Parents under siege: the psychological impact of COVID-19 outbreak on children’s caregivers
DOI: https://doi.org/10.4414/SMW.2021.w30012
Eirini
Kostopouloua*, Xenophon
Sinopidisa*, Dimos
Gidarisb, Nikolaos
Karantaglisc, Dimitrios
Cassimosd, Despoina
Gkentzia, Ageliki A.
Karatzaa, Emmanouil
Paraskakisd, Eleni
Jelastopulua, Gabriel
Dimitrioua, Sotirios
Fouzasa
a School of Medicine, University of Patras, Greece
b University of Nicosia, Cyprus
c 3rd Paediatric Department, Aristotle University of Thessaloniki, Greece
d School of Medicine, Democritus University of Thrace, Greece
* These authors contributed equally.
Summary
AIMS OF THE STUDY: It is well known that parenting stress is an important but often underestimated psychosocial variable. Data regarding the impact of the corona virus disease 2019 (COVID-19) outbreak on parental psychology are currently lacking. The aim of the present study was to assess parenting stress during the COVID-19 pandemic in Greece.
METHODS: An Internet e-survey was conducted adhering to CHERRIES guidelines of the EQUATOR network and released from 16 March to 22 March 2020, using the Perceived Stress Scale (PSS) and Revised Impact of Event Scale (IES-R). A convenience sample of 1105 Greek parents of children with or without chronic or severe underlying disorders was enrolled, identified by a network of collaborating paediatricians across the country, and invited via personal emails.
RESULTS: The participation rate was 91.6% and the completion rate was 100%. A total of 178 (16.1%) of the participants had children with underlying disorders (198 affected children in total). Parents of children with underlying disorders had significantly higher stress levels than those of healthy children (PSS 21.22 ± 5.06 vs 19.02 ± 6.85, p <0.001; IES-R 40.71 ± 11.58 v. 35.86 ± 12.69, p <0.001), particularly those caring for children with cardiovascular or respiratory disorders, or immunodeficiencies. The presence of children with underlying disorders was a strong predictor of PSS and IES-R scores, independently of parental sex, age, education and place of residence.
CONCLUSIONS: The impact of COVID-19 outbreak on parental stress is substantial, and those caring for children with underlying disorders are more profoundly affected. Pending the global socioeconomic rebooting after the pandemic, the possible short- and long-term consequences of parental stress should not be ignored. As for other vulnerable groups, accurate health information and resources for psychological support should be provided to parents, especially those caring for children with underlying disorders.
Introduction
Historically, infectious disease outbreaks have a significant psychosocial impact on society [1]. Any readily and rapidly transmitted agent, especially when associated with increased mortality, may precipitate negative psychological responses ranging from fear, denial and frustration to helplessness and acceptance [2]. Although these reactions are shaped at the individual subconscious level, they eventually diffuse in the community and trigger “cyclical fear” phenomena [1, 2], which may even facilitate the spread of the disease [1, 2].
Health authorities have already warned about the psychological implications of corona virus disease 2019 (COVID-19) [3]. The high mortality rate, the unprecedented measures taken to control the outbreak and the pervasive uncertainty around its outcome may cause significant psychological distress and increase the risk of relevant mental disorders [1, 2]. In this context, older adults, people with underlying health conditions, healthcare workers, and children and adolescents have been identified as the most vulnerable and special recommendations have been issued [3, 4].
Parenting stress represents an important psychosocial variable that is often unrecognised and underestimated [5]. Although it primarily affects the parents, it may easily diffuse to their social and work environment with significant consequences [5]; this is particularly true for caregivers of children with underlying diseases [6]. Arguably, healthy children are less likely to be severely affected by COVID-19 [7]; however, data on paediatric populations with chronic or serious underlying disorders remain scant and controversial [7], thus potentially increasing the psychological distress of their caregivers during the pandemic.
The aim of this study was to investigate the psychological burden of parents during the COVID-19 epidemic in Greece. We hypothesised that the parents, especially those caring for children with underlying disorders, may experience increased stress levels and thus be prone to stress-related mental disorders.
