Figure 1 Flowchart summarising sampling of the study participants.
DOI: https://doi.org/10.4414/SMW.2021.w30054
Cannabidiol (CBD) is a cannabinoid produced by the Cannabis sativa plant that has become very popular over the past few years, notably in Europe [1]. Cannabis sativa contains several active principles including more than 90 cannabinoids, and the 2 most abundant cannabinoids are delta-9-tetrahydrocannabinol (THC), commonly used for its psychoactive effects, and CBD [2]. Although the concentration of CBD does not appear to have changed over the past five decades, there has been a significant increase in THC concentration in international cannabis markets [3]. Unlike THC, CBD has no psychoactive effects and has potential anti-inflammatory, anti-oxidant, anxiolytic and analgesic effects [4, 5]. In Switzerland, following a change in the ordinance on illegal drugs by the Swiss Federal administration, use and sales of CBD products containing less than 1% of THC are legal (products with 1% or more THC are still illegal). Since 2016, following the delivery of authorisations to commercialise CBD products by the authorities, there has been a strong increase in sales of CBD in Switzerland, and different CBD products are available on the market. CBD is sold as dried flowers, CBD cigarettes or pre-rolled joints that are generally smoked, or as liquid for e-cigarettes. It is also sold as CBD oil or tincture, which is generally placed under the tongue. Less commonly, CBD is sold as pills, crystals, edibles and cosmetics. Studies have tested the effect of CBD on health but, as of today, evidence concerns pharmacological products (pure form of CBD) and more high quality evidence is needed [6]. There are hypothesised beneficial effects based on animal models and pharmacological studies, but evidence regarding the efficacy of CBD retail products is lacking [7]. Specifically, one should not assume that evidence from research with pharmaceutical CBD products such as Epidiolex® can be applied to retail CBD products [7].
To date, data on use of CBD products in Switzerland are scarce. One exception is a study by Zobel and colleagues, with data collected on modes of administration and motives for CBD use in a sample of 1500 CBD users recruited online and through social media [8]. Results showed that most CBD users also use tobacco/e-cigarettes (80%) and THC (61%). The CBD products that were the most frequently used were flowers (83%), oil (17%) and cigarettes (13%). Zobel and colleagues showed that the main motive to initiate CBD use was out of curiosity (44%). In contrast, among current users, CBD was most frequently used for perceived beneficial effects on well-being and health, to be able to use cannabis legally and to control their use of THC. The main limitation of this study was the use of a convenience sample of users, which prevents estimation of the prevalence of use of CBD in the general population.
Given that CBD can only recently be legally bought and consumed in Switzerland, and that it is perceived as having beneficial effects on health or that it could be used as an alternative to THC [9–11], it is important to have data on the prevalence of use and whether or not it is associated with other behaviours, notably behaviours with negative effects on health such as smoking.
Using data from a cohort study, we aimed to estimate prevalence of use, modes of administration and motives for using CBD in an unselected population sample of young Swiss men. We also tested associations between CBD use, THC use and tobacco use and demographic characteristics.
The sample consisted of an unselected population sample of young Swiss men who participated in the Cohort Study on Substance Use Risk Factors (C-SURF). C-SURF participants were recruited in 2010 and completed four waves of assessment (wave 1: 2010–2011; wave 2: 2012–2013; wave 3: 2016–2017; wave 4: 2019–2020).
