COVID-19 pandemic and health related quality of life in primary school children in Switzerland: a repeated cross-sectional study
DOI: https://doi.org/10.4414/SMW.2021.w30071
Bettina
Bringolf-Islerab, Johanna
Hänggiab, Bengt
Kayserc, L. Suzanne
Suggsd, Alain
Dösseggere, Nicole
Probst-Hensch ab, and the SOPHYA-Study Group
aSwiss Tropical and Public Health Institute, Basel, Switzerland
bUniversity of Basel, Basel, Switzerland
cInstitute of Sport Sciences, University of Lausanne, Lausanne, Switzerland
dInstitute for Public Health and Institute of Communication and Public Policy, Università della Svizzera Italiana, Lugano, Switzerland
eSwiss Federal Institute of Sport Macolin (SFISM), Macolin, Switzerland
Dr. Bettina Bringolf-Isler
Swiss Tropical and Public Health Institute
Socinstrasse 57
CH-4002 Basel
bettina.bringolf[at]swisstph.ch
Summary
BACKGROUND: The COVID-19 pandemic and the resulting containment measures had and still have a profound impact on everyday life. Both the fear of infection and the imposed restrictions can have biopsychosocial consequences. The aim of the present study was to analyze whether there is a difference in the health-related quality of life (HRQoL) of primary school children in 2014/15 compared to in 2020, the first year of the COVID-19 pandemic.
METHODS: The present study included 1,712 children aged 5 to 11 years who either participated in the baseline assessment of the SOPHYA cohort study in 2014/15 or were newly recruited during follow-up of the cohort in 2020. In both surveys, the children invited for participation were identified based on registry data. HRQoL was assessed with the validated KINDL-R questionnaire, which scores HRQoL along six different dimensions.
RESULTS: The overall scores (82.4 [81.8; 83.0] vs. 79.6 [79,1; 80.2]), and in particular the emotional well-being scores (85.6 [84.6; 86.6] vs. 83.3 [82.4; 84.2]), were lower during the year of the pandemic (2020) compared to the survey year 2014/15. The highest decrease between 2014/15 and 2020 in the adjusted models was seen for the youngest age group (–3.9 points), followed by children from families with a high income (–3.2 points), girls (–3.1 points), Swiss citizens (–3.1 points) and children from the German-speaking part of Switzerland (–3.1 points). HRQoL was particularly low during periods with restrictions and at the height of the COVID-19 waves in 2020.
CONCLUSION: The SOPHYA-study showed that HRQoL, and especially emotional well-being, was lower in 5 to 11-year-old children in Switzerland during the first year of the pandemic compared to the results from the survey conducted in 2014/15. In the year of the pandemic, the scores were lowest at the height of the COVID-19 waves and their associated restrictions. As it cannot be distinguished whether fear of the disease itself or the restrictions caused this decrease in HRQoL, containment policies should keep COVID-19 infections as low as possible, but still enable children to profit from protective factors such as leisure activities, physical activity and social contact.
Introduction
The COVID-19 pandemic and the resulting containment measures had and still have a profound impact on everyday life. Both the fear of infection and the imposed restrictions can have biopsychosocial consequences. Children and adolescents, who are generally less susceptible than adults to the health impacts of COVID-19 infection itself [1], are a vulnerable risk group for adverse psychological and social effects of the pandemic [2]. Childhood and adolescence are characterized by a heightened sensitivity to social stimuli and a need for peer interaction [3]. Specifically, social distancing, school closure, loss of leisure activities and familial tensions [3-6], or even exposure to violence and abuse [7], are expected to burden children and adolescents, and there is a worry about negative long-term effects [5]. International studies have found an increase in depressive symptoms and more adolescents suffering from anxiety during the COVID-19 pandemic [8, 9]. Beside mental illnesses, several studies have found stressors like worries [10, 11], helplessness [12], restlessness [10, 11], inattention [11], emotional problems [10], boredom [10], sleep difficulties [13], increased stress [13] and reduced health-related quality of life (HRQoL) in adolescents [4, 14], but also a fear that someone in their closest circle would become seriously ill or die from COVID-19 [11, 15]. As a consequence of the COVID-19 pandemic, adverse health behaviors such as increased media consumption [14], unhealthy diets [16], less physical activity [10, 16] and weight gain [14] have also been described. These unhealthy behaviors form a potentially vicious cycle with poor mental wellbeing. The symptoms related to mental health during the pandemic do not necessarily fall into the category of diseases. They do, however, affect wellbeing and development and may increase the risk of clinical mental disease later in life, depending on genetic make-up and the presence of additional environmental factors [17]. The mental wellbeing of children and adolescents who already had mental health problems before [5, 18], those from families with additional stressors such as a low socioeconomic status or a migration background, younger age groups [4] and those who experienced a severe course of COVID-19 disease in someone in their close social environment were more affected [19, 20]. An important observation was that parents’ and children’s mental health and stress were closely intertwined, and therefore stressors of parents also affected their offspring [20–22].
Most of the studies published to date were conducted in adolescents, and less is known about primary school children. Only very few of the studies were conducted in a population-representative sample [4]. Most of them recruited young people and children via social media and are therefore susceptible to participation bias.
