
Figure 1 Clarity of the recommendations.
DOI: https://doi.org/10.4414/SMW.2022.w30161
The coronavirus disease COVID-19 can be a severe respiratory illness, which can lead to death in the most severe cases [1]. This SARS-CoV-2 virus was first identified in Wuhan, China in December 2019 [2]. With the worldwide spread of the virus, it became rapidly obvious that people aged over 65 years were at higher risk of suffering negative outcomes, including death [3–5]. The presence of the SARS-CoV-2 has been documented in Switzerland since 24 February 2020, with the first death occurring on 5 March 2020 [1]. The wide and rapid spread of the virus led the Swiss government to implement a series of public health restrictive measures, including closing restaurants and nonessential shops (table 1). Persons suffering from chronic diseases and people aged 65 years and over were considered as vulnerable populations. Hence, even though the government strategy to prevent the spread of coronavirus was directed towards the whole population, some measures targeted the older population more specifically. Most notably, the government strongly advised seniors to rigorously confine themselves and to avoid any contact with other generations. People aged 65 years and over were asked to stop seeing their children and grandchildren and to rely on relatives to do their grocery shopping for them [6–8].
Table 1Main public health measures in Switzerland.
| Date | Gatherings | Activities and events | Healthcare setting | At-risk population |
| 28 Feb. 2020 | Public or private events with more than 1000 persons prohibited. | |||
| 13 Mar. 2020 | Public or private events with more than 100 persons prohibited. | Restaurants, bars, discos and nightclubs with more than 50 persons prohibited. / Schools closed. | Older persons (i.e., 65+ years) advised to avoid crowded public places, including shops, and public transport. | |
| 16 Mar. 2020 | All public or private events prohibited. | Shops, restaurants, bars, museums, cinemas, hairdressing, and other business closed. | Older and at-risk persons should stay at home and avoid social contacts. / Older persons should not be involved in childcare. | |
| 20 Mar. 2020 | Gatherings of more than five persons in the public space prohibited. | Healthcare institutions prohibited from carrying out non-urgent examinations and interventions. |
Summary from the media releases issued by the Swiss Federal Council [25]
Soon after the beginning of the partial lockdown, the mass media reported that these recommendations might be as harmful as they are beneficial to seniors: the fact that they have very few opportunities for outdoor mobility and social contacts might negatively influence their well-being [9, 10]. Many healthy young-old adults, typically aged 65 to 75 years, did not consider themselves to be at higher risk than middle-aged ones and some of them did not quite understand why they had to comply with additional measures targeting older persons [11]. Besides, some seniors experienced features of ageism, such as being targeted by negative comments in the case of noncompliance [12, 13].
During the early stages of the epidemic, the mass media provided an overwhelming amount of information, thereby bringing overload and confusion in the whole population about the risk of getting infected and how to avoid infection, as well as about at-risk and prohibited behaviours [14].
Both the lack of a clear understanding of the recommendations and noncompliance with them might endanger the government’s strategy to contain the spread of the epidemic. Yet previous studies have shown that tailored and targeted public health communication may increase compliance [9–11, 15–17]. It is therefore paramount to identify the profile of those who considered that the main recommendations issued by the Swiss Federal Council during the first partial lockdown of the COVID-19 pandemic were unclear, as well as the characteristics of the seniors who did not comply with these recommendations. To our knowledge, no study has investigated these features yet. Similarly, except for a study based on a very small sample [18], the current research literature has not examined the association between personal characteristics and the impact of the partial lockdown on seniors’ daily life (be it difficulties or opportunities), and whether such an impact would differ depending on the seniors’ (non)compliance with the recommendations.
Thus, this study aimed to:
1. Identify the profile of seniors who considered that the main recommendations were unclear.
2. Identify the profile of seniors who did not comply with the main recommendations.
3. Examine the self-reported impact of the recommendations on the daily life of seniors.
In this study, data were drawn from the Lausanne Cohort 65+ study (Lc65+), the methods of which have been published previously [19, 20]. Briefly, this population-based study enrolled three randomly selected representative samples of about 1500 community-dwelling residents of the city of Lausanne, Switzerland aged 65 to 70 years in 2004, 2009 and 2014. The exclusion criteria were "being institutionalised" or "unable to respond due to cognitive impairment." The study follow-up included self-completed yearly questionnaires, as well as an in-person visit every third year.
On 17 April 2020, a four-page COVID-19 questionnaire was sent by mail to the 3087 active participants and asked them about their experience of the partial lockdown. By 19 June 2020, 2756 questionnaires had been completed (response rate 89%). Ten participants living in a nursing home were excluded from the analysis. As a result, the analyses were conducted on 2746 participants.
The Lc65+ study was approved by the Ethics Committee for Human Research in the Canton of Vaud (Initial protocol N°19/04, decision: 23 February 2004, and the specific amendment for the COVID-19 questionnaire: Protocol No PB_2016-02506, decision 10 April 2020). Every participant gave their written informed consent.
The COVID-19 questionnaire included two questions directly related to the four main recommendations of the Swiss Federal Council: (1) do not go grocery shopping; (2) do not use public transport; (3) stay at home; (4) avoid personal contact. In the first question, participants were asked to rate to what extent each recommendation seemed clear to them ("very clear", "quite clear", "quite confusing", and "very confusing"). Given the categorical nature of the variable, a dichotomous variable was created by grouping "very clear" and "quite clear" into "clear", and "quite confusing" and "very confusing" into "unclear". The second question was about the extent to which participants complied with each recommendation ("yes, rigorously", "generally, yes", "generally, no" and "not at all"). Again, a dichotomous variable was used by grouping "yes, rigorously" and "generally, yes" into "compliance", and "generally, no" and "not at all" into "noncompliance".
The impact of the partial lockdown on daily life was assessed by asking one question about difficulties and another about opportunities. The first question asked participants about how often ("less often than usual", "as often as usual", or "more often than usual") they have experienced each of the selected potential difficulties during the partial lockdown: I feel alone; I miss the physical contact with my relatives; I feel isolated from society and I feel like a burden to society; I hardly have any reference point to get through the day; I find it difficult to get food items; I feel dependent on other persons; I suffer from relational strain with relatives; I am a victim of domestic violence; and I feel stressed by the information reported in the media. The second question provided the same response options but focused on a selection of potential opportunities, namely: I feel well supported by people around me; I take time to read and learn; I feel useful to others; I have time for creative activities; people show solidarity towards me; I use digital tools to communicate; I eat healthy food; I feel some solidarity between generations; my friends, relatives or neighbours keep in touch with me on the phone or by text messages and show me that they care about me. These items were selected a priori by the study team on the basis of the expected difficulties and opportunities likely to arise from public health restrictive measures.
The numbers of difficulties and opportunities reported as more frequent than usual during the partial lockdown were separately summed up. Both scores ranged from 0 to 9 (where 9 corresponds to reporting that all difficulties or opportunities were experienced more frequently than usual) and were dichotomised into "fewer than 5", and "5 and above", this cut-off corresponding to the 20% of the sample with a higher level of difficulties or opportunities, respectively.
Characteristics pertaining to age and gender, origin (born in Switzerland, yes or no) and the level of education (compulsory schooling, apprenticeship, or higher education) were collected at recruitment (in 2004, 2009, and 2014, depending on the sample). The answers to the 2019 routine follow-up questionnaire provided data about soci-economic status (receiving means-tested government benefits or not), health status (reporting either zero, one, or more diagnosed conditions among the following: high blood pressure, high cholesterol level, coronary disease, heart failure, valve or myocardial disease, stroke, diabetes, chronic pulmonary disease, asthma, osteoporosis, bone fracture, arthritis, cancer, gastro-intestinal ulcers, depression, Parkinson’s disease, Alzheimer’s disease and human immunodeficiency virus infection), cognitive complaints (reporting problems with memory, attention or decision-making for the past 6 months at least), the frequency at which seniors would leave their home (at least 5 days per week vs less often), having a paid and/or volunteering activity, and being a caregiver.