Materials and methods
This was a cross-sectional study (e-survey) of a convenience sample of Greek parents (either mother or father) conducted in mid-March 2020, shortly after the outbreak of COVID-19 in Greece. These were parents of children with chronic diseases or children without chronic diseases. Chronic diseases included cardiovascular diseases (congenital heart disease, heart failure), respiratory diseases (asthma, chronic lung disease of prematurity), diabetes mellitus, immunodeficiencies (including chemotherapy-induced), renal disorders (chronic renal failure, grades IV or V vesicoureteral reflux) and neuromuscular disorders. Medical conditions such as allergy, gastrointestinal disorders, anaemia, and obesity were characterised as “other”. An English version of the survey is available at https://forms.gle/xdtK3vqaPqFxEXhb6.
The study was conducted according to CHERRIES guidelines for e-surveys; a detailed checklist is presented in table S1 in the appendix. Briefly, potential participants were identified from the patient lists of 19 collaborating paediatricians across Greece (at least one from each of the 13 Administrative Regions) and contacted via email or personal social media messages. The questionnaire was developed in Google Forms and consisted of four sections: (1) introduction page; (2) (general information section, with details on parental demographics, place of residence and number of children; (3) children’s medical history; 4) psychometric testing section, consisting of the validated Greek versions of the Perceived Stress Scale (PSS) (10 items) [8] and the Revised Impact of Event Scale (IES-R) (22 items) [9]. PSS is the most widely used psychological instrument for measuring the perception of stress. PSS items are designed to capture feelings and thoughts of the respondents and to tap how unpredictable, uncontrollable and overloaded they find their lives. The scale also includes a number of direct queries about current levels of experienced stress. The participants could select any of 10 possible psychological responses. IES is a self-report tool consisting of 22 questions developed to measure the subjective response caused by an acute and stressful life event (post-traumatic stress). It is an easily answered and scored questionnaire. An IES-R score higher than 38 is considered suggestive for post-traumatic stress disorder [10]. Both questionnaires were brief and anonymous to guarantee confidentiality. The total number of the displayed questions varied depending on the number of children in the family; the minimum number of questions was 44 (one child) and the maximum 56 (five children).
Potential participants were initially directed to the introduction page, where information regarding study aims and a consent form were available. Parents who did not consent to participate were redirected to the end-of-study page. Responding to all questions was mandatory; participants were able to review their answers or leave the survey at any stage. The survey was released from 16 March (12:00) to 22 March 2020 (23:59) and the responses were automatically stored in a secure database. The study was approved by the Research Ethics Committee of the University of Patras, Greece (Approval ID: 129/10.3.2012), and was conducted in accordance with the Helsinki Declaration as revised in 2013.
Categorical variables (number of cases, %) were compared with the chi-square test, and continuous variables (mean ± standard deviation [SD]) with the Student’s t- or Mann-Whitney U-tests. Comparisons of parental scores among children with underlying disorders were performed using the Kruskal-Wallis test with Dunn’s post-hoc test for multiple comparisons. In the case of parents reporting more than one child with a chronic disease, their questionnaire score was included more than once. The effect of sex, age, education level, place of residence, presence of an adult >65 years old in the family and presence of a child with an underlying disorder on the PSS and IES-R scores was assessed with univariable and multivariable linear regression. Statistical analyses were performed with the IBM SPSS version 25 (IBM Corp., Armonk, NY). The level of statistical significance was set at 5%.
Results
Of the 1476 parents invited, 1206 accessed the survey (view rate 81.7%); 72 visitors declined to participate and 29 were excluded for technical issues, resulting in a response rate of 79.4%. The completion rate was 100%. The geographical distribution of responders and that of COVID-19 cases in Greece during the survey period are presented in supplementary figure S1 in the appendix.
Participants’ characteristics are presented in table 1. Most of the responders (86.7%) in the group of healthy children and 87.6% in the group of children with a chronic disease were mothers, with a mean age ± SD of 40.4 ± 6.8 years and 41.9 ± 7.3 years, respectively. In the group of healthy children, 72.1% of the parents were of higher educational level, as compared with 65.7% in the group of children with a chronic disease (p = 0.013). Most participants were of urban residence in both groups (61.7% vs 57.9%, respectively). The mean age of children without a chronic disease was 9.2 ± 5.6 years and that of children with underlying disorders was 10.5 ± 5.5 years (p <0.001) (table 1).