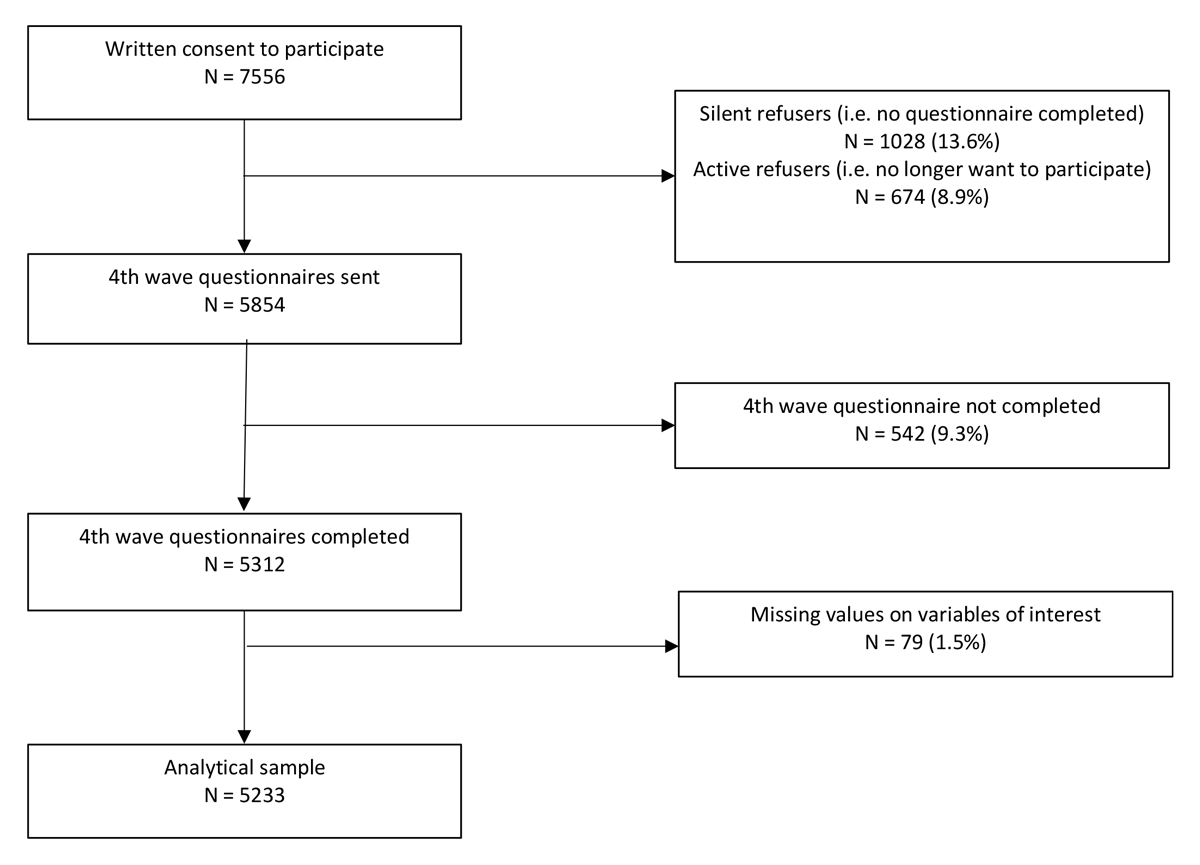
All young men presenting at three of six army recruitment centres for the mandatory procedure assessing their eligibility to serve were offered participation [12]. This mandatory procedure covers 98% of the Swiss male population. C-SURF participation was offered in three centres. These centres cover 21 of the 26 Swiss cantons. Participation in the study was independent of the army. Data for the current study were drawn from the fourth wave of C-SURF. In 2010, 7556 young men gave their written consent to participate in the study during enrolment. Those who did not complete at least one of the first three questionnaires (silent refusers, n = 1028) and those who completed at least one of the three first questionnaires but did not want to participate to additional questionnaires (active refusers, n = 674) were not sent the fourth wave questionnaire. From the 5854 young Swiss men invited, the fourth wave questionnaire was completed between April 2019 and June 2020 by 5312 (90.7% of those invited), including users and non-users of CBD. A total of 79 (1.5%) respondents were excluded from the analyses because they had missing values on the variables of interest, leaving 5233 participants in the analytical sample. A flowchart summarising sampling of the participants included in the analyses is depicted in figure 1. The study was approved by the Ethics committee of the Canton of Vaud (Commission cantonale d’éthique de la recherche sur l’être humain, CER-VD, protocol 15/07).
