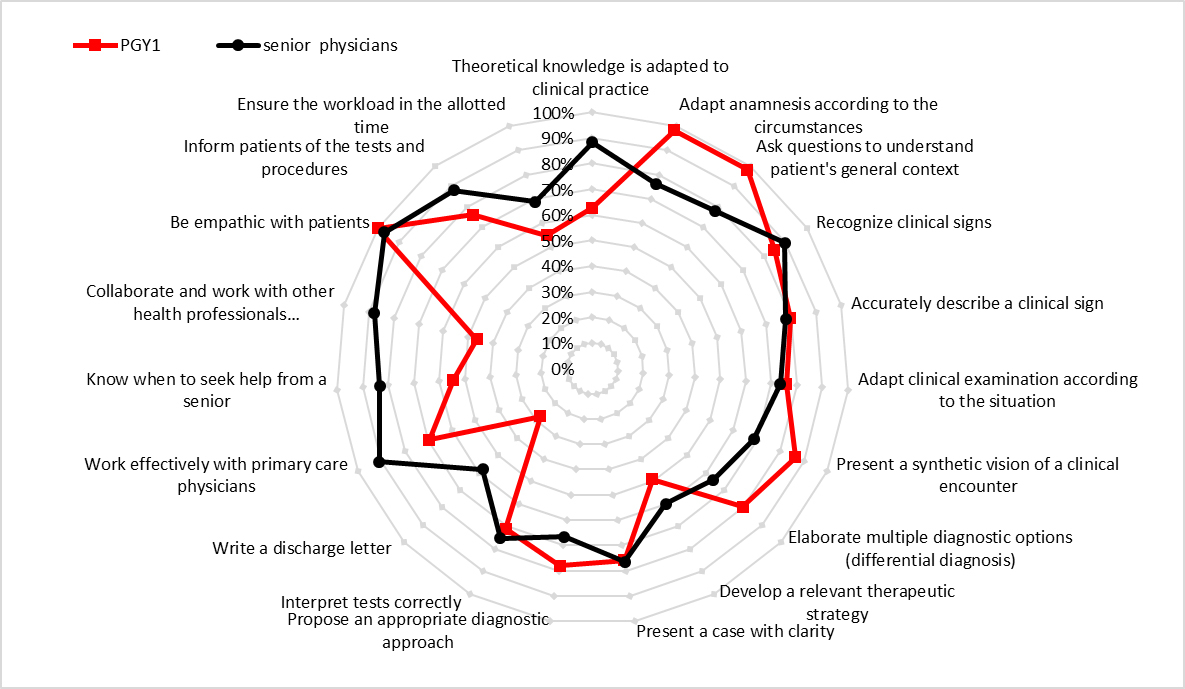
Figure 1 Comparison of residents’ and senior physicians’ perception of performance.
DOI: https://doi.org/10.4414/smw.2020.20370
A key role of medical schools is to train medical students so that they are ready to practice within a postgraduate training program [1, 2]. Lately, medical schools have focused their curricula towards the acquisition of predetermined competences, with the aim of preparing physicians for postgraduate practice [3, 4]. Nevertheless, the transition from being a medical student to residency remains difficult for young physicians. Various international studies exploring young graduates’ perceptions of their preparedness have shown that several aspects of clinical practice are not sufficiently addressed by current curricula [2, 5–13].
Our study follows a period of curricular reforms, triggered by the creation in 2001 of the first catalogue of study objectives, named Swiss Catalogue of Learning Objectives (SCLO) for Undergraduate Medical Education. The SCLO defines the level to be attained by the end of undergraduate training and the content of the new federal licensing exam (2011) [14, 15]. Under the new Federal Act on University Medical Professions (2007), adherence to the document also became an essential prerequisite for the accreditation of the curricula of the five Swiss medical faculties [14, 16]. The SCLO was heavily redesigned in 2008, incorporating the concept of competency-based medical education and the CanMEDS framework [17].
In order to meet these new standards and requirements, all Swiss medical schools have engaged in a first wave of curriculum reforms. The Lausanne School of Medicine moved from a traditional, six-year, discipline-, hospital-, and lecture-based curriculum to a more transdisciplinary, integrated and system-based curriculum. The new curriculum was aligned with the Bologna system, corresponding to a three-year bachelor’s part followed by a three-year master’s part [18]. A transdisciplinary committee created a new clinical skills curriculum, starting in the second year of the bachelor’s, along with an immersion in the clinical environment starting in the third year of the bachelor’s. In all Swiss medical schools, new teaching approaches have been introduced at various stages. These include systematic simulation-based learning sessions (role-play, mannequins, simulated patients), the inclusion of objective structured clinical examinations, and an increased number of periods of clinical immersion.
