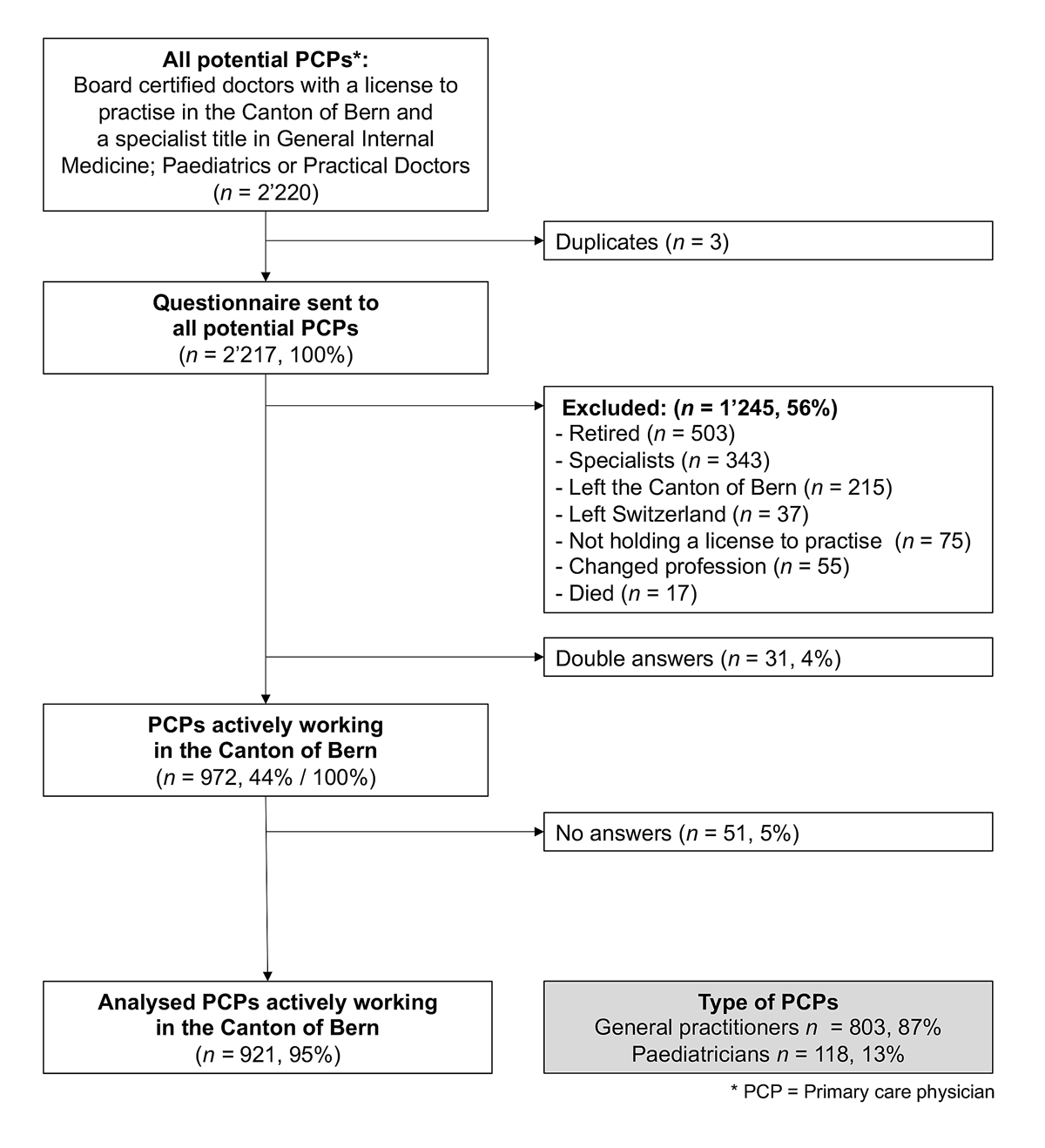
Figre 1 Study flow chart.
DOI: https://doi.org/10.4414/SMW.2021.w30024
Berner Institut für Hausarztmedizin (Institute of Primary Health Care Bern)
Aerztegesellschaft des Kantons Bern (Medical Society of the Canton of Bern)
Confidence Interval
Swiss Medical Association
Full-time equivalent
General practitioner
Global location number
Berner Stiftung zur Förderung der Hausarzt-Medizin (Bern Foundation to Support Primary Care)
Haus- und Kinderärzte Schweiz (Association of Swiss General Practitioners and Pediatricians)
Medizinalberuferegister (Register of medical professions)
Schweizerisches Gesundheitsobservatorium (Swiss Health Observatory)
Primary care physician
Standard Deviation
Universitäres Notfallzentrum, Inselspital Bern (Department of Emergency Medicine, University Hospital of Bern)
Verein Berner Haus- und Kinderärzte (Society of Family Doctors and Pediatricians in Bern)
Several studies have shown that there is a shortage of primary care physicians (PCPs) in Switzerland [1–4]. In their latest survey in 2020, the association of Swiss General Practitioners and Paediatricians (mfe) asked their members if they felt that there was a shortage of PCPs in their region, and concluded that the most affected region was the one including the second largest canton (i.e. federal state) of Bern, with 72% [5].
