Suicides and ambient temperature in Switzerland: A nationwide time-series analysis
DOI: https://doi.org/10.4414/SMW.2022.w30115
Séverine
Bära, Marvin
Bundoabc, Evan
de Schrijverabc, Thomas J.
Müllerde, Ana Maria
Vicedo-Cabreraab
aInstitute of Social and Preventive Medicine, University of Bern, Bern, Switzerland
bOeschger Centre for Climate Change Research, University of Bern, Bern, Switzerland
cGraduate School for Health Sciences, University of Bern, Bern, Switzerland
dTranslational Research Centre, University Hospital of Psychiatry and Psychotherapy University of Bern, Bern, Switzerland
ePrivate Clinic Meiringen, Meiringen, Switzerland
Summary
AIM OF THE STUDY: Previous literature suggests that ambient temperature may play a role in increasing the risk of suicide. Although in Switzerland suicides are an important cause of death, limited research exists on risk factors for suicidal behaviour, including ambient temperature. We aimed to assess the short-term association between ambient temperature and suicide risk in Switzerland between 1995 and 2016, and the differences by region, individual characteristics and method of suicide.
METHODS: We collected daily data on suicides and mean temperatures in each canton of Switzerland. We used a two-stage approach, consisting of a case time series analysis using conditional quasi-Poisson and distributed lag non-linear models followed by a multivariate meta-regression analysis. We conducted subgroup analyses by sex, age (<35, 35–65 and >65 years) and method of suicide (violent or nonviolent).
RESULTS: Between 1995 and 2016, there were a total of 24,067 suicides in Switzerland. Overall, we found a positive and non-linear temperature–suicide association in all regions. On average, the risk of suicide increased by 34% (1.34 relative risk [95% confidence interval: 1.19–1.52]) from the 10th to the 99th temperature percentile in Switzerland (lag period of 0–2 days). Indications of larger risks were mostly found in females, younger individuals (<35 years) and with nonviolent methods. Regional risks ranged from 24% (East region) to 55% (North-West region).
CONCLUSIONS: Our findings suggest that increasing temperatures could be considered a risk factor for suicidal behaviour in Switzerland. Knowledge of the profile of people committing suicide could help us to understand the mechanisms behind this association and thus support policymakers in suicide prevention.
Introduction
Suicide worldwide
Suicide is a global phenomenon resulting in a major public health burden. With an estimated 700,000 suicide deaths occurring worldwide every year, suicides account for half of all violent deaths in men and more than two-thirds in women [1]. Suicide amounted to 1.4% of all deaths worldwide, making it the 18th most common cause of death overall in 2016 and the fourth most common in 15–19 year olds in 2019 [1, 2]. There are indications that for each adult who dies by suicide there may be more than 20 others attempting suicide [1]. Notably, there are regional differences in suicide rates worldwide, particularly with respect to sex [2].
Suicides in Switzerland
In Switzerland, almost 10 suicides per 100,000 inhabitants were registered in 2019 (14.2 for men and 5.6 for women) [2]. According to the Federal Statistical Office (BfS), in females this corresponds to approximately the same death rate as for colorectal cancer and leads to almost as many potential life years lost as breast cancer [3]. In comparison, the age-standardized suicide rate per 100,000 inhabitants in Europe was 10.5 overall (e.g., 10.4 in Austria, 9.6 in France, 8.3 in Germany, 4.3 in Italy) in 2019 [2]. However, since the year 2002, the suicide rate in Switzerland has declined slightly. The restriction of firearm availability due to a reform of the Swiss army in 2003 has been found to be a reason for this decline [4]. In contrast, the rate of assisted suicides (in Switzerland performed by “right to die” organizations like EXIT and Dignitas, who assist persons wishing to end their life in taking a lethal substance) has risen constantly since the registry started in 1998 [5]. Nevertheless, the 2017 Swiss Health Survey estimated that there were 33,000 suicide attempts in one year [6].
Pathogenesis of suicide
Suicide is a complex event. Several neurobiological factors influencing suicidal behaviour have been proposed, including alterations of the serotonergic mechanism, receptor-linked signalling mechanisms, dysregulation in the hypothalamic-pituitary-adrenal axis and abnormalities of neurotrophins and neurotrophin receptors [7]. Most suicide victims have been diagnosed with a mental disorder prior to their death [8]. These primarily involve major depressive episodes or schizophrenia, as well as eating disorders and personality disorders [9,10]. Multiple other interacting factors, such as alcohol and drug-related disorders as well as histories of more than one mental disorder, may play a role in suicidal behaviour [10].
In addition to health conditions, individual characteristics and social factors have been associated with a higher risk of suicide [9–18]. In particular, social and socioeconomic factors like unemployment, financial or legal difficulties, being a single parent, living alone, living in an urban area, lower educational level and migration background have been reported as risk factors for suicidal behaviour in the Swiss population [6].
Based on studies on the seasonality of suicide, several environmental factors have been proposed as potential triggers of suicide. These include several climatic factors or phenomena such as droughts, changes in atmospheric pressure, air pollution, melting ice, sunshine and ambient temperature [9, 14, 18–21]. In Europe, it has recently been suggested that the effect of weather (e.g. rainfall, temperature) on national suicide rates seems stronger than the effect of economic conditions such as, e.g., national unemployment rate, national growth rate, gross domestic product per capita or inflation [14].
Ambient temperature, mental health and suicides
Recent evidence suggests that ambient temperature may play an important role in the pathogenesis of suicide [9, 11, 16, 19, 22–26]. Potential mechanisms, such as over-activation of brown adipose tissue or alteration of the serotoninergic system, have been proposed [27, 28]. Additionally, high ambient temperatures might lead to worse mental health in psychiatric patients [29–37], which could eventually lead to suicidal behaviour, as mentioned above. For example, heat has been associated with mood disorders, bipolar disorder, anxiety, alcohol/drug abuse, dementia, schizophrenia, aggressive thoughts and increased self-reported mental distress [20, 35, 38–42]. A recent study in the city of Bern (Switzerland) found that the risk of hospitalization for mental health reasons increases by 4% for each 10 °C increase in ambient temperature [37]. In particular, larger risks of hospitalization of 10–30% were found in patients with schizophrenia and developmental disorders, which have been associated with suicidal behaviour [8, 37]. Additionally, association estimates seem to vary across regions and populations, suggesting differential vulnerability patterns [24]. For example, in some Asian countries, older adults and people living in rural areas were more affected [19, 25], and in Croatia and Brazil men seem to be more susceptible, while females were more affected in Japan [9, 22, 25]. So far, there has been limited research assessing whether heat influences suicidal behaviour in the Swiss population. In a multi-country study, Kim et al. found a positive association between high ambient temperature and suicides in eight cantons in Switzerland [24]. However, this association has not yet been assessed across the whole Swiss population, nor has whether individual characteristics influence vulnerability to the temperature–suicide association. Also, to our knowledge there is no study evaluating whether temperature affects the method of suicide.
We aimed to assess further the impact of temperature on suicidal behaviour in Switzerland by using a nationwide dataset on suicides between 1995 and 2016 to identify regional patterns as well as predisposing individual characteristics.
Materials and Methods
Data collection & preparation
Suicides
Data on suicides in Switzerland between 1995 and 2016 were collected from anonymized individual mortality data provided by the Federal Statistical Office of Switzerland (BfS). Based on the reported cause of death, suicide was defined as intentional self-harm (International Statistical Classification of Diseases and Related Health Problems, 10th revision [ICD-10]), corresponding to codes X60 to X84 [43]. We excluded assisted suicides, usually coded as X61.8 (if the name of the right-to-die society was mentioned) or X61.9 (if barbiturates were mentioned). Of note, since 2009 assisted suicide has been consistently coded as a circumstance concomitant with death. That is, the disease leading to the assisted suicide was classified as the primary cause of death and the assisted suicide only as a concomitant of death [44].