Table 1Characteristics of study participants.
|
Parents of healthy children
|
Parents of children with chronic/severe disorders
|
| N |
927 |
178 |
| Mothers, n (%) |
804 (86.7) |
156 (87.6) |
| Age, years |
40.4 ± 6.8* |
41.9 ± 7.3* |
| Education**, n (%) |
|
|
| – Primary (<6 years) |
16 (1.7) |
8 (4.5) |
| – Secondary (7–12 years) |
242 (26.1) |
53 (29.8) |
| – Tertiary – no university |
283 (30.5) |
59 (33.1) |
| – Tertiary – university |
386 (41.6) |
58 (32.6) |
| Place of residence, n (%) |
|
|
| – Urban |
572 (61.7) |
103 (57.9) |
| – Semi-urban |
185 (20.0) |
36 (20.2) |
| – Rural |
170 (18.3) |
39 (21.9) |
| Adult >65 years old in close contact, n (%) |
438 (47.2) |
76 (42.7) |
| Number of children in the family***, n (%) |
|
|
| – 1 |
308 (33.2) |
44 (24.7) |
| – 2 |
511 (55.2) |
96 (53.9) |
| – 3 |
96 (10.4) |
31 (17.4) |
| – 4 |
12 (1.2) |
7 (3.9) |
| Average age of children |
9.2 ± 5.6**** |
10.5 ± 5.5**** |
Overall, 178 parents (16.1%) had 198 children with underlying disorders (fig.1). Of these, 17 (9.5%) had a cardiovascular disease, 97 (54.5%) a respiratory disease, 38 (21.3%) diabetes mellitus, 8 (4.5%) immunodeficiency, 7 (3.9%) a renal disorder, 12 (6.7%) a neuromuscular disease and 10.6% other chronic disorders. In 12 children, a second chronic disease was reported (7 obesity, 5 anaemia); these secondary diagnoses were not included in the analysis.
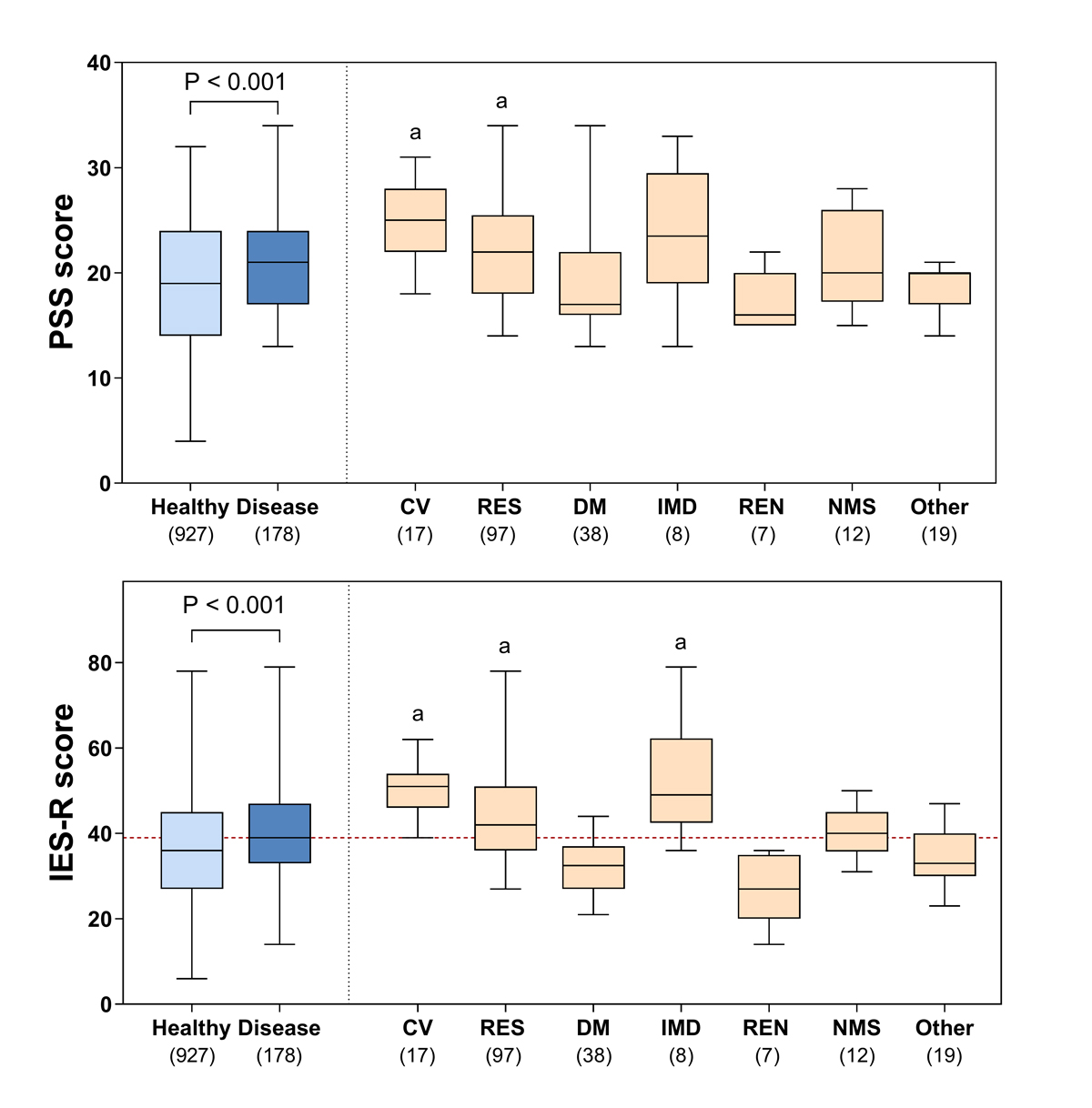
Figure 1 PSS and IES-R scores (box-and-whisker plots with median, 75th percentile and range). Left panels: score comparisons between parents of healthy children and those of children with underlying disorders (Mann-Whitney U-test). Right panels: comparisons of parental scores among children with underlying disorders (n = 198) (Kruskal-Wallis test with Dunn’s post-hoc test for multiple comparisons). Red dotted line: cut-off for diagnosis of post-traumatic stress disorder. Number of cases are given in parentheses. a: significantly higher (p <0.01) compared with DM, REN and “other” disorders.