The SOPHYA-study (Swiss children’s objectively assessed PHYsical Activity) [23] is a nationwide representative study in children and adolescents. The main focus of the study is on the determinants of physical activity in Swiss youths. Within the framework of the study, the validated KINDL-questionnaire for HRQoL [24] was used in the context of two cross-sectional surveys. The first survey, conducted in 2014/15, is the baseline assessment for the SOPHYA cohort. The second survey, conducted in 2020, is the baseline assessment for a new sample of 5 to 11-year-olds recruited into the 2014/15 cohort at its first follow-up. The aim of the present study was to analyze whether there was a difference in the HRQoL of primary school children in 2014/15 compared to in 2020, the first year of the COVID-19 pandemic.
Material and methods
Study population
The present study included children aged 5 to 11 years who either participated in the baseline assessment of the SOPHYA cohort study in 2014/15 (SOPHYA1) [23] or were newly recruited during follow-up of the cohort in 2020 (SOPHYA2). In both surveys, the children invited for participation were identified based on national inhabitant registry data. All children living in Switzerland and aged 5 to 11 years at the time of the respective survey were eligible. From these children a random sample, stratified by year of birth and language area, was drawn by the Federal Statistical Office. The two study samples are therefore representative for the Swiss population and comparable across the two survey time points, allowing temporal trends to be tested. In SOPHYA1 and SOPHYA2, 2,241 and 2,760 valid addresses could be obtained respectively. Participant contact was exclusively remote, by phone and by mail, as the participants lived all over Switzerland. The SOPHYA-study is a collaboration between the Swiss Tropical and Public Health Institute in Basel, the leading partner and responsible for the participants in the German- and Romansh-speaking regions, the University of Lausanne, which recruits families in the French-speaking region, and the Università della Svizzera Italiana (USI), which recruits participants in the Italian-speaking part of Switzerland. Because of the time-consuming measurements by accelerometry and to cover seasonal variation, the data collection lasted more than one whole year for each of the two surveys. All parents gave written informed consent for their participation. The study obtained ethics approval from the local competent research ethics commission EKNZ (https://www.eknz.ch/; Project-ID: 2019-01340). The study complied with the latest Helsinki declaration.
Health-related quality of life (HRQoL)
HRQoL was assessed with the validated KINDL-R questionnaire [24]. For each of the three language areas in Switzerland, the official translation of the questionnaire was used (Romansh-speaking people filled in the German questionnaire) [25]. The questionnaire was self-reported by parents, acting as proxies. They provided answers to 24 items on a five-point ordinal Likert scale ranging from “never” to “always”. The questionnaire asked about the situation of the child in the preceding week. Answers were scored along six different dimensions: physical well-being, emotional well-being, self-esteem, family, friends and school. Each of these dimensions consists of four items. The modules were analyzed separately and summed up to give a total HRQoL score. Negatively oriented items were scored inversely. The single scores and the total score were translated into a scalable form between 0 and 100. If missing values occurred and affected less than 70% of the answers contributing to a dimension or the total score, an algorithm proposed by the authors of the KINDL-R-questionnaire was used to replace these missing data [26]. If more than 70% of the answers were missing, the score of the respective participant was excluded from the analyses. The exclusion of participants affected only 2% in SOPHYA1 and less than 1% in SOPHYA2. In 2014/15, all parents answered the questionnaire in paper format. Questionnaires were filled in over the period from May 2014 (first questionnaire answered) to August 2015 (last questionnaire answered). In 2020, parents could either use a QR access code to an online questionnaire or alternatively answer the questions on paper. 96% of the parents preferred the online questionnaire. Questionnaires were filled in over the period from the end of December 2019 (first questionnaire answered) to February 2021 (last questionnaire answered). For an analysis by the month of data collection, participants were labelled as January 2020 if they filled in the questionnaire at the end of December 2019 and as December 2020 if they filled in the questionnaire in January or February 2021, as the COVID situation in Switzerland and the related restrictions did not change within these periods.
Sample characteristics
In 2014/15, sociodemographics like age, sex, parental education (low, medium or high), nationality (Swiss, foreign nation or dual citizen) and household income (less than 6,000 CHF/month, 6,000 to 9,000 CHF/month or more than 9,000 CHF/month) were assessed through a combination of questionnaires and structured telephone interviews, with the parents as proxy contacts, whereas in 2020, sociodemographic information was exclusively obtained via self-reporting online questionnaires. Parental education was classified as “high” if a university degree (including a university of applied sciences degree) was obtained and as “medium” in the case of a professional apprenticeship of at least two years. As only 3-4% were below the cut-off for medium, low and medium education were combined for the statistical analysis. The classification into language regions (German, French and Italian regions) and urbanicity (urban area including isolated cities, agglomerations and rural areas) was done according to the definitions of the Federal Office of Statistics and was assigned for each community via ZIP code [27, 28].
