Bailey E , Witt K , Stefanac N , Milner A , Currier D , et al. What works in youth suicide prevention? a systematic review and meta-analysis. EClinicalMedicine. 2018 Oct;4-5:52–91. https://doi.org/10.1016/j.eclinm.2018.10.004
10. Wasserman D , Hoven CW , Wasserman C , Wall M , Eisenberg R , Hadlaczky G , et al. School-based suicide prevention programmes: the SEYLE cluster-randomised, controlled trial. Lancet. 2015 Apr;385(9977):1536–44. https://doi.org/10.1016/S0140-6736(14)61213-7
11. Wasserman C , Hoven CW , Wasserman D , Carli V , Sarchiapone M , Al-Halabí S , et al. Suicide prevention for youth—a mental health awareness program: lessons learned from the Saving and Empowering Young Lives in Europe (SEYLE) intervention study. BMC Public Health. 2012 Sep;12(1):776. https://doi.org/10.1186/1471-2458-12-776
12. Baggio S , Kanani A , Nsingi N , Sapin M , Thélin R . Evaluation of a suicide prevention program in Switzerland: protocol of a cluster non-randomized controlled trial. Int J Environ Res Public Health. 2019 Jun;16(11):2049. https://doi.org/10.3390/ijerph16112049
13. Batterham PJ , Calear AL , Christensen H . Correlates of suicide stigma and suicide literacy in the community. Suicide Life Threat Behav. 2013 Aug;43(4):406–17. https://doi.org/10.1111/sltb.12026
14. Bailey E , Spittal MJ , Pirkis J , Gould M , Robinson J . Universal suicide prevention in young people: an evaluation of the safeTALK program in Australian high schools. Crisis. 2017 Sep;38(5):300–8. https://doi.org/10.1027/0227-5910/a000465
15. Carver CS , Scheier MF , Weintraub JK . Assessing coping strategies: a theoretically based approach. J Pers Soc Psychol. 1989 Feb;56(2):267–83. https://doi.org/10.1037/0022-3514.56.2.267
16. Posner K , Brown GK , Stanley B , Brent DA , Yershova KV , Oquendo MA , et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011 Dec;168(12):1266–77. https://doi.org/10.1176/appi.ajp.2011.10111704
17. Arnaud B , Malet L , Teissedre F , Izaute M , Moustafa F , Geneste J , et al. Validity study of Kessler’s psychological distress scales conducted among patients admitted to French emergency department for alcohol consumption-related disorders. Alcohol Clin Exp Res. 2010 Jul;34(7):1235–45. https://doi.org/10.1111/j.1530-0277.2010.01201.x