CV =cardiovascular disorders (congenital heart disease, heart failure); RES = respiratory disorders (asthma, chronic lung disease of prematurity); DM = diabetes mellitus; IMD = immunodeficiency (including chemotherapy) REN = renal disorders (chronic renal failure, grades IV or V vesicoureteral reflux); NMS = neuro-muscular disorders; Other = allergy, gastrointestinal disorders, anaemia, obesity.
PSS and IES-R scores (19.37 ± 6.64 and 36.64 ± 12.64, respectively) were significantly correlated (Pearson’s r = 0.666, p <0.001). Parents of children with underlying disorders reported higher stress levels than those of healthy children (Student’s t-test; PSS 21.22 ± 5.06 vs 19.02 ± 6.85, p <0.001; IES-R 40.71 ± 11.58 vs 35.86 ± 12.69, p <0.001) (fig.1). An IES-R score higher than 38 [10] was noted in 51.7% (n = 92) of parents of children with underlying disorders and 40.3% (n = 374) of those with healthy children (p = 0.007) (fig.1). Higher stress scores were noted in parents caring for children with cardiovascular and respiratory disorders or immunodeficiencies (fig.1). Multivariable linear regression analysis revealed that the presence of children with underlying disorders was a strong predictor of PSS and IES-R scores, independently of parental sex, age, education and place of residence (table 2).
Table 2Determinants of PSS and IES-R scores.
|
Variable
|
PSS
|
IES-R
|
|
|
Unadjusted effect
|
Adjusted effect
|
Unadjusted effect
|
Adjusted effect
|
|
| Female sex |
0.209*
|
0.196*
|
0.251*
|
0.229*
|
|
| Age |
–0.098**
|
–0.056 |
–0.135*
|
–0.086***
|
|
| Education (lower to higher) |
–0.042 |
–0.028 |
–0.060 |
–0.047 |
|
| Residence (urban, semi-urban, rural) |
–0.012 |
–0.068 |
–0.017 |
–0.026 |
|
| Adult >65 years in close contact |
0.024 |
0.039 |
0.013 |
0.022 |
|
| Child with underlying disorder |
0.122*
|
<0.124*
|
0.141*
|
0.143*
|
|
Discussion
In this study we assessed the psychological impact of the COVID-19 pandemic on a large sample of Greek parents. We found that the levels of perceived stress were extremely high, particularly among caregivers of children with chronic or severe underlying disease. Increased stress levels were consistent in both psychometric tools, and almost half of the parents were classified as at high risk for post-traumatic stress disorder (fig.1).