Covariables regarding the seniors’ living environment during the partial lockdown (alone or not; house or apartment; in town, in the suburbs or in the country; with/without a balcony, a terrace, or a garden), their level of fear of the virus (for their own sake, for their relatives, for Switzerland and/or for humanity), and whether one of their relatives has been infected by the virus, were collected in the COVID-19 questionnaire.
Participants who answered "yes, a little" or "absolutely" to the question about their fear of the virus were categorised as afraid of the virus, as opposed to those who replied "neither yes nor no", "not really" or "not at all". Participants who feared for their own sake, for their relatives, for Switzerland and for humanity were categorised as having a high level of fear, whereas the others were categorised as having a low level of fear.
The perceived clarity of, compliance with and the impact of the recommendations were first examined using descriptive statistics. Even though the cohort began in 2004, participants were found to be still representative of the Lausanne population regarding age and sex distribution in 2016, so that no weighting procedure was used in the current analyses [21].
Bivariable analyses between each of the dependent variables (clarity of, compliance with, and impact of the recommendations) and independent variables were performed with chi-square tests. Then, a multivariable logistic regression model was run for each of the dependent variables. Age group and gender were systematically included as covariables, alongside variables significantly associated in the bivariable analyses. Interactions between gender and, respectively, age and level of fear of the virus, were tested for the association with clarity; none of them proved significant.
Given the relatively large number of covariables, the significance level was set at p <0.01. The sample size varies slightly owing to a few missing values in the COVID-19 questionnaire (with a maximum of 109 [4.0%] missing answers to one subquestion), as well as in previous questionnaires (less than 3.5% missing answers to each question). However, the highest number of observations lost in the multivariable models was 91 (3.3%), as the variable that had the highest number of missing values was not included in these models.
All analyses were performed with STATA 16 (StataCorp©).
As a result of the study design, the age of the 2746 participants ranged from 72 to 86 years, and 60.0% of participants were women (table 2). Three out of four participants were born in Switzerland and 45.0% had a higher education degree (baccalaureate, university, or high school). Almost half of them were living alone (44.5%) and had several conditions (47.5%). Approximately one in four participants (22.5%) had a relative who been infected by the coronavirus. Most participants thought that the virus constitutes a threat to them (71.6%), to their relatives (76.1%), to Switzerland (84.8%) or to humanity (86.0%). Almost two thirds (62.4%) reported that they feared for all these four items, which corresponds to our definition of a high level of fear.
Table 2Characteristics of the study sample.
| Characteristic | Percent | |
| Age | 72–76 years | 41.5% |
| 77–81 years | 33.5% | |
| 82–86 years | 25% | |
| Women | 60.4% | |
| Born in Switzerland | 75.5% | |
| Level of education | Compulsory schooling | 15.9% |
| Apprenticeship | 38.9% | |
| Higher education | 45.2% | |
| Living alone | 44.5% | |
| High level of fear of the virus | 62.4% | |
| Having a relative infected by the virus | 22.5% | |
| Receiving means-tested government benefits* | 25.8% | |
| Number of conditions* | 0 | 22.2% |
| 1 | 30.3% | |
| 2+ | 47.5% | |
| Reporting cognitive complaints* | 16.2% | |
| Leaving home frequently* | 77.2% | |
| Having a paid and/or volunteering activity* | 35.1% | |
| Being a caregiver* | 8% | |
* Based on information collected in 2019, i.e., before the pandemic.
Sample size: nmin = 2651; nmax = 2746
Each recommendation was rated as being very clear (i.e., clearly worded) by more than half of the participants, and an additional 25–30% rated them as quite clear (fig. 1). When "quite unclear" was grouped with "very unclear", the recommendation that respondents considered the most unclear was the one about grocery shopping, followed by the one about staying at home, whereas less than one in ten persons reported that the recommendations to avoid public transport and personal contact were unclear.
Figure 1 Clarity of the recommendations.
The proportion of participants who strictly complied with each recommendation ranged from 35.9% for staying at home to 75.4% for avoiding public transport (fig. 2). After "yes, rigorously" was grouped with "generally, yes", almost two thirds (63.6%) of the participants complied with all four recommendations. The level of noncompliance was highest regarding the recommendation not to go grocery shopping, followed by the ones about staying at home and avoiding public transport and personal contact.
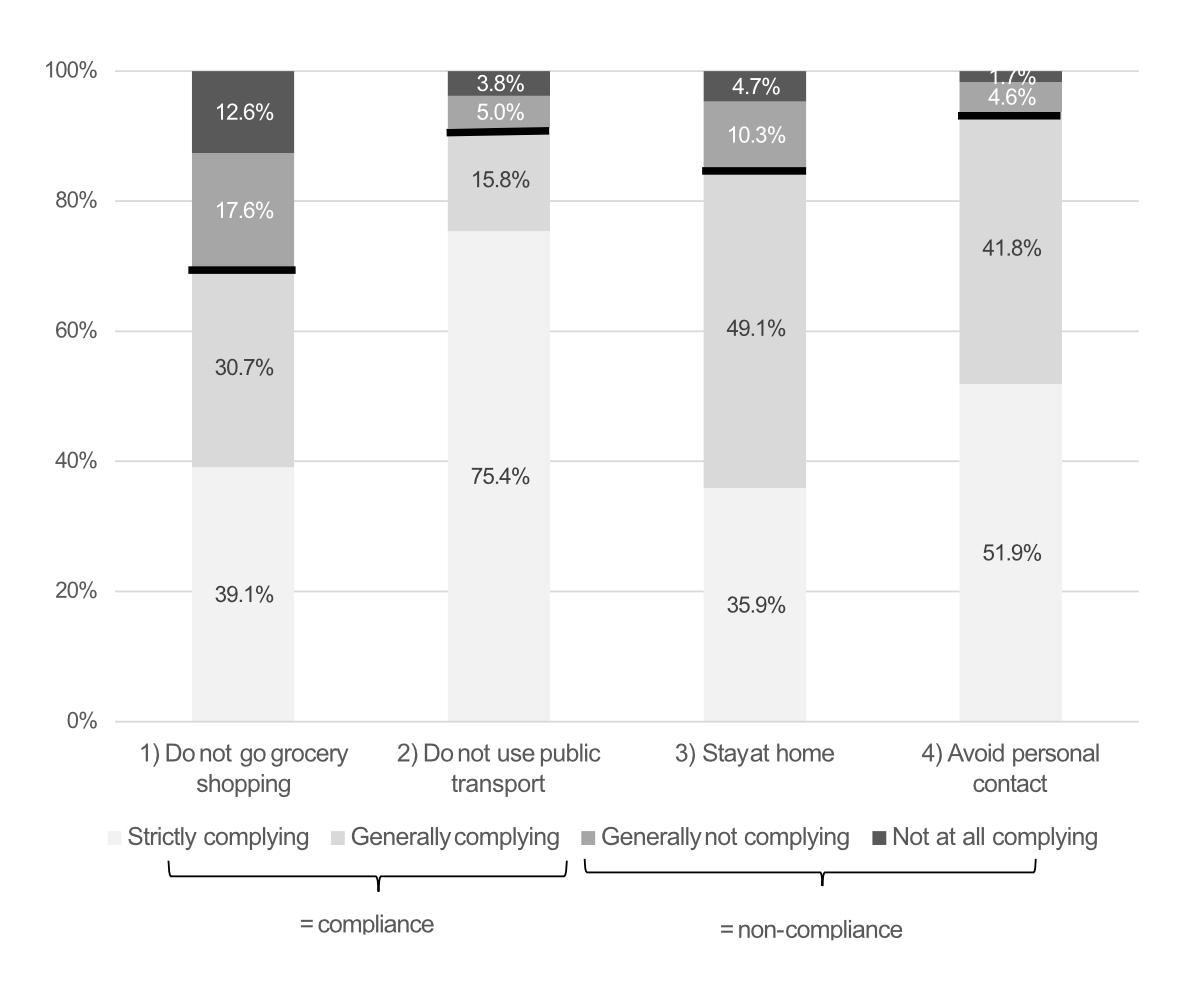
Figure 2 Compliance with the recommendations.
