A retrospective epidemiological study of paediatric femoral fractures
DOI: https://doi.org/10.4414/smw.2020.20360
Raimonda
Valaikaite, Anne
Tabard-Fougère, Christina
Steiger, Eleftheria
Samara, Romain
Dayer, Dimitri
Ceroni
Paediatric Orthopaedic Service, Children’s Hospital, Hopitaux Universitaires de Geneve, Departement de la Femme, de l'Enfant et de l'Adolescent, Geneva, Switzerland
Summary
BACKGROUND
Femoral fracture is a significant major trauma in children and adolescents, sometimes resulting in serious complications. This study aimed to determine the epidemiology of femoral fractures and to define associated injuries and mortality incidence in a pediatric population below 16 years old.
METHODS
The medical records of all patients with a femoral fracture treated in our hospital from 1997–2016 were reviewed retrospectively. Age, gender, mechanism of the trauma, month and season of fracture occurrence, fracture type, associated injuries, and mortality data were collected. Patients were divided into four age groups and compared.
RESULTS
The study included 348 children with 353 femoral fractures. The mean annual prevalence of femoral fracture during the study period was 22.7 per 100,000 children. Except for children less than 1 year old, most fractures occurred in male patients (69%), with a male-to-female ratio of 2.2:1. Road accidents were the most common mechanism at all ages. Femoral fractures were mainly due to low-energy trauma in neonates and infants, to road accidents and low-energy trauma in preschool children, to sports accidents in school-age children, and to road traffic accidents in teenagers. February was the month with the most occurrences of femoral fractures. Winter was the peak season for femoral fractures in children aged <1 year and 6–11 years (37.8% and 46.4% of fractures respectively), whereas autumn was the most common season (29.5%) for preschool children and spring (31.1%) the most common in the teenagers group. Diaphyseal fractures were the most commonly reported lesions in all four age groups, representing 72.3% of all fractures. Only 18 fractures were open (5.1%). Eighty-eight patients (25.3%) presented with associated injuries at admission, 12 presented with Waddell’s triad of injuries, and the mortality rate was calculated to be 1.1% (four cases).
CONCLUSION
The circumstances of injury and the seasonality of femoral fractures differed significantly depending on the children’s ages. Moreover, the morbidity of femoral fractures in children was closely correlated with associated injuries. (Level of evidence: Level III)
Introduction
Femoral fracture is a significant major trauma in children and adolescents, sometimes resulting in serious complications and disability. Paediatric femoral fractures may involve all femoral parts. They occur in children of all ages and may have a significant impact on the child and family [1]. In Western countries, femoral shaft fractures are among the most common diaphyseal fractures in children, with a mean estimated incidence of 20 fractures per 100,000 children [2–5]; in some series this incidence may rise to 35–60 per 100,000 [6–8].
Falls and motor vehicle collisions are responsible for two thirds of femoral fractures [3, 4, 9]. Mortality associated with femoral fracture is estimated at 1 in 600 patients [9] and is closely correlated with associated injuries resulting from high-energy trauma [4].
Although many publications have reported on the various options for treating paediatric femoral fractures, fewer studies have focused on their demographical and etiological characteristics. Thus, the present study aimed to assess femoral fractures in a single Swiss health district in children below 16 years old, with particular reference to epidemiology, fracture patterns and associated injuries. This retrospective study includes some previously unexplored criteria, such as the rate of pathological fractures, the mortality rate and the prevalence of open fractures.
Methods
Following approval from the Children’s Hospital Review Board, we retrospectively reviewed the inpatient data of all children aged 0 to less than 16 years old admitted to Geneva University Hospital for femoral fractures between January 1997 and December 2016. Osteochondral fractures and slipped capital femoral epiphysis were excluded. Our children’s hospital is the only medical facility providing inpatient and specialised medical services, especially for paediatric trauma, to the canton’s 460,000 inhabitants. The health district’s annual population of children aged 0–15 years old was extracted from statistics published by the regional population office [10].
All files were identified via a computerised search using codes matching diagnoses containing the items femur and fracture. We focused on cases from 1997 to 2016 specifically because this was the time period for which it was possible to retrieve the data from computer files without the intermediate step of accessing medical paper files. However, data were only extracted from the inpatient database.
Data on patient demographics (age and sex), admission month, injury mechanism and trauma circumstances, associated lesions, open fractures, and pathological fractures were collected. Fractures were retrospectively classified according to their location (epiphyseal, physeal, metaphyseal or diaphyseal), the Salter–Harris classification for distal physeal fractures, the Delbet classification for femoral head and neck fractures, and, if the fracture was open, the Gustilo–Anderson classification. Trauma circumstances were divided into six groups: low-energy trauma (domestic accident in or around the house/at school), road accident, playful activities (swing, slide, trampoline, skateboarding or similar), sporting activities, falls from a height >2 m, and confirmed child abuse or iatrogenic (birth trauma). The fracture was considered pathological when it was caused by an underlying disease or medical condition. The results were then organised into four age groups: infants (<1 year old), preschool children (1–5 years old), primary school age children (6–11 years old) and teenagers (12–15 years old). These groups were chosen to facilitate comparisons with data in the existing literature and because of the different mechanisms of injury linked to age-related differences in children’s physical activities. The results were also analysed according to the season of the trauma. Seasonal fracture occurrence was grouped in winter (Dec–Feb), spring (Mar–May), summer (Jun–Aug) and autumn (Sep–Nov).