18. Kessler RC , Andrews G , Colpe LJ , Hiripi E , Mroczek DK , Normand SL , et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002 Aug;32(6):959–76. https://doi.org/10.1017/S0033291702006074
19. Lindow JC , Hughes JL , South C , Gutierrez L , Bannister E , Trivedi MH , et al. Feasibility and acceptability of the Youth Aware of Mental Health (YAM) intervention in US adolescents. Arch Suicide Res. 2020 Apr-Jun;24(2):269–84. https://doi.org/10.1080/13811118.2019.1624667
20. Zimmer-Gembeck MJ , Skinner EA . Review: The development of coping across childhood and adolescence: An integrative review and critique of research. Int J Behav Dev. 2011;35(1):1–17. https://doi.org/10.1177/0165025410384923
21. Kahn JP , Cohen RF , Tubiana A , Legrand K , Wasserman C , Carli V , et al. Influence of coping strategies on the efficacy of YAM (Youth Aware of Mental Health): a universal school-based suicide preventive program. Eur Child Adolesc Psychiatry. 2020 Dec;29(12):1671–81. https://doi.org/10.1007/s00787-020-01476-w
22. Portzky G , van Heeringen K . Suicide prevention in adolescents: a controlled study of the effectiveness of a school-based psycho-educational program. J Child Psychol Psychiatry. 2006 Sep;47(9):910–8. https://doi.org/10.1111/j.1469-7610.2006.01595.x
23. Robinson J , Pan Yuen H , Martin C , Hughes A , Baksheev GN , Dodd S , et al. Does screening high school students for psychological distress, deliberate self-harm, or suicidal ideation cause distress—and is it acceptable? An Australian-based study. Crisis. 2011;32(5):254–63. https://doi.org/10.1027/0227-5910/a000087
24. Theberath M , Bauer D , Chen W , Salinas M , Mohabbat AB , Yang J , et al. Effects of COVID-19 pandemic on mental health of children and adolescents: A systematic review of survey studies. SAGE Open Med. 2022 Mar;10:20503121221086712. https://doi.org/10.1177/20503121221086712
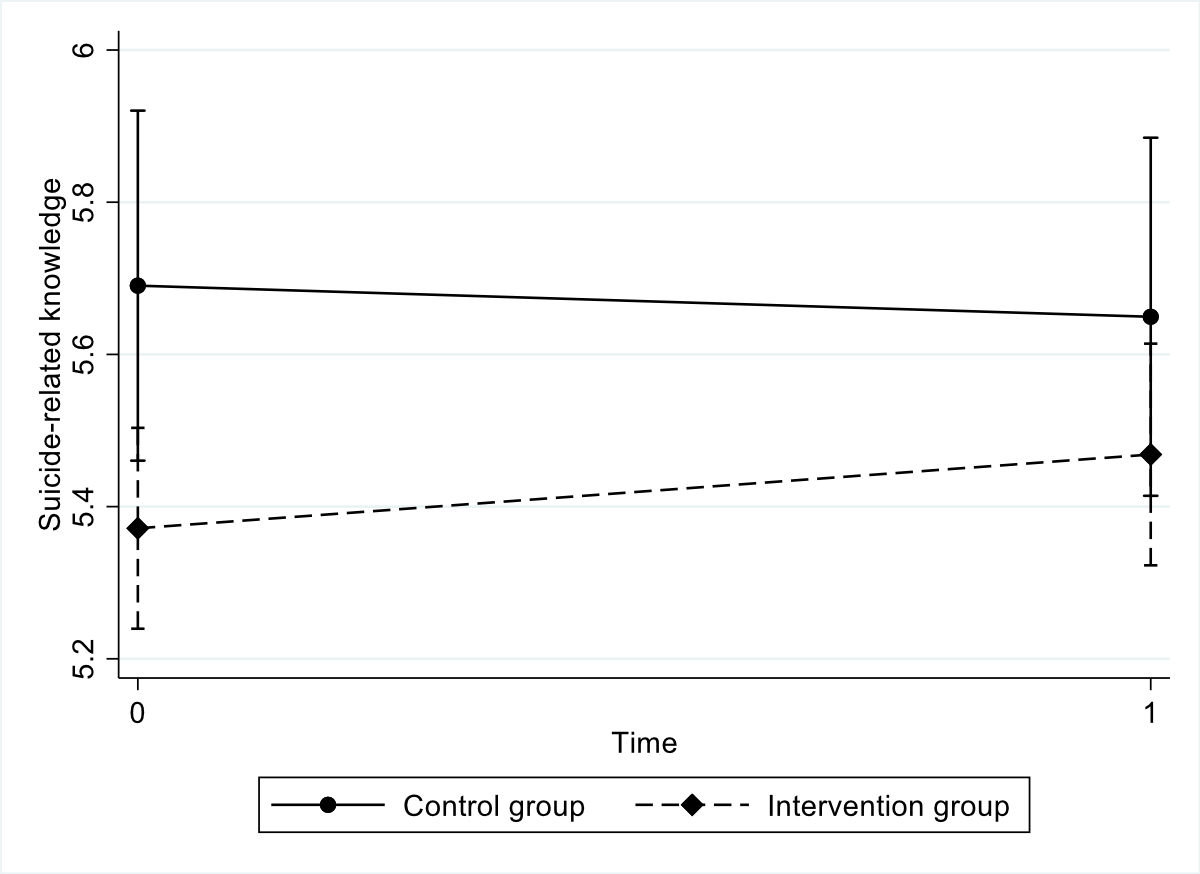
Figure S1 Interaction plot for suicide-related knowledge.
Interaction group x time: p = 0.312
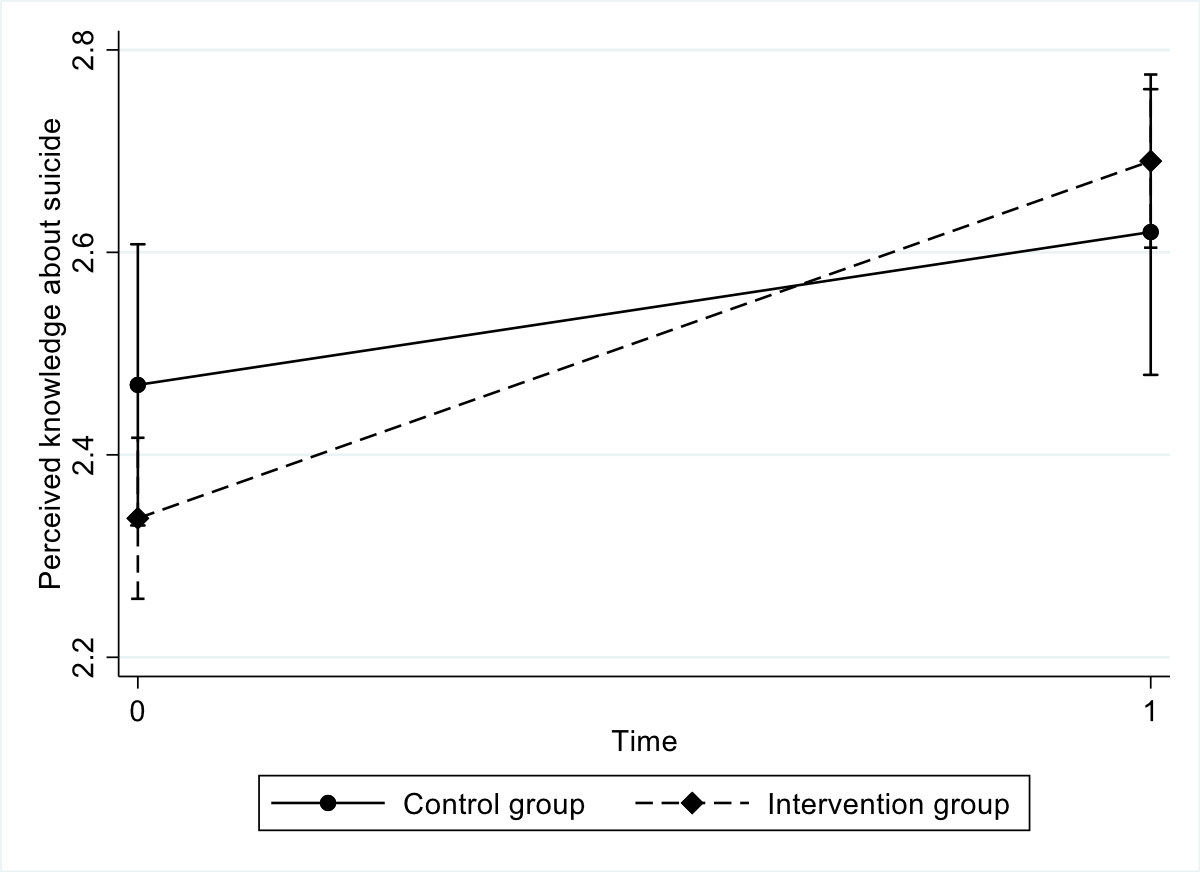
Figure S2 Interaction plot for perceived knowledge about suicide and help seeking.