However, workforce studies have been facing well known challenges [4]: (1) surveys on PCPs often have low participation rates (e.g., 38% in the mfe-study [5] ), and therefore generalisability is often questioned; (2) neither a membership of the mfe nor the Swiss Medical Association (FMH) is mandatory, and therefore surveys might fail to include some PCPs; (3) the FMH has a large membership database and regularly publishes its annual report, but in 2020 52% of all physicians did not actively update their characteristics through its platform myFMH [6]; (4) although Switzerland has a registry for all physicians holding a professional license (Medizinalberuferegister, MedReg), general practitioners (GPs) and hospital physicians share the same board certification (FMH General Internal Medicine). Therefore, it is challenging to define which board-certified specialist is working as a PCP and which is working in a hospital. In addition, foreign PCPs (37.5% of all physicians in Switzerland in 2020 [6]) often receive the title of “Praktischer Arzt (practical doctor)” (in 2020 n = 1597) [6].
Thus, the current estimates on the workforce of PCPs might either be correct or biased through selection (surveys), missing information (less frequent updates in myFMH), or under- or overestimated due to systematic problems in registries (MedReg).
Therefore, the aim of this study was to invest all resources that were needed to (1) conduct a full count of all PCPs in the Canton of Bern and to describe their characteristics, (2) to calculate the density of full-time-equivalent (FTE) PCPs per 1000 inhabitants for the whole of the Canton of Bern and for each of its 10 administrative districts, and (3) to forecast workforce development for the next 5years, based on different scenarios for new domestic and foreign PCPs.
We conducted a cross-sectional study using several sequential methods to determine the workforce of PCPs in the Canton of Bern. Data collection lasted from November 2019 to June 2020.
The Ethics Committee of the Canton of Bern issued a waiver of non-responsibility (Req-2019-00383) for this study. No participant received a financial incentive to participate and all of them agreed to the data protection declaration that was developed with the legal office of the University of Bern and with the knowledge and approval of the Data Protection Supervisory Board of the canton of Bern. The content of this policy was compliant with the data protection act of Switzerland. Participants gave consent to participate by accepting the terms before completing our survey on paper or online.
To identify our study population, we used the following inclusion criteria: board certification in general internal medicine, paediatrics or “Praktischer Arzt” and holding a professional license in the Canton of Bern. We applied these criteria in MedReg to identify all potential PCPs, removed duplicates using names and GLN (i.e. a unique identifier of all physicians issued by the government), and cross-checked this list from MedReg with FMH membership data to exclude retired PCPs or PCPs who had previously moved outside of Bern. All potential PCPs received a letter with a paper-based questionnaire and the possibility to use an online-based questionnaire. However, when letters were returned by the postal service, they also mentioned the reason for returning the mail such as migration from Switzerland or death. This allowed us to confidently exclude these individuals from the list of active PCPs. For those returned due to an invalid address, we used the subjects’ MedReg data (names, GLN, last working place) to find a new postal address, email address, or phone number and then sent up to three reminders. All non-responders were then contacted by phone, social media, email, or through their practice assistant, with repeated attempts until the respective person had been identified and was willing to participate. To increase response rate, a short version of the survey was offered to (a) confirm that they are an active PCP or not and (b) to declare their workload (in half-days or percent). We also cross-checked our non-responders with the membership data from the Medical Society of the Canton of Bern (BEKAG), which allowed us to reliably eliminate PCPs from our list, who (a) were e.g. retired or (b) working as e.g. specialist in an hospital. Through this process, we established categories of physicians not working as active PCPs, who were excluded: those in retirement, specialists (working in hospitals), physicians working in another canton or who had left Switzerland, PCPs without a professional license to practice, or with a professional license that was inactive or withdrawn, or PCPs who had died. All data were exported, entered and validated in LimeSurvey (LimeSurvey GmbH, Hamburg, Germany) and analyzed in STATA 15.1 (StataCorp, College Station, TX, USA).
We designed a questionnaire with two parts. The first part was prefilled with data from the publicly available MedReg: name, sex, year and country of diploma, board certification, workplace. Physicians participating in the survey were asked if these data were correct. Physicians who confirmed that they were active PCPs then continued to the second part of the questionnaire, which contained questions about: age, current workload (measured both in half-days and percent) and planned workload changes during the next 5 years (unchanged, de-/increase, or retirement), type of practice (single, group, other), employment (self-employed or employed), region of work (using their zip code that we allocated to their administrative district [7] and whether they accepted new patients (yes, fully; yes, partly; no). They were also asked if they felt there was a shortage of PCPs (yes of GPs, yes of paediatricians, no shortage, unknown) in their region of work.
The questions in part 2 were developed by the project group, which incorporated different stakeholders and academics with extensive experience in workforce estimations for Switzerland and the Canton of Bern. The survey was piloted on PCP colleagues in order to check for readability and length. The final paper questionnaire was sent in German, but physicians could also access a French version online (www.workforce-bern.ch).