Figure 1 Flowchart summarising sampling of the study participants.
All C-SURF assessments rely on self-report. The C-SURF fourth wave questionnaire included questions to specifically assess use of CBD (defined as legal cannabis containing <1% of THC) and THC (defined as illegal cannabis containing 1% or more of THC). Questions on CBD use included lifetime use (yes/no) and use in the past 12 months (yes/no with additional response options among those reporting use: once a month or less, two to four times a month, two to three times per week, four to five times per week, daily or almost daily). We investigated the use of nine CBD products: flowers of legal cannabis with and without tobacco to be smoked in joints, bongs or waterpipes, CBD cigarettes (commercially available), oil (or tincture, drops), food products, pills, wax and crystals.
Motives for using CBD were investigated with nine questions: to treat a disease / reduce symptoms, for well-being and health, to feel the effects of cannabis, to avoid the effect of THC, to take cannabis legally, to reduce/stop using THC, to reduce/stop using tobacco, to reduce/stop using other substances, and out of curiosity. For the CBD-related questions we used the same approach as a study commissioned by the Swiss Federal Office of Public Health and conducted by Zobel et al. [8].
Use of THC, cigarettes and e-cigarettes in the past 12 months were also requested , as well as age, linguistic region (German- or French-speaking), highest achieved educational level (primary; vocational; secondary and post-secondary), perceived income relative to others (below average; average; above average). All measures were self-reported.
Descriptive statistics (absolute and relative frequencies) were used to estimate the prevalence of use, the prevalence of the various modes of administration, and the reason for using CBD in the total sample. Prevalence of the various modes of administration and the reason for using CBD were also computed separately for infrequent (once a month or less often) and frequent (more than once a month) CBD users and differences were tested using the chi-square test and Fisher exact test (when cells had expected counts <5). P-values, considered as significant when p <0.05, were reported for results of chi-square and Fisher exact tests. Logistic regressions models were used to assess the bivariate and fully adjusted (with all predictors in the model) associations between past 12 months use of CBD use and THC, cigarette, e-cigarette use, age, highest achieved educational level, perceived income, and linguistic region. Logistic regression models were used to assess the associations between frequent vs infrequent use of CBD and THC, cigarette, e-cigarette use, age, highest achieved educational level, perceived income, and linguistic region. Odds ratios (ORs) and 95% confidence intervals (CIs) were used to report results of logistic regressions. ORs were considered as significant when the 95% CI did not include 1.
The sample comprised 5233 men, with a mean age of 28.2 years (standard deviation 1.3) ; 57.7% were from the French-speaking region of Switzerland, 42.3% from the German-speaking region. Details are presented in table 1.
Lifetime prevalence of use of CBD was 32.4% and prevalence of use in the past 12 months was 18.5%. Among users in the past 12 months, 79.4% used CBD once a month or less often, whereas regular use was rare, with only 20.6% of users using it more than once a month (2–4 times a month, 11.8%; 23 times per week, 3.7%; 45 times per week, 2.0%; daily or almost daily, 3.1%)
Table 1Characteristics of the study sample (n = 5233).
| Mean ± SD / n (%) | ||
| Age (years) | 28.2 ± 1.3 | |
| Linguistic region | French speaking | 3020 (57.7%) |
| German speaking | 2213 (42.3%) | |
| Highest achieved educational level | Primary schooling | 133 (2.5%) |
| Vocational | 1915 (36.6%) | |
| Secondary and post-secondary | 3185 (60.9%) | |
| Perceived income | Below average | 1681 (32.1%) |
| Average | 1598 (30.5%) | |
| Above average | 1954 (37.3%) | |
| Use of CBD products | Never | 3536 (67.6%) |
| Yes, but not in the past 12 months | 729 (13.9%) | |
| Yes, past 12 months | 968 (18.5%) | |
| Frequency of use of CBD products (among past 12-month users) | Once a month or less often | 769 (79.4%) |
| More than once a month | 199 (20.6%) | |
| Use of THC, past 12 months | No | 3850 (73.6%) |
| Yes | 1383 (26.4%) | |
| Use of cigarettes (tobacco), past 12 months | No | 3163 (60.4%) |
| Yes | 2070 (39.6%) | |
| Use of e-cigarettes, past 12 months | No | 4540 (86.8%) |
| Yes | 693 (13.2%) | |
CBD: cannabidiol; SD: standard deviation; THC: tetrahydrocannabinol
Note: all measures are self-reported
Modes of administration of CBD are presented in table 2. The most often reported modes of administration were in association with tobacco: 67.5% reported using cannabis flowers mixed with tobacco in joints or bong, and 37.1% used CBD cigarettes with tobacco, whereas 18.6% used cannabis flowers without tobacco. CBD oil and food was reported less often with only slightly more than 10% of the users.