Interaction group x time: p = 0.002
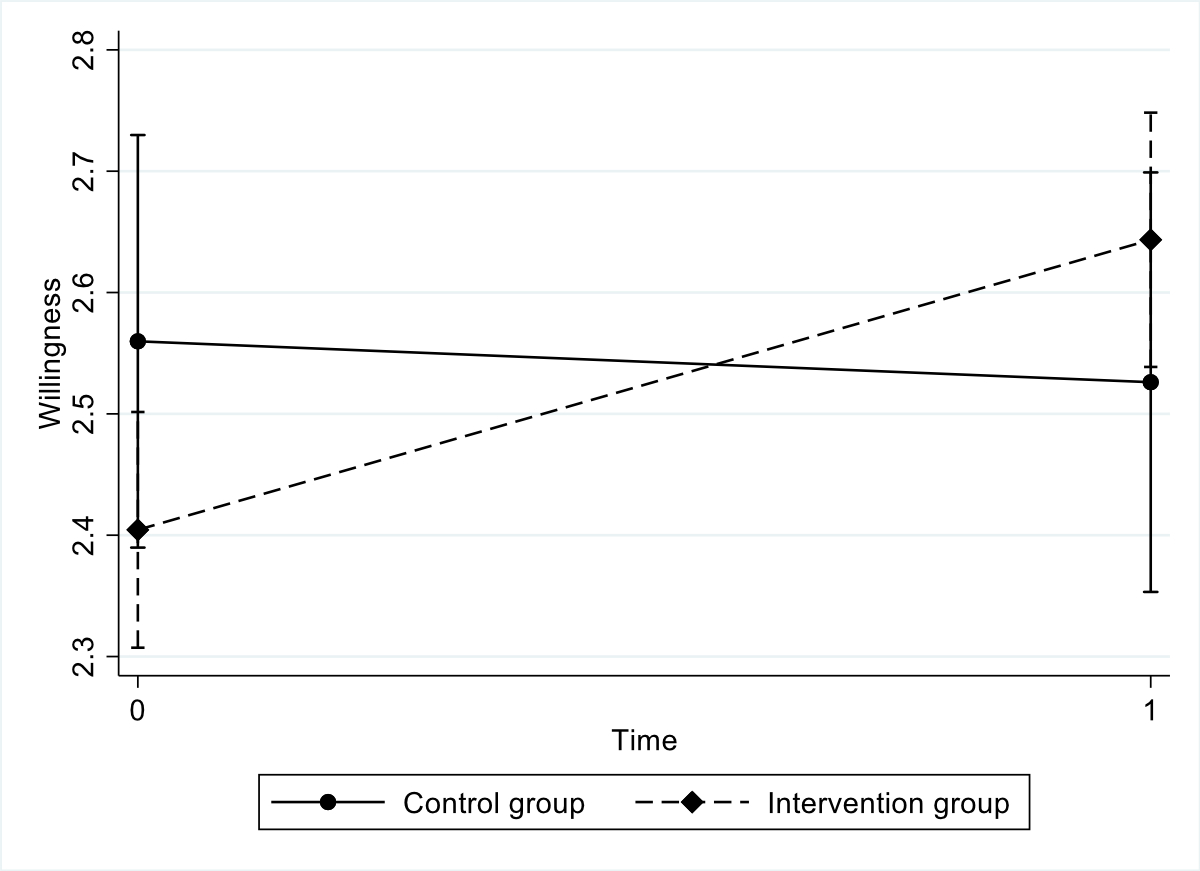
Figure S3 Interaction plot for willingness to talk about suicide/help seeking.