Overall, most participants reported that difficulties and opportunities occurred as frequently as usual. However, two items were reported as more frequent than usual by the majority of the participants (table 3): missing physical contact with relatives (63.5%) and friends, relatives or neighbours keeping in touch with them on the phone or by text messages and showing them that they care about them (55.8%). Some difficulties were reported as more frequent than usual, namely feeling stressed by the information in the media (44.5%) and feeling dependent on others (41.1%). Regarding opportunities, almost half of the participants felt that people showed solidarity towards them (43.6%) and between generations (46.1%) more often than usual, whereas 32.7% of them felt useful to others less often than usual. After summing up the difficulties or the opportunities, 18.1% of the participants indicated that at least five difficulties occurred more often than usual, and a similar proportion (22.2%) reported that at least five opportunities occurred more often than usual.
Table 3The impact of the partial lockdown on the daily life of seniors.
| Less often than usual | As often as usual | More often than usual | |
| Difficulties | |||
| I feel alone | 7.2% | 61.5% | 31.3% |
| I miss the physical contact with my relatives | 4.4% | 32% | 63.5% |
| I feel isolated from society and I feel like a burden to society | 10.4% | 55.9 | 33.6% |
| I hardly have any reference point to get through the day | 8.9% | 67.3% | 23.7% |
| I find it difficult to get food items | 12.1% | 71.9% | 15.9% |
| I feel dependent on other persons | 7.1% | 51.8% | 41.1% |
| I suffer from relational strain with relatives, friends, neighbours | 18.7% | 75.7% | 5.7% |
| I am a victim of domestic violence | 14.2% | 84.7% | 1.1% |
| I feel stressed by the information reported in the media | 4.7% | 50.8% | 44.5% |
| Opportunities | |||
| I feel well supported by people around me | 6.3% | 66.9% | 26.8% |
| I take time to read and learn | 2.7% | 68.6% | 28.7% |
| I feel useful to others | 32.7% | 59.8% | 7.5% |
| I have time for creative activities | 5.6% | 71.6 % | 22.8% |
| People show solidarity towards me | 2.6% | 53.8% | 43.6% |
| I use digital tools to communicate | 5% | 60.6% | 34.4% |
| I eat healthy food | 3.1% | 88.5% | 8.3% |
| I feel some solidarity between generations | 5.4% | 48.5% | 46.1% |
| My friends, relatives or neighbours keep in touch with me on the phone or by text messages and show me that they care about me | 1.6% | 42.6% | 55.8% |
Sample size: nmin = 2637, nmax = 2741
In bivariable analyses, gender was significantly associated with three out of four recommendations (table 4). Indeed, compared with women, men were more likely to rate the recommendations "do not go grocery shopping" (19.2% vs 13.1%, p <0.001), "do not use public transport" (11.6% vs 6.9%, p <0.001), and "avoid personal contact" (11.2% vs 7.6%, p <0.01) as unclear. Having a low level of fear of the virus was also significantly associated with rating the recommendations to "avoid public transport" (10.7% vs 7.7%, p <0.01), to "stay at home" (15.7% vs 11.2%, p <0.01) and to "avoid personal contact" (11.7% vs 7.5%, p <0.001) as unclear. Finally, caregivers were more likely to rate the recommendation to "avoid personal contact" as unclear than participants who were not caregivers (15.7% vs 8.6%, p <0.01).
Table 4Results from bivariable and multivariable analyses examining factors associated with rating the recommendations as unclear.
| Do not go grocery shopping | Do not use public transport | Stay at home | Avoid personal contact | |||||||||||||
| Unclear | p-value a | adjOR b | 95% CI b | Unclear | p-value a | adjOR b | 95% CI b | Unclear | p-value a | adjOR b | 95%CI ‡ | unclear | p-value a | adjOR b | 95% CI b | |
| Age group | ||||||||||||||||
| 72–76 years | 16.2% | 0.53 | ns | ns | 7.8% | 0.19 | ns | ns | 13.2% | 0.89 | ns | ns | 9.2% | 0.84 | ns | ns |
| 77–81 years | 14.5% | 8.9% | 12.5% | 8.6% | ||||||||||||
| 82–86 years | 15.9% | 10.2% | 12.6% | 9.4% | ||||||||||||
| Gender | ||||||||||||||||
| Women | 13.1% | <0.001 | 1.57 | 1.28–1.94 | 6.9% | <0.001 | 1.78 | 1.36–2.33** | 11.9% | 0.08 | ns | ns | 7.6% | <0.01 | 1.48 | 1.14–1.93* |
| Men | 19.2% | 11.6% | 14.2% | 11.2% | ||||||||||||
| Born in Switzerland | ||||||||||||||||
| Yes | 16.3% | 0.06 | 8.7% | 0.72 | 13.6% | 0.03 | 9.3% | 0.44 | ||||||||
| No | 13.3% | 9.1% | 10.3% | 8.3% | ||||||||||||
| Level of education | ||||||||||||||||
| Compulsory schooling | 15.9% | 0.62 | 10.4% | 0.37 | 12.6% | 0.85 | 9.9% | 0.37 | ||||||||
| Apprenticeship | 16.3% | 8.1% | 12.5% | 8.1% | ||||||||||||
| Higher education | 14.8% | 8.8% | 13.2% | 9.6% | ||||||||||||
| Living alone | ||||||||||||||||
| Yes | 16.7% | 0.12 | 10.2% | 0.01 | 14.3% | 0.03 | 9.9% | 0.19 | ||||||||
| No | 14.5% | 7.5% | 11.6% | 8.4% | ||||||||||||
| Level of fear of the virus | ||||||||||||||||
| Low | 17.7% | 0.02 | 10.7% | <0.01 | ns | ns | 15.7% | <0.01 | 1.10 | 1.04-1.17 | 11.7% | <0.001 | 1.13 | 1.06–1.21** | ||
| High | 14.3% | 7.7% | 11.2% | 7.5% | ||||||||||||
| Having a relative infected by the virus | ||||||||||||||||
| Yes | 14.1% | 0.24 | 7.1% | 0.09 | 12.3% | 0.66 | 8.1% | 0.28 | ||||||||
| No | 16.1% | 9.2% | 13.0% | 9.5% | ||||||||||||
| Receiving means-tested government benefitsc | ||||||||||||||||
| Yes | 16.9% | 0.29 | 8.8% | 0.87 | 13.5% | 0.64 | 9.6% | 0.52 | ||||||||
| No | 15.2% | 8.6% | 12.8% | 8.8% | ||||||||||||
| Having a paid and/or volunteering activityc | ||||||||||||||||
| Yes | 16.0% | 0.75 | 8.2% | 0.41 | 14.6% | 0.06 | 8.8% | 0.66 | ||||||||
| No | 15.5% | 9.1% | 12.0% | 9.3% | ||||||||||||
| Being a caregiverc | ||||||||||||||||
| Yes | 20.4% | 0.05 | 9.7% | 0.63 | 15.7% | 0.19 | 15.7% | <0.01 | 1.96 | 1.31–2.86* | ||||||
| No | 15.3% | 8.7% | 12.6% | 8.6% | ||||||||||||
| Cognitive complaintsc | ||||||||||||||||
| Yes | 15.9% | 0.93 | 11.7% | 0.02 | 13.1% | 0.92 | 10.4% | 0.35 | ||||||||
| No | 15.7% | 8.2% | 13% | 9% | ||||||||||||
“Unclear” corresponds to the answers "quite confusing" and "very confusing” grouped together, and “clear” to "very clear" and "almost clear."