This paper presents the results of a quantitative and qualitative survey of junior residents and senior physicians from all 13 postgraduate training hospitals of the canton of Vaud (Switzerland). The paper explores the range of situations in which graduates felt less competent and assesses the reasons behind these perceptions.
At a time when Swiss medical faculties are facing a new phase of reforms, triggered by the publication in 2018 of the new national framework for undergraduate medical education (“PROFILES”) [19], we deem it useful to present the experience of the Lausanne School of Medicine and to analyse the successes and failures of the previous reform phase.
A cross-sectional, triangulation mixed-methods study was performed between September 2012 and April 2013. The study integrated qualitative and quantitative data to expand, cross-check and corroborate its results [20]. The data used for analysis originated from questionnaire surveys and six focus groups, performed in two convenience samples. The first sample included junior residents who graduated from the Lausanne School of Medicine under the reformed study curriculum. As evidence exists that new graduates experience performance stress, moral distress and discouragement during the initial months of their professional practice in acute care [21], we selected residents in their first 6-12 months of postgraduate training. This is a phase in which performance in the workplace still depends to a large extent on the skills and knowledge acquired during formal studies. The second sample contained senior physicians and heads of departments of the Lausanne University Hospital and the 12 regional hospitals of the canton of Vaud, where the vast majority of graduates from Lausanne begin their postgraduate training.
A committee composed of the director of the medical school, representatives of regional hospital departments and the president of the local branch of the medical residents association (l'Association Suisse des Médecin(e)s Assistants et Chef(fe)s de Clinique, section Vaud, ASMAV), as well as a resident and a medical student, created both questionnaires. These were then tested for content validity by a committee composed of the associate dean for education, senior physicians, and a group of residents and medical students. The resulting 28-item residents’ questionnaire and 26-item senior physicians’ questionnaire were designed to explore four domains of competence: (1) theoretical knowledge; (2) clinical skills; (3) collaboration and relational skills; and (4) self-confidence and ability to cope with the daily work. All items were answered on a four-point Likert response scale, ranging from 1, “not at all prepared” to 4, “fully prepared”. The value 0 was assigned to the answer “not applicable”. Demographic data were also collected.
Both questionnaires were administered using the open-source statistical survey web application LimeSurvey®. The link to the questionnaires was sent to participants by e-mail. The e-mail addresses of the cohort of graduates were provided by the students’ affairs bureau of the medical school. The e-mail addresses of the heads of departments, available on the corresponding hospital websites, were searched for manually. Since the data from the completed questionnaires were fully anonymous, no follow-up of nonrespondents was possible. We therefore opted for a second general reminder.
The data from the questionnaires were analysed using STATA 12 software (StataCorp LLC, Texas, USA). In addition to descriptive statistics, each item was adjusted for respondents’ “gender” and “clinical setting” using ordinal logistic regression. Three categories of “clinical setting” were created: “internal medicine,” “surgery” and “other” (including anaesthesiology, gynaecology, paediatrics, psychiatry, radiology and emergency medicine) Frequencies of positive responses to items in the two questionnaires were compared using Pearson’s chi-square or Fisher’s exact test.
The qualitative part of the study was carried out through focus groups (FGs) involving first-year postgraduate residents who had graduated from our university and who agreed to participate in the study after telephone and email contact. The sessions, which lasted about 60 minutes, were audio-recorded and transcribed verbatim. Two authors (LB, MM) developed the focus group guide and ran the focus group sessions. The focus group sessions were semi-structured, with an initial open discussion about experiences during the first few months of work. Participants were invited to describe aspects of their work for which they felt prepared and those for which they felt poorly prepared. They were encouraged to share concrete situations that illustrated their perceptions. In the second, more structured part of the session, each participant received a set of cards describing the seven roles that make up the CanMEDS framework, which inspired the Swiss model of medical competences [14]. Moderators then asked participants to order the cards by level of perceived mastery of these roles and invited the participants to explain and discuss their choices. Analysis of the verbatim transcripts was performed using a thematic analysis approach [22]. The generation of codes and identification of themes were performed independently by two authors (LB, MM). Discrepancies were discussed until a consensus was reached.