Interaction group x time: p = 0.001
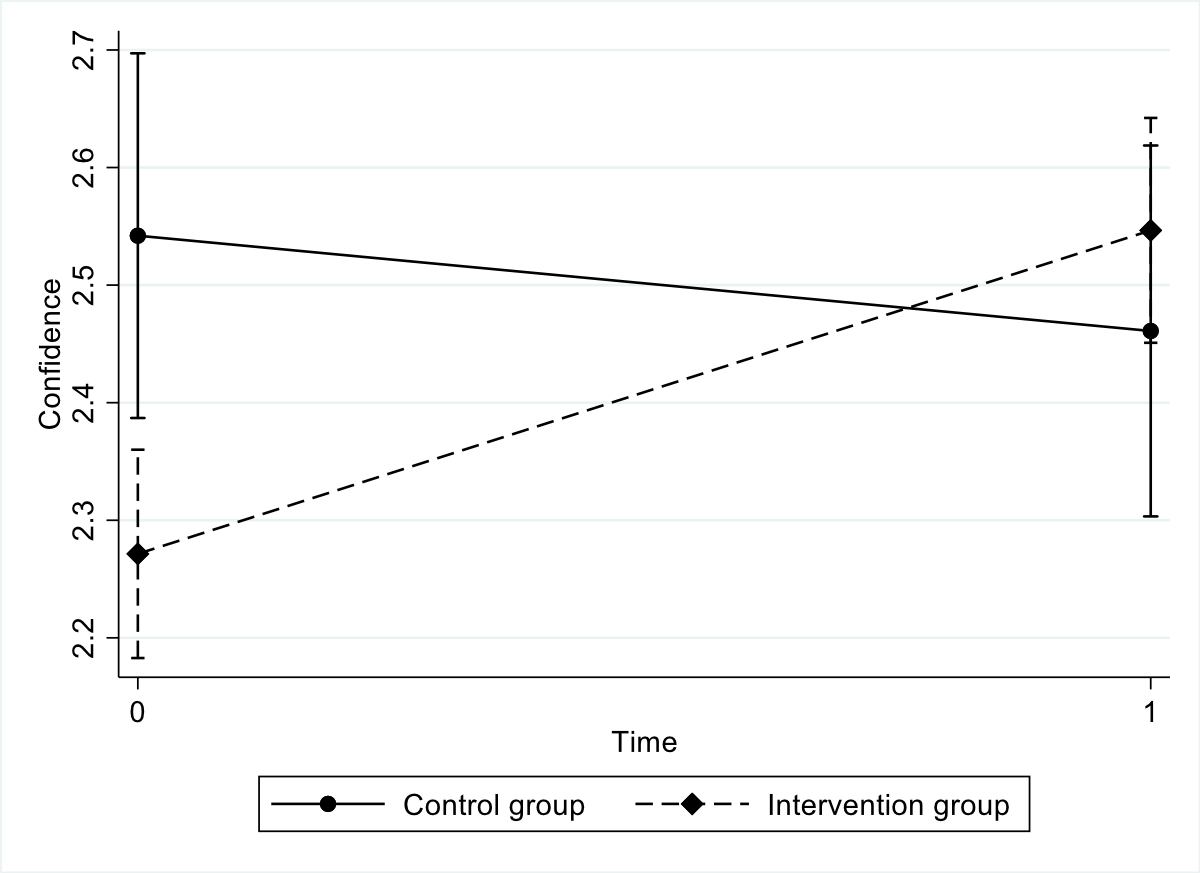
Figure S4 Interaction plot for confidence to talk about suicide/help seeking.
Interaction group x time: p<.001
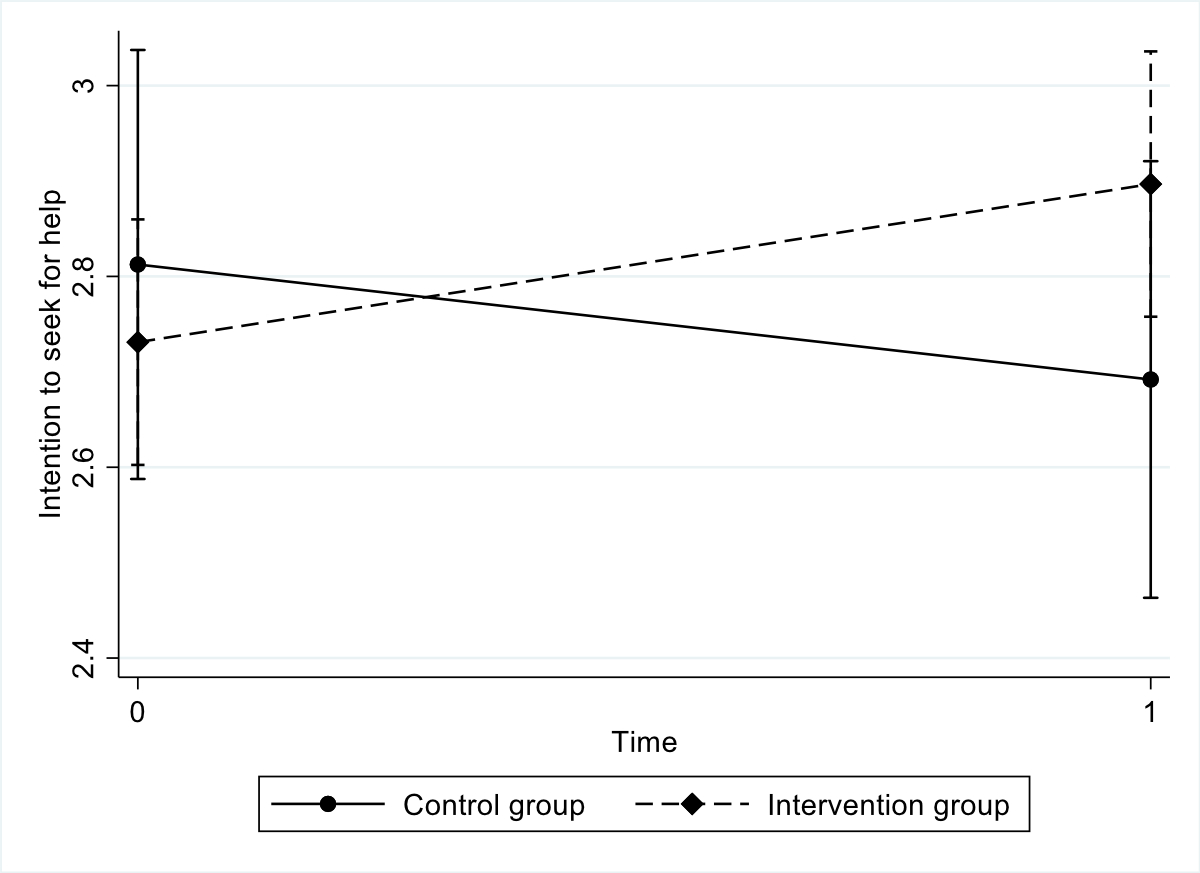
Figure S5 Interaction plot for intention to seek for help.