Data analysis and statistical analysis
Data were collected on patients’ demographical and epidemiological characteristics, on fracture-specific information including fracture location and fracture type, and on associated lesions. The results were subsequently interpreted, considering firstly all the patients together and then the four previously defined age groups. Statistical analyses were performed using R v.3.1.3 software and the RStudio interface (RStudio, Inc., Boston, MA, US). Chi squared statistical tests were used and the results were presented as n/total (%). For outcomes with significant effects (p <0.05), post-hoc analyses were performed with the Bonferroni correction (age group effect: p <0.008 (0.05/6), circumstances effect: p <0.003 (0.05/15)).
Results
Patients’ characteristics
The study included 348 children with 353 femoral fractures (fig. 1a, b). These patients were identified as being part of a mean community population of 76,840 children under 16 years old during the period studied (1997–2016). Thus, the average annual incidence of femoral fracture was 22.7 new cases per 100,000 children. Male patients suffered 240 fractures (69%), giving a male/female ratio of 2.2:1. We found an almost equal distribution of fractures between the right side (n = 176, 50.6%) and the left side (n = 167, 48.0%) and found no differences in laterality within the different age groups (fig. 1a). Bilateral fractures occurred in five cases (1.4%). The patient cohort’s mean age was 7.5 years (SD ±4.7; range 0–15 years); 37 children (10.6%) were younger than 1 year old, 112 (32.2%) were aged 1–5, 125 (35.9%) were aged 6–11, and the remaining 74 (21.3%) were teenagers (12–15 y/o). In children younger than 1 year old, there was a predominance of girls (25 cases; 68%), whereas females suffered four, three and six times fewer fractures than males in Groups II (1–5 years old), III (6–11 years old) and IV (12–15 years old), respectively.
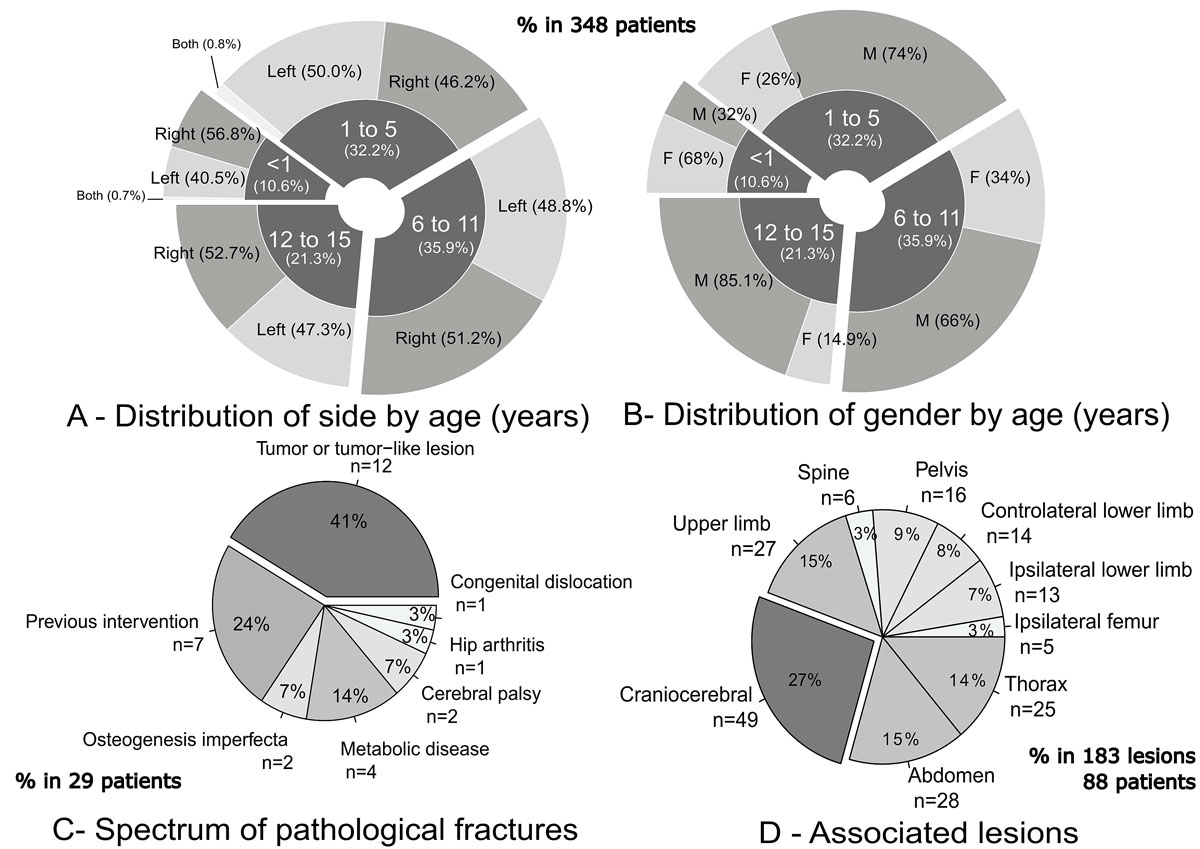
Figure 1 Demographic data of patients. Waddell’s triad, a triad of injuries associated with pedestrian–motor vehicle collisions, includes fractured femoral shaft, intra-thoracic or intra-abdominal injuries, and head injury. Patients with two fractures can be count twice for the associated lesions (183 lesions for 88 patients). Age is reported in years. F is female and M is male.