We used descriptive statistics presenting proportions, 95% confidence intervals (CIs), means, and standard deviation (SD) for normally distributed data where appropriate. To compare characteristics of GPs and paediatricians, we calculated column percentages and used t-tests and chi-square tests. We handled missing data by excluding them. Table 2 displays the proportion of missing data per variable. In general, no values were missing from the MedReg data. We defined 1 FTE as 10 half-days per week. To calculate density, we calculated FTEs per 1000 inhabitants using STATPOP-Data from 2018 (closest data set available to 2020) [8] and predictions for 2025 [9]. To best inform our scenarios of new PCPs needed by 2025, we had to calculate how many medical students in Switzerland would decide to work in the Canton of Bern. Since there are no data or models available, we decided to use this pragmatic assumption that the proportion of past medical students (i.e., currently active PCPs) choosing to work/live in the Canton of Bern would be identical in the future. We found 972 PCPs (12%) working in the Canton of Bern from the approximately 8000 PCPs working in Switzerland [10]). With 1100 medical students currently graduating [11], we hypothesised that an identical share (12%) annually would decide to later work as physicians in the Canton of Bern and are therefore potentially available to become PCPs for the Canton of Bern in the future.
Out of 2217 potential PCPs in MedReg, we eventually excluded 1245 (56%) in accordance with our exclusion criteria, primarily because of retirement, specialisation and change of canton (fig. 1). We identified 972 active PCPs. All but 51 (5%) PCPs participated by returning the paper-based or online questionnaire, or by phone.
Figre 1 Study flow chart.
Table 1 describes their personal characteristics: 851 (88%) were GPs and 121 (12%) paediatricians. GPs on average were older (53 years, SD 10.3) than paediatricians (50 years, SD 10.4, p <0.001). More GPs were still working at age 65 and older (14.1%) than paediatricians (7.4%, p = 0.043). GPs were mainly male (61%) and paediatricians female (71%, p <0.001). Almost 20% of the PCP workforce was foreign PCPs, with no significant difference between GPs and paediatricians (p = 0.39). Less than half of all PCPs (45.3%) worked in the largest administrative district of Bern-Mittelland, which includes the capital of Switzerland (table 1).
Table 1 Personal characteristics of primary care physicians in the Canton of Bern in 2020.
| Personal characteristics | All | General practitioners | Paediatricians | p-value | |
| (n = 972) | (n = 851, 87.6%) | (n = 121, 12.4%) | |||
| Age (years), mean (SD) | 52.6 (10.4) | 53.1 (10.3) | 49.6 (10.4) | <0.001 | |
| Age ≥65, n (%) | Yes | 129 (13.3) | 120 (14.1) | 9 (7.4) | 0.043 |
| No | 843 (86.7) | 731 (85.9) | 112 (92.6) | ||
| Sex, n (%) | Female | 415 (42.7) | 329 (38.7) | 86 (71.1) | <0.001 |
| Male | 557 (57.3) | 522 (61.3) | 35 (28.9) | ||
| Origin of medical diploma, n (%) | Switzerland | 783 (80.6) | 682 (80.1) | 101 (83.5) | 0.39 |
| Foreign country | 189 (19.4) | 169 (19.9) | 20 (16.5) | ||
| Administrative district, n (%) | Bern-Mittelland | 440 (45.3) | 377 (44.3) | 63 (52.1) | 0.024 |
| Thun | 116 (11.9) | 106 (12.5) | 10 (8.3) | ||
| Emmental | 99 (10.2) | 83 (9.8) | 16 (13.2) | ||
| Biel/Bienne | 85 (8.7) | 68 (8.0) | 17 (14.1) | ||
| Oberaargau | 64 (6.6) | 61 (7.2) | 3 (2.5) | ||
| Seeland | 48 (4.9) | 44 (5.2) | 4 (3.3) | ||
| Jura bernois | 39 (4.0) | 38 (4.5) | 1 (0.8) | ||
| Interlaken-Oberhasli | 38 (3.9) | 33 (3.9) | 5 (4.1) | ||
| Frutigen-Niedersimmental | 32 (3.3) | 30 (3.5) | 2 (1.7) | ||
| Obersimmental-Saanen | 11 (1.1) | 11 (1.3) | 0 (0) | ||
Table 2 describes the working characteristics of PCPs responding to the questionnaire (n = 921, 95%). The mean workload in half-days per week was 7.6 for GPs and significantly less at6.9 for paediatricians (p = 0.002). Further, female PCPs worked 6.4 and male PCPs 8.3 half-days per week in practice (p <0.001). Most PCPs (63%) worked in group practices, with a trend towards more paediatricians (75%) being in group practices than GPs (61%, p = 0.045). However, the proportion of self-employed PCPs was about 60% in both groups.
Of all PCPs, 13% had completely stopped accepting new patients, 47% reported a partial stop and 40% had no stop in place. Sixty-seven percent of PCPs considered that there was a lack of GPs in their region, with no significant difference between GPs and paediatricians in this respect. On the other hand, more paediatricians (79%) considered there to be a lack of pediatricians than did GPs (60%, p = 0.004). Only 6% of data on workload were missing, but the percentage of missing data for other questions of part two of the questionnaire ranged from 35% to 53%, partially due to the fact that some participants were questioned by telephone and responded to only few questions because of time constraints (table 2).