In bivariable analyses, the sample size ranged from nmin = 2697 to nmax = 2738; in multivariable logistic models, the sample size ranged from nmin = 2677 to nmax = 2717.
a p-value from chi-square tests.
b adjusted odds ratio (adjOR) and 95% confidence interval (CI) from multivariable logistic models, adjusted for age and gender; * p <0.01; ** p <0.001
c Based on information collected in 2019, i.e., before the pandemic.
ns means that the variable was included in the multivariable logistic model, but the association did not remain significant.
In multivariable analyses, men remained more likely than women to rate the recommendations "do not use public transport" (adjOR 1.78, 95% CI 1.36–2.32; p <0.001) and "avoid personal contact’" (adjOR 1.48, 95% CI 1.14–1.93; p <0.01) as unclear. Male gender was also the only characteristic associated with rating the recommendation "do not go shopping" (adjOR 1.57, 95% CI 1.28–1.94) as unclear. Having a low level of fear of the virus (adjOR 1.13, 95% CI 1.06–1.21; p <0.001) and being a caregiver (adjOR 1.96, 95% CI 1.31–2.86; p <0.01) remained significantly associated with rating the recommendation "avoid personal contact" as unclear. Finally, a low level of fear of the virus was the only characteristic related to rating the recommendation "stay at home" as unclear (adjOR 1.10, 95% CI 1.07–1.17).
Table 5 displays the results of the bivariable and multivariable analyses regarding the association between covariables and the participants’ noncompliance with each recommendation. Interestingly, bivariable analyses showed a significant relationship between having a low level of fear of the virus and noncompliance with the four recommendations, namely 2do not go grocery shopping" (34.7% vs 27.7%, p <0.001), "do not use public transport" (11.6% vs 7.2%, p <0.001), "stay at home" (19.9% vs 12.0%, p <0.001) and "avoid personal contact" (9.4% vs 4.4%, p <0.001). Whenever participants rated one of the recommendations as unclear, they were significantly more likely to declare not complying with it: "do not go grocery shopping" (60.3% vs 24.7%, p <0.001); "do not use public transport" (29.7% vs 6.8%, p <0.001); "stay at home" (41.7% vs 11.0%, p <0.001) and "avoid personal contact" (30.2% vs 3.8%, p <0.001). Living alone was associated with not complying with three out of the four recommendations, i.e., about shopping (33.5% vs 27.5%, p <=.01), public transport (11.7% vs 6.3%, p <=.001) and personal contact (7.7% vs 5.0%, p <0.01). Other characteristics were associated with not complying with one or two out of the four recommendations.
Table 5Results from bivariable and multivariable analyses examining factors associated with not complying with the recommendations.
| Do not go grocery shopping | Do not use public transport | Stay at home | Avoid personal contact | |||||||||||||
| Non-compliance | p-value a | adjOR b | 95% CI b | Non-compliance | p-value a | adjOR b | 95% CI b | Non-compliance | p-value a | adjOR b | 95%CI b | Non-compliance | p-value a | adjOR b | 95%CI b | |
| Age group | ||||||||||||||||
| 72–76 years | 35.2% | <0.001 | 2.20 | 1.72–2.86** | 8.4% | 0.74 | ns | ns | 17.2% | <0.01 | ns | ns | 6.4% | 0.25 | ns | ns |
| 77–81 years | 31.1% | 1.85 | 1.45–2.38** | 9.4% | ns | ns | 14.5% | ns | ns | 7.0% | ns | ns | ||||
| 82–86 years | 21.0% | ref | ref | 8.6% | ns | ns | 11.7% | ns | ns | 5.0% | ns | ns | ||||
| Gender | ||||||||||||||||
| Women | 26.3% | <0.001 | 1.72 | 1.42–2.08** | 8.2% | 0.18 | ns | ns | 13.4% | <0.01 | ns | ns | 6.3% | 0.90 | ns | ns |
| Men | 36.4% | 9.7% | 17.3% | 6.2% | ||||||||||||
| Born in Switzerland | ||||||||||||||||
| Yes | 29.9% | 0.48 | 8.0% | 0.01 | 15.1% | 0.55 | 6.5% | 0.46 | ||||||||
| No | 31.4% | 11.2% | 14.2% | 5.6% | ||||||||||||
| Level of education | ||||||||||||||||
| Compulsory schooling | 26.6% | 0.16 | 12% | <0.01 | ns | ns | 10.8% | <0.01 | ns | ns | 6.2% | 0.97 | ||||
| Apprenticeship | 30.4% | 9.6% | 14.4% | 6.1% | ||||||||||||
| Higher education | 31.5% | 7% | 16.9% | 6.4% | ||||||||||||
| Living alone | ||||||||||||||||
| Yes | 33.5% | <0.01 | 1.64 | 1.35–1.98** | 11.7% | <0.001 | 1.87 | 1.38–2.53** | 15.3% | 0.58 | 7.7% | <0.01 | ns | ns | ||
| No | 27.5% | 6.3% | 14.5% | 5.0% | ||||||||||||
| Type of housing | ||||||||||||||||
| Apartment | 31.1% | 0.01 | 9.5% | <0.01 | ns | ns | 14.8% | 0.65 | 6.2% | 0.94 | ||||||
| House | 24.5% | 4.3% | 15.8% | 6.3% | ||||||||||||
| Location | ||||||||||||||||
| City | 30.9% | 0.26 | 9.5% | 0.02 | 14.8% | 0.47 | 6.3% | 0.02 | ||||||||
| Suburbs | 28.8% | 6.4% | 16.1% | 7.3% | ||||||||||||
| Country | 25.0% | 4.4% | 11.9% | 0.7% | ||||||||||||
| Balcony | ||||||||||||||||
| Yes | 29.8% | 0.13 | 8.8% | 0.46 | 15% | 0.84 | 6.1% | 0.31 | ||||||||
| No | 33.6% | 9.9% | 14.6% | 7.4% | ||||||||||||
| Terrace or garden | ||||||||||||||||
| Yes | 28.7% | 0.18 | 7.2% | 0.06 | 17.3% | 0.04 | 6.2% | 0.94 | ||||||||
| No | 31.3% | 9.4% | 14.3% | 6.3% | ||||||||||||
| Level of fear of the virus | ||||||||||||||||
| Low | 34.7% | <0.001 | 1.07 | 1.02–1.12* | 11.6% | <0.001 | 1.11 | 1.03– 1.18* | 19.9% | <0.001 | 1.14 | 1.08– 1.21** | 9.4% | <0.001 | 1.19 | 1.10– 1.30** |
| High | 27.7% | 7.2% | 12.0% | 4.4% | ||||||||||||
| Relatives infected with the virus | ||||||||||||||||
| Yes | 26.4% | 0.02 | 5.9% | <0.01 | ns | ns | 16.1% | 0.31 | 4.9% | 0.12 | ||||||
| No | 31.5% | 9.5% | 14.5% | 6.7% | ||||||||||||
| Receiving means-tested government benefitsc | ||||||||||||||||
| Yes | 32.3% | 0.22 | 10.6% | 0.05 | 14.6% | 0.69 | 6.7% | 0.47 | ||||||||
| No | 29.8% | 8.1% | 15.3% | 6% | ||||||||||||
| Number of conditionsc | ||||||||||||||||
| 0 | 35.3% | <0.01 | ns | ns | 9.4% | 0.54 | 18.9% | <0.01 | ns | ns | 8.0% | 0.08 | ||||
| 1 | 31.8% | 7.9% | 15.8% | 6.6% | ||||||||||||
| 2+ | 27.0% | 9.2% | 13.0% | 5.4% | ||||||||||||
| Leaving home frequentlyc | ||||||||||||||||