Seasonal variation and mechanisms of injury
Since 1997, the mean number of cases per year has been 17.5 (min = 10; max = 26), as reported in figure 2a.
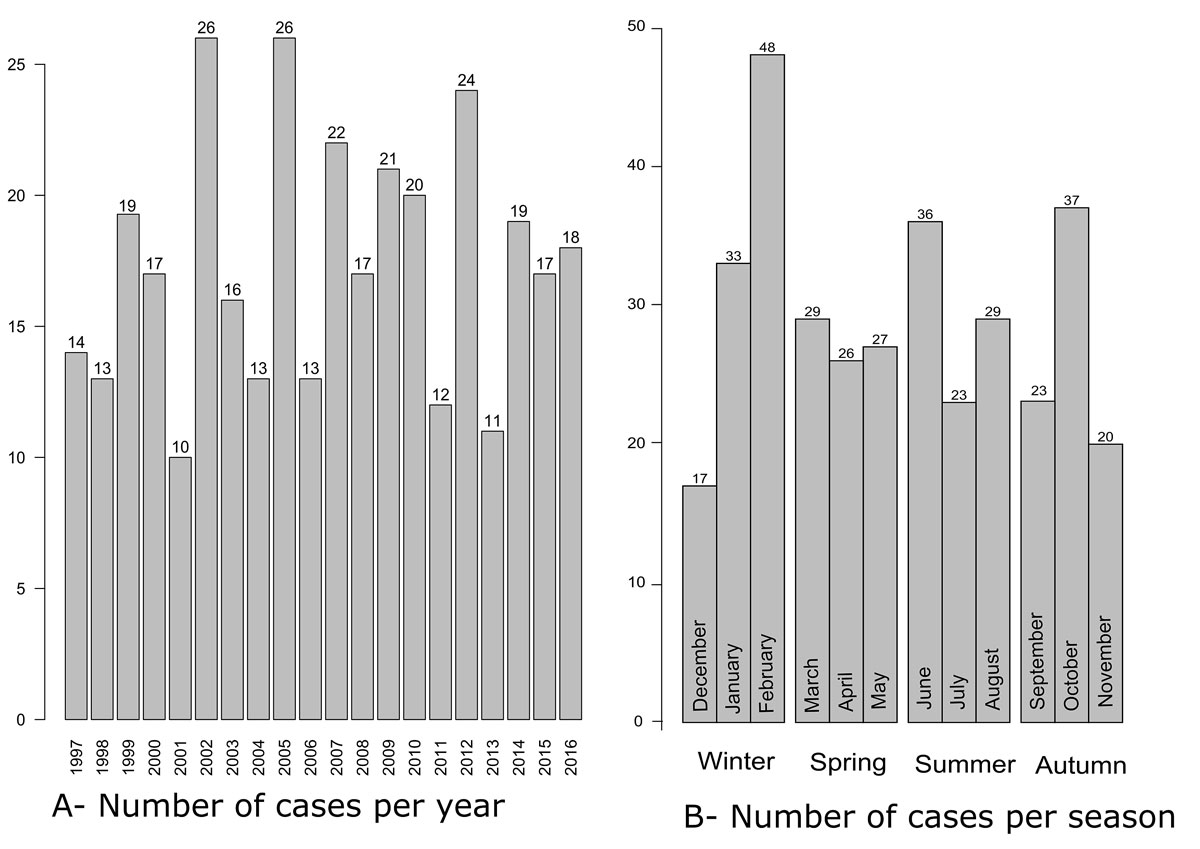
Figure 2 Evolution of number of cases over time (n = 348).
Of the 348 patients reviewed, the most common month was February (48 patients (13.7%)), followed by October (37 patients (10.6%)) and June (36 patients (10.3%)), as reported in figure 2b.
Winter was the peak season for fracture prevalence in children less than 1 year old and those aged 6–11 years old (37.8% and 46.4% respectively), whereas the peak season for children aged 1–5 years old was autumn (29.5%), and for the teenagers group it was spring (31.1%).
