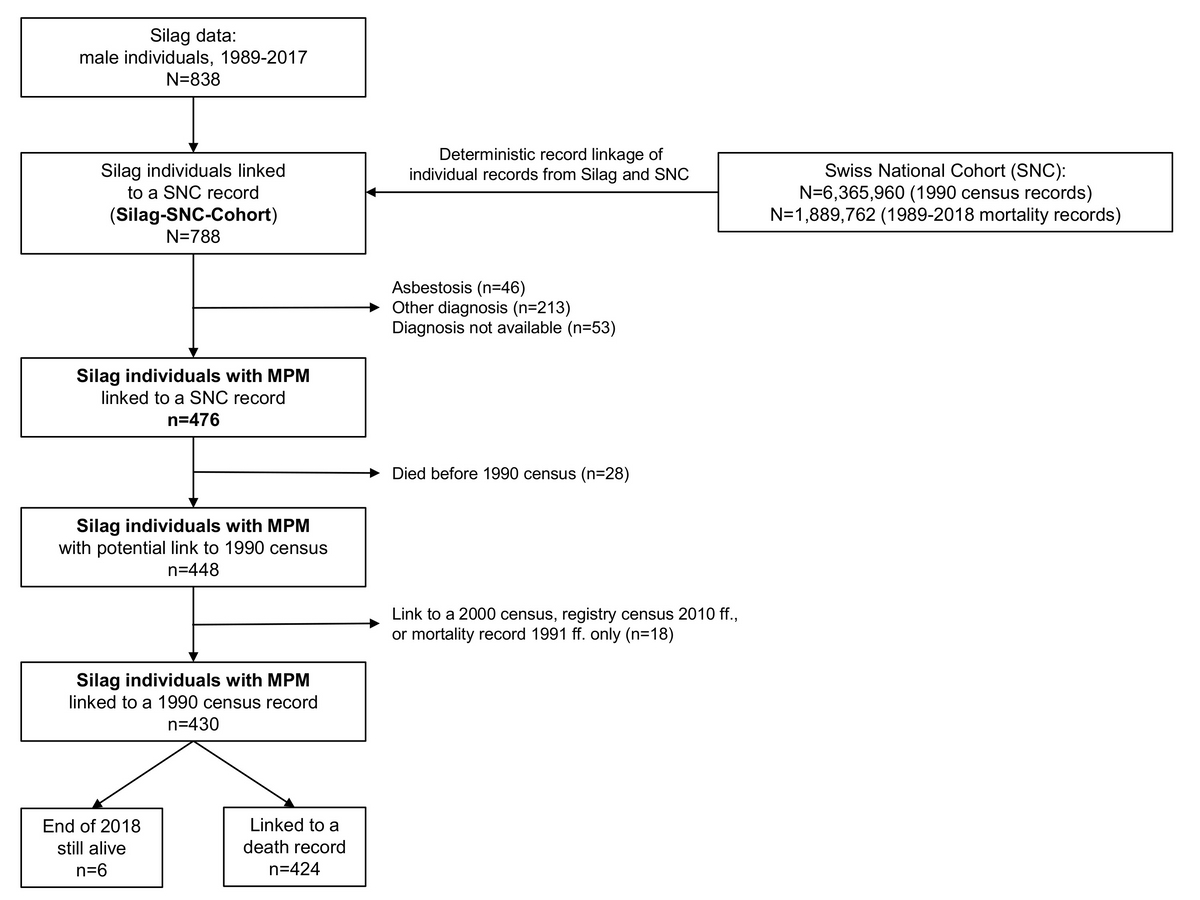
Figure 1 Flow chart of Silag individuals linked to the Swiss National Cohort (SNC) with focus on mesothelioma. MPM: malignant pulmonary mesothelioma
DOI: https://doi.org/10.4414/SMW.2022.w30164
Asbestos is responsible for an estimated 107,000 deaths worldwide each year, primarily due to malignant pleural mesothelioma [1]. Although the use of asbestos has been banned for several decades in most western industrialised countries including Switzerland, the incidence of malignant pleural mesothelioma has not reached its peak yet [2, 3]. According to the Swiss National Accident Insurance Fund (Suva), malignant pleural mesothelioma in Switzerland will peak shortly before 2030 [3]. This is mainly due to the long latency period of 30 to 50 years between exposure and occurrence of the disease [4]. As a result, there is massive health and financial damage caused by asbestos-related diseases [5]. In Switzerland, asbestos-related diseases account for more than half of the costs and 85% of deaths caused by occupational diseases [6]. Worldwide asbestos-related diseases are not expected to peak for several decades, mainly because in many developing countries the use of asbestos is still widespread [1]. To obtain a better impression of incidence and mortality of diseases associated with asbestos exposure, further epidemiological research in this area is of both national and international interest. In the case of Switzerland, the scientific epidemiological knowledge in this area is limited.