The research was exempted from approval by the local ethics committee because under Swiss law, approval is not required for studies in which non-personal health-related data are collected [23]. Participants signed a consent form and were informed that the data would be analysed anonymously.
Of the 136 residents invited to complete the cohort questionnaire, 59 (43.4%) had fully completed it after one reminder. Of the 257 questionnaires sent to senior physicians, 68 (26.5%) were completed. Demographic characteristics of the respondents are summarised in table 1. Sixty-four residents were female, a percentage reflecting the male-to-female ratio among graduating students. Most residents worked in internal medicine (49.2%) and surgical (32.2%) departments. Tables 2 and 3 and figure 1 summarise the responses by residents and senior physicians. Since respondents in the senior physicians’ questionnaire assessed the performance of a group of physicians, while respondents in the residents’ questionnaire evaluated their individual performance, an item-to-item comparison of the results of the two questionnaires was not possible. Therefore, to allow for comparison we converted the categorical data into binary variables. Frequencies represent the percentage of respondents who “rather or strongly agreed” or felt "“rather or very well prepared” (scores 3 and 4 on the four-point Likert scales).
Figure 1 Comparison of residents’ and senior physicians’ perception of performance.
Table 1 Demographics of first-year postgraduate (PGY1) residents and senior physicians.
| PGY1 (n = 59) | Senior physicians (n = 68) | |
|---|---|---|
| Male | 21 (35.6%) | 60 (88.2%) |
| Female | 38 (64.4%) | 8 (11.8%) |
| Under 25 years | 2 (3.4%) | 0 |
| 25–30 years | 56 (94.9%) | 0 |
| 31–40 years | 1 (1.7%) | 10 (14.7%) |
| 41–50 years | 0 | 24 (35.3%) |
| 51–60 years | 0 | 26 (38.3%) |
| Over 61 years | 0 | 8 (11.8%) |
| Internal medicine | 29 (49.2%) | 23 (33.8%) |
| Surgery | 19 (32.2%) | 16 (23.5%) |
| Paediatrics | 4 (6.8%) | 7 (10.3%) |
| Other | 7 (11.9%)* | 22 (32.4%)† |
* Anaesthesia: 1.7%, psychiatry: 3.4%, other: 6.78% † Anaesthesia: 11.8%; gynaecology: 4.4%; psychiatry: 4.4%; radiology: 2.9%; emergency: 2.9%; other: 5.6%
Table 2 First-year postgraduate (PGY1) residents’ assessment of their competences as “well or rather well mastered”.
| Respondents (max = 59) | PGY1 residents % (95% CI) | |
|---|---|---|
| A. Theoretical knowledge | ||
| 1. Knowledge base is adapted to clinical practice | 59 | 62.7 (49.1–75) |
| 2. Knowledge is mainly theoretical and difficult to apply in practice | 59 | 69.5 (56.1–80.8) |
| 3. Theoretical knowledge is incomplete | 57 | 49.1 (35.6–62.7) |
| B. Clinical skills | ||
| B.1. History taking | ||
| 4. Adapt the anamnesis according to the circumstances | 58 | 98.3 (90.8–100) |
| 5. Ask questions to understand the patient’s general context | 58 | 98.3 (90.8–100) |
| B.2. Physical examination | ||
| 6. Recognise clinical signs | 59 | 84.7 (73–92.8) |
| 7. Accurately describe a clinical sign | 59 | 79.7 (67.2–89) |
| 8. Adapt the clinical examination according to the situation | 58 | 75.9 (62.8–86.1) |
| B.3. Clinical reasoning | ||
| 9. Present a synthetic vision of a clinical encounter | 59 | 86.4 (75–94) |
| 10. Elaborate multiple diagnostic options (differential diagnosis) | 59 | 79.7 (67.2–89) |
| 11. Develop a relevant therapeutic strategy | 59 | 49.2 (35.9–62.5) |
| 12. Present a case with clarity | 58 | 75.9 (62.8–86.1) |
| 13. Propose an appropriate diagnostic approach | 59 | 78 (65.3–87.7) |
| 14. Interpret tests correctly | 59 | 71.2 (57.9–82.2) |
| 15. Write a discharge letter | 58 | 27.6 (16.7–40.9) |
| C. Collaboration and relational skills | ||
| 16. Working effectively with primary care physicians | 59 | 69.5 (56.1–80.8) |
| 17. Know when to seek help from a senior | 57 | 54.4 (40.7–67.6) |
| 18. Collaborate with nursing staff | 58 | 69.5 (56.1–80.8) |
| 19. Collaborate and work with other health professionals (physiotherapy, occupational therapy, social services) | 58 | 46.6 (33.3–60.1) |
| 20. Discuss difficult topics with a patient, such as breaking bad news | 59 | 74.6 (61.6–85) |
| 21. Be empathic with patients | 59 | – |
| 22. Inform patients of the tests and procedures | 58 | 75.9 (62.8–86.1) |
| 23. Conducting an interview with family members | 58 | 48.3 (35–61.8) |
| 24. Deal with ethical and confidentiality questions | 59 | 91.5 (81.3 – 97.2) |
| D. Self-confidence and coping with the daily work | ||
| 25. Complete the workload in the allotted time | 59 | 54.2 (40.8–67.3) |
| 26. Feeling fulfilled at work | 59 | 61 (47.4–73.5) |
| 27. Feeling overwhelmed | 59 | 50.8 (37.5–64.1) |
| 28. Undergraduate training is adapted to clinical practice | 59 | 54.2 (40.8–67.3) |
Numbers in bold text indicate competencies in which <70% PGY1 residents considered themselves proficient.