| Yes | 33.3% | <0.001 | 1.64 | 1.35–1.98** | 8.9% | 0.95 | 17.7% | <0.001 | 2.45 | 1.72– 3.57** | 6.7% | 0.09 | ||||
| No | 20.5% | 8.8% | 6.3% | 4.8% | ||||||||||||
| Having a paid and/or volunteering activityc | ||||||||||||||||
| Yes | 31.4% | 0.40 | 7.5% | 0.06 | 18.6% | <0.001 | ns | ns | 6.6% | 0.63 | ||||||
| No | 29.8% | 9.6% | 13.2% | 6.2% | ||||||||||||
| Being a caregiverc | ||||||||||||||||
| Yes | 35.2% | 0.11 | 11.2% | 0.19 | 20.8% | 0.01 | 8.8% | 0.12 | ||||||||
| No | 30% | 8.6% | 14.6% | 6.1% | ||||||||||||
| Recommendation rated as clear | ||||||||||||||||
| Yes | 24.7% | <0.001 | 4.65 | 3.70–5.83** | 6.8% | <0.001 | 5.31 | 3.79–7.43** | 11% | <0.001 | 5.27 | 4.08– 6.82** | 3.8% | <0.001 | 11.16 | 7.84– 15.88** |
| No | 60.3% | 29.7% | 41.7% | 30.2% | ||||||||||||
"Noncompliance" corresponds to the answers "generally no" and "not at all" grouped together, whereas "compliance" emcompasses the answers "strictly yes" and "generally yes".
In bivariable analyses, the sample size ranged from nmin = 2641 to nmax = 2744; in multivariable logistic models, the sample size ranged from nmin = 2655 to nmax = 2707.
a p-value from chi-square tests.
b adjusted odds ratio (adjOR) and 95% confidence interval (CI) from multivariable logistic models, adjusted for age and gender; * p <0.01; ** p <0.001.
c Based on information collected in 2019, i.e., before the pandemic.
ns means that the variable was included in the multivariable logistic model, but the association did not remain significant.
Multivariable analyses revealed an independent association between not complying with the recommendation and reporting a low level of fear of the virus, as well as with rating the recommendation as unclear. Living alone remained was significantly associated with not complying with two recommendations, namely "do not go grocery shopping" (adjOR 1.63, 95% CI 1.35–1.98; p <0.001) and "do not use public transport" (adjOR 1.68, 95% CI 1.26–2.24; p <0.001). A significant relationship was found between leaving home frequently before the pandemic and not complying with the recommendations about shopping (adjOR 1.64, 95%CI 1.3–2.08; p <0.001) and about staying at home (adjOR 2.44, 95% CI 1.72–3.57; p <0.001). Finally, younger age was associated with not complying with the recommendation about shopping (adjOR72-76yrs 2.22, 95% CI 1.72–2.86; p <0.001, and adjOR77-81yrs 1.85, 95% CI 1.45–2.38; p <0.001), and a similar result was observed in men (adjOR 1.71, 95% CI 1.41–2.07; p <0.001).
Participants who respected all four recommendations were more likely than the others to report at least five difficulties (20.5% vs 13.9%, p<.001, Table 6), as well as at least five opportunities (25.9% vs 16.0%, p<.001). In bivariable analyses, reporting at least five difficulties was more frequent among participants with two or more chronic diseases than in those reporting only one or no disease (21.3% vs 15.0% and 16.0%, p<.001). Participants who indicated that they went frequently out of their home (23.8% vs 16.9%, p<.001) or that they had engaged in a paid and/or volunteering activity (28.7% vs 18.8%, p<.001) in the year before the pandemic were more likely to report at least five opportunities.
Table 6Results from bivariable and multivariable analyses examining factors associated with the impact of the partial lockdown on the daily life of seniors.
| Difficulties (at least 5) | Opportunities (at least 5) | |||||||
| No | p-value a | adjOR b | 95% CI b | No | p-value a | adjOR b | 95% CI b | |
| Age group | ||||||||
| 72–76 years | 82.3% | 0.49 | ns | ns | 74.9% | 0.01 | ns | ns |
| 77–81 years | 82.5% | 79.6% | ||||||
| 82–86 years | 80.3% | 80.1% | ||||||
| Gender | ||||||||
| Women | 80.4% | 0.01 | ns | ns | 76.1% | 0.01 | ns | ns |
| Men | 84.1% | 80.2% | ||||||
| Living alone | ||||||||
| Yes | 80.1% | 0.03 | 77.5% | 0.80 | ||||
| No | 83.3% | 77.9% | ||||||
| Location | ||||||||
| City | 81.2% | 0.07 | 78.2% | 0.54 | ||||
| Suburbs | 81.9% | 76.4% | ||||||
| Country | 89.1% | 75.2% | ||||||
| Number of conditionsc | ||||||||
| 0 | 84.0% | <0.001 | ns | ns | 78.0% | 0.70 | ||
| 1 | 85.0% | 76.8% | ||||||
| 2+ | 78.7% | 78.3% | ||||||
| Leaving home frequentlyc | ||||||||
| Yes | 82.1% | 0.41 | 76.2% | <0.001 | 1.50 | 1.18– 1.91* | ||
| No | 80.7% | 83.1% | ||||||
| Having a paid and/or volunteering activityc | ||||||||
| Yes | 82.8% | 0.35 | 71.3% | <0.001 | 1.62 | 1.33– 1.97** | ||
| No | 81.3% | 81.2% | ||||||
| Compliance with all four recommendations | ||||||||
| Yes | 79.5% | <0.001 | 1.56 | 1.25–1.93** | 74.1% | <0.001 | 1.97 | 1.60– 2.42** |
| No | 86.1% | 84.0% | ||||||
No = a score between 0 and 4; Yes = a score between 5 and 9. The score ranges from 0 to 9, where 0 corresponds to reporting difficulties/opportunities not more often than usual and where 1 to 9 is the number of difficulties/opportunities reported as experienced more often than usual.
In bivariable analyses, the sample size ranged from nmin = 2709 to nmax = 2746; in multivariable logistic models, the sample size ranged from nmin = 2690 to nmax = 2697.
a p-value from chi-square tests.
b odds ratio (OR) and 95% confidence interval (CI) from multivariable logistic models, adjusted for age and gender; * p <0.01; ** p <0.001.
c Based on information collected in 2019, i.e., before the pandemic.
ns means that the variable was included in the multivariable logistic model, but the association did not remain significant
In multivariable analyses, complying with all four recommendations remained significantly associated with reporting difficulties more often than usual (adjOR 1.59, 95% CI 1.28–1.97; p <0.001) as well as with reporting opportunities more often than usual (adjOR 1.97, 95% CI 1.61–2.42; p <0.001). Finally, being active before the pandemic (adjORpaid/volunteering activity 1.67, 95% CI 1.38–2.02; p <0.001; and adjORleaving home frequently 1.52, 95% CI 1.19–1.93; p = 0.001) remained associated with experiencing opportunities more often than usual.