We collected information on date of death, canton of residence, sex and age. We distinguished two subgroups of suicide: nonviolent suicides, defined as self-poisoning [ICD-10: X60–X69] (e.g. overdose of drugs), and violent suicides, defined as self-harm [ICD-10 code X70–X84] (e.g. hanging, drowning, shot gun, jumping from a high place). Details of the ICD-10 codes are described in table S1 (appendix).
Data on suicides were aggregated into daily counts by canton of residence for all suicides and for the subgroups of sex (male, female), age (<35, 35–65, >65 years) and method of suicide (violent, nonviolent).
Weather data
We used population-weighted daily mean temperature data from each canton between 1995 and 2016. We used daily mean temperature instead of other temperature metrics (e.g. maximum temperature) because we were interested in exploring the association across the whole temperature spectrum, including heat and cold. It should also be noted that previous studies have shown that mean temperature can be considered a suitable indicator with which to capture temperature–mortality associations [45]. Population-weighted daily mean temperature data were obtained and validated for assessing temperature–mortality risks in a previous study [46]. In brief, spatially-resolved temperature data with 1.6 × 2.3 km resolution were originally obtained from the Federal Office of Meteorology and Climatology, MeteoSwiss, and combined with population data from EOSDIS (Earth Observing System Data and Information System, UN WPP-adjusted population count, v4.11, 2010) with a 1x1 km resolution to derive population-weighted daily mean temperatures for each canton [47]. In brief, we calculated the weights as a ratio between the population residing in the corresponding grid cell and the total population residing in the canton. This population-weighted temperature metric has been shown to be a better approximation of the average exposure of the population living in a large area with a highly heterogeneous climate and orography, as is particularly the case for large cantons in Switzerland [46].
The sunshine duration data (hours of sunshine per day and percentage of maximum duration of sunshine possible on that day at that location) were collected from the IDAweb database [48], which is provided by the Federal Office of Meteorology and Climatology, MeteoSwiss (details are described in the supplementary information).
Statistical modelling
We assessed the association between ambient temperature and suicide using the so-called two-stage approach commonly used in multi-location time series studies. In brief, we first performed a case time series analysis, a newly developed study design by Gasparrini [49], and combined this with distributed lag non-linear models to derive the region-specific association estimates. Second, we pooled the temperature-suicide associations in each region in a multivariate meta-regression model to derive the country-wide exposure-response functions for all suicides and for the subgroups of sex, age and method.
First, for each major region (figure S1), we performed a case time series analysis with conditional quasi-Poisson regression and distributed lag non-linear models (DLNMs) [50, 51]. The case time series design was developed recently as an alternative to the usual case-crossover design [49]. It allows multiple canton-specific time series of suicide and temperature to be modelled within each region through a conditional Poisson regression. That is, it allows analysis of the exposure and the outcome aggregated at a smaller geographical unit (i.e. the canton), thus reducing the exposure misclassification, while reporting more precise risks at an upper geographical level (i.e. the region). The method uses the usual data structure of time series analysis, in which a common exposure level is defined for all subjects within the study area, in this case the canton. The aggregated case-crossover approach applies the concept of a bidirectional, time-stratified design to control for long-term and seasonal trends by matching case and control days within the year, month and day of the week [37]. Thus, any factors altering the temporal patterns which vary over longer time scales beyond this timeframe (i.e. long-term trends, seasonality) are accounted for by design. Unlike the usual case-crossover design, the matching pairs are defined within each canton in each region-specific model.
We modelled the association between temperature and suicide through DLNMs. This methodological framework allows assessment of the complex non-linear and lagged dependencies typically found in temperature studies. It consists of the combination of two functions that define the conventional exposure–response association and the additional lag–response association, respectively [51]. The exposure–response dimension represents how the risk changes at each temperature with respect to a reference value, usually expressed as a relative risk (RR). The lag–response association represents the temporal distribution of the risk after the exposure, accounting for immediate and delayed effects that cumulate across the lag period [51]. Specifically, we used a quadratic B-spline with one internal knot placed at the 75th percentile of the canton-specific mean temperature distribution to model the exposure-response dimension. Additionally, we modelled the lag–response association with up to two days of lag with an integer function (i.e., unconstraint DLNM). We tested several nonlinear functions (natural-spline, quadratic B-spline) with internal knots placed at different percentiles (25th, 50th, 75th, 90th, 95th) for the exposure-response dimension. We selected the model specifications using quasi-Akaike Information Criteria (Q-AIC). For each model combination, we computed the sum of the Q-AIC in each region and selected the combination with the lowest value [24]. The number of lags was restricted to two based on a previous study [24].
Second, we pooled the region-specific temperature-suicide associations in a multivariate random effects meta-analysis [52]. In the meta-analysis model we included the region-specific average temperature and temperature range as covariates to partially capture the heterogeneity of the association between regions. We derived from the model the pooled country-wide exposure–response curve and the corresponding region-specific best linear unbiased predictions (BLUPS). BLUPs are improved estimates of the temperature-suicide association which borrow information across units within the same hierarchical level (i.e. regions) and based on similarities with respect to the covariates included in the model (i.e. average temperature and temperature range). These can offer more accurate estimates and more stable curves, especially in locations with small daily mortality counts.
Results were expressed as RRs and 95% confidence intervals (CI) for each temperature value in each region. The 10th percentile was used here as a reference, following the procedure of a recent study [24]. Finally, we conducted a subgroup analysis by sex, age group (<35, 35–65 and >65 years) and method of suicide (violent or nonviolent).
We tested whether sunshine was a potential confounder of the temperature-suicide association. Specifically, we included the variables hours of daily sunshine and percentage of the maximum possible sunshine duration (as a linear function of the value on the same day of the death) in separate temperature models and checked whether the association between temperature and suicide risk changed or remained similar.
The statistical analysis was performed using R statistical software (version 1.3.1093 © 2009–2020 RStudio, PBC) and the gnm, dlnm and mixmeta R packages.
Results
Description of the data
Between 1995 and 2016, a total of 24,067 suicides were registered in Switzerland. These do not include the 3,233 cases (11.8%) identified as assisted suicides during the study period. Overall, 74.3% (17,873) were male and 53.5% (12,870) were aged between 35 and 65 years, 20.8% (5,009) were younger than 35 years and 25.7% (6,188) were older than 65 years. Violent suicide accounted for a large proportion (90.2%) of all suicides, compared to 9.8% who died by a nonviolent method (table 1). The highest proportion of suicides was registered in the region of Midland (25.3%), while the lowest was in Ticino (2.9%). Nevertheless, we generally found homogenous patterns among the regions regarding the subgroups of sex, age and method (table 1). The annual number of suicides declined slightly over the study period, from 1,306 deaths in 1995 to 998 deaths in 2016 (figure S2 and table S4 in appendix). Regarding the subgroup analysis, between 1995 and 2016 there was a decrease among the age group <35 years and an increase among the age group >65 years (table S4 in appendix). The patterns generally did not change over time in the subgroups of sex and method.