Statistical analyses
First, differences by sample characteristics were calculated using a Χ2 test to assess socioeconomic differences resulting from participation differences between the two surveys. Second, associations between the HRQoL score and each social characteristic were tested using linear regression models, adjusting for the SOPHYA wave (1 or 2). Third, the differences in mean HRQoL scores between 2014/15 and 2020 (year of the COVID-19 pandemic) were tested not only for all subjects, but also for socioeconomic subgroups separately. Linear regressions with HRQoL as the dependent variable and the year of the survey as the independent one were conducted for all subjects and in the respective subgroups, as both bivariate analyses and multivariate analyses, adjusting for sample characteristics showing significant associations with the HRQoL score or differences in participation by survey year. Finally, to calculate the adjusted means for the six different dimensions, as well as for the overall HRQoL score by the month of data collection, multivariate linear regression models with the domain-specific and month-specific HRQoL respectively as the dependent variable and the survey year and month respectively as the independent variables were run, adjusting for all characteristics showing significant associations with the HRQoL score. The few missing values, which occurred in sociodemographic variables, were each replaced by an own category value in order not to lose power. A transformation of the HRQoL score was not necessary as the residuals were normally distributed and all assumptions of linear regressions were met. Because of an oversampling of Italian-speaking children, a sensitivity analysis using weights for language area was conducted. The weights were based on the proportions according to the Federal Statistical Office and introduced separately for each survey year. A second sensitivity analysis was done excluding children with missing values. All analyses were performed using STATA 15.1. The level of statistical significance was set at p ≤0.05.
Results
Of the contacted families, 799 (35.6% of valid addresses) filled in the proxy questionnaire about children’s HRQoL in 2014/15 and 913 (33.1% of valid addresses) in 2020, resulting in a total sample of 1,712 children. In 2020, the mean age was significantly younger and more parents from the Italian-speaking part filled in a questionnaire, while in 2014/15 more parents did not want to disclose their income (table 1). For all other sample characteristics, no significant difference by SOPHYA wave was found.
Table 1Characteristics of the participants of the two repeated cross-sectional surveys.
|
SOPHYA1 survey 2014/15
a
|
SOPHYA2 survey 2020
a
|
| Total |
n (%) |
799 (46.7%) |
912 (53.3%) |
| Age |
5–7 years |
168 (21.0%) |
487 (53.3%) |
| 8–9 years |
360 (45.1%) |
370 (40.6%) |
| 10–11 years |
271 (33.9%) |
55 (6.0%)* |
| Sex |
Boys |
405 (50.7%) |
492 (54.0%) |
| Girls |
394 (49.3%) |
417 (45.7%) |
| Other |
No option in 2014 |
3 (0.2%) |
| Parental education
|
Low |
30 (3.8%) |
28 (3.1%) |
| Medium |
415 (51.9%) |
427 (46.8%) |
| High |
350 (43.8%) |
438 (48.0%) |
| No information |
2 (0.5%) |
19 (2.1%) |
| Income |
<6000 CHF/month |
155 (19.4%) |
137 (15.0%) |
| 6001-9000 CHF/month |
233 (29.1%) |
336 (36.8%) |
| >9000 CHF/month |
314 (39.3%) |
389 (42.7%) |
| No information |
97 (12.1%) |
50 (5.55)* |
| Nationality |
Swiss |
531 (66.5%) |
569 (62.4%) |
| Foreign nation |
91 (11.4%) |
112 (12.3%) |
| Dual citizen |
177 (22.2%) |
212 (23.3%) |
| No information |
0 (0.0%) |
19 (2.1%) |
| Language region |
German-speaking |
552 (69.1%) |
490 (53.7%) |
| French-speaking |
166 (20.85) |
227 (24.9%) |
| Italian-speaking |
81 (10.15) |
195 (21.4%)* |
| Urbanicity |
Urban area |
168 (21.0%) |
223 (24.5%) |
| Agglomeration |
363 (45.4%) |
421 (46.3%) |
| Rural area |
268 (33.5%) |
267 (29.4%) |
Supplementary Table 1 shows that the HRQoL score was significantly associated with several sample characteristics. HRQoL decreased with age and increased with household income. Girls, those living in the French-speaking areas and those from rural areas achieved statistically significantly lower scores.
Analyses on differences in the mean HRQoL scores between the survey periods in 2014/15 and 2020 were adjusted for factors associated with differential participation between surveys and for factors associated with HRQoL. Results are presented for both unadjusted and adjusted analyses (Table 2). Irrespective of adjustment, mean HRQoL was lower in the total study sample and in the subgroups during the survey period that coincided with the pandemic when compared to 2014/15. Most of the associations between mean HRQoL and the survey year by characteristic reached statistical significance, particularly in the adjusted analyses. The biggest decrease between 2014/15 and 2020 in the adjusted models was seen for the youngest age group (–3.9 points), followed by children from families with a high income (–3.2 points), girls (–3.1 points), Swiss citizens (–3.1 points) and German-speaking children (–3.1 points). Sensitivity analyses using weights for language areas or excluding children with missing values confirmed all results except for low-income households, where the difference between the survey years also reached statistical significance if weights for language areas were used.