Interaction group x time: p = 0.010
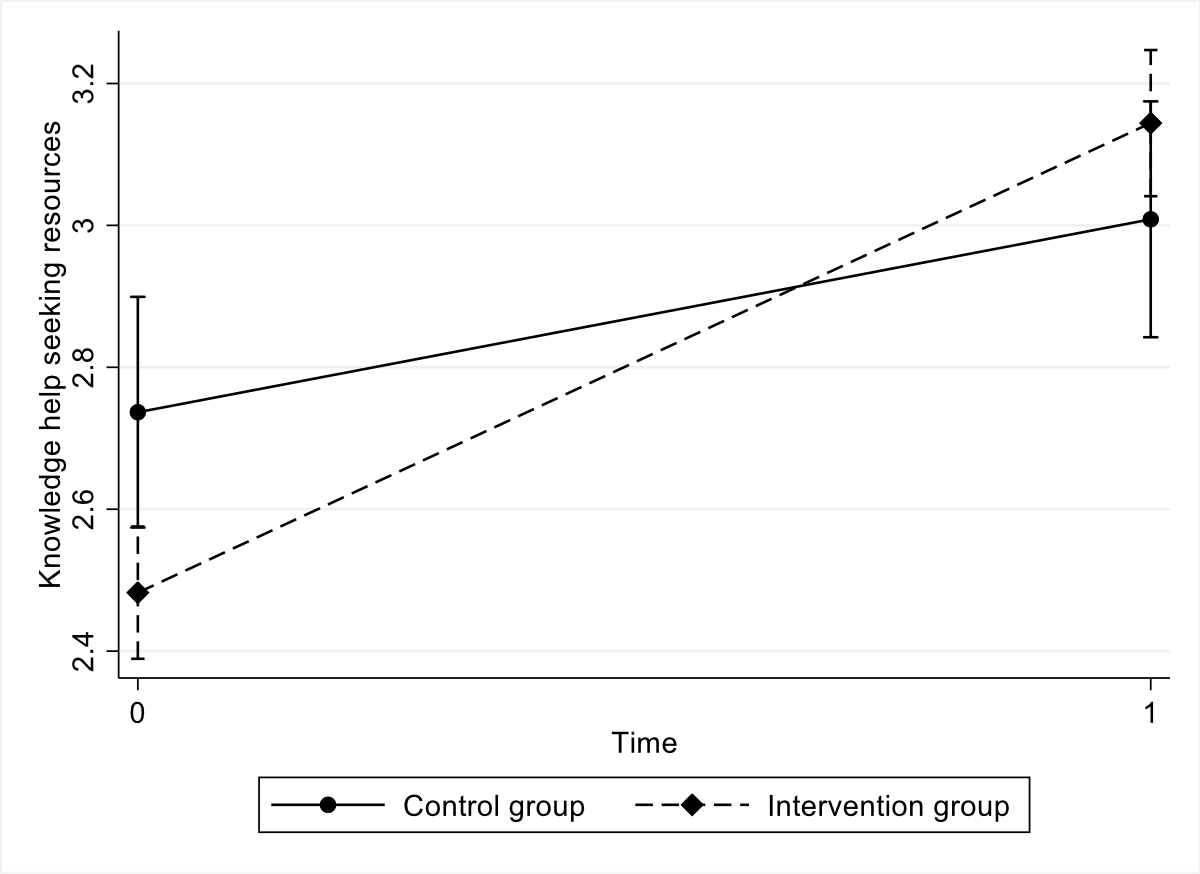
Figure S6 Interaction plot for perceived knowledge of help-seeking resources.