Table 2Working characteristics as reported in the questionnaire by 921 primary care physicians (95%).
| Working characteristics | Missing data | All | General practitioners | Pediatricians | p-value |
| n (% of 972) | n = 921 | n = 803 (87.2%) | n = 118 (12.8%) | ||
| Workload (half-days/week), mean (SD) | 54 (5.6) | 7.5 (2.3) | 7.6 (2.3) | 6.9 (2.3) | 0.002 |
| – Female, n (%) | 6.4 (2.0) | 6.5 (2.0) | 6.4 (2.0) | ||
| – Male, n (%) | 8.3 (2.2) | 8.3 (2.2) | 8.1 (2.5) | ||
| Practice form, n (%) | 348 (35.8) | 0.045 | |||
| – Single practice | 170 (27.3) | 157 (28.9) | 13 (16.3) | ||
| – Group practice | 394 (63.1) | 334 (61.4) | 60 (75.0) | ||
| – Other | 60 (9.6) | 53 (9.7) | 7 (8.7) | ||
| Employment, n (%) | 342 (35.2) | 0.88 | |||
| – Self-employed | 378 (60.0) | 330 (60.3) | 48 (57.8) | ||
| – Employed | 212 (33.7) | 182 (33.3) | 30 (36.1) | ||
| – Mixed | 40 (6.3) | 35 (6.4) | 5 (6.1) | ||
| Stop to taking on new patients, n (%) | 360 (37.0) | 0.47 | |||
| – Yes, complete stop | 80 (13.1) | 73 (13.7) | 7 (8.9) | ||
| – Yes, partial stop | 287 (46.9) | 247 (46.3) | 40 (50.6) | ||
| – No | 245 (40.0) | 213 (40.0) | 32 (40.5) | ||
| Lack of GPs, n (%) | 428 (44.0) | 0.47 | |||
| – Yes | 365 (67.1) | 323 (66.3) | 42 (73.7) | ||
| – No | 120 (22.1) | 109 (22.4) | 11 (19.3) | ||
| – I don’t know | 59 (10.8) | 55 (11.3) | 4 (7.0) | ||
| Lack of paediatricans, n (%) | 514 (52.9) | 0.004 | |||
| – Yes | 279 (60.9) | 224 (57.7) | 55 (78.6) | ||
| – No | 120 (26.2) | 109 (28.1) | 11 (15.7) | ||
| – I don’t know | 59 (12.9) | 55 (14.2) | 4 (5.7) |
The density of PCPs in FTEs per 1000 inhabitants was 0.75 (95% CI 0.69–0.81) in 2020, with a drop by 0.19 up to 2025 to a density of 0.56 FTEs per 1000 inhabitants (95% CI 0.49–0.62). We found differences in the workforce of PCPs across districts for 2020 ranging from 0.59 (95% CI 0.40–0.79) in Biel and 0.59 (95% CI 0.33–0.85) in Frutigen-Niedersimmental to 0.93 (95% CI 0.65–1.21) in Thun. Although, according to our data, the density of PCPs will decrease in every district between 2020 and 2025, the relative changes in the mean value range widely from 10% (Jura bernois: from 0.68 to 0.61) up to 75% (Obersimmental-Saanen: from 0.67 to 0.17) (table 3).
Table 3Density of primary care physicians (full-time equivalents per 1000 inhabitants) in the Canton of Bern and by administrative district in 2020 and by 2025.
| Year | 2020 (95% CI) | 2025 (95% CI) |
| Total of Canton of Bern | 0.75 (0.69–0.81) | 0.56 (0.49–0.62) |
| By administrative district, sorted by density in 2020: | ||
| Thun | 0.93 (0.65–1.21) | 0.74 (0.43–1.06) |
| Interlaken-Oberhasli | 0.91 (0.67–1.15) | 0.58 (0.35–0.81) |
| Emmental | 0.81 (0.62–1.00) | 0.67 (0.50–0.85) |
| Seeland | 0.81 (0.55–1.08) | 0.55 (0.19–0.91) |
| Oberaargau | 0.75 (0.52–0.98) | 0.48 (0.22–0.74) |
| Bern-Mittelland | 0.72 (0.63–0.80) | 0.54 (0.45–0.63) |
| Jura bernois | 0.68 (0.39–0.97) | 0.61 (0.32–0.89) |
| Obersimmental-Saanen | 0.67 (0.39–0.94) | 0.17 (0.00–0.50) |
| Biel/Bienne | 0.59 (0.40–0.79) | 0.44 (0.21–0.67) |
| Frutigen-Niedersimmental | 0.59 (0.33–0.85) | 0.43 (0.18–0.68) |
To offset this drop of 0.19 PCPs in FTEs per 1000 inhabitants, we calculated the need for new PCPs by 2025 depending on different scenarios. Figure 2 shows how many new PCPs are needed by 2025 to retain the workforce in 2020 and what percentage of medical students would be needed to become PCPs to achieve this number. Each scenario accounts for the number of half-days new PCPs will choose to work (10, 7.5 or 6.5 half-days) and how much support from abroad will be available (migration of 0%, 10% or 20%). The caption to figure 2 provides further explanation.