The Swiss Laboratory for Particle Analysis in Tissues (Silag) collects clinical data and performs lung dust analysis on tissue samples obtained from subjects with suspected asbestos exposure to quantify asbestos burden. In the absence of a national malignant pleural mesothelioma register, the Silag data provide a unique source of information concerning asbestos-related diseases in Switzerland. However, the value of the dataset is limited by the incompleteness of certain demographic data such as occupation and year of death. In order to enhance the Silag dataset with this information, we carried out a record linkage with the Swiss National Cohort (SNC) [7]. Basically, the SNC is a nationwide record linkage of individual data from census and mortality records and has been successful for valorising other studies lacking follow-up information (see for example [8]).
In this study we focused on two major questions. Firstly, we wanted to assess the feasibility and success of anonymous record linkage of Silag and SNC data. Secondly, we aimed at describing the epidemic of asbestos-related lung diseases, in particular malignant pleural mesothelioma, according to geographical and sociodemographic aspects including occupations and industries.
Silag investigates lung tissue samples of patients with a suspected asbestos-related disease in Switzerland through dust analysis. Asbestos analysis is conducted according to internationally established methods described by De Vuyst et al. [9]. The results are recorded and integrated with other patient characteristics, including smoking status and diagnosis, mainly derived from medical reports that were sent to Silag with the sample material. As only cases with lung dust analysis are included, the Silag cohort is highly selected.
For linkage with the SNC data, recorded Silag data were selected according to the following inclusion criteria: (1) suspected or a diagnosed asbestos-related disease; (2) lung dust analysis performed; (3) male gender. Even though the Silag cohort contains a few females, the numbers are too small for a meaningful interpretation and the data of females were therefore omitted for this study. Data between 1989 and 2017 were selected and completely revised, i.e., the information in the Silag files was aligned with the information in clinical and pathological reports according to an internal standardised procedure.
The Swiss National Cohort (SNC, https://www.swissnationalcohort.ch) is a nationwide census-based cohort (covering all residents of Switzerland) that combines anonymised individual data from the 1990 and 2000 federal population censuses, the yearly registry censuses since 2010 and the death registries [7]. The SNC provides information on education, occupation, place of residence (canton in Switzerland) and other sociodemographic characteristics on an individual level.
Owing to the lack of a unique person identifier, census data from 1990 and 2000 were linked to death and migration records using deterministic and probabilistic linkage methods based on sex, date of birth, place of residence, nationality, marital status, religious affiliation and profession. From 2010 onwards, a registry census is performed yearly, and information from different registries can be linked via a unique anonymous person identifier. Currently, the SNC database includes mortality follow-up until the end of 2018. More information about the SNC is given elsewhere [7, 10].
The National Institute for Cancer Epidemiology and Registration (NICER) was founded in May 2007 by the Swiss Cancer Registries Network and Oncosuisse with the contribution of the University of Zurich. NICER promotes and supports population-based cancer registration and epidemiological cancer research in Switzerland [11]. NICER data on pleural cancer are stratified by gender and presented in aggregated form over five-year periods [12].
Data on cancer incidence have only recently become available for all cantons [12]. For this reason we have refrained from performing a linkage with the data from NICER.
We used data of the NICER database to estimate the incidence of pleural cancer and to compare it with the incidence of pleural mesothelioma estimated by Silag data.
Except for age and sex, Silag does not record sociodemographic data. Furthermore, date of death is often missing and cause of death almost always. Therefore, we linked Silag and SNC data based on date of birth and place of residence. Even in larger communities this combination is very specific [13]. For subjects with partly missing identification variables, cause of death was included in the decision whether to accept or decline a potential link. A link was accepted and classified as successful when there was evidence that the respective records belonged to the same person and there were no other equivalent matches.
The linkage resulted in a Silag-SNC-cohort dataset containing both data from Silag (e.g. diagnosis or smoker status of an individual) and data from SNC (e.g., data on occupation or canton of residence in Switzerland).
Sociodemographic and occupational characteristics were derived from the 1990 census, causes of death up to the end of 2018.
To determine whether linkage success was associated with language area, the postcode of the place of residence from the Silag data was used for allocation of patients to the German- or French/Italian-speaking areas of Switzerland. This was accomplished by comparing postcodes with the language area map of the Swiss Federal Statistical Office [14].
Information on occupations classified according to the international standard classification of occupations (ISCO) was taken from the 1990 census information in the SNC. ISCO is an internationally recognised hierarchical classification of occupations. Its aim is to allow international comparison of occupations and thereby facilitate descriptive statistics across countries [15]. Four versions have been published by the International Labour Office. In our study, occupations were classified according to ISCO-88, which was the most recent version at the time of the 1990 census. In order to achieve sufficient group sizes only the highest two of the four hierarchical levels were used (10 major groups, 28 sub-major groups) [16].
Industries were classified according to the classification of the Swiss Federal Statistical Office used for the 1990 census [17].
Geographical distribution of mesothelioma cases from Silag data were analysed by utilising information on the canton of residence in Switzerland provided by the linkage with the SNC (taken from the 1990 census). Then we made a comparison with pleural cancer incidence data from the NICER data, which combines the cancer registers of different cantons [2]. It should be noted that at the time, when the NICER data were accessed, NICER used the term “pleural cancer” to include both, malignant pleural mesothelioma (ICD-10 C45.0) and other malignant neoplasms of the pleura (ICD-10 C38.4). Furthermore, NICER data were reported separately for the periods 1991–1995, 1996–2000, 2001–2005, 2006–2010 and 2011–2015. Since NICER set up cancer registration in key cantons only in the early 1990s, we used only data from 1996 to 2015. Reported NICER data of the above mentioned periods were summed up and then averaged in order to obtain results for the period 1996–2015. Incidence rates both for Silag and NICER data are reported as age standardised rates (ASRs) per 100,000 person years with the European standard population used as reference population [18, 19].