Use of CBD products in multiple forms was frequent: of those using flowers with tobacco, 51.6% used other CBD products. Percentage of use of other products was 63.2% among those using CBD cigarettes, 74.3% among those using CBD oil, 78.4% among those using e-liquid, 82.7% among those using CBD food products, 82.8% among those using flowers without tobacco, 83.3% among those using pills and 100% among those using wax or crystals.
As opposed to infrequent CBD users, frequent users were significantly more likely to report use of CBD flowers with and without tobacco and CBD oil, whereas infrequent CBD users were significantly more likely to report use of CBD cigarettes than frequent users.
Table 2Modes of administration of CBD among users in the past 12 months(n = 968).
| Mode of administration of CBD | Total (n = 968) | Infrequent users (once a month or less often, n = 769) | Frequent users (more than once a month, n = 199) | p-value | ||||
| N | % | N | % | N | % | |||
| Flowers with tobacco | 653 | 67.5% | 501 | 65.1 | 152 | 76.4 | 0.003a | |
| Cigarettes | 359 | 37.1% | 312 | 40.6 | 47 | 23.6 | <0.001a | |
| Flowers without tobacco | 180 | 18.6% | 127 | 16.5 | 53 | 26.6 | 0.001a | |
| Oil | 136 | 14.0% | 89 | 11.6 | 47 | 23.6 | <0.001a | |
| Food | 110 | 11.4% | 82 | 10.7 | 28 | 14.1 | 0.177a | |
| E-liquid | 51 | 5.3% | 36 | 4.7 | 15 | 7.5 | 0.108a | |
| Wax | 18 | 1.9% | 13 | 1.7 | 5 | 2.5 | 0.392b | |
| Crystals | 13 | 1.3% | 8 | 1.0 | 5 | 2.5 | 0.157b | |
| Pills | 12 | 1.2% | 9 | 1.2 | 3 | 1.5 | 0.719b | |
Note: Participants could select multiple response options. a from chi-square test. b from Fisher exact test. All measures were self-reported.
The majority of users reported using CBD out of curiosity. Between 30% and 40% reported using CBD as a means to use cannabis legally, to feel and avoid the effects of THC and for health and well-being. Using CBD out of curiosity was significantly more prevalent among infrequent than frequent CBD users. The other motives were significantly more prevalent among frequent than infrequent CBD users. Details are reported in table 3.
Table 3Motives for using CBD products among users in the past 12 months (n = 968).