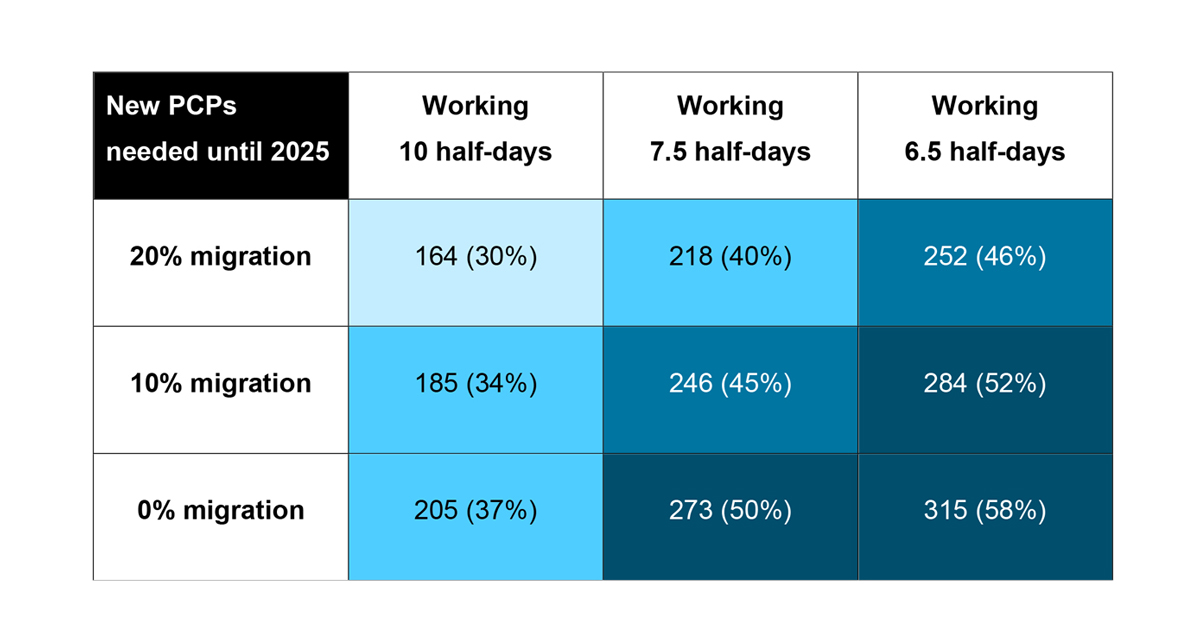
Figure 2 Need for new primary care physicians (PCPs) by 2025 to offset the drop in density between 2020 and 2025 in the Canton of Bern. Percentages in brackets are the estimated proportion of medical students leaving university and working in the Canton of Bern that will need to become PCPs to achieve the needed PCPs. For example, if new PCPs all work 7.5 half-days on average and only 10% of PCPs are from abroad, 246 new PCPs will be needed by 2025 and this means 45% of medical students will need to become PCPs.
In 2020, the workforce of PCPs in the Canton of Bern consisted of 972 individuals (88% GPs, 12% paediatricians), on average 53 years old, 43% female, and with a workload of 7.5 half-days per week. One in eight worked despite being 65 years old or older and one in five came from abroad. The majority were self-employed in group practices. Almost two thirds reported a lack of PCPs in their region, and to be able to cope with this shortage, only 40% reported that they were still taking new patients, whereas the others had a full or partial stop in place. In 2020, 0.75 PCPs (FTEs) were serving 1000 inhabitants with a decline by 25% up to 2025. To offset this drop, the Canton of Bern needs between 164 and 315 new PCPs, depending on different scenarios of workload and migration, which can only be achieved if between 30% and 58% of medical students choose to become PCPs each year. We do not know how many students end up working as PCPs. From a recent study among end-stage medical students, 20% had decided to become GPs and 40% were interested in the field [12]. Only in the best-case scenario, where most of the interested students become GPs too, can we fill the gap.
In the Canton of Bern, a high mean age of PCPs of 52.6 years was noted in our study for both GPs and paediatricians . This is in line with other data from Switzerland [1, 6]. The mfe-study in 2020 showed similar results [1], as did the FMH statistics from 2020, where the average age in the outpatient sector was 54.9 years . This was 10 years more than for hospital physicians, but also included non-PCPs such as specialists in the outpatient sector [2, 6]. An international statistic, the International Health Policy (IHP) survey in 2019, ranked Switzerland third, as one of the countries with the highest average age of PCPs, after France and Germany. The IHP survey noted that in no other country did as many PCPs work over their retirement age as in Switzerland (15%) [2]. In the mfe-study there was an increase from 28% to 49% over the last 5 years in PCPs planning to work over the retirement age . In 2020 they found that15% of GPs and 5% of paediatricians worked at or over the retirement age. In our study 13.3% of PCPs were still working at or over the retirement age.
We found an overall workload of 7.5 half-days. This can be compared to results of the mfe study , which recorded data from PCPs from all over Switzerland, and where the average workload for PCPs in Bern was 7.2 for GPs and 7.1 for paediatricians [1]. Other studies found a lower workload for paediatricians, and they noted that females work fewer hours per week [1, 6]. This in in line with our finding that female PCPs work a mean of 2.0 half-days less than their male colleagues, and that more paediatricians are female (70%), working a mean of 0.7 half-days less than GPs. Part-time work has become more and more popular, given the fact that both men and women equally want to combine work and family life. A survey in 2017 with members of the Swiss Young General Practitioners Association (JHaS) showed that the majority would like to work part-time and group practice are favoured [13].
In recent years, the type of practice has shifted from single practices to group practices. The mfe-study noted a change from 12% in 2005 to 45% PCPs working in group practices in 2020. In our study the number was even higher, with 61% of GPs and 76% paediatricians working in a group practice.
The yearly FMH statistics in 2020 showed that 34.5% of all doctors in the outpatient sector have a foreign medical diploma [6]. In our study this proportion was 20% for GPs and even less for paediatricians, at 16.5%. Because the FMH statistics included all the doctors working in the outpatient sector, we assume that the other specialisations might have even higher numbers of foreign doctors.