Interaction group x time: p<.001
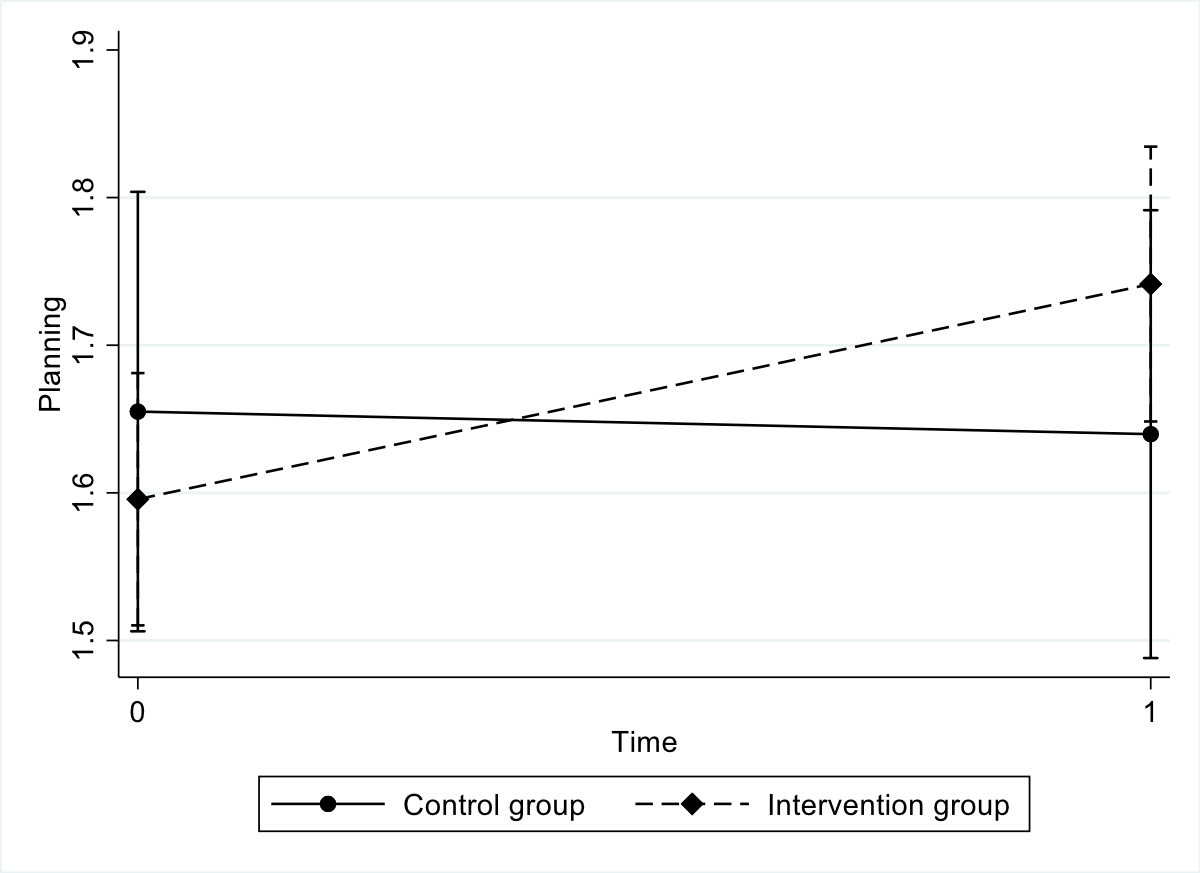
Figure S7 Interaction plot for coping skills: planning.
Interaction group x time: p = 0.038
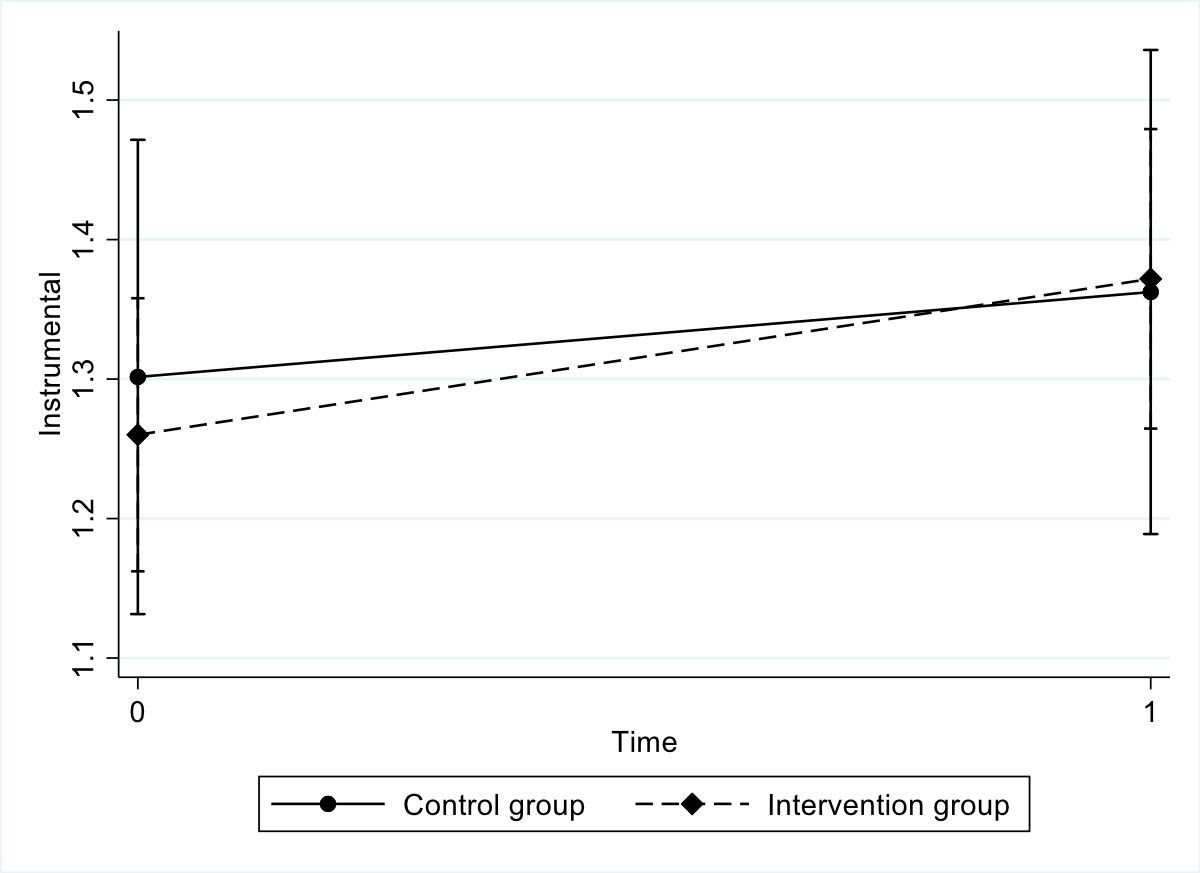
Figure S8 Interaction plot for coping skills: instrumental social support.