Females, younger parents and those carrying for children with underlying disorders had higher stress levels (table 2). However, in the multivariable regression analysis only the presence of a child with a chronic disorder and female sex emerged as significant predictors of PSS and IES-R scores, independently of the education level and the place of residence. Higher PSS and IES-R scores in females have been consistently reported previously [8–11].
The impact of environmental stressors may be more profound in parents of children with chronic or severe underlying disorders [6]. During infectious disease outbreaks, for example, compliance with chronic medication and regular health care utilisation may be difficult for such children, thus causing additional psychological distress to their caregivers [5]. Interestingly, the parents of children with cardiovascular, respiratory and immune system disorders appeared to be more stressed (fig.1). The predilection of COVID-19 for the respiratory system, the frequency of cardiovascular complications and the pivotal role of the immune system in coping with the disease may explain these differences.
To the best of our knowledge, this is the first study reporting on the psychological burden of parents during the COVID-19 pandemic. Other strengths include the large sample size, the wide population coverage and the high participation rate. Parenting anxiety is a well-recognised distress factor for the family [5, 6]. However, since parents represent a substantial part of the economically active population in westernised societies, parenting stress may also have significant socioeconomic implications [5]. This important aspect has been generally unrecognised and underestimated in the current literature.
Inevitably, our study has weaknesses. First, the participants were recruited from the patient lists of collaborating paediatricians, which may have resulted in an overrepresentation of children with chronic disorders. However, all children in Greece visit a paediatrician who follows them closely, performs the vaccinations, monitors their growth, keeps detailed medical records and treats acute illnesses that do not require in-hospital care. Therefore, most children on paediatricians’ patient lists are, in principal, healthy. Second, the IES-R was developed to measure the subjective response to a traumatic incident and, thus, might not be suitable for exploring the psychological impact of long-lasting events such is the pandemic. However, our survey was released shortly after the outbreak of COVID-19 in Greece and in parallel with the escalation of the restriction measures; therefore, the use of this tool should be considered valid. The strong correlation between IES-R and PSS lends further support to the above hypothesis. Of note, the IES-R has been applied to explore the psychological burden at the peak of COVID-19 epidemic in China [11]. Finally, our study lacks a proper control group. For example, the inclusion of adults who were not parents would permit us to estimate more precisely the psychological burden of COVID-19 on the parents. Also, data on the PSS or IES-R scores of parents of children with chronic disorders before the pandemic would enable us to describe the net impact of COVID-19 on this group. It should be mentioned, however, that the PSS score of our participants was higher than the value reported for the Greek general population (i.e. 17.73 ± 6.64) [8]. Future studies, with a longitudinal design and repeated psychometric measurements, will allow for a better understanding of the psychological burden of COVID-19 in specific population groups and the factors that may influence it.
In conclusion, the impact of COVID-19 on parental psychology is substantial and unprecedented, and those caring for children with underlying disorders are more profoundly affected. Pending the global socioeconomic rebooting after the pandemic [12], the possible short- and long-term consequences of parental stress should not be ignored. Like other vulnerable groups, accurate health information and resources for psychological support should be provided to parents, especially those caring for children with underlying disorders.
Dr Eirini Kostopoulou
Department of Paediatrics
University Hospital of Patras
GR-Rion-Patras, 26504
Irekost[at]upatras.gr, eirini.kost[at]gmail.com
References
1
Van Bortel T
,
Basnayake A
,
Wurie F
,
Jambai M
,
Koroma AS
,
Muana AT
, et al.
Psychosocial effects of an Ebola outbreak at individual, community and international levels. Bull World Health Organ. 2016 Mar;94(3):210–4. https://doi.org/10.2471/BLT.15.158543
2
Pappas G
,
Kiriaze IJ
,
Giannakis P
,
Falagas ME
. Psychosocial consequences of infectious diseases. Clin Microbiol Infect. 2009 Aug;15(8):743–7. https://doi.org/10.1111/j.1469-0691.2009.02947.x
3
Centers for Disease Control and Prevention
. Mental health and coping during COVID-19. Available at: http://www.cdc.gov/coronavirus/2019-ncov/prepare/managing-stress-anxiety.html. Accessed 2021 June 6.