The mfe study in 2020 had already mentioned that PCPs in the region Espace Mittelland (of which the Canton of Bern is the largest area) noted the greatest shortage: 72% of GPs and 65% of paediatricians reported a shortage there. These results are similar to our findings for the GPs, but more paediatricians in our survey mentioned a shortage in their region: 78% compared with 65% in the mfe-study [5].
We found a PCP workforce density of 0.75 FTEs per 1000 inhabitants. There is no internationally consistent definition of what density of the primary care workforce is adequate. Some studies claim that one PCP per 1000 inhabitants is enough [4], others argue that every additional 0.1 PCP per 1000 inhabitants reduces mortality rates [14]. Moreover, some look at countries with a well functioning healthcare system such as Canada, which has 1.33 PCPs per 1000 inhabitants, in order to give a recommendation on the ideal workforce. Anyhow, the density in the Canton of Bern is lower than these numbers. In addition, in 2020 a majority of PCPs described a shortage in their region. Around 60% could not take on new patients without restrictions in their practice and 13% of the workforce was provided by doctors at or over retirement age.
Therefore, the Canton of Bern already has a shortage in 2020 and the shortage is predicted to increase over just 5 years. In a study by the Swiss health observatory (Obsan), the regional distribution of the primary care workforce has been already reported. For GPs, there are important differences between rural areas, with 0.6 GPs per 1000 inhabitants compared with 1.4 GPs per 1000 inhabitants for city centres, and 1 GP per 1000 inhabitants for intermediate areas. The same has been noted for paediatricians. From 2012 to 2019, the total number of paediatricians in city centres has increased, whereas in rural areas it has decreased [15]. The study did not comment on whether the numbers represented a shortage or not. Another study by BEKAG in 2010 found that in all the administrative districts physicians noted a PCP shortage, with Oberaargau, Jura bernois, and Emmental as the most affected regions [16]. In our study in 2020, we found a slightly different picture as the districts Biel, Frutigen-Niedersimmental followed by Berner Jura and Obersimmental-Saanen were the most affected regions. However, without new PCPs coming in, all other more populated regions will soon be affected too. A difference between rural and urban areas can be found in other European countries also [17, 18]. A study from Germany evaluated the regional distribution and found a difference in working hours per week. On average, PCPs in single-handed practices in rural areas worked 4 hours more per week than their urban counterparts [17]. In contrast, no significant difference in average working hours was observed in group practices. Single practices are more popular in rural areas [13]. These observations could contribute to the lower attractiveness and the more imminent shortage of primary care in rural areas.
Altogether our findings imply an imminent shortage of PCPs already in 2020 and that PCPs will struggle to find successors for their practices in the Canton of Bern. This is worrying, as we know of various studies showing that the basis of a well functioning and cost-effective healthcare system is a good primary care supply. It is believed that 94% of medical problems can be solved in a GP’s office, while generating only about 7.9% of all the healthcare costs [19]. Furthermore, having more actively working PCPs in the primary healthcare system means fewer visits to emergency rooms and fewer visits to specialists [20]. A strong primary care service in Europe is positively associated with improving population health, reducing socioeconomic inequalities in health and avoiding potentially unnecessary hospitalisations [21].
To be able to fulfil these goals for the Canton of Bern and Switzerland, we need to have a well-distributed primary care workforce. In former years there was a slight increase of medical students, but with an increasing and ageing population, the demand for primary care has grown more than its availability.
Within the next 5 years the shortage will become more pressing. To overcome this, the trend to work part time and migration are influential factors, but, as shown in our models, part-time work has less effect than the share of new PCPs coming from Swiss universities. Assuming that only 20% of medical students become PCPs [12], we will have a shortage of 50% by the year 2035 [3].
The government had already passed a strategy against the shortage of physicians in 2011, which aimed at increasing the number of physicians trained each year to around 1300 by 2023 [22, 23]. But these additional young doctors need to be motivated to become PCPs, even during undergraduate training. Programmes are currently being implemented in different universities. Additionally, building up more attractive postgraduate training programmes in general practice seems to be an important aspect of the promotion of primary care. Having a supervisor during the trainee period, having a structured trainee programme and the wish for part-time work are all important for young doctors [24]. Programmes such as the cantonal practice traineeship programme can help to promote a career in primary care in regions where there is a shortage. In a long-term evaluation of the programme in the Canton of Bern, around 50% of trainees later started work in the same practice as their mentor and 81% of the doctors who participated in the programme became or will become PCPs after their traineeship [25].
All these steps can help in promoting primary care, but due to the length of educational programmes it will still be at least 10 years until trainees can succeed the older generation of PCPs. When they do, we need good conditions for PCPs in practice and these must take into account new working trends and the aging population.
Furthermore, building a register of PCPs in every cCanton could help to provide an overview by gathering information on workload and region of work. The register needs to be easy to access and suitable for every PCP. In this way an impending shortage in the supply of primary care would be noticed and could be acted on in good time. Lastly, we believe our methods provide a basis for future research in Switzerland and beyond to compute FTEs by allowing PCPs to reduce or increase workload and incorporating growth of the population served, as well as selecting different scenarios to offset the drop in the workforce.
By using different methods (letters, emails, internet research and telephone calls) to gather information, we were able to achieve a higher than usual response rate of 95%. To our knowledge, this is the first time, the Canton of Bern has data with such high external validity.