Table 2Comparison of mean health-related quality of life (HRQoL) scores in 2014/15 versus 2020 (year of COVID-19 pandemic) according to socioeconomic subgroup.
|
Characteristic
|
Subgroup
|
Unadjusted mean HRQoL score (95% confidence interval)
|
Adjusted
a
mean HRQoL score (95% confidence interval)
|
|
|
SOPHYA1 2014/5
|
SOPHYA2 2020
|
p-value
|
SOPHYA1 2014/5
|
SOPHYA2 2020
|
p-value
|
| Total |
|
81.7 (81.1; 82.3) |
80.3 (79.7; 80.8) |
<0.001 |
82.4 (81.8; 83.0) |
79.6 (79.1; 80.2) |
<0.001 |
| Age |
5–7 years |
84.5 (83.4; 85.6) |
81.3 (80.6; 81.9) |
<0.001 |
85.0 (83.7; 86,2) |
81.1 (80.4; 81.8) |
<0.001 |
| 8–9 years |
81.2 (80.3; 82.0) |
79.0 (78,2; 79.8) |
<0.001 |
81.2 (80.3; 82.1) |
79.0 (78,1; 79.8) |
<0.001 |
| 10–11 years |
80.7 (79.6; 81.8) |
79.8 (77.4; 82.2) |
0.5 |
81.0 (79.9; 82.0) |
78.6 (76.1; 81.1) |
0.09 |
| Sex |
Boys |
81.1 (80.3; 81.9) |
80.0 (79.3; 80.8) |
0.005 |
81.9 (81.0; 82.7) |
79.4 (78.6; 80.1) |
<0.001 |
| Girls |
82.4 (81.5; 83.2) |
80.5 (79,8; 81.4) |
0.002 |
83.0 (82.1; 83.8) |
80.0 (79,1; 80.9) |
<0.001 |
| Parental education |
Low to medium |
81.6 (80.8; 82.4) |
80.2 (79.5; 81.0) |
0.001 |
82.0 (81.2; 82.8) |
79.8 (79.0; 80.7) |
0.001 |
|
High |
81.9 (81.0; 82.8) |
80.3 (79.5; 81.1) |
0.001 |
82.8 (81.9; 83.7) |
79.6 (78.7; 80.4) |
<0.001 |
| Income |
<6000 CHF/month |
79.8 (78.4; 81.2) |
79.5 (78.0; 81.0) |
0.7 |
80.7 (79.1; 82.2) |
78.5 (76.8; 80.2) |
0.1 |
| 6001-9000 CHF/month |
81.5 (80.4; 82.6) |
80.0 (79.1; 81.0) |
0.05 |
82.4 (81.2; 83.6) |
79.4 (78.5; 80.4) |
<0.001 |
| >9000 CHF/month |
82.6 (81.8; 83.5) |
80.9 (80.1; 81.6) |
0.03 |
83.1 (82.3; 84.0) |
80.5 (79.7; 81.20) |
<0.001 |
| Language region |
German-speaking |
82.4 (81.7; 83.0) |
80.2 (79.5; 80.9) |
<0.001 |
82.8 (82.1; 83.5) |
79.7 (79.0; 80.5) |
<0.001 |
| French-speaking |
79.1 (77.8; 80.4) |
79.3 (78,2; 80.4) |
0.9 |
80.3 (78.9; 81.6) |
78.5 (77.3; 79.6) |
0.07 |
| Italian-speaking |
82.6 (80.7; 84.5) |
81.5 (80.3; 82.8) |
0.4 |
83.2 (81.2; 85.3) |
81.3 (80.0; 82.5) |
0.1 |
| Nationality |
Swiss |
82.1 (81.4; 82.8) |
80.2 (79.5; 80.9) |
<0.001 |
82.8 (82.0; 83.5) |
79.6 (78.9; 80.3) |
<0.001 |
| Foreign nation |
80.9 (79.3; 82.5) |
79.8 (78.3; 81.2) |
0.3 |
81.0 (79.3; 82.8) |
79.6 (78.1; 81.2) |
0.3 |
| Dual citizen |
81.0 (79.7; 82.2) |
80.8 (79.6; 82.0) |
0.9 |
81.8 (80.4; 83.2) |
80.1 (78.9; 81.4) |
0.1 |
| Urbanicity |
Urban |
82.1 (80.9; 83.3) |
80.3 (79.3; 81.4) |
0.03 |
82.7 (81.4; 84.0) |
79.9 (78.8; 81.0) |
0.003 |
| Agglomeration |
82.3 (81.4; 83.1) |
80.7 (79.9; 81.5) |
0.007 |
82.8 (81.9; 83.7) |
80.3 (79.5; 81.1) |
<0.001 |
| Rural area |
80.7 (79.7; 81.8) |
79.5 (78,4; 80.5) |
0.1 |
81.5 (80.4; 82.6) |
78.7 (77.6; 79.8) |
0.001 |
Figure 1 presents the change in the mean HRQoL scores between the two survey periods by HRQoL dimension. The largest decrease was seen for “emotional well-being”, followed by “family” and “school”. The smallest decline, and the only one which was not statistically significant, was observed in the “friends” dimension.