4
Xiang YT
,
Yang Y
,
Li W
,
Zhang L
,
Zhang Q
,
Cheung T
, et al.
Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry. 2020 Mar;7(3):228–9. https://doi.org/10.1016/S2215-0366(20)30046-8
5
Golics CJ
,
Basra MK
,
Finlay AY
,
Salek S
. The impact of disease on family members: a critical aspect of medical care. J R Soc Med. 2013 Oct;106(10):399–407. https://doi.org/10.1177/0141076812472616
6
Cousino MK
,
Hazen RA
. Parenting stress among caregivers of children with chronic illness: a systematic review. J Pediatr Psychol. 2013 Sep;38(8):809–28. https://doi.org/10.1093/jpepsy/jst049
7
Cruz AT
,
Zeichner SL
. COVID-19 in Children: Initial Characterization of the Pediatric Disease. Pediatrics. 2020 Jun;145(6):e20200834. https://doi.org/10.1542/peds.2020-0834
8
Andreou E
,
Alexopoulos EC
,
Lionis C
,
Varvogli L
,
Gnardellis C
,
Chrousos GP
, et al.
Perceived Stress Scale: reliability and validity study in Greece. Int J Environ Res Public Health. 2011 Aug;8(8):3287–98. https://doi.org/10.3390/ijerph8083287
9
Mystakidou K
,
Tsilika E
,
Parpa E
,
Galanos A
,
Vlahos L
. Psychometric properties of the Impact of Event Scale in Greek cancer patients. J Pain Symptom Manage. 2007 Apr;33(4):454–61. https://doi.org/10.1016/j.jpainsymman.2006.09.023
10
Creamer M
,
Bell R
,
Failla S
. Psychometric properties of the Impact of Event Scale - Revised. Behav Res Ther. 2003 Dec;41(12):1489–96. https://doi.org/10.1016/j.brat.2003.07.010
11
Wang C
,
Pan R
,
Wan X
,
Tan Y
,
Xu L
,
Ho CS
, et al.
Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020 Mar;17(5):1729. https://doi.org/10.3390/ijerph17051729
12
United Nations
. Report on socio-economic impacts of COVID-19. March 31, 2020. Available at: https://www.un.org/en/un-coronavirus-communications-team/launch-report-socio-economic-impacts-covid-19 Accessed June 6, 2021.
Appendix: Supporting data
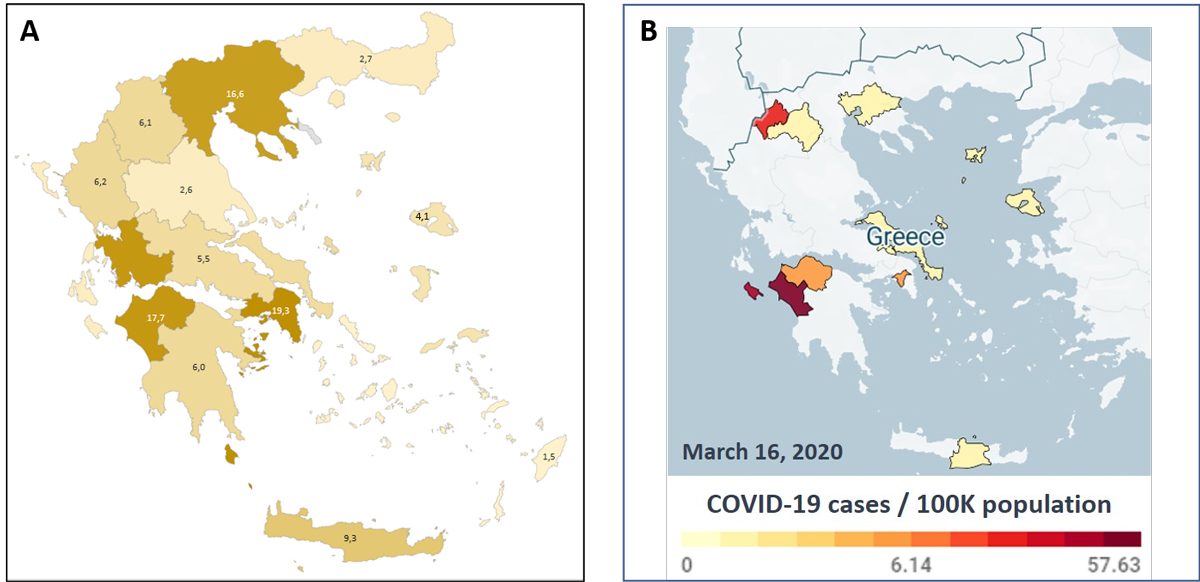
Figure S1 A: Distribution of responders (n = 1105; 16–22 March 2020) per Greek Administrative Region. Β: Distribution of COVID-19 cases per 100,000 population in Greece on 22 March 2020 (Available at: https://lab.imedd.org/covid19).