Identifying the characteristics of seniors who do not understand and do not comply with the COVID-19-related recommendations as well as assessing the impact of such recommendations on the daily life of seniors is essential for developing effective public health campaigns in the current and future pandemics. Indeed, more specifically targeted public health communication may increase the compliance with the recommendations, which may, in turn, reduce the risk of COVID-19 resurgence [15]. Data from a longitudinal cohort of older persons, including a specific questionnaire completed during the COVID-19 pandemic, were leveraged to examine what factors were associated with rating the main recommendations as unclear, not complying with them, and with the impact on seniors’ daily life.
Male gender was the characteristic most consistently related with rating the recommendations as unclear. An independent association was observed in three out of the four recommendations, even after accounting for potential confounders. To our knowledge, only one publication based on an online survey in Sweden directly reported gender-specific results about how clear the recommendations were from the point of view of the older population. That study supports our findings, as it indicated that the government’s recommendations were less often rated as clear by men [22]. Other studies focused rather on self-reported knowledge of the COVID-19 disease and of the measures taken to control the epidemic, and found that both were poorer in men [23–25]. The explanation for these findings may be that men are more likely than women to be less interested in health matters and to be less prone to prevention or to accept restrictions for the sake of prevention [26, 27].
In this study, we expected to find an association between a lower level of education and rating the recommendations as unclear. In a loosely comparable way, one of the several studies that have examined the role of education in understanding the disease reported an association between level of education and familiarity with the recommendations, which was lower among less educated respondents [28]. However, no such association was found in this study. This unexpected finding may be the consequence of a possible misunderstanding of the question about how clear the wording of the recommendations was to respondents: instead, the participants may have understood that the question was about their understanding of why these measures are being implemented. A similar phenomenon might also be involved in the relationship we observed between having a low level of fear of the virus and rating the recommendations to "stay at home" and "avoid personal contacts" as unclear. This finding may suggest that the persons who do not consider COVID-19 as a threat for themselves or for other persons, do not understand why such measures might be necessary, even though they might have understood what the recommendations expected them (not) to do. Such a result not only highlights that effective public health communication should give clear and coherent information about the disease, about how it spreads and how to avoid getting it, as well as clearly worded and coherent recommendations. It also shows the importance of ensuring that the messages are appropriately tailored to the different subgroups of the population.
Our finding that perceiving the recommendations as unclear was the characteristic most strongly associated with a low level of compliance with all the recommendations underlines the importance of producing clear messages. Although the cross-sectional nature of the study does not rule out the possibility that the persons who do not want to comply with restrictions might be prone to rate the recommendations as unclear, it seems reasonable to hypothesise that a clear understanding of the meaning of the recommendations is a prerequisite for complying with them. This finding further points to the necessity of testing the clear understanding of important public health messages by the target population before communicating them. Interestingly, a review of the factors influencing the compliance with recommendations during epidemics further found that the population were more likely to comply with these when they had a more extensive knowledge of the virus, when they perceived protective behaviours as highly effective or rated the information communicated by authorities as coherent and transparent [29]. In light of the above, it seems very relevant that authorities should explain the foundation of their recommendations and what specific parameters these influence.
Seniors who reported a low level of fear of the virus were less likely to comply with all the recommendations. This result is also supported by the literature, including a study carried out in England and in the USA [30]. It similarly observed that fearing the virus predicted the adoption of the behaviours recommended by the government in matters of public health. Furthermore, according to a study conducted in 2003 on the outbreak of the severe acute respiratory syndrome in Hong Kong, respondents with a higher perception of the virus-related risk were most likely to take comprehensive precautions against infection [31].
In this study, both younger age and male gender were associated with a lower level of compliance with the recommendation "do not go grocery shopping", whereas no significant association with any other recommendation was found. Similarly, other studies indicated that younger seniors and men were less likely to comply with COVID-19 public health measures [28, 31–33]. This association with age might be in line with the fact that the recommendations issued by the Federal Council in March 2020 targeted all persons above the age of 65 years as a single at-risk group. The relevance of this strategy has been questioned by young healthy seniors, because statistics about COVID-19 and mortality indicated that the death rate was up to five times lower among people aged 70–79 years than in the older ones [3]. It also raised feelings of stigmatisation in seniors. Moreover, young seniors, being quite an active population, experienced more disruption in their daily life due to the restrictions than older seniors did. Therefore, should similar restrictive recommendations be needed again in the future, the implementation should differentiate people aged 65 to 79 years from those aged 80 years and over – a strategy that seems reasonable, considering the increase in total and healthy life expectancy. Furthermore, differentiating between different old age categories would be in line with the Health Belief Model, a widely known theory of health-related behaviour. According to this, people's beliefs about whether they are at risk for a disease and their perception of the efficacy and disadvantages of the measures against infection influence their likeliness to undertake them [34]. Notably, COVID-19 vaccination was introduced in December 2020 in Switzerland, first among the most vulnerable seniors (aged 75 and over or reporting comorbidities), then in all persons from age 65 years on. As vaccination led to a rapid reduction of COVID-19 hospitalisations and death in these subgroups [35], it may also have influenced how subgroups of seniors perceived their own risk for COVID-19 [36].
Men have been found to be generally less prone than women to comply with preventive behaviours during the influenza pandemic [29]. Several factors likely interplay to explain this contrast, but men’s more risk-taking attitude was mentioned, and might result from biological specificities such as higher testosterone levels and from social norms [37, 38]. Consequently, one way of better reaching the male population might be to put more emphasis on the advantages, and not so much on the risks for oneself, when communicating the recommendations. Nevertheless, underlining the risks that o ther people and their loved ones are facing might also generate feelings of responsibility in this group [39].
In the early stages of the partial lockdown, the impact of COVID-19 restrictions was regarded as especially negative for older persons. Studies later showed that the older population was rather more resilient than the younger population and suffered less from mental health issues [40-42]. We also found an independent association between strongly complying with recommendations and reporting facing difficulties as well as opportunities more often than usual. It may be that, while facing restrictions in their activities and social contacts, many seniors managed to reorganise their occupations. A study conducted in Ireland highlighted that engaging in exercise, going outdoor for walks or gardening, pursuing hobbies, and looking after children were associated with great benefits in terms of well-being [43]. Similarly, this study found that the seniors who reported going out at least five days per week before the pandemic, as well as those who had a remunerated or voluntary activity, experienced a significant increase in opportunities during this period. In this regard, and as documented in previous studies, one might expect a more negative impact of the pandemic-related restrictions in persons with chronic health problems [44]. However, after accounting for other personal characteristics, this study did not find any significant association between having a chronic disease and facing difficulties more often than usual during this period. One of the potential reasons for this might be that these persons benefited from much more support and help during the partial lockdown than they usually would – which might counterbalance the difficulties they were facing – and that this might have helped them be more resilient and better able to regulate their emotions [45].
A major strength of this study is that it was based on a large sample of older persons and representative of the general population of the same age. Furthermore, external validity is supported by the findings of studies conducted in Switzerland and other countries with similar proportions of respondents who considered the virus as a threat, and of respondents who followed the recommendations [22, 32, 46, 47], whether they were strictly imposed as in Italy or more loosely recommended as in Sweden [22, 32, 48, 49]. In addition, the questionnaire was wisely sent in the middle of the first partial lockdown in Switzerland and had a very high response rate. Finally, this study took a large set of socioeconomic and health-related confounders into account.