The ASRs were displayed graphically in maps to allow visual comparison and to detect “hotspots”. Owing to the limitations in the datasets and low case numbers, we did not perform statistical comparison.
All our analyses were performed in R version 3.6.1 (The R Foundation for Statistical Computing, 2019). The illustrations of the incidence of malignant pleural mesothelioma in Swiss maps were generated as described in reference [20]. Approval for use and linkage of the Silag and SNC data was obtained from the Ethics Committee of the Canton of Zurich (approval number 2016-02208).
Using the inclusion criteria, 838 male individuals were selected from the original Silag dataset. Data of these individuals were then checked with archive files and, if required, amended and afterwards anonymised. After this revision, 788 of the selected 838 individuals (94.0%) were successfully linked to the SNC database. Out of these, 432 could be linked based on full dates of birth and death, 219 based on date of birth and year of death, place of residence and/or cause of death, and 137 based on manual linkage taking into account potential typos, change of residence or a matching record in the end of 2018 registry census. Overall, 725 of the 788 linked individuals (92.0%) had also a link to a mortality record in the SNC database.
Of the 788 linked individuals, 49 died before 1990 leaving 739 individuals potentially linkable to the 1990 census. Out of these 706 (95.5%) could in fact be linked to the 1990 census. From the 470 linked individuals from Silag registered before end of 2010 and with no mortality record before the 2000 census, 445 (94.7%) were retrieved in the 2000 census.
Out of the 788 individuals successfully linked to the SNC database, 476 individuals with malignant pleural mesothelioma could be linked to a SNC record (fig. 1). Twenty-eight individuals died before the 1990 census, leaving 448 individuals with a potential link to the 1990 census, and finally 430 individuals could be linked to a 1990 census record. Out of these 430 individuals, 424 individuals could be linked to a death record, and 6 individuals were found to be still alive at the end of 2018 (fig. 1).
Figure 1 Flow chart of Silag individuals linked to the Swiss National Cohort (SNC) with focus on mesothelioma. MPM: malignant pulmonary mesothelioma
The language region was examined as a possible determinant of linkage success. Patients living in German-speaking Switzerland (n = 569) were linked slightly less often (n = 558, 98.1% of 569) than patients residing in French/Italian-speaking Switzerland (100%, n = 32). The latter were considered as one group for reasons of group size. Patients with an unknown place of residence (n = 237) had the lowest linkage success rate (n = 198, 83.5% of 237).
Age at death ranged from 31 to 94 with a mean of 67.0 years (standard deviation [SD] 10.5).
Table 1 shows diagnoses associated with exposure to asbestos. Diagnoses unrelated to asbestos were not a subject of this investigation. malignant pleural mesothelioma was the dominant disease in the dataset, diagnosed in 476 (60.4%) of the individuals. Other common diagnoses were pulmonary carcinoma, pleural plaques and asbestosis (including “mild asbestosis”). Overall, 19.4% of the individuals had more than one asbestos-related disease.
Table 1Diagnoses in the linked dataset (n = 788). Only potentially asbestos-related diagnoses were subject to the investigation.
| Diagnoses | n | % |
| Malignant pleural mesothelioma | 476 | 60.4% |
| – Malignant pleural mesothelioma only | 406 | 51.5% |
| – Malignant pleural mesothelioma + other diagnoses1 | 70 | 8.9% |
| Asbestosis (without pleural mesothelioma2) | 46 | 5.8% |
| – Asbestosis only | 10 | 1.3% |
| – Asbestosis + other diagnoses3 | 36 | 4.6% |
| Other diagnoses 3(incl. combinations of diagnoses) | 213 | 27.0% |
| – Pleural plaques only | 36 | 4.6% |
| – Pulmonary carcinoma only | 126 | 16.0% |
| Not available | 53 | 6.7% |
1 Asbestosis, pleural plaques, pulmonary carcinoma, pleural fibrosis, chronic obstructive pulmonary disease (COPD)
2 8 patients had malignant pleural mesothelioma and asbestosis. They were included in “malignant pleural mesothelioma + other diagnoses”
3 Pleural plaques, pulmonary carcinoma, pleural fibrosis, COPD
Within the group of 476 individuals with malignant pleural mesothelioma, age at death ranged from 36 to 94 years with a mean of 65.4 years (SD 10.0).
One focus of this study was to analyse the occupations and industries of the individuals with malignant pleural mesothelioma (table 2).