Table S1Checklist for Reporting Results of Internet E-Surveys (CHERRIES).
|
Item Category
|
Checklist Item
|
|
|
Design
|
Survey design |
Target population: parents of children with or without chronic disorders with permanent residence in Greece.Sample: A convenience sample of parents with healthy children or with children suffering from at least one chronic disorder. Potential participants were identified from the patient lists of pediatric offices (general or specialized pediatricians) across Greece and contacted by email or personal messages through social media. |
|
IRB (Institutional Review Board) approval and informed consent process
|
IRB approval |
This study was reviewed and approved by the Ethics Committee of the University Hospital of Patras, Greece. |
| Informed consent |
In the introduction page, potential participants were briefly informed about the purpose of the study and assured that all survey responses would remain anonymous and no personal information was recorded. They were also informed that a valid email address was required for authenticity purposes which would remain strictly confidential. Finally, it was clarified that all items were “mandatory” and once the survey was launched the participant should either answer all questions or quit the survey.Consent was granted by selecting the option “Yes” in the item “I consent and want to proceed” which was available at the end of introduction page. The option “No” was also available; in this case the visitor was redirected to the last page of the survey where an end-of-survey message was displayed. |
| Data protection |
All data were stored on a secure server of the University of Patras. Only the principal investigator (PI; Prof. Sotirios Fouzas) has access to the database including the corresponding emails. The data were de-identified prior to analysis by deleting all email addresses. |
|
Development and pre-testing
|
Development and testing |
The survey was developed by the PI’s research team. It consisted of five parts:Introduction and consent pageGeneral information page, including parental demographics and information about place of residence and number of children in the familyInformation regarding age and possible chronic diseases of each childPsychometric testing section, consisting of the 10 items of the Perceived Stress Scale (PSS) and the 22 items of the Impact of Event Scale Revised (IES-R) tools. All items were presented according to their official Greek translation (PSS-GR and IES-R-GR, respectively), after the relevant permissions were obtained.A first version of the questionnaire was evaluated on 13 March 2020 (10 responders not related to the research team) and, after refinement, a pilot version of the survey was launched between 14 and 15 March 2020 (20 responders not related to the research team).The final version of the survey is available at https://forms.gle/rX67XUmB9EtFJVU87 and its English version at
https://forms.gle/xdtK3vqaPqFxEXhb6
|
|
Recruitment process and description of the sample having access to the questionnaire
|
Open survey versus closed survey |
This was an open survey of a convenience sample of parents with healthy children or with children suffering from at least one chronic disorder. Potential participants were identified from the patient lists of pediatric offices (general or specialized pediatricians). |
| Contact mode |
Initial contact of potential participants was performed by collaborating pediatricians via personal emails or social media messages. At least one pediatricians (collaborators in PI’s network) from each Greek Administrative Region was contacted and asked to distribute the survey. In total, 19 pediatricians participated. Only parents with an email or social media messaging address were contacted. All eligible parents received the following message: “Dear parents. Colleagues at the University of Patras are launching a research survey regarding your thoughts and feelings during the COVID-19 pandemic. The questionnaire is brief and anonymous. Please take a moment to fill out the survey by following this https://forms.gle/rX67XUmB9EtFJVU87
. Thank you!”. Senders could include their personal details at the end of the message; they were also kindly requested to provide the number of potential participants they contacted. There were no limits in the number of questionnaires each pediatrician could send.