| Motives to use CBD products | Total (n = 968) | Infrequent users (once a month or less often, n = 769) | Frequent users (more than once a month, n = 199) | p-valuea | |||
| N | % | N | % | N | % | ||
| Out of curiosity | 716 | 74.0% | 611 | 79.5 | 105 | 52.8 | <0.001 |
| To feel the effects of THC | 369 | 38.1% | 255 | 33.2 | 114 | 57.3 | <0.001 |
| For well-being and health | 363 | 37.5% | 233 | 30.3 | 130 | 65.3 | <0.001 |
| To use cannabis legally | 352 | 36.4% | 235 | 30.6 | 117 | 58.8 | <0.001 |
| To avoid the effect of THC | 307 | 31.7% | 187 | 24.3 | 120 | 60.3 | <0.001 |
| To reduce / stop using THC | 188 | 19.4% | 106 | 13.8 | 82 | 41.2 | <0.001 |
| To treat a disease / reduce symptoms | 149 | 15.4% | 90 | 11.7 | 59 | 29.6 | <0.001 |
| To reduce / stop using tobacco | 104 | 10.7% | 50 | 6.5 | 54 | 27.1 | <0.001 |
| To reduce / stop using other substances | 48 | 5.0% | 32 | 4.2 | 16 | 8.0 | 0.025 |
CBD: cannabidiol; THC: tetrahydrocannabinol
Note: Participants could select multiple response options. a from chi-square test. All measures were self-reported
In bivariate analyses, use of CBD in the past 12 months was significantly associated with the use of THC, cigarettes, e-cigarettes, linguistic region, age, and perceived income (table 4). The association between CBD use and THC use was particularly strong: more than half of THC users reported CBD use (50.6%), compared with 7% of those not using THC (OR 13.70, 95% CI 11.64–16.12). Participants living in the French-speaking part of Switzerland were more likely (OR 1.31, 95% CI 1.14–1.51]) to use CBD than those living in the German-speaking part of the country. There was no association between socioeconomic status and CBD use.
In multivariable analyses, associations remained significant for use of THC (OR 9.85, 95% CI 8.28–11.73), cigarettes (OR 2.74, 95% CI 2.28–3.29) or e-cigarettes (OR 1.57, 95% CI 1.27–1.95), as well as for the linguistic region (OR 1.38, 95% CI 1.15–1.65).
Bivariate analyses investigating the associations of frequent (vs infrequent) CBD use showed significant associations for THC (OR 1.56, 95% CI 1.07–2.26) and e-cigarette (OR 1.47, 95% CI 1.05–2.07]) use and age (OR 1.17, 95% CI 1.05–1.31). In multivariable analyses, associations remained significant for use of THC (OR 1.61, 95% CI 1.10–2.37) and age (OR 1.17, 95% CI 1.04–1.32).
Table 4Associations between CBD use and demographics and other substance use.
| CBD use, n (%) | Logistic regression predicting past 12 months use of CBD | Frequent use of CBD (among CBD users), n (%) | Logistic regression predicting frequent (vs infrequent) use of CBD | ||||||||
| Bivariate | Fully adjusted | Bivariate | Fully adjusted | ||||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | ||||
| THC | Users (n = 1383) | 700 (50.6%) | 13.70 | 11.64–16.12 | 9.85 | 8.28–11.73 | 157 (22.4%) | 1.56 | 1.07–2.26 | 1.61 | 1.10–2.37 |
| Non-users (n = 3850) | 268 (7.0%) | ref. | ref. | 42 (15.7%) | ref. | ref. | |||||
| Cigarette | User (n = 2070) | 710 (34.3%) | 5.88 | 5.03, 6.87 | 2.74 | 2.28–3.29 | 153 (21.5%) | 1.27 | 0.88–1.83 | 1.04 | 0.71–1.53 |
| Non-users (n = 3850) | 258 (8.2%) | ref. | ref. | 46 (17.8%) | ref. | ref. | |||||
| E-Cigarette | User (n = 693) | 247 (35.6%) | 2.93 | 2.46, 3.49 | 1.57 | 1.27–1.95 | 63 (25.5%) | 1.47 | 1.05–2.07 | 1.41 | 0.99–2.02 |
| Non-users (n = 4540) | 721 (15.9%) | ref. | ref. | 136 (18.9%) | ref. | ref. | |||||
| Linguistic region | French-speaking (n = 3020) | 610 (20.2%) | 1.31 | 1.14–1.51 | 1.38 | 1.15–1.65 | 132 (21.6%) | 1.20 | 0.86–1.67 | 1.07 | 0.76–1.52 |