Table 2Reported occupations of the individuals with malignant pleural mesothelioma (n = 340)
| Occupations | |||
| ISCO Major group | ISCO Submajor group 1 | n | % |
| 1: Legislators, senior officials and managers | 44 | 12.9% | |
| 10: not specified otherwise | 2 | 0.6% | |
| 12: Corporate managers | 42 | 12.4% | |
| 2: Professionals | 25 | 7.4% | |
| 21: Physical, mathematical and engineering science professionals | 14 | 4.1% | |
| 22: Life science and health professionals | 1 | 0.3% | |
| 23: Teaching professionals | 3 | 0.9% | |
| 24: Other professionals | 7 | 2.1% | |
| 3: Technicians and associate professionals | 50 | 14.7% | |
| 31: Physical and engineering science associate professionals | 31 | 9.1% | |
| 33: Teaching associate professionals | 2 | 0.6% | |
| 34: Other associate professionals | 17 | 5% | |
| 4: Clerks | 16 | 4.7% | |
| 41: Office Clerks | 14 | 4.1% | |
| 42: Customer services clerks | 2 | 0.6% | |
| 5: Service workers and shop and market sales workers | 22 | 6.5% | |
| 51: Personal and protective services workers | 15 | 4.4% | |
| 52: Models, salespersons and demonstrators | 7 | 2.1% | |
| 6: Skilled agricultural and fishery workers | 3 | 0.9% | |
| 61: Market-oriented skilled agricultural and fishery workers | 3 | 0.9% | |
| 7: Craft and related trades workers | 118 | 34.7% | |
| 71: Extraction and building trades workers | 51 | 15% | |
| 72: Metal, machinery and related trades workers | 41 | 12.1% | |
| 73: Precision, handicraft, printing and related trades workers | 5 | 1.5% | |
| 74: Other craft and related trades workers | 21 | 6.2% | |
| 8: Plant and machine operators and assemblers | 25 | 7.4% | |
| 81: Stationary-plant and related operators | 1 | 0.3% | |
| 82: Machine operators and assemblers | 9 | 2.6% | |
| 83: Drivers and mobile-plant operators | 15 | 4.4% | |
| 9: Elementary occupations | 37 | 10.9% | |
| 91: Sales and services elementary occupations | 9 | 2.6% | |
| 93: Labourers in mining, construction, manufacturing and transport | 28 | 8.2% | |
1 Only submajor groups with at least one case are listed. Submajor groups according to Federal Statistical Office [16].
In the 1990 census, occupation as well as industry was reported in 79.1% (n = 340 of 430 individuals with 1990 census information). The following percentages in this and the next paragraph always refer to n = 340. One third of them worked as “Craft and related trades workers” (major group 7, 34.7%), of which the majority belonged to sub-major groups 71 (“Extraction and building trades workers”, 15.0%) and 72 (“Metal, machinery and related trades workers”, 12.1%). Other occupational groups with a substantial number of malignant pleural mesothelioma cases were “Technicians and associate professionals” (major group 3, 14.7%), most of whom were in sub-major group 31 (“Physical and engineering science associate professionals”, 9.1%), as well as “Legislators, senior officials and managers” (major group 1, 12.9%), where nearly all belonged to sub-major group 12 (“Corporate managers”, 12.4%). One out of ten individuals had an “Elementary occupation” (major group 9, 10.9%).
The industries mainly associated with malignant pleural mesothelioma were mechanical/electrical/precision engineering (17.4%), wood processing (5.9%), the railway industry (5.3%), construction industry (5.0%) and metal processing (4.7%).
Smoking status was available in 147 cases (30.9% of 476 individuals with malignant pleural mesothelioma). Of these, 42 (28.6%) were active smokers, 45 (30.6%) non-smokers and 60 (40.8%) former smokers at the time of lung dust analysis.
The histological subtype was reported in 398 cases (83.6% of 476 individuals with malignant pleural mesothelioma). In about half of them (n = 204, 51.3%) the epithelioid subtype had been identified. Biphasic and sarcomatoid mesothelioma were diagnosed in 153 cases (38.4%) and 41 cases (10.3%), respectively.
Canton of residence in Switzerland could be retrieved for all 430 individuals with malignant pleural mesothelioma linked to a 1990 census record from the SNC. Incidence rates for malignant pleural mesothelioma in males calculated from the Silag data are reported as age standardised rates (ASRs) for the period 1996-2015 and are shown in figure 2.