|
| Advertising the survey |
This survey was not posted on websites or social media platforms. Potential participants were also advised to avoid sharing the survey link with other parents. |
|
Survey administration
|
Web/Email |
This was a web-based survey developed on the platform Google Forms. Potential participants were invited by a personal email or social media message which included the survey link (see above). Once linked to the survey, responders directly entered the data and their coded answers were stored automatically in an Excel spreadsheet. The investigator team did not intervene at any phase of the process. On the day the study was completed, the database was downloaded and stored in a secure server of the University of Patras. |
| Context |
The survey was developed on Google Forms and not posted on websites or social media platforms. Potential responders were identified by the collaborating pediatricians (pediatric office patient lists) and contacted via a personal emails or social-media messages. No special recruitment strategy was applied. Participants were by default familiar with computers and comfortable in navigating websites or social media. The research center out of which the survey was conducted is located in the Region of Western Greece, which influenced both recruitment and participation rates in this area (Supplemental Figure 1). Recruitment and participation rates may have also been influenced by the geographical distribution of COVID-19 cases in Greece during the study period (Supplemental Figure 1). Thus, the study sample was not representative of the distribution of population in Greece. |
| Mandatory/voluntary |
The survey was voluntary; it was accessed by clicking on the provided link and launched only after informed consent was granted. |
| Incentives |
No incentives were offered to potential participants. |
| Time/date |
The survey was open for one week, from March 16, 2020 to March 22, 2020; this was also the active recruitment period of the survey. |
| Randomization of items or questionnaires |
No item randomization was applied. |
| Adaptive questioning |
No efforts were made to reduce the number and complexity of questions. All items were presented according to their official Greek translation (PSS-GR and IES-R-GR). |
| Number of items |
The number of displayed questions varied depending on the number of children in the family; the minimum number of questions was 44 (one child) and the maximum 56 (five children). The number of questions per page ranged from 3 to 22. |
| Number of screens (pages) |
The number of displayed pages varied depending on the number of children in the family; the minimum number of pages was 6 and the maximum 11. |
| Completeness check |
All questions were created as “mandatory”; therefore, once the survey was launched the participant should either complete all questions or quit the survey. This was clearly stated in the introduction page and repeated at the beginning of each section. |
| Review step |
Respondents were able to review and change their answers by using the back button located at the bottom of each page. They were also able to return to the introduction page, withdraw their consent and quit the survey. |
|
Response rates
|
Unique site visitor |
Non applicable. The survey link was not posted on any website. |
| View rate (ratio of unique site visitors / unique survey visitors) |
A total of 1476 personal invitations were sent via email or personal social-media messages. However, it is unknown if all recipients received the invitation or eventually used the link. The number of registered unique visitors (see below) was 1206. Yet, it was not possible to calculate the number of visitors who left the survey by simply closing their browser, i.e. without returning to the introduction page and withdraw their consent. Therefore, the view rate 1206/1476 (81.7%) is an estimate; the true view rate cannot be calculated. |
| Participation rate (ratio of unique survey page visitors / agreed to participate) |
From a total of 1206 visitors, 72 declined to participate. In addition, 20 provided an invalid email address and 9 entries were deleted due to duplicate emails (see below); both groups (N=29) were also classified as non-responders. Therefore, the participation rate was 91.6% (1105/1206). |
| Completion rate (ratio of agreed to participate / finished survey) |
Since all questions were created as “mandatory”, the completion rate was 100%.However, it was not possible to identify the number of visitors who left the survey by simply closing their browser, i.e. without returning to the introduction page and withdraw their consent. |
|
Preventing multiple entries from the same individual
|
Cookies used |
No cookies were used in this survey. |
| IP check |
An IP check was not applied in this survey. |
| Log file analysis |
In case of duplicate email addresses, the most recently submitted survey was retained. Following that procedure, nine entries were removed from the database prior to data de-identification and analysis. All nine cases were contacted via email by the research team and stated that they repeated the procedure because they were not sure if the answers were submitted. |
| Registration |
The survey was an anonymous open survey; no registration was required. |
|
Analysis
|
Handling of incomplete questionnaires |
All questions were created as “mandatory”; therefore, there were no incomplete items. |
| Statistical correction |
No item-specific weighting or other statistical corrections was performed. |
| Questionnaires submitted with an atypical timestamp |
Not applicable. The time required to complete the survey was not recorded. |