Injury mechanism was divided into six groups for analytical purposes (fig. 3a). Trauma mechanism was unknown in 62 cases (88 fractures). Overall, road accidents accounted for the largest percentage of fractures (88 fractures, 25.1%). Femoral fractures caused by low-energy trauma affected mostly children younger than 6 y/o (44% and 26% respectively in Groups I and II). Femoral fractures due to sports injuries were mostly seen in patients aged 6–11 years old (35% of fractures in group III), whereas in teenagers most femoral fractures were due to traffic accidents (37% of fractures in group VI; p <0.001). Confirmed child abuse (three cases; 9%) and birth trauma (two cases; 5%) contributed to 14% of the fractures in those younger than 1 year (p <0.001).
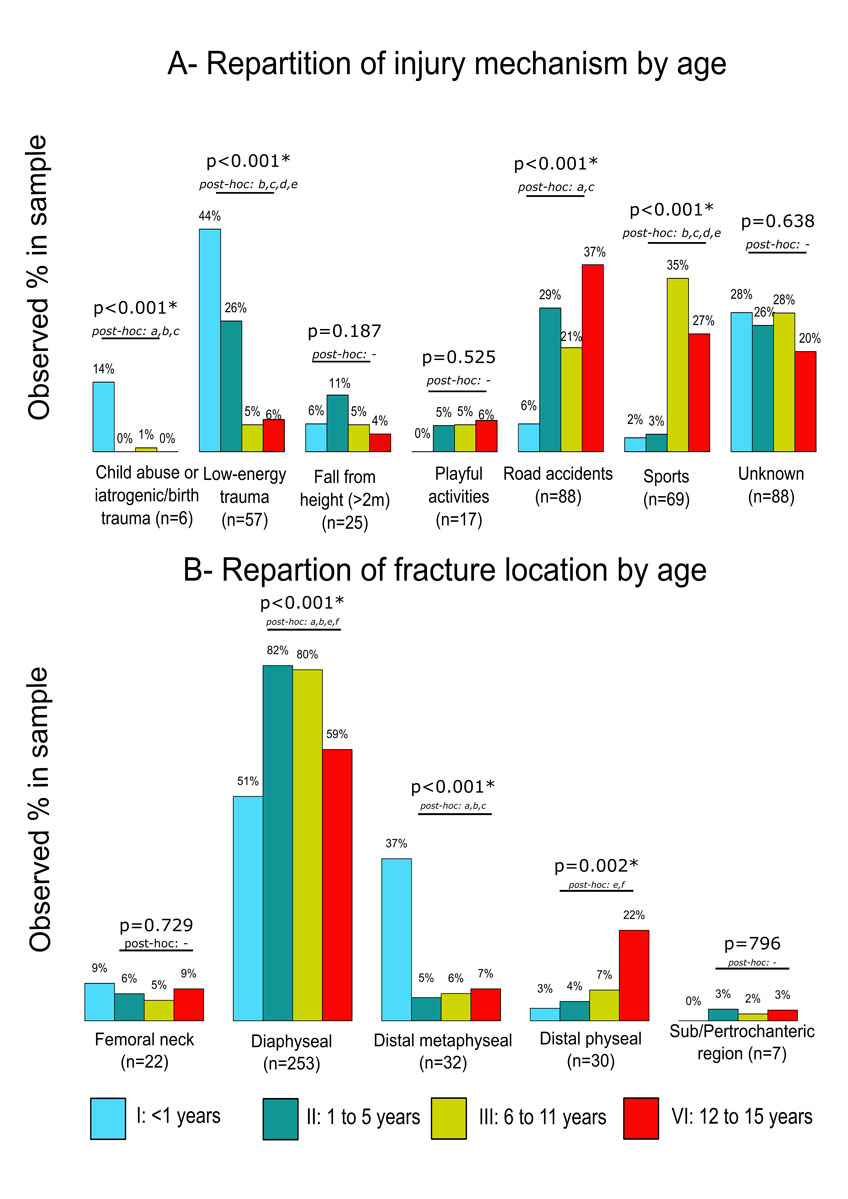
Figure 3 Comparison of age groups regarding distribution of injury mechanism and fracture location (A: n = 350 fractures, B: n = 344 fractures; due to missing information). Chi-square statistical tests were used and results are presented as n/total (%). Significant differences between groups were considered at p <0.05 level for global age effect and p <0.008 with the Bonferroni correction (0.05/6) for post-hoc analyses. Significant post-hoc analyses were represented as: a = I vs II, b = I vs III, c = I vs VI, d = II vs III, e = II vs VI, f = III vs VI
Most traffic accident victims (51.3%) suffered their femoral fracture in vehicle–vehicle collisions, followed by vehicle–pedestrian collisions (33.3%), and bicycle/motorcycle accidents (15.4%). Regarding age, older children (≥12 years old) were more likely to be injured in vehicle–vehicle collisions (55% of all motor vehicle collisions; p <0.001) and bicycle/motorcycle accidents (50%), whereas those between 6–11 years old made up most of the pedestrian injuries (53.8%).