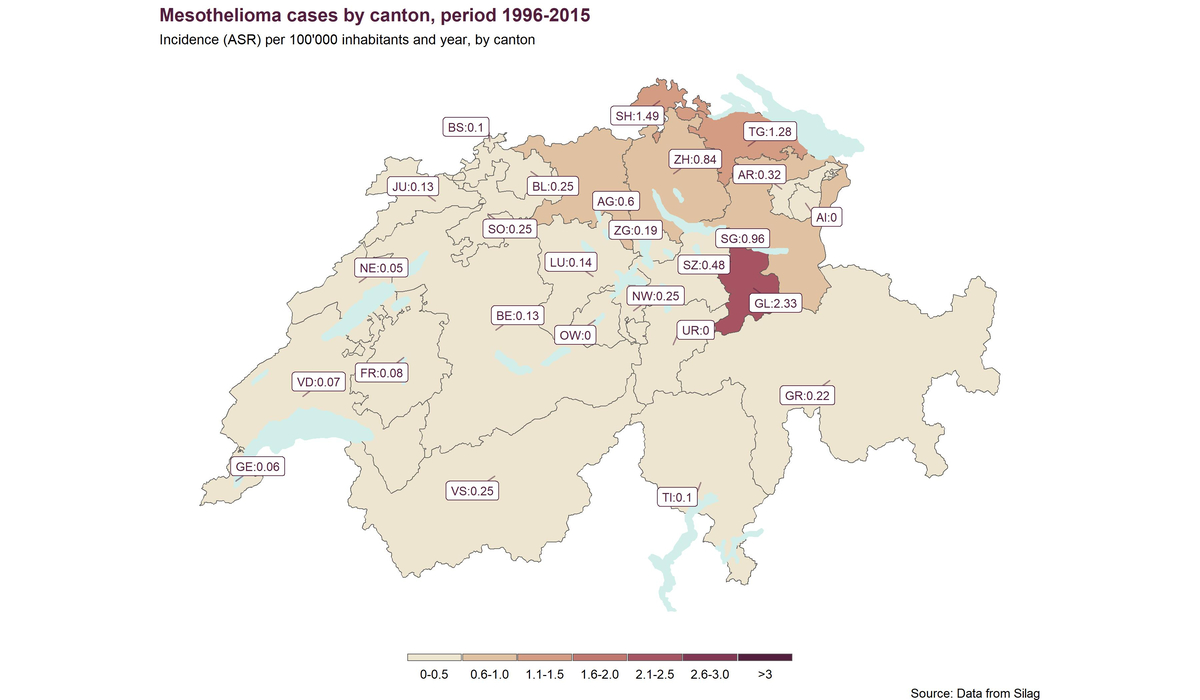
Figure 2 Age standardised rates of malignant pleural mesothelioma according to the Silag data 1996–2015
In eastern Switzerland, more cases per population were recorded than in western and southern Switzerland. The highest incidence was found in the canton of Glarus with an ASR of 2.33 cases/100,000 person years between 1996 and 2015. Figure 3 shows malignant pleural mesothelioma incidence rates in men in the same time period according to data from NICER [2].
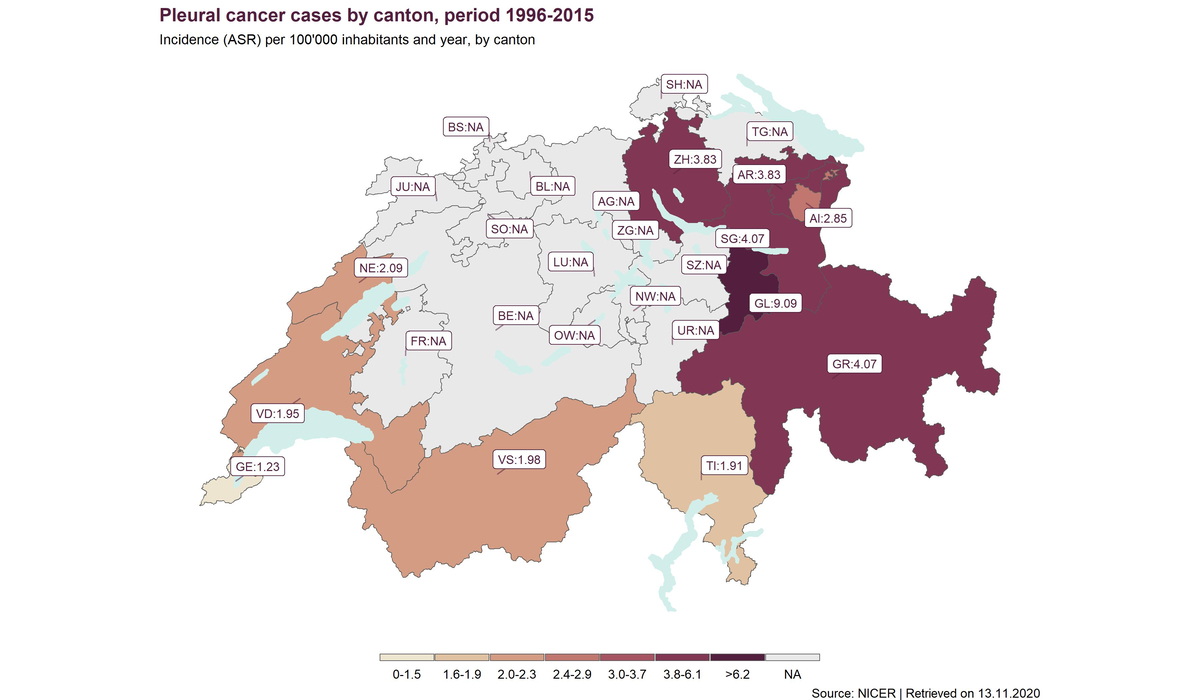
Figure 3 Age standardised rates of malignant pleural cancer according to the data of the National Institute for Cancer Epidemiology and Registration (aggregated data from 1996–2015, see methods)
Silag-based ASRs are clearly lower than those based on NICER data. However, the hotspot canton of Glarus stands out in both cases.
We were able to link data from the SNC to 94% of an asbestos-exposed clinical population by means of anonymous record linkage. From this linkage we obtained information on occupation and geographical distribution of malignant pleural mesothelioma in Switzerland.