Table 1Summary statistics of suicides and mean daily temperature in the seven major regions of Switzerland.
|
Region
|
All
|
Sex
|
Age group
|
Method
|
Mean temperature
|
|
Male
|
Female
|
<35
|
35–65
|
>65
|
Nonviolent
|
Violent
|
| Lake Geneva |
4,323 (18.0) |
3,074 (71.1) |
1,249 (28.9) |
895 (20.7) |
2,378 (55.0) |
1,050 (24.3) |
512 (11.8) |
3,811 (88.2) |
8.9 (3.1, 14.8) |
| Midland |
6,098 (25.3) |
4,606 (75.5) |
1,492 (24.5) |
1,183 (19.4) |
3,232 (53.0) |
1,683 (27.6) |
489 (8.0) |
5,609 (92.0) |
9.1 (3.0, 14.7) |
| North-West |
3,225 (13.4) |
2,465 (76.4) |
760 (23.6) |
653 (20.2) |
1,705 (52.9) |
867 (26.9) |
335 (10.4) |
2,890 (89.6) |
10.7 (4.6, 16.2) |
| Zurich |
4,073 (16.9) |
2,992 (73.5) |
1,081 (26.5) |
859 (21.1) |
2,110 (51.8) |
1,104 (27.1) |
440 (10.8) |
3,633 (89.2) |
9.9 (3.6, 15.6) |
| East |
3,620 (15.0) |
2,726 (75.3) |
894 (24.7) |
819 (22.6) |
1,933 (53.4) |
868 (24.0) |
335 (9.3) |
3,285 (90.7) |
7.8 (1.8, 13.5) |
| Central |
2,034 (8.5) |
1,498 (73.6) |
536 (26.4) |
466 (22.9) |
1,134 (55.8) |
434 (21.3) |
176 (8.7) |
1,858 (91.3) |
7.7 (1.9, 13.4) |
| Ticino |
694 (2.9) |
512 (73.8) |
182 (26.2) |
134 (19.3) |
378 (54.5) |
182 (26.2) |
66 (9.5) |
628 (90.5) |
10.5 (4.2, 16.4) |
| TOTAL |
24,067 |
17,873 (74.3) |
6,194 (25.7) |
5,009 (20.8) |
12,870 (53.5) |
6,188 (25.7) |
2,353 (9.8) |
21,714 (90.2) |
8.6 (2.7, 14.4) |
We observed modest differences in average temperature between the seven major regions (table 1). The warmest region was North-West Switzerland (median 10.7 °C), while the coldest mean temperatures were measured in Central Switzerland (median 7.7 °C). Ticino was the sunniest region (median 6.5 hours of sunshine per day and 66% of the maximum possible sunshine duration), while in Central Switzerland the median hours of sunshine per day was 2.8, with a median of 26% of the maximum possible sunshine duration (table S2 in appendix).
Association between temperature and suicide
The pooled and region-specific exposure–response curves representing the associations for all suicides and for the subgroups of sex, age group and method of suicide are shown in figure 1, while the corresponding RRs at the 99th percentile are reported in table 2. The association between mean temperature and suicides remained similar when sunshine duration was included in the model (table S3 in appendix). Therefore, we assumed that sunshine duration was not a confounder in our analysis.
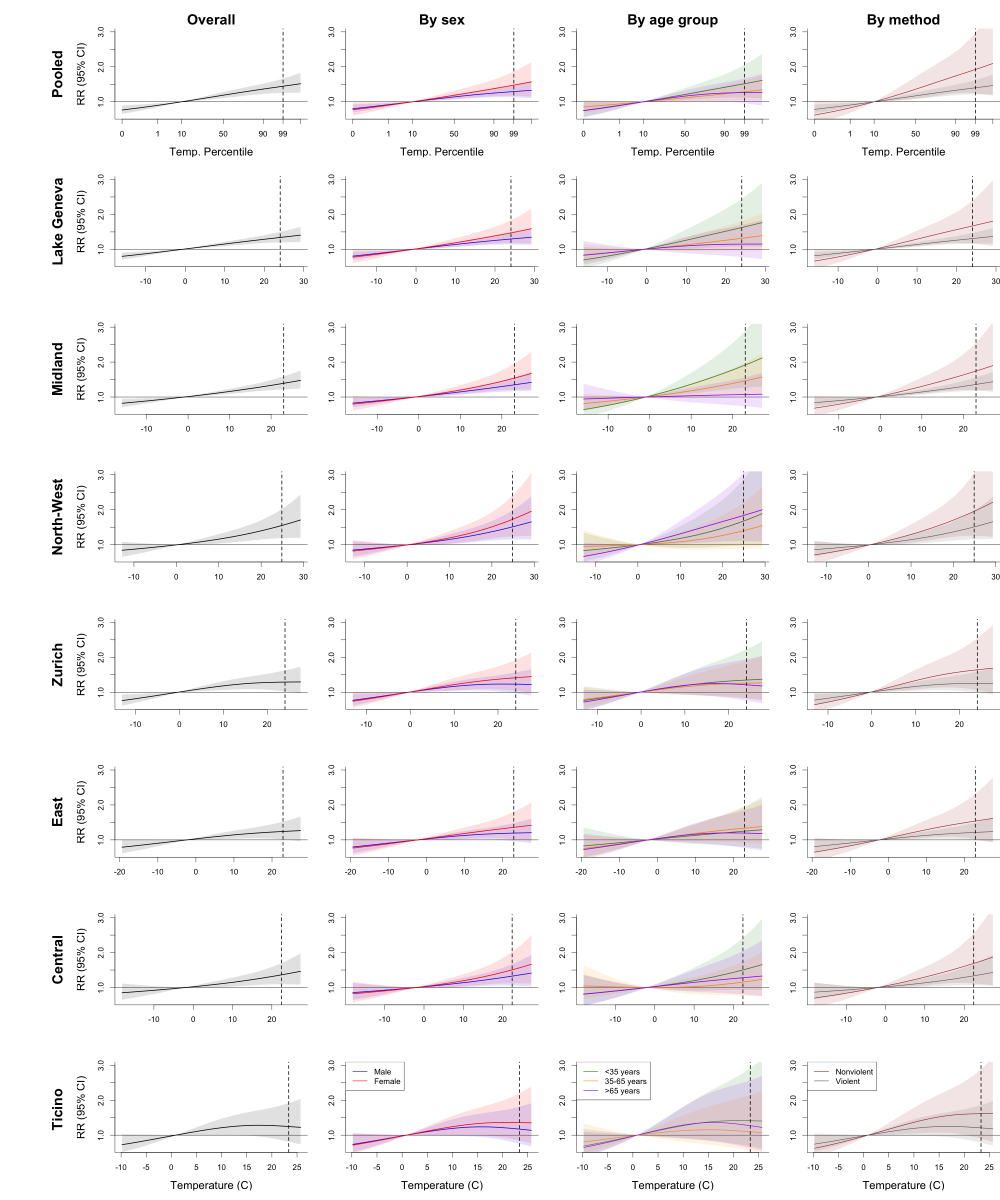
Figure 1 Exposure-response curves of the temperature-suicide association overall and across the seven major regions of Switzerland.
Relative risk (RR) of suicide with the 95% CI (transparent colour) against daily mean temperature (°C) with the corresponding 99th percentile of the temperature distribution (dashed line). Overall exposure-response curves for each region and for pooled data, and stratified analyses by sex, age group and method of suicide.