Interaction group x time: p = 0.587
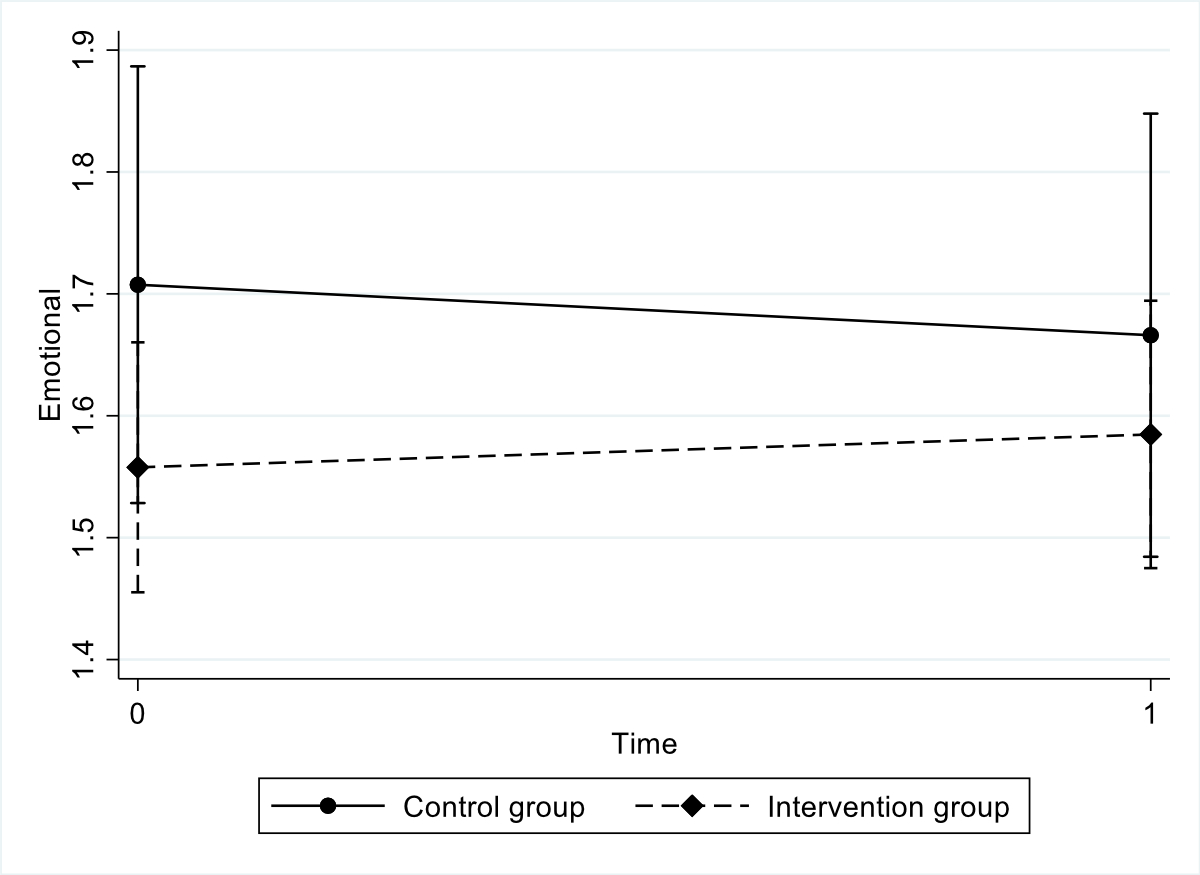
Figure S9 Interaction plot for coping skills: emotional social support.
Interaction group x time: p = 0.388
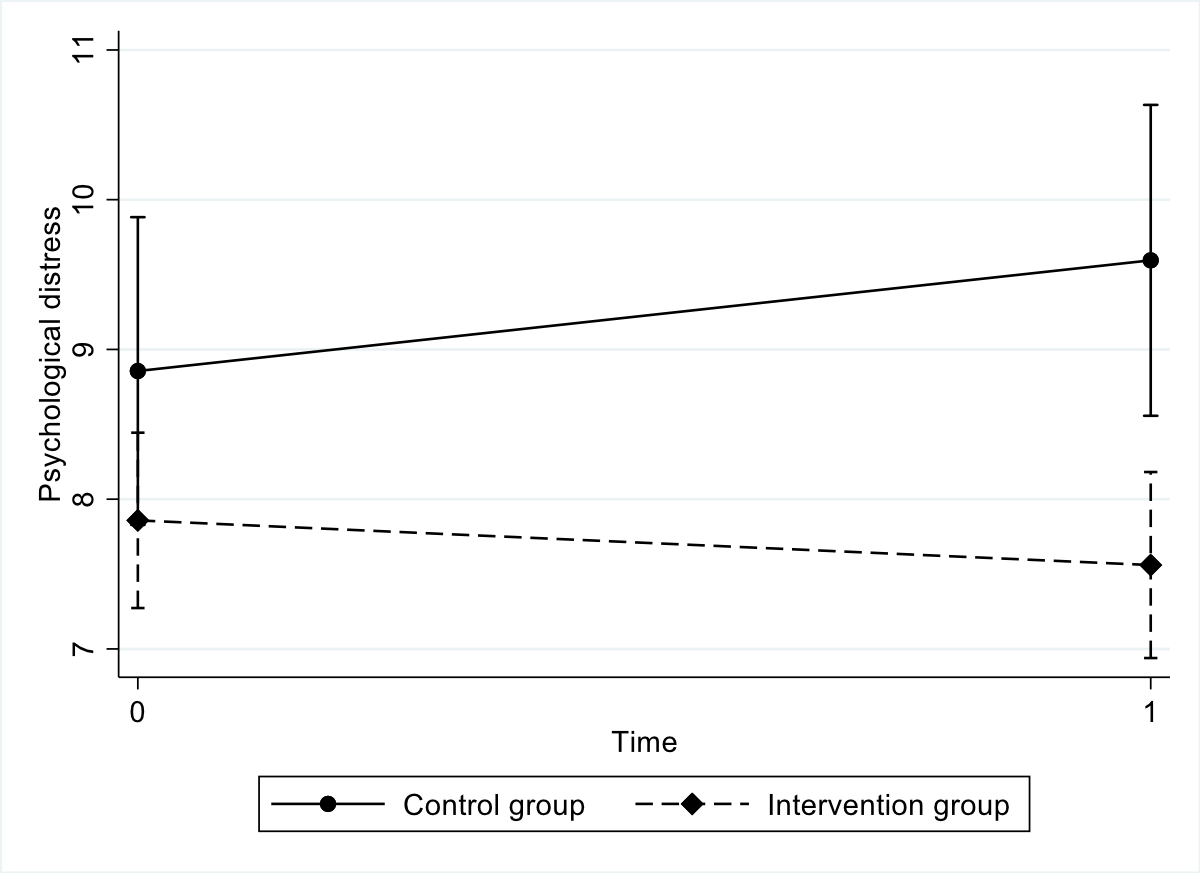