Workforce data is based on self-declaration. We asked about the workload as a percentage and in half-days, in order to minimise bias, and we therefore think this is the best possible approach in a survey study. For our future scenario, we not only asked about retirement, or stopping work, but also about planned alteration of the workload upwards or downwards, which has not been done before.
We could not collect data from residents, who contribute to the workforce as well, mainly during traineeships in practice. This was not the case in other studies either. Residents cannot be tracked, because of changing workplaces and because they are not registered. On the other hand, this workforce is fluctuating and has to be compensated for in practices during times when there is no trainee. Of course, trainees can only work in existing PCP practices for which we had data on the workforce of PCPs.
The PCPs working near cantonal boarders, so not within the canton of Bern, were not included even though when they are probably treating patients from over the cantonal border and therefore contribute to the PCP workforce in the canton of Bern. We are, however, preparing to collaborate with Obsan to provide such estimates using a floating-catchment-area (FCA) method, which allows small area density estimates that take into account patient flows across administrative borders [26].
Moreover, calculating the workforce in half-days does not give an exact number, as it can vary between 4 to 6hours for a regular workday. Therefore, doctors can have the same work load on the basis this calculation, but one doctor might work up to about 20 hours more per week. However, our data of working percent and working half-days correlated well. In addition, this work load does not define how many consultations per day were carried out and neither how complex they were.
Lastly, we acknowledge that due to uncertainty one must make assumptions: how many physicians will still move to Switzerland as PCPs? How many medical students will choose to become PCPs in the Canton of Bern? Will there be a competition between regions within Switzerland for new PCPs? This study does not provide all answers to all potential questions, but provides a basis to build assumptions, which is why we chose to showcase different scenarios.
With this study we could show that in 2020 we had a mean PCP density of 0.75 full-time PCPs per 1000 inhabitants and in some regions as few as 0.59 full-time PCPs per 1000 inhabitants. Because there is no uniform definition of the ideal PCP workforce density, we cannot define how low this is. In fact, in 2020 two thirds of PCPs already described a shortage in their region and only 40% could take on new patients without restrictions. Furthermore, 13% of PCPs worked in 2020 despite being at or over retirement age. In the next 5 years, the workforce density will drop by 25%.
We need to strengthen primary care physician education programmes and promote them even to medical students. Furthermore, we need a good register for PCPs to be able to better monitor developements in the workforce .
Due to data protection regulations, it is not possible to share original study data. For further projects, highly aggregated data can be shared upon request and only if the research group member’s consent.
This study was fully funded by HaSt (Berner Stiftung zur Förderung der Hausarzt-Medizin), BEKAG (Aerztegesellschaft des Kanton Berns), VBHK (Verein Berner Haus- und KinderärzteInnen), FMH and UNZ (Universitäres Notfallzentrum, Inselspital Bern).
The authors declare no conflict of interest.
We would like to thank all physicians in the canton of Bern who participated in this study. Furthermore, we would like to thank our partner organisations for funding and support: HaSt, BEKAG, VBHK, FMH and UNZ, as well as to our project partners at Obsan for support.
We want to thank Liselotte Aeschimann and Susanne Kick for their administrative support at BIHAM, which enabled us to achieve such a high participation number.
1. Zeller A , Giezendanner S . Resultate der 4. Workforce Studie. Prim Hosp Care. 2020;20(11):325–8. https://doi.org/10.4414/phc-d.2020.10311
2. Pahud O . Ärztinnen und Ärzte in der Grundversorgung-Situation in der Schweiz und im internationalen Vergleich. Schweizerisches Gesundheitsobservatorium (Obsan). 2019;15:160.
3. Zeller A , Tschudi P . «Anamnese und Status» bei Schweizer Hausärzten. Prim Hosp Care. 2016;16(15):277–80. https://doi.org/10.4414/phc-d.2016.01327
4. Dürrenmatt U , Kissling B , Marty F . Hausärztedichte im Kanton Bern 2005 - 1-Minuten-Umfrage des VBH. Prim Hosp Care. 2006;6(24):441–4. https://doi.org/10.4414/pc-f.2006.07157
5. mfe Haus- und Kinderärzte Schweiz. 2020 [cited 2021 Jun 24]. Available from: https://www.hausaerzteschweiz.ch/information/news/detail/workforce-studie-zur-medizinischen-grundversorgung-hausaerztemangel-aber-mit-licht-am-horizont
6. Hostettler S , Kraft E . FMH-Ärztestatistik 2020 – die Schweiz im Ländervergleich. Schweiz Arzteztg. 2021;102(12):1–6. https://doi.org/10.4414/saez.2021.19698
7. Die 10 Verwaltungskreise (Kanton Bern). [cited 2021 Jun 24]. Available from: https://www.jgk.be.ch/jgk/de/index/direktion/organisation/rsta.html#originRequestUrl=www.be.ch/regierungsstatthalter
8. Population and Households Statistics (STATPOP) . [cited 2021 Jun 25]. Available from: https://www.bfs.admin.ch/bfs/en/home/statistics/population/surveys/statpop.assetdetail.8541.html
9. Regionalisierte Bevölkerungsszenarien für den Kanton Bern bis ins Jahr 2050. (Kanton Bern). [cited 2021 Jun 24] Available from: https://www.be.ch/portal/de/index/mediencenter/medienmitteilungen.meldungNeu.html/portal/de/meldungen/mm/2021/04/20210401_1404_moderates_bevoelkerungswachstumundstarkeveraenderungderaltersstr?utm_source=rss&utm_medium=Medienmitteilungen&utm_campaign=Moderates+Bevölkerungswachstum+und+starke+Veränderung+der+Altersstruktur+bis+ins+Jahr+2050
10. Hostettler S , Kraft E . FMH-Ärztestatistik 2018. Wenig Frauen in Kaderpositionen. Schweiz Arzteztg. 2019;100(12):411–6. https://doi.org/10.4414/saez.2019.17687
11. Unimedsuisse facts and figures [Internet]. [cited 2021 Jun 25]. Available from: https:/www.unimedsuisse.ch/de/universitaere-medizin/facts-figures
12 Diallo B , Rozsnyai Z , Bachofner M , Maisonneuve H , Moser-Bucher C , Mueller YK , et al. How many advanced medical students aim for a career as a gp? Survey among Swiss students. Praxis (Bern 1994). 2019;108(12):779-786. doi: https://dx.doi.org/https://doi.org/10.1024/1661-8157/a003300.