Table 2Temperature-suicide association.
|
All
|
Sex
|
Age
|
Method
|
|
Male
|
Female
|
<35 years
|
35–65 years
|
<65 years
|
Nonviolent
|
Violent
|
| Pooled |
1.34 (1.19–1.52) |
1.29 (1.12–1.49) |
1.48 (1.17–1.87) |
1.52 (1.12–2.06) |
1.29 (1.03–1.61) |
1.26 (0.96–1.67) |
1.68 (1.15–2.46) |
1.31 (1.15–1.49) |
| Lake Geneva |
1.34 (1.20–1.50) |
1.30 (1.14–1.48) |
1.47 (1.18–1.84) |
1.63 (1.08–2.45) |
1.32 (0.96–1.81) |
1.15 (0.78–1.70) |
1.67 (1.16–2.40) |
1.31 (1.17–1.47) |
| Midland |
1.39 (1.22–1.59) |
1.35 (1.16–1.57) |
1.54 (1.21–1.96) |
1.92 (1.27–2.89) |
1.46 (1.08–1.99) |
1.07 (0.73–1.56) |
1.74 (1.19–2.56) |
1.36 (1.19–1.56) |
| North-West |
1.55 (1.19–2.02) |
1.51 (1.15–1.98) |
1.73 (1.23–2.41) |
1.67 (0.98–2.86) |
1.40 (0.89–2.20) |
1.83 (1.11–3.04) |
1.95 (1.25–3.05) |
1.51 (1.15–1.97) |
| Zurich |
1.29 (1.03–1.63) |
1.23 (0.97–1.57) |
1.42 (1.04–1.93) |
1.35 (0.82–2.23) |
1.26 (0.84–1.90) |
1.21 (0.76–1.95) |
1.64 (1.06–2.55) |
1.26 (0.99–1.59) |
| East |
1.24 (1.01–1.52) |
1.19 (0.96–1.48) |
1.36 (1.02–1.80) |
1.25 (0.80–1.96) |
1.34 (0.92–1.94) |
1.19 (0.77–1.85) |
1.54 (1.02–2.32) |
1.21 (0.99–1.49) |
| Central |
1.36 (1.09–1.70) |
1.33 (1.05–1.67) |
1.51 (1.12–2.02) |
1.50 (0.93–2.42) |
1.16 (0.77–1.74) |
1.28 (0.80–2.04) |
1.69 (1.12–2.56) |
1.33 (1.07–1.67) |
| Ticino |
1.25 (0.81–1.92) |
1.17 (0.76–1.82) |
1.36 (0.84–2.20) |
1.41 (0.68–2.92) |
1.10 (0.56–2.15) |
1.27 (0.63–2.57) |
1.61 (0.90–2.89) |
1.21 (0.78–1.86) |
Overall, we observed a positive and nearly linear association between ambient temperature and suicide risk in all regions (figure 1), although the shape of the association varied slightly across regions and subgroups. On average, the risk of committing suicide increased by 34% (1.34 [95% CI: 1.19–1.52]) from the 10th to the 99th temperature percentile in Switzerland. Regarding the subgroup analysis, although the confidence intervals largely overlapped, we found larger risk increases in females (1.48 [1.17–1.87]) compared to males (1.29 [1.12–1.49]) and in the population aged <35 years (1.52 [1.12–2.06]) relative to the 35-65 years (1.29 [1.03–1.61]) and the older than 65 years (1.26 [0.96–1.67]) age groups. An indication of larger risk increases for nonviolent methods (1.68 [1.15–2.46]) compared to violent methods (1.31 [1.15–1.49]) was found.
The suicide-temperature association seemed to diverge slightly between regions. In the Lake Geneva, Midland and Central regions we found a nearly linear association with similar increases in risk at the 99th percentile, ranging between 34–39%. In the Zurich, East and Ticino regions the association reaches a maximum increased risk of 20–25% around a temperature of 15 ºC, followed by a plateau or even a decrease in risk with extreme temperatures. In the North-West region we found a steeper, nonlinear increase in risk, reaching a relative risk of 1.55 [1.19–2.02] at the 99th percentile. The results by subgroup followed similar patterns across regions and the confidence intervals largely overlapped.
Discussion
The aim of this study was to assess the association between ambient temperature and suicide in Switzerland between 1995 and 2016. We found that risk of suicide increased almost linearly with increasing temperatures in all seven regions in Switzerland. We also found indications of a stronger association in females, those younger than 35 years and for suicides by nonviolent methods.
Our findings align with evidence from previous studies showing a slightly non-linear temperature–suicide relationship characterized by an increased risk with increasing temperatures over cold-to-moderately-warm temperature ranges, followed by a plateau or decrease in risk at very high temperatures [24, 25]. This pattern was more visible in the Zurich, East and Ticino regions. Our results are also consistent with previous findings from studies performed in the Swiss population. For example, Kim et al. found a similar shape to the association, as well as a similar range of results with moderate regional variability [24].
Association estimates varied across the seven major regions of Switzerland, which could be due to the heterogenous population in Switzerland. In fact, the major regions are characterized by different urbanicity, economic, social, cultural, linguistic and religious profiles, which could result in variable levels of vulnerability. For example, people living in urban areas in Switzerland have been shown to have suicidal thoughts more often [6], while there is some evidence that the temperature–suicide association is larger in rural prefectures [25]. Furthermore, in Switzerland suicide prevention plans are implemented by cantonal authorities, following the federal guidelines. Thus, differences in the cantonal interventions might also partly explain regional patterns.
Our findings suggest differential vulnerability patterns. However, we could not derive consistent conclusions from these patterns due to the large uncertainty of the estimates. First, our results indicate larger risk increases with temperature for females, as found in some previous investigations [9, 24, 25]. In contrast, other studies have found stronger associations in men because they tend to do more outdoor work and are exposed to high ambient temperatures more frequently [28]. We also observed larger risk increases in people aged younger than 35 years. A potential reason for this could be that the onset of schizophrenia, a common disorder associated with suicide which has also been seen to be associated to heat stress [37], occurs in early adulthood [40]. However, interestingly we found larger risk increases for suicide by nonviolent methods (e.g. poisoning), which are usually associated with substance-related disorders, while high-severity psychiatric disorders tend to correlate with more violent suicides (often seen in schizophrenia, bipolar disorder and major depression) [53, 54]. Furthermore, it is known that deficiencies in serotonergic innervation, which may be associated with heat exposure, lead to increased aggression [7, 55, 56]. Aggression is generally other-directed or self-directed, and in the case of self-directed aggression it could consequently lead to violent suicide [56]. These contradicting patterns and mechanisms show the complex and still unclear interrelation between exposure to ambient temperature, mental disorders and suicide. Further studies are needed to clarify how ambient temperature affects mental health conditions, and in particular, to identify vulnerable subgroups towards which specific public health interventions should be targeted.
To the best of our knowledge, this is the first nationwide analysis in Switzerland of the short-term association between ambient temperature and suicide, focusing on individual factors and the method of suicide. The results of this study have important implications for public health. In particular, our findings are relevant given the current scenario of progressive warming due to climate change. Additionally, our results suggest that individual characteristics may modify a person’s vulnerability to higher ambient temperatures. However, we failed to identify clear conclusions about the most vulnerable groups and the potential mechanisms behind the variable vulnerability. Understanding the influence of socioeconomic (e.g., culture, religion, income, housing, education) and other environmental factors (e.g., pollen, air pollution) on suicides could enable policymakers shaping public health measures for suicide prevention to be better informed.
Finally, we acknowledge several limitations of this study. First, we reported estimates for the seven major regions of Switzerland, and not for cantons or smaller units, due to limited statistical power. Although these regions have been classified according to criteria of economic, demographic, linguistic and cultural connectivity, they could still include heterogeneous populations as well as climatic differences. The region-specific estimates are considered average associations for all populations in each region, and thus we cannot disregard potential variability in risks across the cantons within each region – as found in previous assessments of temperature-mortality associations [46]. Second, related to the previous point, we acknowledge that despite using regional estimates, our estimates in the subgroup analysis were still highly imprecise, which prevented us from deriving solid conclusions on the differential vulnerability across populations. Third, residual confounding by other known time-variant factors (e.g. humidity, air pressure, air pollution) or other unknown factors might be present. However, we argue that the confounding effect would be minimal, as shown in previous research [24]. Lastly, this study applies the assumption that ambient temperature exposures were the same for the whole canton, which in turn affects the precision of the estimates, the so-called Berkson error [57]. To partially overcome any potential exposure misclassification, however, daily mean temperatures were weighted based on the distribution of the population across cells within a canton [46].