This study has some limitations. First, data were self-reported, which might result in respondents overestimating their compliance with public health recommendations. Second, the data on perceived opportunities and difficulties were based on quantitative variables about the frequency of occurrence during the partial lockdown as compared with before, without any information about the perceived severity of difficulties or meaning of the opportunities, which would rather pertain to a qualitative study. Lastly, the questionnaire did not ask participants about their trust in the government, a factor that might influence their compliance, although inconsistently [44]. However, that piece of information is unlikely to change our results fundamentally. A survey conducted among Swiss adults during the same period revealed that a large part of the population trusted the federal and local authorities, without any significant difference according to age, gender or political stance [50].
Overall, a high proportion of seniors rated the main COVID-19 recommendations ("do not go grocery shopping", "do not use public transports", "avoid personal contact", and "stay at home") as clear and observed them. However, some subgroups of this older population, notably younger seniors, men, as well as the respondents who did not consider the virus as a threat, were less likely to understand the meaning of the recommendations and to follow them. Therefore, public health communication should be tailored to these subgroups, so as to improve their understanding of the recommendations and, consequently, their compliance with these.
Data are not publicly available and the authors do not have permission to share data. Any request can be addressed to the corresponding author.
We are deeply grateful to all participants of the Lc65+ study. We also thank the past and present Lc65+ collaborators for their involvement at all stages of the study, as well as Prof. Brigitte Santos-Eggimann for her review of the manuscript.
Author contributions: All the authors meet criteria for authorship stated in the Uniform Requirements for Manuscripts Submitted to Biomedical Journals and all four ICJME criteria. In particular, authors contribution to the manuscript were the following: -Conceptualisation, methodology: all the authors. -Formal analyses and writing original draft: CP. -Supervision: LSr-B. -Review, editing and validation of final text: all the authors.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest was disclosed.
This work did not receive any funding from agencies in the public, commercial, or not-for-profit sectors. The Lc65 + study has been supported by University of Lausanne Hospital Centre; University of Lausanne Department of Ambulatory Care and Community Medicine; Canton de Vaud Department of Public Health; City of Lausanne; Loterie Romande [research grant 2006–2008]; Lausanne University Faculty of Biology and Medicine [multidisciplinary research grant 2006]; Swiss National Foundation for Scientific Research [grant 3247B0-120795/1]; and Fondation Médecine Sociale et Préventive, Lausanne. The sponsors had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
1. Office Fédéral de la santé publique. Coronavirus: situation en Suisse: Office fédéral de la santé publique; 2020 [Available from: https://www.bag.admin.ch/bag/fr/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/novel-cov/situation-schweiz-und-international.html
2. Liu YC , Kuo RL , Shih SR . COVID-19: the first documented coronavirus pandemic in history. Biomed J. 2020 Aug;43(4):328–33. https://doi.org/10.1016/j.bj.2020.04.007
3. World Health Organization . COVID-19 Strategy Update. 2020. https://www.who.int/publications/m/item/covid-19-strategy-update
4. United Nations . The impact of COVID-19 on older persons. 2020. https://www.un.org/sites/un2.un.org/files/un_policy_brief_on_covid-19_and_older_persons_1_may_2020.pdf
5. Nguyen S , Major K , Cochet C , Bizzozzero T , Barbarossa L , Bosshard W , et al. [COVID-19 infection in the elderly in French-speaking Switzerland: an inventory of beliefs, convictions and certainties]. Rev Med Suisse. 2020 Apr;16(691-2):835–8. https://doi.org/10.53738/REVMED.2020.16.691.0835
6. Office Fédéral de la santé publique. Nouveau coronavirus : campagne d’information de l’OFSP intitulée « Voici comment nous protéger » [press release]. 2020.
7. Office Fédéral de la santé publique. Le Conseil fédéral renforce les mesures contre le coronavirus pour protéger la santé de la population et soutient les secteurs touchés [press release]. 2020.
8. Office Fédéral de la santé publique. Coronavirus : le Conseil fédéral qualifie la situation de « situation extraordinaire » et renforce les mesures [press release]. 2020.
9. Hartmann D . Mourir de «fatigue de vivre». Courrier. 2020.
10. Rubín MA ; Domínguez N . La pandémie a mis à nu la fragilité des seniors. Swiss Info (swissinfo.ch).
11. Genecand M . Confinement, la révolte des aînés. Le Temps. 2020 Apr;2020:23.
12. Ayalon L , Chasteen A , Diehl M , Levy BR , Neupert SD , Rothermund K , et al. Aging in Times of the COVID-19 Pandemic: Avoiding Ageism and Fostering Intergenerational Solidarity. J Gerontol B Psychol Sci Soc Sci. 2021 Jan;76(2):e49–52. https://doi.org/10.1093/geronb/gbaa051
13. Seifert A . Older adults during the COVID-19 pandemic - Forgotten and stigmatized? Int Soc Work. 2021;64(2):275–8. https://doi.org/10.1177/0020872820969779
14. Tagliabue F , Galassi L , Mariani P . The “Pandemic” of Disinformation in COVID-19. SN Compr Clin Med. 2020 Aug;•••:1–3.
15. Prati G , Pietrantoni L , Zani B . A social-cognitive model of pandemic influenza H1N1 risk perception and recommended behaviors in Italy. Risk Anal. 2011 Apr;31(4):645–56. https://doi.org/10.1111/j.1539-6924.2010.01529.x
16. Asmundson GJ , Taylor S . Coronaphobia: fear and the 2019-nCoV outbreak. J Anxiety Disord. 2020 Mar;70:102196. https://doi.org/10.1016/j.janxdis.2020.102196
17. Lennon RP , Sakya SM , Miller EL , Snyder B , Yaman T , Zgierska AE , et al. Public Intent to Comply with COVID-19 Public Health Recommendations. Health Lit Res Pract. 2020 Aug;4(3):e161–5. https://doi.org/10.3928/24748307-20200708-01
18. Macdonald B , Hülür G . Well-Being and Loneliness in Swiss Older Adults During the COVID-19 Pandemic: The Role of Social Relationships. Gerontologist. 2021 Feb;61(2):240–50. https://doi.org/10.1093/geront/gnaa194
19. Santos-Eggimann B , Karmaniola A , Seematter-Bagnoud L , Spagnoli J , Büla C , Cornuz J , et al. The Lausanne cohort Lc65+: a population-based prospective study of the manifestations, determinants and outcomes of frailty. BMC Geriatr. 2008 Aug;8(1):20. https://doi.org/10.1186/1471-2318-8-20
20. Henchoz Y , Blanco JM , Fustinoni S , Nanchen D , Büla C , Seematter-Bagnoud L , et al. Cohort Profile: the Lausanne cohort 65+ (Lc65+). Int J Epidemiol. 2021 Nov;dyab245. https://doi.org/10.1093/ije/dyab245
21. Abolhassani N , Santos-Eggimann B , Büla C , Goy R , Guessous I , Henchoz Y . Quality of life profile in three cohorts of community-dwelling Swiss older people. BMC Geriatr. 2019 Apr;19(1):96. https://doi.org/10.1186/s12877-019-1112-4
22. Gustavsson J , Beckman L . Compliance to Recommendations and Mental Health Consequences among Elderly in Sweden during the Initial Phase of the COVID-19 Pandemic-A Cross Sectional Online Survey. Int J Environ Res Public Health. 2020 Jul;17(15):E5380. https://doi.org/10.3390/ijerph17155380
23. Rattay P , Michalski N , Domanska OM , Kaltwasser A , De Bock F , Wieler LH , et al. Differences in risk perception, knowledge and protective behaviour regarding COVID-19 by education level among women and men in Germany. Results from the COVID-19 Snapshot Monitoring (COSMO) study. PLoS One. 2021 May;16(5):e0251694. https://doi.org/10.1371/journal.pone.0251694
24. Zhong BL , Luo W , Li HM , Zhang QQ , Liu XG , Li WT , et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020 Mar;16(10):1745–52. https://doi.org/10.7150/ijbs.45221
25. Lazarus JV , Ratzan S , Palayew A , Billari FC , Binagwaho A , Kimball S , et al. COVID-SCORE: A global survey to assess public perceptions of government responses to COVID-19 (COVID-SCORE-10). PLoS One. 2020 Oct;15(10):e0240011. https://doi.org/10.1371/journal.pone.0240011
26. Beier ME , Ackerman PL . Determinants of health knowledge: an investigation of age, gender, abilities, personality, and interests. J Pers Soc Psychol. 2003 Feb;84(2):439–48. https://doi.org/10.1037/0022-3514.84.2.439
27. Molina-Barceló A , Salas Trejo D , Peiró-Pérez R , Málaga López A . To participate or not? Giving voice to gender and socio-economic differences in colorectal cancer screening programmes. Eur J Cancer Care (Engl). 2011 Sep;20(5):669–78. https://doi.org/10.1111/j.1365-2354.2011.01263.x
28. Varghese NE , Sabat I , Neumann-Böhme S , Schreyögg J , Stargardt T , Torbica A , et al. Risk communication during COVID-19: A descriptive study on familiarity with, adherence to and trust in the WHO preventive measures. PLoS One. 2021 Apr;16(4):e0250872. https://doi.org/10.1371/journal.pone.0250872
29. Bish A , Michie S . Demographic and attitudinal determinants of protective behaviours during a pandemic: a review. Br J Health Psychol. 2010 Nov;15(Pt 4):797–824. https://doi.org/10.1348/135910710X485826
30. Harper CA , Satchell LP , Fido D , Latzman RD . Functional Fear Predicts Public Health Compliance in the COVID-19 Pandemic. Int J Ment Health Ad. 2020.