Figure S10 Interaction plot for psychological distress.
Interaction group x time: p = 0.012
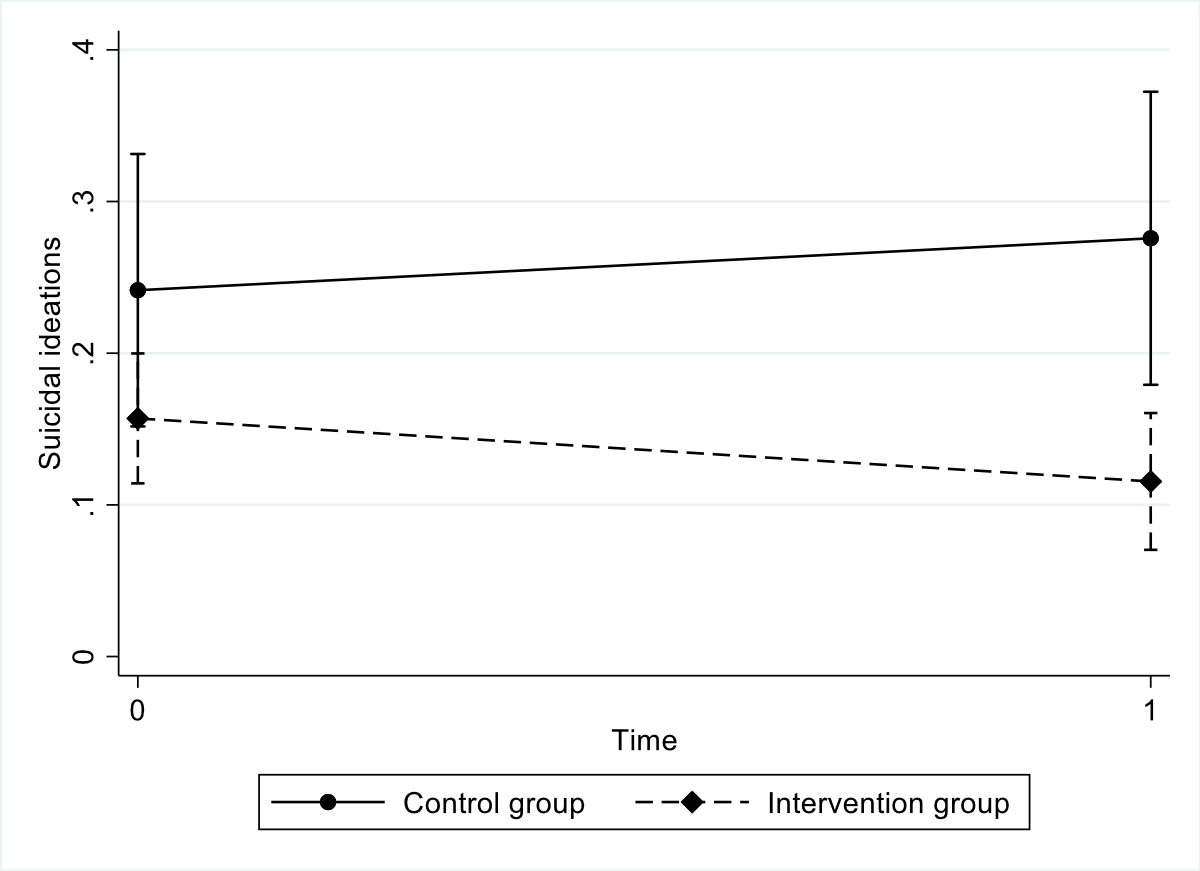
Figure S11 Interaction plot for suicidal ideations.
Interaction group x time: p = 0.019