In conclusion, our findings support the existing hypothesis that higher ambient temperature could be a trigger of suicide. The heterogeneous risks across subpopulations suggest differential vulnerability patterns and mechanisms. Further research should aim to understand the mechanisms behind the relationship between ambient temperature and suicide, in particular in relation to potential links to mental health conditions of those who commit suicide.
Data sharing statement
The anonymized suicide data (daily counts by canton and sub-category) in Switzerland between 1995 and 2016 is deposited in BORIS portal under the DOI https://doi.org/10.48620/38. The R code can be found in the GitHub repository of the last author https://github.com/anavica/SuicideTempCH_SMW22.git.
Acknowledgement
We would like to thank the Swiss Federal Statistical Office (BFS) for providing data on the daily mortality in Switzerland used in this study.
Dr. Ana Maria Vicedo-Cabrera
Institute of Social and Preventive Medicine (ISPM)
University of Bern
Mittelstrasse 43
CH-3012 Bern
anamaria.vicedo[at]ispm.unibe.ch
and
Dr. Thomas J. Müller
Translational Research Centre
University Hospital of Psychiatry and Psychotherapy
University of Bern
Hochschulstrasse 6
CH-3012 Bern
thomas.mueller[at]upd.unibe.ch
References
1. Suicide [Internet]. World Health Organisation (WHO). [cited 2021 Jul 21]. Available from: https://www.who.int/westernpacific/health-topics/suicide
2.
WHO
. Suicide worldwide in 2019: global health estimates. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.; 2021.
3. Verlorene potentielle Lebensjahre, Frauen - 1990-2018 [Internet]. Bundesamt für Statistik. 2020 [cited 2021 Jul 21]. Available from: https://www.bfs.admin.ch/bfs/de/home/statistiken/kataloge-datenbanken/tabellen.assetdetail.14966035.html
4.
Reisch T
,
Steffen T
,
Habenstein A
,
Tschacher W
. Change in suicide rates in Switzerland before and after firearm restriction resulting from the 2003 “Army XXI” reform. Am J Psychiatry. 2013 Sep;170(9):977–84. https://doi.org/10.1176/appi.ajp.2013.12091256
5. Suizid und Suizidhilfe [Internet]. Schweizer Gesundheitsobservatorium OBSAN. 2021 [cited 2021 Jul 2]. Available from: https://www.obsan.admin.ch/de/indikatoren/suizid-und-suizidhilfe
6.
Peter C
,
Tuch A
. Suizidgedanken und Suizidversuche in der Schweizer Bevölkerung (Obsan Bulletin 7/2019). [Internet]. Neuchâtel: Schweizerisches Gesundheitsobservatorium; 2019. Available from: https://www.obsan.admin.ch/de/publikationen/suizidgedanken-und-suizidversuche-der-schweizer-bevoelkerung
7.
Pandey GN
. Biological basis of suicide and suicidal behavior. Bipolar Disord. 2013 Aug;15(5):524–41. https://doi.org/10.1111/bdi.12089
8.
Arsenault-Lapierre G
,
Kim C
,
Turecki G
. Psychiatric diagnoses in 3275 suicides: a meta-analysis. BMC Psychiatry. 2004 Nov;4(1):37. https://doi.org/10.1186/1471-244X-4-37
9.
Dumenčić B
,
Rajc J
,
Marjanović K
,
Požgain I
,
Pavoković D
. Impact of meteorological factors on suicide attempts and completed suicides in Croatia, Osijek-Baranja county. Psychiatr Danub. 2019 Dec;31(4):405–12. https://doi.org/10.24869/psyd.2019.405
10.
Turecki G
,
Brent DA
. Suicide and suicidal behaviour. Lancet. 2016 Mar;387(10024):1227–39. https://doi.org/10.1016/S0140-6736(15)00234-2
11.
Akkaya-Kalayci T
,
Vyssoki B
,
Winkler D
,
Willeit M
,
Kapusta ND
,
Dorffner G
, et al.
The effect of seasonal changes and climatic factors on suicide attempts of young people. BMC Psychiatry. 2017 Nov;17(1):365. https://doi.org/10.1186/s12888-017-1532-7
12.
Astudillo-García CI
,
Rodríguez-Villamizar LA
,
Cortez-Lugo M
,
Cruz-De la Cruz JC
,
Fernández-Niño JA
. Air Pollution and Suicide in Mexico City: A Time Series Analysis, 2000-2016. Int J Environ Res Public Health. 2019 Aug;16(16):E2971. https://doi.org/10.3390/ijerph16162971
13.
Fernández-Niño JA
,
Astudillo-García CI
,
Rodríguez-Villamizar LA
,
Florez-Garcia VA
. Association between air pollution and suicide: a time series analysis in four Colombian cities. Environ Health. 2018 May;17(1):47. https://doi.org/10.1186/s12940-018-0390-1
14.
Fountoulakis KN
,
Chatzikosta I
,
Pastiadis K
,
Zanis P
,
Kawohl W
,
Kerkhof AJ
, et al.
Relationship of suicide rates with climate and economic variables in Europe during 2000-2012. Ann Gen Psychiatry. 2016 Aug;15(1):19. https://doi.org/10.1186/s12991-016-0106-2
15.
Lin GZ
,
Li L
,
Song YF
,
Zhou YX
,
Shen SQ
,
Ou CQ
. The impact of ambient air pollution on suicide mortality: a case-crossover study in Guangzhou, China. Environ Health. 2016 Aug;15(1):90. https://doi.org/10.1186/s12940-016-0177-1
16.
Pervilhac C
,
Schoilew K
,
Znoj H
,
Müller TJ
. Wetter und Suizid : assoziation zwischen meteorologischen Variablen und suizidalem Verhalten – eine qualitative systematische Übersichtsarbeit. Nervenarzt. 2020 Mar;91(3):227–32. https://doi.org/10.1007/s00115-019-00795-x
17.
Petridou E
,
Papadopoulos FC
,
Frangakis CE
,
Skalkidou A
,
Trichopoulos D
. A role of sunshine in the triggering of suicide. Epidemiology. 2002 Jan;13(1):106–9. https://doi.org/10.1097/00001648-200201000-00017
18.
Yu J
,
Yang D
,
Kim Y
,
Hashizume M
,
Gasparrini A
,
Armstrong B
, et al.
Seasonality of suicide: a multi-country multi-community observational study. Epidemiol Psychiatr Sci. 2020 Aug;29:e163. https://doi.org/10.1017/S2045796020000748
19.
Chau PH
,
Yip PS
,
Lau HY
,
Ip YT
,
Law FY
,
Ho RT
, et al.
Hot Weather and Suicide Deaths among Older Adults in Hong Kong, 1976-2014: A Retrospective Study. Int J Environ Res Public Health. 2020 May;17(10):E3449. https://doi.org/10.3390/ijerph17103449
20.
Cianconi P
,
Betrò S
,
Janiri L
. The Impact of Climate Change on Mental Health: A Systematic Descriptive Review. Front Psychiatry. 2020 Mar;11:74. https://doi.org/10.3389/fpsyt.2020.00074
21.
Fernández-Niño JA
,
Flórez-García VA
,
Astudillo-García CI
,
Rodríguez-Villamizar LA
. Weather and Suicide: A Decade Analysis in the Five Largest Capital Cities of Colombia. Int J Environ Res Public Health. 2018 Jun;15(7):E1313. https://doi.org/10.3390/ijerph15071313
22.