When considering injury mechanisms by time of year, sport was the most common mechanism in winter (46% of all winter femoral fractures; p <0.001), road accidents were the most common mechanism in spring (31%), and low-energy traumas were the most common mechanism in autumn (29%) and summer (38%). The incidence of sports injuries was more than ten times higher in winter (77%) than in summer (6%). It is noteworthy that skiing injuries accounted for more than half the femoral fractures resulting from sporting activities in this series (48 cases, 69%).
Type of fracture
Three hundred and forty-three patients sustained unilateral femoral fractures, two had unilateral bi-focal fractures (a combination of mid-shaft fractures with physeal/metaphyseal fractures), and the remaining three had fractured both femurs. Of the 353 fractures, 255 (72.2%) affected the femoral shaft, 31 (8.8%) the distal metaphysis, 32 (9.1%) the distal femur physis, 22 (6.2%) the femoral neck and 7 (2.0%) the per/subtrochanteric region. Six (1.7%) medical records failed to report the fracture’s location. Types of fracture by patient age are reported in Figure 3b. Three hundred and forty-four femoral fractures (94.4%) were closed and 18 were open (5.1%). There were nine grade I, five grade II and four grade III open fractures. One medical record failed to report the open/closed fracture information.
Diaphyseal fractures represented more than 70% of the total: 51% in Group I, 82% in Group II, 80% in Group III and 59% in Group IV (fig. 3b). Thirty-seven percent of diaphyseal fractures were transverse (supplementary fig. S1a in appendix 1), 30.0% were spiral, 31.4% were oblique (fig. S1b), and only 1.3% were comminuted fractures. Spiral fractures were mostly observed in the 1–5 y/o group (35.4%), whereas transverse fractures were mostly seen in infants <1 year old (54.5%) and those 6 years old and older (43% in Group III and 70.5% in Group IV; p <0.001). Diaphyseal fracture was the most common type of fracture sustained by all mechanisms (fig. 4). Distal metaphyseal fractures were mainly observed in children less than 1 y/o (33%). Finally, distal physeal fractures (fig. S1c) occurred mostly during the growth spurt (mean age 12 years) and affected mainly males (male-to-female ratio of 5:1).
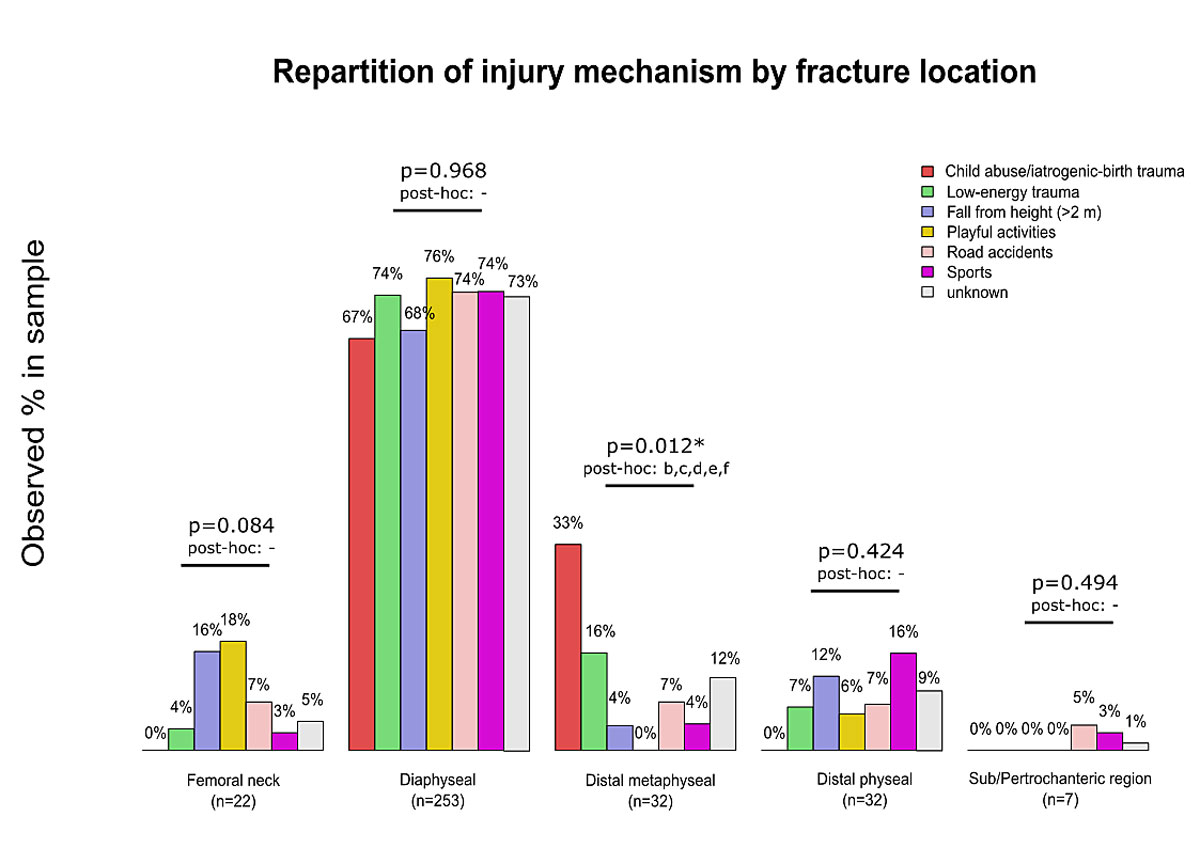
Figure 4 Comparison of injury mechanism considering type of fracture proportions (n=346 fractures due to seven cases with missing information). Chi-square statistical tests were used and results are presented as n/total (%). Significant differences between groups were considered at p <0.05 level for global age effect and p <0.003 with the Bonferroni correction (0.05/15) for post-hoc analyses. Significant post-hoc analyses were represented as: b = child abuse/iatrogenic birth trauma vs fall from height (>2 m), c = child abuse / iatrogenic birth trauma vs playful activities, d = child abuse / iatrogenic birth trauma vs road accidents, e = child abuse / iatrogenic birth trauma vs sports
Pathological fractures
Pathological fractures were observed in 29 cases (8.1%) and were located on the femoral shaft (13 cases), the distal metaphysis (6 cases), the femoral neck (5 cases) and the per/subtrochanteric region (5 cases). The most common mechanism of pathological fracture (17 cases) was low-energy trauma (58.6%); the aetiologies are listed in figure 1c.