| German-speaking (n = 2213) | 358 (16.2%) | ref. | ref. | 67 (18.7%) | ref. | ref. | |||||
| Age | 1.06 | 1.002–1.12 | 1.06 | 0.99–1.14 | 1.17 | 1.05–1.31 | 1.17 | 1.04–1.32 | |||
| Education | Primary schooling (n = 133) | 31 (23.3%) | ref. | ref. | 7 (22.6%) | ref. | ref. | ||||
| Vocational (n = 1915) | 350 (18.3%) | 0.74 | 0.48–1.12 | 1.49 | 0.91–2.44 | 81 (23.1%) | 1.03 | 0.43–2.48 | 1.27 | 0.52–3.14 | |
| Post-secondary (n = 3185) | 587%) | 0.74 | 0.49–1.12 | 1.53 | 0.94–2.49 | 111(18.9%) | 0.80 | 0.34–1.90 | 1.07 | 0.44–2.62 | |
| Perceived income | Below average (n = 1681) | 394%) | 1.37 | 1.16–1.62 | 1.06 | 0.86–1.30 | 83 (21.1%) | 0.91 | 0.63–1.32 | 0.92 | 0.63–1.34 |
| Average (n = 1598) | 292 | ref. | ref. | 66 (22.6%) | ref. | ref. | |||||
| Above average (n = 1954) | 282 | 0.75 | 0.63–0.90 | 0.83 | 0.67–1.03 | 50 (17.7%) | 0.74 | 0.49–1.11 | 0.76 | 0.50–1.16 | |
CBD: cannabidiol; THC: tetrahydrocannabinol; OR: odds ratio; CI: confidence interval; ref:reference
This study shows that CBD self-reported use is common in a non-selected population sample of young Swiss men. About one third used it at least once in their lifetime and about one in five used it in the previous 12 months. Most CBD users used it infrequently and out of curiosity. Only 20% of users (corresponding to a 4% prevalence in the full sample) used it more than once a month. With a prevalence of CBD use of more than 50% among illegal cannabis users (vs 7% among non-users), CBD use was strongly associated with illegal cannabis use, with about three out offour CBD users also using cannabis with THC. Zobel and colleagues showed similarly that the most frequently encountered profile was that of people using THC also using CBD products [8]. As of today, while prevalent, CBD is thus mostly used out of curiosity, by people using THC, and regular use is not the norm. Prevalence was higher in the French-speaking region than in the German-speaking region, indicating regional differences. There are known regional differences in Switzerland with higher prevalence of unhealthy alcohol use, tobacco use and illicit drug use in the French-speaking region than the German speaking region [13]. CBD appears to follow the same pattern. CBD use, unlike use of other substances, was not associated with socioeconomic status [14].
There were differences in modes of administration of CBD and motives for CBD use between frequent and infrequent CBD users. Frequent users were more likely to use flowers with and without tobacco and oil, whereas infrequent users were more likely to report use of CBD cigarettes. These differences may be explained by the cost of the different products and indicate a tendency among frequent users to prepare their own product (compared with already prepared CBD cigarettes), a mode of administration that is more similar to THC. Unsurprisingly, frequent users were less likely to report using CBD out of curiosity.
According to our results, and in accordance with the study by Zobel et al. conducted in Switzerland [8], CBD is mostly used in combination with tobacco and is smoked. Nevertheless, CBD use in multiple forms is reported by the majority and more than half of those using CBD flowers with tobacco, the most frequently reported mode of administration, reported using CBD in other forms. CBD use in multiple forms also appears to be the norm in other studies [9]. Nevertheless, compared with studies conducted in the US, smoking CBD products was the most often reported mode of administration in Switzerland, compared with the use of edible products in the US [9, 10].