13. Gisler LB , Bachofner M , Moser-Bucher CN , Scherz N , Streit S . From practice employee to (co-)owner: young GPs predict their future careers: a cross-sectional survey. BMC Fam Pract. 2017 Feb;18(1):12. https://doi.org/10.1186/s12875-017-0591-7
14. Basu S , Berkowitz SA , Phillips RL , Bitton A , Landon BE , Phillips RS . Association of Primary Care Physician Supply With Population Mortality in the United States, 2005-2015. JAMA Intern Med. 2019 Apr;179(4):506–14. https://doi.org/10.1001/jamainternmed.2018.7624
15 Sturny I , Widmer M. Unterschiede in der Entwicklung des Angebots und der Inanspruchnahme in der Stadt und auf dem Land. Neuchâtel: Obsan Swiss Health Observatory. Report Nr.: 13/2020.
16. Heuberger T , Kilchherr C . Hausarztmedizin im Kanton Bern – Bericht an den Grossen Rat zu den Motionen Heuberger (035/2005) und Kilchherr (090/2005). 2011[cited 2021 Jun 24] Available from: https://www.bve.be.ch/bve/de/index/wasser/wasser/aktuell.assetref/dam/documents/portal/Medienmitteilungen/de/2011/11/2011-11-04-bericht-hausarztmedizin-de.pdf
17. Steinhaeuser J , Joos S , Szecsenyi J , Miksch A . A comparison of the workload of rural and urban primary care physicians in Germany: analysis of a questionnaire survey [Pubmed]. BMC Fam Pract. 2011 Oct;12(112):112. https://doi.org/10.1186/1471-2296-12-112
18. Groenewegen PP , Bosmans MW , Boerma WG , Spreeuwenberg P . The primary care workforce in Europe: a cross-sectional international comparison of rural and urban areas and changes between 1993 and 2011. Eur J Public Health. 2020 Sep;30(4 Suppl_4):iv12–7. https://doi.org/10.1093/eurpub/ckaa125
19 Pellegrini S , Roth S. Entwicklung der Kosten und der Finanzierung des Versorgungssystems seit der Revision der Spitalfinanzierung. Neuchâtel: Obsan Swiss Health Observatory Report Nr.: 1/2016.
20. Gulliford MC . Availability of primary care doctors and population health in England: is there an association? J Public Health Med. 2002 Dec;24(4):252–4. https://doi.org/10.1093/pubmed/24.4.252
21 Kringos D , Boerma W , Hutchinson A , Saltman RB . Building primary care in a changing Europe. Eur Obs Heal Syst Policies. 2015;No.38 Pubmed
22. Der Hochschulrat genehmigt das Sonderprogramm 2017-2020 «Erhöhung der Anzahl Abschlüsse in Humanmedizin» (Schweizerische Hochschulkonferenz). [cited 2021 Jun 25]. Available from: https://www.admin.ch/gov/de/start/dokumentation/medienmitteilungen.msg-id-60790.html. 2016
23. Aufnahmekapazitäten für medizinische Studiengänge 2021/2022 (Swiss Universities). [cited 2021 Jun 25]. Available from: https://www.swissuniversities.ch/fileadmin/swissuniversities/Dokumente/Lehre/Medizin/200828_Kapazitaeten_Medizin_21_22_konsolidiert.pdf. 2020
24. Rozsnyai Z , Tal K , Bachofner M , Maisonneuve H , Moser-Bucher C , Mueller Y , et al. Swiss students and young physicians want a flexible goal-oriented GP training curriculum. Scand J Prim Health Care. 2018 Sep;36(3):249–61. https://doi.org/10.1080/02813432.2018.1487582
25 Rozsnyai Z , Diallo B , Streit S. Eine Erfolgsgeschichte: 10 Jahre Praxisassistenzprogramm im Kanton Bern. Schweiz Arzteztg. 2019;100(19):642-643. doi: https://dx.doi.org/https://doi.org/10.4414/saez.2019.17691
26 Jörg R , Lenz N , Wetz S , Widmer M. Modell zur Analyse der Versorgungsdichte: Herleitung eines Index zur räumlichen Zugänglichkeit mithilfe von GIS und Fallstudie zur ambulanten Grundversorgung in der Schweiz. Neuchâtel: Obsan Swiss Health Observatory Report Nr.: 01/2019.