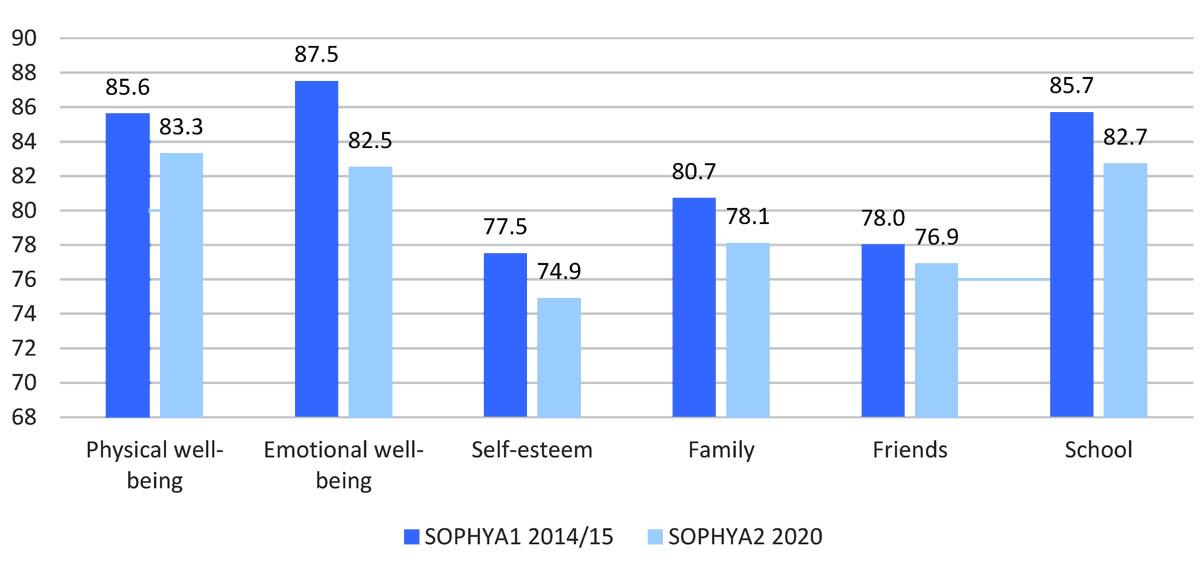
Figure 1 Comparison of adjusteda means for the different dimensions of health-related quality of life in 2014 versus 2020 (year of the COVID-19 pandemic).
a Multivariate linear regression models adjusted for all characteristics which showed a significant association with health-related quality of life (supplementary Table 1): age, sex, income, language region and urbanicity.
The scores of the different dimensions were between 1 and 100. The axis scale was based on the span of the interquartile ranges of the scores.
* p<0.05
Figure 2 compares the mean monthly HRQoL scores by survey period. While the monthly means were quite stable over the years 2014/15, the scores fluctuated more in 2020 and were lowest in April 2020, coinciding with the first COVID wave and school closures, and in December 2020 and early 2021, at the peak of the second COVID wave and at the start of stronger restrictions in Switzerland.

Figure 2 Adjusteda monthly means of health-related quality of life, by survey year.
a Multivariate linear regression models adjusted for all characteristics which showed a significant association with health-related quality of life (supplementary Table1): age, sex, income, language region and urbanicity.
Lockdown one, during the first COVID wave from 16th March 2020 to 11th May 2020. The lockdown included the closure of schools, shops (except groceries and pharmacies), sports and cultural facilities, hospitality, and zoos.
Lockdown two, during the second COVID wave from December 2020 to the end of the data collection in February 2021. The lockdown included the closure of sports and cultural facilities, hospitality and zoos and limits for group sizes (e.g. a maximum of 5 people for sport during leisure time or 10 people at Christmas). Schools remained open.
The axis scale was based on the span of the interquartile ranges for the scores.
Discussion
To our knowledge, this is the first study testing the effect of COVID-19 and of restrictions related to the pandemic on HRQoL in a representative sample of children aged 5 to 11 over the course of one year. In this population-based, repeated cross-sectional study of primary school children in Switzerland, we found that the overall and dimension-specific HRQoL scores, and in particular the emotional well-being scores, were lower during the year of the pandemic (2020) compared to the survey year 2014/15. The fact that HRQoL in 2020 was particularly low during restriction periods, whereas in 2014/15 differences by month were more stable, supports the hypothesis that the pandemic had a negative impact on children’s HRQoL. The differences in HRQoL scores in April and December compared to the neighboring months was even larger than the differences between children with and without asthma or with and without pain in the last three months [24].
Although the overall mean HRQoL score was still above the mean of reference data from Germany (79.0 (78.7–79.3) in 7 to 10-year-old children) [24], it was lower in the total study population and in every subgroup when compared to before the pandemic. This is in line with two previous COVID studies, conducted in 7 to 13-year-olds in Turkey [14] and in 7 to 17-year-olds from Germany [4] using the same or a comparable instrument [29], and a systematic review about HRQoL in the context of the COVID-19 pandemic [30]. Our observation that the relative decrease was largest in the youngest age group is in line with previous findings [4, 15]. However, the current study did not confirm findings from the above-mentioned German survey by Ravens-Sieberer, where HRQoL decreased most in socioeconomically disadvantaged children and in children with a migration background [4]. Instead, preexisting differences in HRQoL according to sociodemographic factors in the SOPHYA sample became smaller during the pandemic and the decrease in HRQoL was larger and statistically more significant in socioeconomically advantaged children. On the one hand, in families with children at such a young age, the impact of lockdown-related problems may have been more pronounced than the socioeconomic difficulties per se. Working from home during school closures has been reported to be a burden for families with young children [22], and home working was possibly more prevalent in highly educated parents. However, information on home schooling and home working was not assessed in the present survey. On the other hand, the restrictions in Switzerland were less drastic than in most other countries (no curfew, only eight weeks of school closure). Being constrained to a limited living space, which is more common in families with lower household incomes, may have had less of an impact on family stress than in other countries. In fact, the large but not population-representative Swiss Corona Stress Study in adolescents and adults also did not find a significant difference in the prevalence of moderate to severe depressive symptoms by education level [15]. Moreover, a qualitative study from Switzerland in families with young children found that well-being in families during the COVID-19 pandemic was independent of their socioeconomic position, but was influenced by the amount of social support, the flexibility of employers and whether home working and home schooling had to be managed at the same time [22].