In Switzerland, a linkage between data sources is difficult, as no universal personal identification number may be used. Under certain conditions, this problem can be circumvented by anonymous record linkage using common identification variables in the respective data sources.
The combination of postal code and date of birth has a high specificity and individuals with both pieces of information generally could be retrieved in the SNC. Even when the information was incomplete, a substantial proportion of individuals could be linked based on additional information as for example date or cause of death. The relatively good overall linkage success underlines the potential of the SNC for providing sociodemographic data but also for establishing a mortality follow-up of past study populations.
In our cohort, average age at the time of death of the individuals with malignant pleural mesothelioma (65.4 years) was comparable to those reported in other European countries such as Germany, but substantially lower than in the US [21, 22]. Other European studies, which looked at the age at the time of diagnosis instead of death, also found a similar age distribution [23–25]. This is to be expected because survival after diagnosis is generally limited to a couple of months or few years. The 5-year survival is described as only 5-10%, even with the newest therapeutic interventions [26].
Regarding the histological subtype, our results are comparable to other studies, with the epithelioid malignant pleural mesothelioma being the most common subtype [23, 25, 27]. However, individual studies with large tissue samples have found biphasic malignant pleural mesothelioma to be the most prevalent subtype [21]. These differences may be attributable to interobserver variability [28]. Compatible with previous observations, the sarcomatoid subtype is the least common subtype [21, 23, 25, 27].
Regarding occupations, comparability of our results with international literature is limited, since to our knowledge only one study used an ISCO classification [29]. Information on industries was available in several studies, but classifications are inconsistent and differ from our study.
The majority of patients in our cohort were blue-collar workers (ISCO major group 7–9], which corresponds to the literature [29–31]. The French study using the ISCO-68 classification found similar results to ours for the other major groups too: major groups 1 (legislators, senior officials and managers) and 3 (technicians and associate professionals) were also the next most frequent and the other major groups accounted for only few cases [29]. Remarkable is the considerable share of major group 1 in our data, which includes academic professions which would not be expected to be associated with asbestos exposure. Possible sources of asbestos exposure in such occupations were discussed in a study by Muller et al. [32]. They include occupational exposure (mainly in engineers), exposure during studies and internships, as well as environmental and domestic exposure [32]. Previous exposures in a non-academic job would be another conceivable explanation.
The industries most affected were manufacturing, construction and the railway industry, which is largely consistent with the literature [29, 31, 33–35]. Shipbuilding, which in certain coastal regions contributes a large proportion of malignant pleural mesothelioma cases, did not play a noticeable role in this Swiss cohort.
The incidences estimated from the Silag data amount on average to only about quarter of the incidences calculated by NICER. This can be explained by the fact that not all malignant pleural mesothelioma cases are included in the Silag dataset (see also under limitations). On the other hand the NICER diagnostic category investigated included not only malignant pleural mesothelioma (ICD-10 C45.0) but also other malignant neoplasms of the pleura (ICD-10 C38.4) [2].
The distribution of malignant pleural mesothelioma cases in our dataset showed a clear concentration in eastern Switzerland, especially in the canton of Glarus. This is consistent with the data from NICER. It should be noted that NICER data and Silag data have different sources.
In comparison with other countries [36], the incidence of malignant pleural mesothelioma in the canton of Glarus was high, which could be explained by the importance of the local asbestos industry in the past. In our data, some Swiss cantons had similar or higher mesothelioma incidence rates as described for Great Britain by Janes et al. [26].
The difference between eastern and southern/western Switzerland was more pronounced in the Silag sample than in the NICER sample. This indicates that French and Italian speaking Switzerland is underrepresented in the Silag dataset.
For the cantons which were not covered by a cancer registry (NA on the NICER map) our findings are novel.
It should be emphasised that the incidence for Switzerland as a whole might be overestimated by NICER, since a homogeneous distribution of cases between the cantons is presumed, but the cantons not covered by a cancer registry may have below average case numbers.
As described earlier the aetiology in a small proportion of cases, including women and children, appears not to be attributable to occupational asbestos exposure [37]. However, in such cases the development of mesothelioma may be explained by indirect exposure from asbestos-exposed workers living in the same household. This stresses the need for an accurate family history next to an occupational history.
In general it is of high importance to continue the investigations of pleural disease, including dust analysis, and to improve epidemiological data and registries for mesotheliomas.
Unlike in other European countries no national malignant pleural mesothelioma register exists in Switzerland. This makes our study valuable for characterising the extent of asbestos-related diseases in Switzerland. Our record linkage was successful with a linkage rate of 94%, minimising the risk of bias resulting from the linkage process. Further advantages are the considerable time period that was covered and the fact that cases were available from all parts of the country. However, it must be emphasised that the individuals in the Silag dataset are not representative for all subjects with malignant pleural mesothelioma in Switzerland. One reason is that lung dust analysis is currently only performed in those patients with a discrepancy between occupation and the diagnosis of malignant pleural mesothelioma. For cases with typical occupational exposure, malignant pleural mesothelioma has become recognised as an occupational disease that does not require additional lung dust analysis. Furthermore, samples are not sent to the Silag with equal diligence throughout Switzerland, especially in the Italian- and French-speaking parts of Switzerland, as suggested by a comparison with NICER data. A sufficient representation of cases from Latin Switzerland is therefore not guaranteed.