Associated injuries and mortality rate
Of the 348 patients reviewed, 88 (25.3%) sustained a concomitant injury in addition to the femoral fracture (fig. 1d). Femoral neck fractures (fig. S1d I appendix 1) were often associated with pelvic fractures (9% of all associated injuries in femoral neck fractures). Most patients (12 cases) presenting with Waddell’s triad (a triad of injuries associated with pedestrian–motor vehicle collisions and including fractured femoral shaft, intra-thoracic or intra-abdominal injuries and head injury) were traffic accident victims: four pedestrians, six injured in motor vehicle collisions and two injured in bicycle/motorcycle accidents. The mortality rate associated with known femoral fracture was 1.1% (four cases). In this series, three patients died after traffic accidents resulting in a Waddell’s triad of injuries and the remaining patient died due to a metastatic Ewing sarcoma of the femur.
Discussion
The annual incidence of childhood femoral fractures in the Geneva health district (22.7 per 100,000) was 35–70% lower than in most previous studies (35–60 per 100,000) [6–8]. However, the reported incidence of femoral fracture may have been underestimated in this study since undisplaced fractures (especially in toddlers or in patients with osteogenesis imperfecta or cerebral palsy) are often managed in ambulatory care clinics. Also, many femoral fractures derived from skiing injuries were probably initially treated at the nearest medical centres. However, we noted that most of the children from the Geneva population with femoral fractures were transferred to our hospital either for surgery, for immediate postoperative re-education or for treatment follow-up. These cases were thus recorded, minimising this confounding bias.
Similarly to other studies [3–5, 9, 11, 12], our results show a male predominance, which is probably associated with more vigorous types of play and sports and with reinforced behaviours [13, 14].
Contrary to former studies, our results showed no bimodal age distribution, with the highest number of fractures in children aged 6–11 years old [1]. These fractures were derived mostly from sporting accidents, especially skiing injuries, which are specific to mountainous regions.
In our study, most femoral fractures occurred in winter, with peaks in January and, especially, February. These findings contradict the data of previous studies [6]. Winter sports are enjoyed and widely practiced throughout Switzerland, and thus the increase in the incidence of femoral fractures in the winter months reflects injuries related to sporting activities such as skiing and snowboarding.
The present study suggests that the most common mechanisms of injury were low-energy trauma (26.1%), ahead of road accidents (20.9%) and sports-related accidents (20.4%). This confirms the theory that environmental factors are more important than endogenous factors for the risk of fracture [15, 16].
In agreement with previous studies, femoral shaft fractures were the most commonly diagnosed femoral fracture in all age groups (72.2%) [3, 4]. The prevalence of open fractures was 5.4% of all femoral fractures, which supports the notion that open femoral fractures are uncommon in children [17, 18].
Our results show that distal physeal fractures were rare, representing less than 10% of all femoral fractures, and were usually due to high-energy trauma in school-age patients and to sports-related injuries in teenagers [19].
The main aetiology behind the 29 pathological femoral fractures treated in our institution over the 27-year period was benign tumours or tumour-like conditions (41.0%), typical of pathological paediatric bone fractures [20]. As mentioned before, these incidences might be underestimated in this study since undisplaced fractures in patients with osteogenesis imperfecta or cerebral palsy are often managed in ambulatory care clinics. Thus, osteogenesis imperfecta and cerebral palsy are considered risk factors for fractures, and dedicated recommendations for medical staff to prevent fractures in these patients are merited [21].