Consistent with the Swiss Corona Stress Study, which found that people in the French-speaking part of Switzerland experienced more depressive symptoms compared to those from the German-speaking part [15], HRQoL in the SOPHYA-study was also lowest in the French-speaking part. However, this was pre-existent in 2014/15 and the pandemic did not lead to a further increase, but rather a decrease in the regional differences in HRQoL. Before the pandemic, protective factors for mental health [31, 32] were more prevalent in the German-speaking part: German-speaking children were significantly more physically active [33] and spent more time playing outdoors [34]. These protective factors were at least partly reduced by the pandemic restrictions in 2020 (no sports training in clubs, no active commuting to school during school closures, maximum group sizes, recommendations to stay at home and to reduce social interactions) in all language regions.
Among the individual HRQoL dimensions, emotional well-being was most affected, followed by the school- and family-related HRQoL domains. These dimensions have previously been associated with COVID-19 related conflicts or stress [4, 5, 7, 14]. An impact on the “friends” dimension score would be expected as a result of fewer opportunities for social interaction. But it is important to point out that the questionnaire focuses on whether the child feels different from others or whether the child is accepted, rather than on the intensity of social interactions. The quality of interactions may actually improve for some children if social groups are smaller and more selective.
There are some limitations to this study which must be acknowledged. First, the study was cross-sectional, making it impossible to draw any causal conclusion. Regarding the increased fluctuation of HRQoL scores in 2020 and its alignment with periods of more intense restrictions, it is not clear whether the restrictions or the fear of COVID-19 itself were the main driver for lower HRQoL, as both are time-correlated. The influence on mental health of both has been described in the literature [4, 11, 15]. Second, the participation rate was satisfactory for this type of recruitment but selection bias cannot be excluded. Specifically, fewer children of parents with low education seem to have participated in the survey, which could limit the generalizability of the findings. However, there is no evidence that this selection was very different between the SOPHYA waves and the analyses were adjusted for sociodemographic factors affecting participation or HRQoL. Finally, information on the HRQoL of children was obtained using parents as proxies. Parents’ own HRQoL may have influenced their perception and reporting of their child’s HRQoL. However, a correlation between the HRQoL of parents and their children has also been observed in studies in the absence of proxy reports [21]. Among the strengths of the study are its large sample size, its use of a validated and internationally used questionnaire to assess HRQoL, that it gathered data over a full year to allow testing of differences in HRQoL by month in parallel to the COVID-19 situation, and its recruitment using registry data to avoid clusters of participants.
Conclusion
The SOPHYA-study showed that HRQoL, and especially emotional well-being, was lower in 5 to 11-year-old children in Switzerland during the first year of the pandemic compared to results from a survey conducted in 2014/15. In the first year of the pandemic, the score was lowest at the height of the COVID waves and the related restrictions imposed in parallel by the government to address the threat. It cannot be determined whether fear of the disease itself or the restrictions caused this decrease in HRQoL. Therefore, containment policies should keep COVID-19 infections as low as possible, but still enable children to profit from protective factors such as leisure activities, physical activity and social contact. This includes avoiding the closure of schools. In addition, parents should be supported if they feel stressed, as parents’ and children’s stress are intertwined. Consequently, low threshold contact points providing psychosocial support should be available for both children and their parents. Finally, more research is needed to better understand the factors contributing to the decrease in HRQoL and to investigate whether or not HRQoL recovers to pre-pandemic levels.
Acknowledgments
We thank the SOPHYA-Study Group and Emmanuel Schaffener for their support, the fieldworkers for the data collection and all the children and parents participating in the SOPHYA-study.
The SOPHYA-Study Group: Nadja Mahler (FOSPO), Urs Mäder (FOSPO), Thomas Wyss (FOSPO), Andrea Poffet (FOPH), Lisa Guggenbühl (Health Promotion Switzerland) and Simone Isler (Swiss TPH)
1.
Castagnoli R
,
Votto M
,
Licari A
,
Brambilla I
,
Bruno R
,
Perlini S
, et al.
Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents: A Systematic Review. JAMA Pediatr. 2020 Sep;174(9):882–9. https://doi.org/10.1001/jamapediatrics.2020.1467
2.
Green KH
,
van de Groep S
,
Sweijen SW
,
Becht AI
,
Buijzen M
,
de Leeuw RN
, et al.
Mood and emotional reactivity of adolescents during the COVID-19 pandemic: short-term and long-term effects and the impact of social and socioeconomic stressors. Sci Rep. 2021 Jun;11(1):11563. https://doi.org/10.1038/s41598-021-90851-x
3.
Orben A
,
Tomova L
,
Blakemore SJ
. The effects of social deprivation on adolescent development and mental health. Lancet Child Adolesc Health. 2020 Aug;4(8):634–40. https://doi.org/10.1016/S2352-4642(20)30186-3
4.