Another limitation is the fact that data on occupations and industries were missing to a significant extent and limited to 1990 census information, and may therefore not be representative for life course expositions.
We thank Dr Patrick Beeler MD for his valuable help regarding data preparation and data processing.
We thank the Swiss Federal Statistical Office for providing mortality and census data, and for the support, which made the construction of the Swiss National Cohort and this study possible.
The SNC and the record linkage with Silag were supported by the Swiss National Science Foundation (Grants 3347CO-108806, 33CS30-134273 and 33CS30–148415).
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest was disclosed.
1. Collegium R ; Collegium Ramazzini . The 18th Collegium Ramazzini statement: the global health dimensions of asbestos and asbestos-related diseases. Scand J Work Environ Health. 2016 Jan;42(1):86–90. https://doi.org/10.5271/sjweh.3541
2. Cancer Incidence in Switzerland . https://www.krebsregistrierung.ch/NicerReportFiles2018/EN/report/atlas.html [retrieved on 13 Nov. 2020]. NICER Foundation (National Institute for Cancer Epidemiology and Registration).
3. Unfallstatistik UVG 2020. SUVA Luzern: Koordinationsgruppe für die Statistik der Unfallversicherung UVG (KSUV); 2020.
4. Robinson BW , Musk AW , Lake RA . Malignant mesothelioma. Lancet. 2005 Jul;366(9483):397–408. https://doi.org/10.1016/S0140-6736(05)67025-0
5. Robinson BW , Lake RA . Advances in malignant mesothelioma. N Engl J Med. 2005 Oct;353(15):1591–603. https://doi.org/10.1056/NEJMra050152
6. Unfallstatistik UVG 2019. SUVA Luzern: Koordinationsgruppe für die Statistik der Unfallversicherung UVG (KSUV); 2019.
7. Bopp M , Spoerri A , Zwahlen M , Gutzwiller F , Paccaud F , Braun-Fahrländer C , et al. Cohort Profile: the Swiss National Cohort—a longitudinal study of 6.8 million people. Int J Epidemiol. 2009 Apr;38(2):379–84. https://doi.org/10.1093/ije/dyn042
8. Bopp M , Braun J , Faeh D , Gutzwiller F ; Swiss National Cohort Study Group . Establishing a follow-up of the Swiss MONICA participants (1984-1993): record linkage with census and mortality data. BMC Public Health. 2010 Sep;10(1):562. https://doi.org/10.1186/1471-2458-10-562
9. De Vuyst P , Karjalainen A , Dumortier P , Pairon JC , Monsó E , Brochard P , et al.; European Respiratory Society . Guidelines for mineral fibre analyses in biological samples: report of the ERS Working Group. Eur Respir J. 1998 Jun;11(6):1416–26. https://doi.org/10.1183/09031936.98.11061416
10. Spoerri A , Zwahlen M , Egger M , Bopp M . The Swiss National Cohort: a unique database for national and international researchers. Int J Public Health. 2010 Aug;55(4):239–42. https://doi.org/10.1007/s00038-010-0160-5
11. Nationales Institut für Krebsepidemiologie und –registrierung, NICER. https://www.nicer.org/ [retrieved on 24.01.2022]. NICER Foundation (National Institute for Cancer Epidemiology and Registration).
12. Beeler PE , Meier SL , Bopp M , Dressel H . Datenquellen zur Häufigkeit des malignen Pleuramesothelioms in der Schweiz seit 2001. Arbeitsmedizin, Sozialmedizin. Umweltmedizin. 2021;56(9):567–73.
13. Bopp M , Braun J , Faeh D , Egger M , Spoerri A , Zwahlen M , et al.; Swiss National Cohort Study Group . Variation in mortality patterns among the general population, study participants, and different types of nonparticipants: evidence from 25 years of follow-up. Am J Epidemiol. 2014 Nov;180(10):1028–35. https://doi.org/10.1093/aje/kwu226
14. Die 4 Sprachgebiete der Schweiz nach Gemeinden: Bundesamt für Statistik; 2016.
15. International Standard Classification of Occupations, version 1988 (ISCO-88). http://www.ilo.org/public/english/bureau/stat/isco/isco88/ [retrieved on 30 July 2020]. International Labour Organization (ILO); 1988.
16. ISCO 88 (COM) (International Standard Classification of Occupations). https://www.bfs.admin.ch/bfs/de/home/statistiken/arbeit-erwerb/nomenclaturen/isco-88-com.assetdetail.4082545.html [last retrieved on 24 Jan 2022]. Bundesamt für Statistik; 2017.
17. Meier U . Eidgenössische Volkszählung 1990: Verzeichnis der persönlichen Berufe. Bern: Bundesamt für Statistik; 1996.
18. Doll R , Cook P . Summarizing indices for comparison of cancer incidence data. Int J Cancer. 1967 May;2(3):269–79. https://doi.org/10.1002/ijc.2910020310
19. Data and methods. Cancer Incidence and Mortality in Switzerland by NICER. https://www.nicer.org/NicerReportFiles2015-2/EN/methods_file/methods.htm [retrieved on 15 Apr 2021]. NICER Foundation (National Institute for Cancer Epidemiology and Registration).