The incidence of associated injuries among the children in our cohort was within the range of 20–40% reported previously [7, 8, 22]. Craniocerebral injuries were the most common associated injuries in this case series (27%), followed by abdominal (15%) and thoracic injuries (14%). These data confirm the results of other studies [23]. Interestingly, 95% of open femoral fractures were associated with additional injuries, and 70% of these were due to a vehicle-related trauma mechanism. Considering the lesions mentioned above is crucial, since the presence of a head or thoracic injury has been demonstrated to be associated with higher mortality [24]. We found Waddell’s triad in 18.7% of all cases of femoral fractures with associated injuries. Thus, in children with femoral fractures resulting from a high-impact mechanism, it is strongly recommended to carefully check the head, chest and abdomen, since the rapid detection and adequate treatment of severe injuries associated with these areas improves patient outcome and reduces mortality.
The mortality rate of children with femoral fractures was 1.1% in our study, and 75% of these fatalities were associated with concomitant injuries, which is consistent with previous findings [25].
Femoral fractures in very young patients, especially before they are able to walk, may suggest physical child abuse [26]. In our study, femoral fractures due to abuse were only diagnosed in three patients aged less than six months (9% of this youngest group of patients). Since Leventhal et al. found that the incidence of femoral fractures due to abuse was 15.3–36.1 cases per 100,000 children [27], in agreement with Loder et al. [3], we suspect that the true number is probably higher, due to the difficulty in diagnosing this. Thus, attention must be paid to caregivers’ explanations of events in order to differentiate fabrications from true descriptions of actual mishaps [28].
In conclusion, the present study represents a large, retrospective, consecutive-case series on femoral fractures affecting a paediatric population. The large cohort of children and teenagers constitutes the study’s core strength, whereas its main limitations are its retrospective and observational nature. A further limitation is the small sample sizes in the subgroup analyses, making these analyses less reliable. The circumstances of injury and the seasonality of femoral fractures differ significantly with regard to the age of the child. Femoral fractures were mainly due to low-energy trauma in neonates and infants, road accidents and low-energy trauma in preschool children, sports accidents in school-age children, and road traffic accidents in teenagers. There may be regional differences regarding the sports practiced (skiing in our region), the traffic situation and the driving age in the studied area. Moreover, the morbidity of femoral fractures in children was closely correlated with associated injuries. Some fractures could probably be avoided, and we expect that the results of this work will be helpful for establishing recommendations for the prevention of femoral fractures in childhood.
Anne Tabard-Fougère, MD, Geneva University Hospital, 6 Rue Willy Donzè, CH-1211 Geneva 14, anne.tabard[at]hcuge.ch
Reference
1Beaty J, Kasser J. Rockwood and Wilkins’ Fractures in Children (6th Edition). Philadelphia, PA: Lippincott Williams & Wilkins: 2006.
2
Hunter
JB
. Femoral shaft fractures in children. Injury. 2005;36(Suppl 1):S86–93. doi:.https://doi.org/10.1016/j.injury.2004.12.018
3
Loder
RT
,
O’Donnell
PW
,
Feinberg
JR
. Epidemiology and mechanisms of femur fractures in children. J Pediatr Orthop. 2006;26(5):561–6. doi:.https://doi.org/10.1097/01.bpo.0000230335.19029.ab
4
Rewers
A
,
Hedegaard
H
,
Lezotte
D
,
Meng
K
,
Battan
FK
,
Emery
K
, et al.
Childhood femur fractures, associated injuries, and sociodemographic risk factors: a population-based study. Pediatrics. 2005;115(5):e543–52. doi:.https://doi.org/10.1542/peds.2004-1064
5
Hinton
RY
,
Lincoln
A
,
Crockett
MM
,
Sponseller
P
,
Smith
G
. Fractures of the femoral shaft in children. Incidence, mechanisms, and sociodemographic risk factors. J Bone Joint Surg Am. 1999;81(4):500–7. doi:.https://doi.org/10.2106/00004623-199904000-00007
6
Landin
LA
. Epidemiology of children’s fractures. J Pediatr Orthop B. 1997;6(2):79–83. doi:.https://doi.org/10.1097/01202412-199704000-00002
7
Buess
E
,
Kaelin
A
. One hundred pediatric femoral fractures: epidemiology, treatment attitudes, and early complications. J Pediatr Orthop B. 1998;7(3):186–92. doi:.https://doi.org/10.1097/01202412-199807000-00002
8
Vetti
N
,
Lindtjørn
B
,
Engesaeter
LB
. [406 femoral fractures in children]. Tidsskr Nor Laegeforen. 1998;118(22):3415–8. Article in Norwegian.
9
Galano
GJ
,
Vitale
MA
,
Kessler
MW
,
Hyman
JE
,
Vitale
MG
. The most frequent traumatic orthopaedic injuries from a national pediatric inpatient population. J Pediatr Orthop. 2005;25(1):39–44.
10Republique et canton de Geneve. [Statistiques cantonales]. http://www.ge.ch/statistique/population_residante/welcome.asp.