Ravens-Sieberer U
,
Kaman A
,
Erhart M
,
Devine J
,
Schlack R
,
Otto C
. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur Child Adolesc Psychiatry. 2021 Jan.
5.
United Nations
. Policy Brief: The Impact of COVID-19 on Children. 15. April 2020.
6.
OECD
. Combatting COVID-19's effect on children. 2020.
7.
UNICEF
. UNICEF (2020) COVID-19: children at heightened risk of abuse, neglect, exploitation and violence amidst intensifying containment measures. 2020 [Available from: https://www.unicef.org/guineabissau/press-releases/covid-19-children-heightened-risk-abuse-neglect-exploitation-and-violence-amidst
8.
Nearchou F
,
Flinn C
,
Niland R
,
Subramaniam SS
,
Hennessy E
. Exploring the Impact of COVID-19 on Mental Health Outcomes in Children and Adolescents: A Systematic Review. Int J Environ Res Public Health. 2020 Nov;17(22):E8479. https://doi.org/10.3390/ijerph17228479
9.
Fancourt D
,
Steptoe A
,
Bu F
. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. Lancet Psychiatry. 2021 Feb;8(2):141–9. https://doi.org/10.1016/S2215-0366(20)30482-X
10.
Orgilés M
,
Morales A
,
Delvecchio E
,
Mazzeschi C
,
Espada JP
. Immediate Psychological Effects of the COVID-19 Quarantine in Youth From Italy and Spain. Front Psychol. 2020 Nov;11:579038. https://doi.org/10.3389/fpsyg.2020.579038
11.
Jiao WY
,
Wang LN
,
Liu J
,
Fang SF
,
Jiao FY
,
Pettoello-Mantovani M
, et al.
Behavioral and Emotional Disorders in Children during the COVID-19 Epidemic. J Pediatr. 2020 Jun;221:264–266.e1. https://doi.org/10.1016/j.jpeds.2020.03.013
12.
Saurabh K
,
Ranjan S
. Compliance and Psychological Impact of Quarantine in Children and Adolescents due to Covid-19 Pandemic. Indian J Pediatr. 2020 Jul;87(7):532–6. https://doi.org/10.1007/s12098-020-03347-3
13.
Uccella S
,
De Grandis E
,
De Carli F
,
D’Apruzzo M
,
Siri L
,
Preiti D
, et al.
Impact of the COVID-19 Outbreak on the Behavior of Families in Italy: A Focus on Children and Adolescents. Front Public Health. 2021 Feb;9:608358. https://doi.org/10.3389/fpubh.2021.608358
14.
Adıbelli D
,
Sümen A
. The effect of the coronavirus (COVID-19) pandemic on health-related quality of life in children. Child Youth Serv Rev. 2020 Dec;119:105595. https://doi.org/10.1016/j.childyouth.2020.105595
15.
de Quervain D
,
Aerni A
,
Amin E
,
Bentz D
,
Coynel D
,
Gerhards C
, et al.
The Swiss Corona Stress Study: second pandemic wave, November 2020 Basel: OSFPreprints; 2020 [Available from: https://osf.io/jqw6a/
16.
Ravens-Sieberer U
,
Kaman A
,
Otto C
,
Adedeji A
,
Napp AK
,
Becker M
, et al.
[Mental health and psychological burden of children and adolescents during the first wave of the COVID-19 pandemic-results of the COPSY study]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2021.
17.
Kwong AS
,
López-López JA
,
Hammerton G
,
Manley D
,
Timpson NJ
,
Leckie G
, et al.
Genetic and Environmental Risk Factors Associated With Trajectories of Depression Symptoms From Adolescence to Young Adulthood. JAMA Netw Open. 2019 Jun;2(6):e196587. https://doi.org/10.1001/jamanetworkopen.2019.6587
18.
Campion J
,
Javed A
,
Sartorius N
,
Marmot M
. Addressing the public mental health challenge of COVID-19. Lancet Psychiatry. 2020 Aug;7(8):657–9. https://doi.org/10.1016/S2215-0366(20)30240-6
19.
Mazza C
,
Ricci E
,
Biondi S
,
Colasanti M
,
Ferracuti S
,
Napoli C
, et al.
A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int J Environ Res Public Health. 2020 May;17(9):E3165. https://doi.org/10.3390/ijerph17093165
20.
Gassman-Pines A
,
Ananat EO
,
Fitz-Henley J 2nd
. COVID-19 and Parent-Child Psychological Well-being. Pediatrics. 2020 Oct;146(4):e2020007294. https://doi.org/10.1542/peds.2020-007294
21.
Patrick SW
,
Henkhaus LE
,
Zickafoose JS
,
Lovell K
,
Halvorson A
,
Loch S
, et al.
Well-being of Parents and Children During the COVID-19 Pandemic: A National Survey. Pediatrics. 2020 Oct;146(4):e2020016824. https://doi.org/10.1542/peds.2020-016824
22.
Lannen P
,
Sticca F
,
Simoni H.
Kleinkinder und ihre Eltern während der Covid-19 Pande-mie2020 28.04,2021.
23.
Bringolf-Isler B
,
Schindler C
,
de Hoogh K
,
Kayser B
,
Suggs LS
,
Dössegger A
, et al.; SOPHYA Study Group
. Association of objectively measured and perceived environment with accelerometer-based physical activity and cycling: a Swiss population-based cross-sectional study of children. Int J Public Health. 2019 May;64(4):499–510. https://doi.org/10.1007/s00038-019-01206-3
24.