Bando DH
,
Teng CT
,
Volpe FM
,
Masi E
,
Pereira LA
,
Braga AL
. Suicide and meteorological factors in São Paulo, Brazil, 1996-2011: a time series analysis. Br J Psychiatry. 2017 Jul-Sep;39(3):220–7. https://doi.org/10.1590/1516-4446-2016-2057
23.
Kim Y
,
Kim H
,
Honda Y
,
Guo YL
,
Chen BY
,
Woo JM
, et al.
Suicide and Ambient Temperature in East Asian Countries: A Time-Stratified Case-Crossover Analysis. Environ Health Perspect. 2016 Jan;124(1):75–80. https://doi.org/10.1289/ehp.1409392
24.
Kim Y
,
Kim H
,
Gasparrini A
,
Armstrong B
,
Honda Y
,
Chung Y
, et al.
Suicide and Ambient Temperature: A Multi-Country Multi-City Study. Environ Health Perspect. 2019 Nov;127(11):117007. https://doi.org/10.1289/EHP4898
25.
Sim K
,
Kim Y
,
Hashizume M
,
Gasparrini A
,
Armstrong B
,
Sera F
, et al.
Nonlinear temperature-suicide association in Japan from 1972 to 2015: its heterogeneity and the role of climate, demographic, and socioeconomic factors. Environ Int. 2020 Sep;142:105829. https://doi.org/10.1016/j.envint.2020.105829
26.
Thompson R
,
Hornigold R
,
Page L
,
Waite T
. Associations between high ambient temperatures and heat waves with mental health outcomes: a systematic review. Public Health. 2018 Aug;161:171–91. https://doi.org/10.1016/j.puhe.2018.06.008
27.
Bach H
,
Arango V
. Neuroanatomy of Serotonergic Abnormalities in Suicide. In: Dwivedi Y, editor. The Neurobiological Basis of Suicide [Internet]. Boca Raton (FL): CRC Press/Taylor & Francis; 2012. Chapter 2. Available from: https://www.ncbi.nlm.nih.gov/books/NBK107204/
28.
Gao J
,
Cheng Q
,
Duan J
,
Xu Z
,
Bai L
,
Zhang Y
, et al.
Ambient temperature, sunlight duration, and suicide: A systematic review and meta-analysis. Sci Total Environ. 2019 Jan;646:1021–9. https://doi.org/10.1016/j.scitotenv.2018.07.098
29.
Yoo EH
,
Eum Y
,
Roberts JE
,
Gao Q
,
Chen K
. Association between extreme temperatures and emergency room visits related to mental disorders: A multi-region time-series study in New York, USA. Sci Total Environ. 2021 Oct;792:148246. https://doi.org/10.1016/j.scitotenv.2021.148246
30.
Chan EY
,
Lam HC
,
So SH
,
Goggins WB
,
Ho JY
,
Liu S
, et al.
Association between Ambient Temperatures and Mental Disorder Hospitalizations in a Subtropical City: A Time-Series Study of Hong Kong Special Administrative Region. Int J Environ Res Public Health. 2018 Apr;15(4):754. https://doi.org/10.3390/ijerph15040754
31.
García FM
,
Boada SS
,
Collsamata AX
,
Joaquim IG
,
Pérez YA
,
Tricio OG
, et al.
[Meteorological factors and psychiatric emergencies]. Actas Esp Psiquiatr. 2009 Jan-Feb;37(1):34–41.
32.
Hansen A
,
Bi P
,
Nitschke M
,
Ryan P
,
Pisaniello D
,
Tucker G
. The effect of heat waves on mental health in a temperate Australian city. Environ Health Perspect. 2008 Oct;116(10):1369–75. https://doi.org/10.1289/ehp.11339
33.
Lee S
,
Lee H
,
Myung W
,
Kim EJ
,
Kim H
. Mental disease-related emergency admissions attributable to hot temperatures. Sci Total Environ. 2018 Mar;616-617:688–94. https://doi.org/10.1016/j.scitotenv.2017.10.260
34.
Peng Z
,
Wang Q
,
Kan H
,
Chen R
,
Wang W
. Effects of ambient temperature on daily hospital admissions for mental disorders in Shanghai, China: A time-series analysis. Sci Total Environ. 2017 Jul;590-591:281–6. https://doi.org/10.1016/j.scitotenv.2017.02.237
35.
Schmeltz MT
,
Gamble JL
. Risk characterization of hospitalizations for mental illness and/or behavioral disorders with concurrent heat-related illness. Shaman J, editor. PLOS ONE. 2017;12(10).
36.
Trang PM
,
Rocklöv J
,
Giang KB
,
Kullgren G
,
Nilsson M
. Heatwaves and Hospital Admissions for Mental Disorders in Northern Vietnam. Schanzer DL, editor. PLOS ONE. 2016;11(5).
37.
Bundo M
,
de Schrijver E
,
Federspiel A
,
Toreti A
,
Xoplaki E
,
Luterbacher J
, et al.
Ambient temperature and mental health hospitalizations in Bern, Switzerland: A 45-year time-series study. Xu M, editor. PLOS ONE. 2021;16(10).
38.
Li M
,
Ferreira S
,
Smith TA
. Temperature and self-reported mental health in the United States. PLoS One. 2020 Mar;15(3):e0230316. https://doi.org/10.1371/journal.pone.0230316
39.
Shapira A
,
Shiloh R
,
Potchter O
,
Hermesh H
,
Popper M
,
Weizman A
. Admission rates of bipolar depressed patients increase during spring/summer and correlate with maximal environmental temperature. Bipolar Disord. 2004 Feb;6(1):90–3. https://doi.org/10.1046/j.1399-5618.2003.00081.x
40.
Sung TI
,
Chen MJ
,
Lin CY
,
Lung SC
,
Su HJ
. Relationship between mean daily ambient temperature range and hospital admissions for schizophrenia: results from a national cohort of psychiatric inpatients. Sci Total Environ. 2011 Dec;410-411:41–6. https://doi.org/10.1016/j.scitotenv.2011.09.028
41.
Sung TI
,
Chen MJ
,
Su HJ
. A positive relationship between ambient temperature and bipolar disorder identified using a national cohort of psychiatric inpatients. Soc Psychiatry Psychiatr Epidemiol. 2013 Feb;48(2):295–302. https://doi.org/10.1007/s00127-012-0542-5
42.
Zhang S
,
Yang Y
,
Xie X
,
Li H
,
Han R
,
Hou J
, et al.
The effect of temperature on cause-specific mental disorders in three subtropical cities: A case-crossover study in China. Environ Int. 2020 Oct;143:105938. https://doi.org/10.1016/j.envint.2020.105938
43.
International Statistical Classification of Diseases and Related Health Problems
. 10th Revision. Geneva, Switzerland: WHO. [Internet]. [cited 2021 Jul 21]. Available from: https://icd.who.int/browse10/2016/en
44.
Junker C
. Assisted suicide and suicide in Switzerland [Internet]. Federal Statistical Office (FSO); 2016. Available from: https://www.bfs.admin.ch/bfs/de/home/statistiken/kataloge-datenbanken/publikationen.assetdetail.3902308.html
45.
Ragettli MS
,
Vicedo-Cabrera AM
,
Schindler C
,
Röösli M
. Exploring the association between heat and mortality in Switzerland between 1995 and 2013. Environ Res. 2017 Oct;158:703–9. https://doi.org/10.1016/j.envres.2017.07.021
46.
de Schrijver E
,
Folly CL
,
Schneider R
,
Royé D
,
Franco OH
,
Gasparrini A
, et al.