20. Ruggeri G . Making a map of COVID-19 incidence in Switzerland using ggplot2 and sf. https://medium.com/epfl-extension-school/making-a-map-of-covid-19-incidence-in-switzerland-using-ggplot2-and-sf-e765f8ea0221 [retrieved on 24 Mar 2021]. 2020.
21. Neumann V , Günthe S , Mülle KM , Fischer M . Malignant mesothelioma—german mesothelioma register 1987-1999. Int Arch Occup Environ Health. 2001 Aug;74(6):383–95. https://doi.org/10.1007/s004200100240
22. NIOSH . 2017. Work-Related Lung Disease Surveillance System (eWoRLD). 2017-897, https://wwwn.cdc.gov/eWorld/Data/897 [retrieved on 30 July 2020]. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Respiratory Health Division, Morgantown, WV.
23. Goldberg M , Imbernon E , Rolland P , Gilg Soit Ilg A , Savès M , de Quillacq A , et al. The French National Mesothelioma Surveillance Program. Occup Environ Med. 2006 Jun;63(6):390–5. https://doi.org/10.1136/oem.2005.023200
24. Marinaccio A , Binazzi A , Marzio DD , Scarselli A , Verardo M , Mirabelli D , et al.; ReNaM Working Group . Pleural malignant mesothelioma epidemic: incidence, modalities of asbestos exposure and occupations involved from the Italian National Register. Int J Cancer. 2012 May;130(9):2146–54. https://doi.org/10.1002/ijc.26229
25. Il registro nazionale dei Mesoteliomi - Sesto Rapporto. Milan: INAIL (Istituto nazionale per l'assicurazione contro gli infortuni sul lavoro); 2018.
26. Janes SM , Alrifai D , Fennell DA . Perspectives on the Treatment of Malignant Pleural Mesothelioma. N Engl J Med. 2021 Sep;385(13):1207–18. https://doi.org/10.1056/NEJMra1912719
27. Thomas A , Chen Y , Yu T , Gill A , Prasad V . Distinctive clinical characteristics of malignant mesothelioma in young patients. Oncotarget. 2015 Jun;6(18):16766–73. https://doi.org/10.18632/oncotarget.4414
28. Galateau Salle F , Le Stang N , Nicholson AG , Pissaloux D , Churg A , Klebe S , et al. New Insights on Diagnostic Reproducibility of Biphasic Mesotheliomas: A Multi-Institutional Evaluation by the International Mesothelioma Panel From the MESOPATH Reference Center. J Thorac Oncol. 2018 Aug;13(8):1189–203. https://doi.org/10.1016/j.jtho.2018.04.023
29. Rolland P , Gramond C , Lacourt A , Astoul P , Chamming’s S , Ducamp S , et al.; PNSM Study Group . Occupations and industries in France at high risk for pleural mesothelioma: A population-based case-control study (1998-2002). Am J Ind Med. 2010 Dec;53(12):1207–19. https://doi.org/10.1002/ajim.20895
30. Pukkala E , Martinsen JI , Lynge E , Gunnarsdottir HK , Sparén P , Tryggvadottir L , et al. Occupation and cancer - follow-up of 15 million people in five Nordic countries. Acta Oncol. 2009;48(5):646–790. https://doi.org/10.1080/02841860902913546
31. Roelofs CR , Kernan GJ , Davis LK , Clapp RW , Hunt PR . Mesothelioma and employment in massachusetts: analysis of cancer registry data 1988-2003. Am J Ind Med. 2013 Sep;56(9):985–92. https://doi.org/10.1002/ajim.22218
32. Müller KM , Dernbach AB , Neumann V . [Mesothelioma in academics. German Bochum mesothelioma register]. Chirurg. 2008 Mar; Suppl:99–102.
33. Yeung P , Rogers A , Johnson A . Distribution of mesothelioma cases in different occupational groups and industries in Australia, 1979-1995. Appl Occup Environ Hyg. 1999 Nov;14(11):759–67. https://doi.org/10.1080/104732299302189
34. Leigh J , Driscoll T . Malignant mesothelioma in Australia, 1945-2002. Int J Occup Environ Health. 2003 Jul-Sep;9(3):206–17. https://doi.org/10.1179/oeh.2003.9.3.206
35. Mensi C , De Matteis S , Dallari B , Riboldi L , Bertazzi PA , Consonni D . Incidence of mesothelioma in Lombardy, Italy: exposure to asbestos, time patterns and future projections. Occup Environ Med. 2016 Sep;73(9):607–13. https://doi.org/10.1136/oemed-2016-103652
36. Soberg MJ , van Zandwijk N . Incidence of malignant mesothelioma in New Zealand and Australia: a global snapshot. N Z Med J. 2015 Dec;128(1427):68–71.
37. Attanoos RL , Churg A , Galateau-Salle F , Gibbs AR , Roggli VL . Malignant Mesothelioma and Its Non-Asbestos Causes. Arch Pathol Lab Med. 2018 Jun;142(6):753–60. https://doi.org/10.5858/arpa.2017-0365-RA