11
Heideken
J
,
Svensson
T
,
Blomqvist
P
,
Haglund-Åkerlind
Y
,
Janarv
PM
. Incidence and trends in femur shaft fractures in Swedish children between 1987 and 2005. J Pediatr Orthop. 2011;31(5):512–9. doi:.https://doi.org/10.1097/BPO.0b013e31821f9027
12
Joeris
A
,
Lutz
N
,
Wicki
B
,
Slongo
T
,
Audigé
L
. An epidemiological evaluation of pediatric long bone fractures - a retrospective cohort study of 2716 patients from two Swiss tertiary pediatric hospitals. BMC Pediatr. 2014;14(1):314. doi:.https://doi.org/10.1186/s12887-014-0314-3
13
Garner
MR
,
Bhat
SB
,
Khujanazarov
I
,
Flynn
JM
,
Spiegel
D
. Fixation of length-stable femoral shaft fractures in heavier children: flexible nails vs rigid locked nails. J Pediatr Orthop. 2011;31(1):11–6. doi:.https://doi.org/10.1097/BPO.0b013e31820321ab
14
Ma
D
,
Jones
G
. Television, computer, and video viewing; physical activity; and upper limb fracture risk in children: a population-based case control study. J Bone Miner Res. 2003;18(11):1970–7. doi:.https://doi.org/10.1359/jbmr.2003.18.11.1970
15
Hedlund
R
,
Lindgren
U
. The incidence of femoral shaft fractures in children and adolescents. J Pediatr Orthop. 1986;6(1):47–56. doi:.https://doi.org/10.1097/01241398-198601000-00010
16
Miettinen
H
,
Mäkelä
EA
,
Vainio
J
. The incidence and causative factors responsible for femoral shaft fractures in children. Ann Chir Gynaecol. 1991;80(4):392–5.
17
Dodd
A
,
Paolucci
EO
,
Parsons
D
. Paediatric femoral shaft fractures: what are the concomitant injuries?
Injury. 2013;44(11):1502–6. doi:.https://doi.org/10.1016/j.injury.2013.02.012
18
Hutchins
CM
,
Sponseller
PD
,
Sturm
P
,
Mosquero
R
. Open femur fractures in children: treatment, complications, and results. J Pediatr Orthop. 2000;20(2):183–8. doi:.https://doi.org/10.1097/01241398-200003000-00010
19
Garrett
BR
,
Hoffman
EB
,
Carrara
H
. The effect of percutaneous pin fixation in the treatment of distal femoral physeal fractures. J Bone Joint Surg Br. 2011;93-B(5):689–94. doi:.https://doi.org/10.1302/0301-620X.93B5.25422
20
De Mattos
CB
,
Binitie
O
,
Dormans
JP
. Pathological fractures in children. Bone Joint Res. 2012;1(10):272–80. doi:.https://doi.org/10.1302/2046-3758.110.2000120
21
Huh
SY
,
Gordon
CM
. Fractures in hospitalized children. Metabolism. 2013;62(3):315–25. doi:.https://doi.org/10.1016/j.metabol.2012.07.018
22
Taylor
MT
,
Banerjee
B
,
Alpar
EK
. The epidemiology of fractured femurs and the effect of these factors on outcome. Injury. 1994;25(10):641–4. doi:.https://doi.org/10.1016/0020-1383(94)90003-5
23
Sala
D
,
Fernández
E
,
Morant
A
,
Gascó
J
,
Barrios
C
. Epidemiologic aspects of pediatric multiple trauma in a Spanish urban population. J Pediatr Surg. 2000;35(10):1478–81. doi:.https://doi.org/10.1053/jpsu.2000.16418
24
Peclet
MH
,
Newman
KD
,
Eichelberger
MR
,
Gotschall
CS
,
Guzzetta
PC
,
Anderson
KD
, et al.
Patterns of injury in children. J Pediatr Surg. 1990;25(1):85–90, discussion 90–1. doi:.https://doi.org/10.1016/S0022-3468(05)80169-1
25
Baldwin
K
,
Pandya
NK
,
Wolfgruber
H
,
Drummond
DS
,
Hosalkar
HS
. Femur fractures in the pediatric population: abuse or accidental trauma?
Clin Orthop Relat Res. 2011;469(3):798–804. doi:.https://doi.org/10.1007/s11999-010-1339-z
26
Paddock
M
,
Sprigg
A
,
Offiah
AC
. Imaging and reporting considerations for suspected physical abuse (non-accidental injury) in infants and young children. Part 1: initial considerations and appendicular skeleton. Clin Radiol. 2017;72(3):179–88. doi:.https://doi.org/10.1016/j.crad.2016.11.016
27
Leventhal
JM
,
Martin
KD
,
Asnes
AG
. Incidence of fractures attributable to abuse in young hospitalized children: results from analysis of a United States database. Pediatrics. 2008;122(3):599–604. doi:.https://doi.org/10.1542/peds.2007-1959
28
Pierce
MC
,
Bertocci
GE
,
Janosky
JE
,
Aguel
F
,
Deemer
E
,
Moreland
M
, et al.
Femur fractures resulting from stair falls among children: an injury plausibility model. Pediatrics. 2005;115(6):1712–22. doi:.https://doi.org/10.1542/peds.2004-0614