A Comparative Analysis of the Temperature-Mortality Risks Using Different Weather Datasets Across Heterogeneous Regions. Geohealth. 2021 May;5(5):GH000363. https://doi.org/10.1029/2020GH000363
47. Spatial Climate Analyses - MeteoSwiss [Internet]. Federal Office of Meteorology and Climatology MeteoSwiss. [cited 2021 Jun 18]. Available from: https://www.meteoswiss.admin.ch/home/climate/swiss-climate-in-detail/raeumliche-klimaanalysen.html
48. MeteoSwiss IDAWEB [Internet]. Federal Office of Meteorology and Climatology MeteoSwiss. [cited 2021 Mar 11]. Available from: https://gate.meteoswiss.ch/idaweb/login.do;idaweb=whXQTQtPkTSbh3dGcrWzyDnBHQ7sJJnQhz01vbZhWhdKTdHkq1h0!-1907983237
49.
Gasparrini A
. The Case Time Series Design. Epidemiology. 2021 Nov;32(6):829–37. https://doi.org/10.1097/EDE.0000000000001410
50.
Armstrong BG
,
Gasparrini A
,
Tobias A
. Conditional Poisson models: a flexible alternative to conditional logistic case cross-over analysis. BMC Med Res Methodol. 2014 Nov;14(1):122. https://doi.org/10.1186/1471-2288-14-122
51.
Gasparrini A
,
Guo Y
,
Hashizume M
,
Lavigne E
,
Zanobetti A
,
Schwartz J
, et al.
Mortality risk attributable to high and low ambient temperature: a multicountry observational study. Lancet. 2015 Jul;386(9991):369–75. https://doi.org/10.1016/S0140-6736(14)62114-0
52.
Sera F
,
Armstrong B
,
Blangiardo M
,
Gasparrini A
. An extended mixed-effects framework for meta-analysis. Stat Med. 2019 Dec;38(29):5429–44. https://doi.org/10.1002/sim.8362
53.
Chen YY
,
Lee MB
,
Chang CM
,
Liao SC
. Methods of suicide in different psychiatric diagnostic groups. J Affect Disord. 2009 Nov;118(1-3):196–200. https://doi.org/10.1016/j.jad.2009.05.020
54.
Huisman A
,
van Houwelingen CA
,
Kerkhof AJ
. Psychopathology and suicide method in mental health care. J Affect Disord. 2010 Feb;121(1-2):94–9. https://doi.org/10.1016/j.jad.2009.05.024
55.
New AS
,
Trestman RL
,
Mitropoulou V
,
Benishay DS
,
Coccaro E
,
Silverman J
, et al.
Serotonergic function and self-injurious behavior in personality disorder patients. 1997;
56.
Siever LJ
. Neurobiology of aggression and violence. Am J Psychiatry. 2008 Apr;165(4):429–42. https://doi.org/10.1176/appi.ajp.2008.07111774
57.
Haber G
,
Sampson J
,
Graubard B
. Bias due to Berkson error: issues when using predicted values in place of observed covariates. Biostatistics. 2020.
Supplementary material
Table S1ICD-10 codes for intentional self-harm.
|
ICD -10
|
Chapter XX: intentional self-harm
|
|
X60–69
|
Intentional self-poisoning by and exposure to:
|
| X60 |
nonopioid analgesics, antipyretics and antirheumatics |
| X61 |
antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified |
| X62 |
narcotics and psychedelics [hallucinogens], not elsewhere classified |
| X63 |
other drugs acting on the autonomic nervous system |
| X64 |
other and unspecified drugs, medicaments and biological substances |
| X65 |
alcohol |
| X66 |
organic solvents and halogenated hydrocarbons and their vapours |
| X67 |
other gases and vapours |
| X68 |
pesticides |
| X69 |
other and unspecified chemicals and noxious substances |
|
X70–84
|
Intentional self-harm by:
|
| X70 |
hanging, strangulation and suffocation |
| X71 |
drowning and submersion |
| X72 |
handgun discharge |
| X73 |
rifle, shotgun and larger firearm discharge |
| X74 |
other and unspecified firearm discharge |
| X75 |
explosive material |
| X76 |
smoke, fire and flames |
| X77 |
steam, hot vapours and hot objects |
| X78 |
sharp object |
| X79 |
blunt object |
| X80 |
jumping from a high place |
| X81 |
jumping or lying before moving object |
| X82 |
crashing of motor vehicle |
| X83 |
other specified means |
| X84 |
unspecified means |

Figure S1 Topographical map of Switzerland, divided into seven major regions: Lake Geneva (cantons Vaud, Valais, Geneva); Midland (cantons Bern, Fribourg, Solothurn, Neuchâtel, Jura); North-West (cantons Basel-Stadt, Basel-Landschaft, Aargau); Zurich (canton Zurich); East (cantons Glarus, Schaffhausen, Appenzell Ausserrhoden, Appenzell Innerrhoden, St. Gallen, Graubünden, Thurgau); Central (cantons Lucerne, Uri, Schwyz, Obwalden, Nidwalden, Zug); Ticino (canton Ticino).
Sunshine duration data
For 13 meteorological stations, we collected the total hours of sunshine per day (measured hourly), as well as the corresponding percentage of the measured sunshine duration in relation to the maximum possible sunshine duration at the location on that day of the year.
We choose the following stations for the seven major regions of Switzerland: Genève/Cointrin, Sion and Pully for Lake Geneva; Neuchâtel and Bern/Zollikofen for Midland; Basel/Binningen and Buchs/Aarau for North-West; Zürich/Fluntern for Zurich; Aadorf/Tänikon, Chur and St. Gallen for East; Luzern for Central; Lugano for Ticino. For some regions, more meteorological stations recording sunshine duration data were available than we selected. However, we only choose the stations with complete data for the whole study period and excluded stations which seemed not representative for the populated area of a region (e.g., meteorological stations on mountain tops). We also referred to meteorological stations used in previous studies [24].
Table S2Summary statistics of sunshine data in the seven major regions of Switzerland.
|
Region
|
Hours per day
|
% of the maximum possible sunshine
|
| Lake Geneva |
5.1 (1.2, 9.2) |
52 (12, 86) |
| Midland |
3.9 (0.4, 8.5) |
35 (4, 75) |
| North-West |
3.3 (0.2, 7.9) |
29 (3, 69) |
| Zurich |
3.5 (0.4, 8.1) |
32 (3, 71) |
| East |
3.6 (0.4, 7.6) |
35 (4, 78) |
| Central |
2.8 (0.1, 7.3) |
26 (1, 66) |
| Ticino |
6.5 (1.7, 9.3) |
66 (16, 93) |
Table S3Confounding by sunshine duration.
|
Model
|
RR
|
| Main model |
1.34 (1.18–1.52) |
| Main model + sunshine (hours) |
1.30 (1.14–1.48) |
| Main model + sunshine (%) |
1.30 (1.13–1.48) |
Table S4Summary statistics of suicides per year in Switzerland.