Given that, in the present study, the most prevalent modes of administration are via smoking, and involve tobacco, most CBD users are exposed to risks associated with smoking, and with smoking tobacco. In addition, little is known about the potential combined effects on health of inhaling CBD and tobacco, and one pilot in vitro study indicated that there may be additive toxic effects when vaping CBD and nicotine products together [15]. In addition, data from Switzerland suggested that users cannot adequately rely on indications from vendors, as deviations in the total CBD content from e-liquid products were frequently observed [16]. Therefore, risks of tobacco/nicotine product exposure should be taken into account when assessing the potential health consequences of CBD use.
Many participants reported using CBD for well-being and health, to treat a disease or reduce symptoms. This is in line with the evaluations of CBD products observed in other studies [9]. There are potential beneficial effects of CBD, notably on chronic pain, epilepsy and chemotherapy caused nausea and vomiting [17, 18], but currently available data are from studies of pharmacological administration of pure CBD. Thus, effects cannot be extrapolated to low-dose administration through other routes. Although research on the effect of CBD is active, there is a current lack of evidence of efficacy and safety for CBD non-pharmacological products and health effects have not been evaluated for inhaled CBD, notably when combined with tobacco products [19, 20].
Although the present study has the advantage of exploring CBD use and motives for CBD use in a large non-selected sample, limitations include the use of a sample consisting of Swiss males only, aged between 25 and 30. Thus results are not generalisable to women and non-Swiss individuals and to other age groups. In addition, this is a cross-sectional study and thus the potential impact of CBD use on THC use could not be evaluated. A longitudinal study may allow assessment of whether CBD use is associated with changes over time in THC and/or tobacco use/co-use.
All measures were self-reported. In addition, there is a known variation in CBD content of CBD products and a known variation in THC content in illegal cannabis markets [3, 16]. Given the legal/illegal status of CBD/THC, we can expect that legally sold products may only contain <1% THC, but the CBD content may differ between products and vendors.
In our study, CBD use was associated with THC use (OR 13.70), cigarette (OR 5.88) and e-cigarette use (OR 2.93). The design of the study does not allow investigation of causal links between CBD and use of other substances and the question of the causality and the direction of the association between CBD use and THC and cigarette use remains open. THC and cigarette use could affect later CBD use or CBD use could influence later use of THC and cigarettes. Notably, as reported among the motives for using CBD and consistently with other surveys [9, 10], CBD products may be used to decrease the use of other substance (or be used instead of other substances in some instances) such as cannabis or tobacco cigarettes. Nevertheless, it could also contribute to their escalation, and the present study cannot address this question. These associations may vary as a function of modes of administration and motives for using CBD, and this should be investigated in future longitudinal studies.
The study was funded by the Swiss National Science Foundation, Grant number: FN33CS30_148493.
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest was disclosed.
1. VanDolah HJ , Bauer BA , Mauck KF . Clinicians’ Guide to Cannabidiol and Hemp Oils. Mayo Clin Proc. 2019 Sep;94(9):1840–51. https://doi.org/10.1016/j.mayocp.2019.01.003
2. Andre CM , Hausman JF , Guerriero G . Cannabis sativa: The Plant of the Thousand and One Molecules. Front Plant Sci. 2016 Feb;7:19. https://doi.org/10.3389/fpls.2016.00019
3. Freeman TP , Craft S , Wilson J , Stylianou S , ElSohly M , Di Forti M , et al. Changes in delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) concentrations in cannabis over time: systematic review and meta-analysis. Addiction. 2021 May;116(5):1000–10. https://doi.org/10.1111/add.15253
4. Pisanti S , Malfitano AM , Ciaglia E , Lamberti A , Ranieri R , Cuomo G , et al. Cannabidiol: state of the art and new challenges for therapeutic applications. Pharmacol Ther. 2017 Jul;175:133–50. https://doi.org/10.1016/j.pharmthera.2017.02.041
5. White CM . A Review of Human Studies Assessing Cannabidiol’s (CBD) Therapeutic Actions and Potential. J Clin Pharmacol. 2019 Jul;59(7):923–34. https://doi.org/10.1002/jcph.1387
6. Larsen C , Shahinas J . Dosage, Efficacy and Safety of Cannabidiol Administration in Adults: A Systematic Review of Human Trials. J Clin Med Res. 2020 Mar;12(3):129–41. https://doi.org/10.14740/jocmr4090
7. Sholler DJ , Schoene L , Spindle TR . Therapeutic efficacy of cannabidiol (CBD): a review of evidence from clinical trials and human laboratory studies. Curr Addict Rep. 2020 Sep;7(3):405–12. https://doi.org/10.1007/s40429-020-00326-8
8. Zobel F, Notari L, Schneider E, Rudmann O , et al. Cannabidiol (CBD): analyse de situation. 2018Lausanne: Addiction Suisse.