Ravens-Sieberer U
,
Ellert U
,
Erhart M.
Gesundheitsbezogene Lebensqualität von Kindern und Jugendlichen in Deutschland. Eine Normstichprobe für Deutschland aus dem Kinder- und Jugendgesundheitssurvey (KIGGS). Bundesgesundheitsbl - Gesundheitsforsch -Gesundheitsschutz. 2007;50:810-8.
25.
Ravens-Sieberer U
,
Bullinger M
. KINDL-R Questionnaires, Language versions: https://www.kindl.org/english/language-versions/ 1998 [
26.
Ravens-Sieberer U
,
Bullinger M
. KINDL-R, Fragebogen zur Erfassung der gesundheitsbezogenen Lebensqualität bei Kindern und Jugendlichen. Revidierte Form. Manual.; 2000.
27.
Bundeamt für Statistik
. Raum mit städtischem Charakter der Schweiz 2012. Eine neue Definition der Agglomerationen und weiteren stadtischen Raumkategorien.; 2014.
28.
Bundesamt für Statistik
. Räumliche Gliederung. https://www.bfs.admin.ch/bfs/de/home/grundlagen/raumgliederungen.html [
29.
Bullinger M
,
Brütt AL
,
Erhart M
,
Ravens-Sieberer U
,
Group BS
; BELLA Study Group
. Psychometric properties of the KINDL-R questionnaire: results of the BELLA study. Eur Child Adolesc Psychiatry. 2008 Dec;17(S1 Suppl 1):125–32. https://doi.org/10.1007/s00787-008-1014-z
30.
Nobari H
,
Fashi M
,
Eskandari A
,
Villafaina S
,
Murillo-Garcia Á
,
Pérez-Gómez J
. Effect of COVID-19 on Health-Related Quality of Life in Adolescents and Children: A Systematic Review. Int J Environ Res Public Health. 2021 Apr;18(9):4563. https://doi.org/10.3390/ijerph18094563
31.
Chtourou H
,
Trabelsi K
,
H’mida C
,
Boukhris O
,
Glenn JM
,
Brach M
, et al.
Staying Physically Active During the Quarantine and Self-Isolation Period for Controlling and Mitigating the COVID-19 Pandemic: A Systematic Overview of the Literature. Front Psychol. 2020 Aug;11:1708. https://doi.org/10.3389/fpsyg.2020.01708
Edifix has not found an issue number in the journal reference. Please check the volume/issue information. (Ref. 31 "Chtourou, Trabelsi, 2020")
32.
Jiménez-Pavón D
,
Carbonell-Baeza A
,
Lavie CJ
. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: special focus in older people. Prog Cardiovasc Dis. 2020 May - Jun;63(3):386–8. https://doi.org/10.1016/j.pcad.2020.03.009
33.
Bringolf-Isler B
,
Mäder U
,
Dössegger A
,
Hofmann H
,
Puder JJ
,
Braun-Fahrländer C
, et al.
Regional differences of physical activity and sedentary behaviour in Swiss children are not explained by socio-demographics or the built environment. Int J Public Health. 2015 Mar;60(3):291–300. https://doi.org/10.1007/s00038-014-0645-8
34.
Bringolf-Isler B
,
Grize L
,
Mäder U
,
Ruch N
,
Sennhauser FH
,
Braun-Fahrländer C
; SCARPOL team
. Built environment, parents’ perception, and children’s vigorous outdoor play. Prev Med. 2010 May-Jun;50(5-6):251–6. https://doi.org/10.1016/j.ypmed.2010.03.008
Appendix
Supplementary Table 1Association of health-related quality of life with sample characteristics (n = 1,712a).
|
|
Adjustedb health-related quality of lifecoefficient(95% confidence interval) |
| Age |
5–7 years (ref.) |
1 (reference) |
| 8–9 years |
–2.6 (–3.5; –1.7)* |
| 10–11 years |
–2.9 (–4.1; –1.7)* |
| Sex |
Boys (ref.) |
1 |
| Girls |
–1.4 (–2.2; -0.6)* |
| Parental education |
Low to medium (ref.) |
1 |
| High |
0.2 (–0.6; 1.0) |
| No indication |
0.4 (–3.1; 3.8) |
| Income |
<6000 CHF/month (ref.) |
1 |
| 6001–9000 CHF/month |
1.2 (0.0; 2.3)* |
| >9000 CHF/month |
2.1 (1.0; 3.3)* |
| No indication |
1.5 (–0.2; 3.1) |
| Language region |
German-speaking (ref.) |
1 |
| French-speaking |
–2.0 (–2.9; –1.0)* |
| Italian-speaking |
0.8 (–0.3; 2.0) |
| Nationality |
Swiss (ref.) |
1 |
| Foreign nation |
–0.8 (–2.0; 0.4) |
| Dual citizen |
–0.2 (–1.1; 0.8) |
| No indication |
–0.9 (–4.7; 2.9) |
| Urbanicity |
Urban area (ref.) |
1 |
| Agglomeration |
0.3 (–0.7; 1.3) |
| Rural area |
–1.1 (–2.2; 0.0)* |