|
Year
|
Total
|
Sex
|
Age group
|
Method
|
|
Male
|
Female
|
<35
|
35–65
|
>65
|
Nonviolent
|
Violent
|
| 1995 |
1,306 (5.4) |
971 (74.3) |
335 (25.7) |
310 (23.7) |
671 (51.4) |
325 (24.9) |
121 (9.3) |
1,185 (90.7) |
| 1996 |
1,200 (5.0) |
884 (73.7) |
316 (26.3) |
307 (25.6) |
615 (51.2) |
278 (23.2) |
101 (8.4) |
1,099 (91.6) |
| 1997 |
1,153 (4.8) |
876 (76.0) |
277 (24.0) |
291 (25.2) |
590 (51.2) |
272 (23.6) |
125 (10.8) |
1,028 (89.2) |
| 1998 |
1,212 (5.0) |
931 (76.8) |
281 (23.2) |
299 (24.7) |
630 (52.0) |
283 (23.3) |
83 (6.8) |
1,129 (93.2) |
| 1999 |
1,148 (4.8) |
855 (74.5) |
293 (25.5) |
267 (23.3) |
593 (51.7) |
288 (25.1) |
90 (7.8) |
1,058 (92.2) |
| 2000 |
1,209 (5.0) |
896 (74.1) |
313 (25.9) |
286 (23.7) |
626 (51.8) |
297 (24.6) |
112 (9.3) |
1,097 (90.7) |
| 2001 |
1,119 (4.6) |
857 (76.6) |
262 (23.4) |
246 (22.0) |
605 (54.1) |
268 (23.9) |
102 (9.1) |
1,017 (90.9) |
| 2002 |
1,246 (5.2) |
908 (72.9) |
338 (27.1) |
271 (21.7) |
677 (54.3) |
298 (23.9) |
114 (9.1) |
1,132 (90.9) |
| 2003 |
1,055 (4.4) |
775 (73.5) |
280 (26.5) |
219 (20.8) |
563 (53.4) |
273 (25.9) |
114 (10.8) |
941 (89.2) |
| 2004 |
1,067 (4.4) |
765 (71.7) |
302 (28.3) |
207 (19.4) |
612 (57.4) |
248 (23.2) |
116 (10.9) |
951 (89.1) |
| 2005 |
1,089 (4.5) |
805 (73.9) |
284 (26.1) |
225 (20.7) |
590 (54.2) |
274 (25.2) |
96 (8.8) |
993 (91.2) |
| 2006 |
1,041 (4.3) |
749 (72.0) |
292 (28.0) |
225 (21.6) |
570 (54.8) |
246 (23.6) |
123 (11.8) |
918 (88.2) |
| 2007 |
1,083 (4.5) |
799 (73.8) |
284 (26.2) |
221 (20.4) |
579 (53.5) |
283 (26.1) |
119 (11.0) |
964 (89.0) |
| 2008 |
1,027 (4.3) |
743 (72.3) |
284 (27.7) |
201 (19.6) |
552 (53.7) |
274 (26.7) |
100 (9.7) |
927 (90.3) |
| 2009 |
1,056 (4.4) |
804 (76.1) |
252 (23.9) |
192 (18.2) |
595 (56.3) |
269 (25.5) |
99 (9.4) |
957 (90.6) |
| 2010 |
950 (3.9) |
705 (74.2) |
245 (25.8) |
166 (17.5) |
533 (56.1) |
251 (26.4) |
109 (11.5) |
841 (88.5) |
| 2011 |
1,007 (4.2) |
748 (74.3) |
259 (25.7) |
192 (19.1) |
531 (52.7) |
284 (28.2) |
106 (10.5) |
901 (89.5) |
| 2012 |
1,027 (4.3) |
753 (73.3) |
274 (26.7) |
187 (18.2) |
560 (54.5) |
280 (27.3) |
107 (10.4) |
920 (89.6) |
| 2013 |
1,038 (4.3) |
774 (74.6) |
264 (25.4) |
175 (16.9) |
583 (56.2) |
280 (27.0) |
112 (10.8) |
926 (89.2) |
| 2014 |
996 (4.1) |
744 (74.7) |
252 (25.3) |
163 (16.4) |
518 (52.0) |
315 (31.6) |
104 (10.4) |
892 (89.6) |
| 2015 |
1,040 (4.3) |
777 (74.7) |
263 (25.3) |
191 (18.4) |
539 (51.8) |
310 (29.8) |
99 (9.5) |
941 (90.5) |
| 2016 |
998 (4.1) |
754 (75.6) |
244 (24.4) |
168 (16.8) |
538 (53.9) |
292 (29.3) |
101 (10.1) |
897 (89.9) |
| Overall |
24,067 |
17,873 (74.3) |
6,194 (25.7) |
5,009 (20.8) |
12,870 (53.5) |
6,188 (25.7) |
2,353 (9.8) |
21,714 (90.2) |
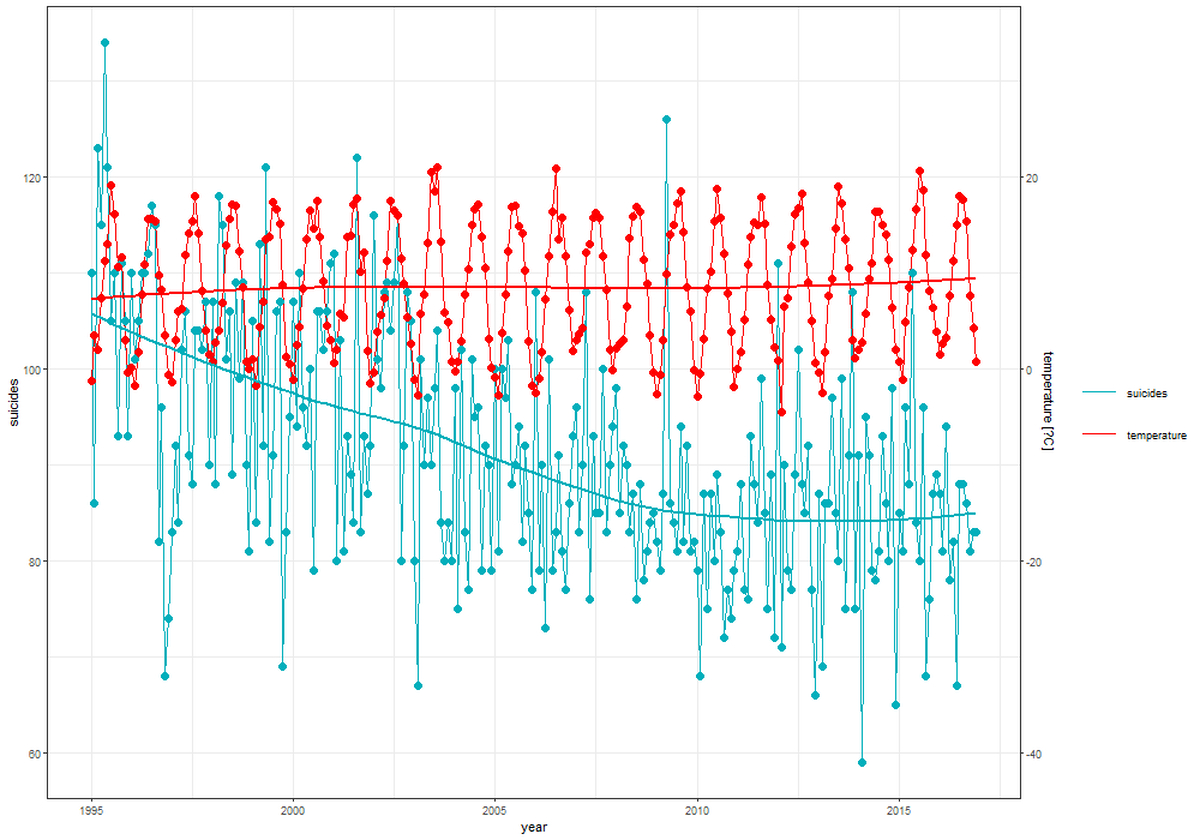
Figure S2 Time trends of suicides and temperature in Switzerland from 1995 to 2016. Suicide counts per month with integrated regression (loess function – blue); temperature in °C per month with integrated regression (loess function – red).