9. Wheeler M , Merten JW , Gordon BT , Hamadi H . CBD (Cannabidiol) Product Attitudes, Knowledge, and Use Among Young Adults. Subst Use Misuse. 2020;55(7):1138–45. https://doi.org/10.1080/10826084.2020.1729201
10. Corroon J , Phillips JA . A Cross-Sectional Study of Cannabidiol Users. Cannabis Cannabinoid Res. 2018 Jul;3(1):152–61. https://doi.org/10.1089/can.2018.0006
11. Berg CJ , Getachew B , Pulvers K , Sussman S , Wagener TL , Meyers C , et al. Vape shop owners’/managers’ attitudes about CBD, THC, and marijuana legal markets. Prev Med Rep. 2020 Sep;20:101208. https://doi.org/10.1016/j.pmedr.2020.101208
12. Gmel G , Akre C , Astudillo M , Bähler C , Baggio S , Bertholet N , et al. The Swiss cohort study on substance use risk factors : findings of two waves. Sucht. 2015;61(4):251–62. https://doi.org/10.1024/0939-5911.a000380
13. Gmel G, Kuendig H, Notari L, Gmel C. Monitorage suisse des addictions : consommation d’alcool, tabac et drogues illégales en Suisse en 2016. 2017, Addiction Suisse: Lausanne, Switzerland.
14. Charitonidi E , Studer J , Gaume J , Gmel G , Daeppen JB , Bertholet N . Socioeconomic status and substance use among Swiss young men: a population-based cross-sectional study. BMC Public Health. 2016 Apr;16(1):333. https://doi.org/10.1186/s12889-016-2949-5
15. Leigh NJ , Goniewicz ML . Effect of aerosolized nicotine on human bronchial epithelial cells is amplified after co-administration with cannabidiol (CBD): a pilot in vitro study. BMC Pharmacol Toxicol. 2020 Jun;21(1):42. https://doi.org/10.1186/s40360-020-00418-1
16. Grafinger KE , Krönert S , Broillet A , Weinmann W . Cannabidiol and tetrahydrocannabinol concentrations in commercially available CBD E-liquids in Switzerland. Forensic Sci Int. 2020 May;310:110261. https://doi.org/10.1016/j.forsciint.2020.110261
17. Freeman TP , Hindocha C , Green SF , Bloomfield MA . Medicinal use of cannabis based products and cannabinoids. BMJ. 2019 Apr;365:l1141. https://doi.org/10.1136/bmj.l1141
18. Whiting PF , Wolff RF , Deshpande S , Di Nisio M , Duffy S , Hernandez AV , et al. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA. 2015 Jun;313(24):2456–73. https://doi.org/10.1001/jama.2015.6358
19. Chesney E , McGuire P , Freeman TP , Strang J , Englund A . Lack of evidence for the effectiveness or safety of over-the-counter cannabidiol products. Ther Adv Psychopharmacol. 2020 Sep;10:2045125320954992. https://doi.org/10.1177/2045125320954992
20. Chesney E , Oliver D , Green A , Sovi S , Wilson J , Englund A , et al. Adverse effects of cannabidiol: a systematic review and meta-analysis of randomized clinical trials. Neuropsychopharmacology. 2020 Oct;45(11):1799–806. https://doi.org/10.1038/s41386-020-0667-2