31. Leung GM , Lam TH , Ho LM , Ho SY , Chan BH , Wong IO , et al. The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. J Epidemiol Community Health. 2003 Nov;57(11):857–63. https://doi.org/10.1136/jech.57.11.857
32. Barari S , Caria S , Davola A , Falco P , Fetzer T , Fiorin S , et al. Evaluating COVID-19 Public Health Messaging in Italy: Self-Reported Compliance and Growing Mental Health Concerns. medRxiv. 2020:2020.03.27.20042820. https://doi.org/10.1101/2020.03.27.20042820
33. Brouard S , Vasilopoulos P , Becher M . Sociodemographic and Psychological Correlates of Compliance with the COVID-19 Public Health Measures in France. Can J Polit Sci. 2020;53(2):253–8. https://doi.org/10.1017/S0008423920000335
34. Rosenstock IM . Health Belief Model and Preventive Health Behavior. Health Educ Q. 1974;2(4):354–86.
35. Wollschläger D , Gianicolo E , Blettner M , Hamann R , Herm-Stapelberg N , Schoeps M . Association of COVID-19 mortality with COVID-19 vaccination rates in Rhineland-Palatinate (Germany) from calendar week 1 to 20 in the year 2021: a registry-based analysis. Eur J Epidemiol. 2021 Dec;36(12):1231–6. https://doi.org/10.1007/s10654-021-00825-6
36. Pullen C , Steele J , Patrick J . Ageism Predicts Prioritizing COVID-19 Vaccines for Older Adults and LTC Residents. Innov Aging. 2021;5 Supplement_1:602. https://doi.org/10.1093/geroni/igab046.2296
37. Harris CR , Jenkins M , Glaser D . Gender differences in risk assessment: why do women take fewer risks than men? Judgm Decis Mak. 2006;1(1):48–63.
38. Mehta PH , Welker KM , Zilioli S , Carré JM . Testosterone and cortisol jointly modulate risk-taking. Psychoneuroendocrinology. 2015 Jun;56:88–99. https://doi.org/10.1016/j.psyneuen.2015.02.023
39. de la Vega R , Ruíz-Barquín R , Boros S , Szabo A . Could attitudes toward COVID-19 in Spain render men more vulnerable than women? Glob Public Health. 2020 Sep;15(9):1278–91. https://doi.org/10.1080/17441692.2020.1791212
40. Adams LM , Gell NM , Hoffman EV , Gibbons LE , Phelan EA , Sturgeon JA , et al. Impact of COVID-19 ‘Stay Home, Stay Healthy’ Orders on Function among Older Adults Participating in a Community-Based, Behavioral Intervention Study. J Aging Health. 2021 Aug-Sep;33(7-8):458–68. https://doi.org/10.1177/0898264321991314
41. Sepúlveda-Loyola W , Rodríguez-Sánchez I , Pérez-Rodríguez P , Ganz F , Torralba R , Oliveira DV , et al. Impact of Social Isolation Due to COVID-19 on Health in Older People: Mental and Physical Effects and Recommendations. J Nutr Health Aging. 2020;24(9):938–47. https://doi.org/10.1007/s12603-020-1500-7
42. Varma P , Junge M , Meaklim H , Jackson ML . Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: A global cross-sectional survey. Prog Neuropsychopharmacol Biol Psychiatry. 2021 Jul;109:110236. https://doi.org/10.1016/j.pnpbp.2020.110236
43. Lades LK , Laffan K , Daly M , Delaney L . Daily emotional well-being during the COVID-19 pandemic. Br J Health Psychol. 2020 Nov;25(4):902–11. https://doi.org/10.1111/bjhp.12450
44. Schwinger M , Trautner M , Kärchner H , Otterpohl N . Psychological Impact of Corona Lockdown in Germany: Changes in Need Satisfaction, Well-Being, Anxiety, and Depression. Int J Environ Res Public Health. 2020 Dec;17(23):E9083. https://doi.org/10.3390/ijerph17239083
45. Wilson JM , Lee J , Shook NJ . COVID-19 worries and mental health: the moderating effect of age. Aging Ment Health. 2021 Jul;25(7):1289–96. https://doi.org/10.1080/13607863.2020.1856778
46. Maggiori C , Dif-Pradalier, M. Les 65 ans et plus au coeur de la crise COVID-19 (Rapport général). Fribourg: HES-SO – Haute école de travail social – Fribourg; 2020.
47. Escasain L , Gilles, I , Perriraz, M . Compréhension du public de la COVID-19 (COP – COVID) : influence du genre et de l’âge sur la compréhension de la pandémie après la 1ère vague. Raisons de santé, Les Essentiels N°28. Lausanne: Unisanté, Université de Lausanne.
48. Heid AR , Cartwright F , Wilson-Genderson M , Pruchno R . Challenges Experienced by Older People During the Initial Months of the COVID-19 Pandemic. Gerontologist. 2021 Jan;61(1):48–58. https://doi.org/10.1093/geront/gnaa138
49. Parsons Leigh J , Fiest K , Brundin-Mather R , Plotnikoff K , Soo A , Sypes EE , et al. A national cross-sectional survey of public perceptions of the COVID-19 pandemic: self-reported beliefs, knowledge, and behaviors. PLoS One. 2020 Oct;15(10):e0241259. https://doi.org/10.1371/journal.pone.0241259
50. Monsch GA , Ehrler F , Steinmetz S . FORS Covid-19 – Enquêtes, fiche d’information n° 2 Politique, droits fondamentaux et enjeux environnementaux pendant la période de confinement.; 2020.