Table 3 Senior physicians’ assessment of residents’ competences as “well or rather well mastered”.
| Respondents (max = 68) | Senior physicians % (95% CI) | |
|---|---|---|
| A. Theoretical knowledge | ||
| 1. Knowledge base is adapted to clinical practice | 68 | 88.2(78.1–94.8) |
| B. Clinical skills | ||
| B.1. History taking | ||
| 2. Adapt the anamnesis according to the circumstances | 67 | 76.1 (64.1–85.7) |
| 3. Take a structured anamnesis | 67 | 92.5 (83.4–97.5) |
| 4. Ask questions to understand the patient’s general context | 68 | 77.9. (66.2–87.1) |
| B.2. Physical examination | ||
| 5. Search for clinical signs | 67 | 88.1 (77.8–94.7) |
| 6. Recognise clinical signs | 67 | 89.6 (79.7–95.7) |
| 7. Accurately describe a clinical sign | 68 | 77.9 (66.2–87.1) |
| 8. Adapt the clinical examination according to the situation | 68 | 73.5 (61.4–83.5) |
| B.3. Clinical reasoning | ||
| 9. Present a synthetic vision of a clinical encounter | 67 | 68.7 (56.2–79.4) |
| 10. Elaborate multiple diagnostic options (differential diagnosis) | 67 | 64.2 (51.5–75.5) |
| 11. Develop a relevant therapeutic strategy | 64 | 60 (47.1–72) |
| 12. Present a case with clarity | 68 | 76.5 (64.6–85.9) |
| 13. Propose an appropriate diagnostic approach | 66 | 66.7 (54–77.8) |
| 14. Interpret tests correctly | 65 | 75.4 (63.1–85.2) |
| 15. Write a discharge letter | 62 | 58.1 (44.8–70.5) |
| 16. Connect theoretical knowledge and clinical findings | 68 | 79.4 (67.9–88.3) |
| C. Collaboration and relational skills | ||
| 17. Working effectively with primary care physicians | 66 | 90.9 (81.3–96.6) |
| 18. Do not seek help from a senior when it is needed | 67 | 16.7 (8.6–27.9) |
| 19. Collaborate and work with other health professionals (physiotherapy, occupational therapy, social services) | 66 | 87.9 (77.5–94.6) |
| 20. Be empathic with patients | 67 | 97 (89.6–99.6) |
| 21. Inform patients of the tests and procedures | 67 | 88.1 (77.8–94.7) |
| 22. Consider the global context of the patient | 67 | 85.1 (74.392.6) |
| D. Self-confidence and coping with the daily work | ||
| 23. Complete the workload in the allotted time | 67 | 68.7 (56.2–79.4) |
| 24. Consider feedback from superiors | 66 | 97 (89.5–99.6) |
| 25. Be able to be self-critical | 65 | 90.8 (81–96.5) |
| 26. To have gained the trust of the service | 65 | 96.9 (89.3–99.6) |
Six focus groups were conducted with 19 residents (7 men, 12 women) working in six different hospitals and four departments (internal medicine, surgery, rehabilitative medicine and paediatrics) between November 2012 and April 2013. Figure 2 shows the residents’ perceived proficiencies in the seven CanMEDS roles. Hereafter, we integrate quantitative and qualitative findings on the six themes that emerged from thematic analysis of the transcripts.
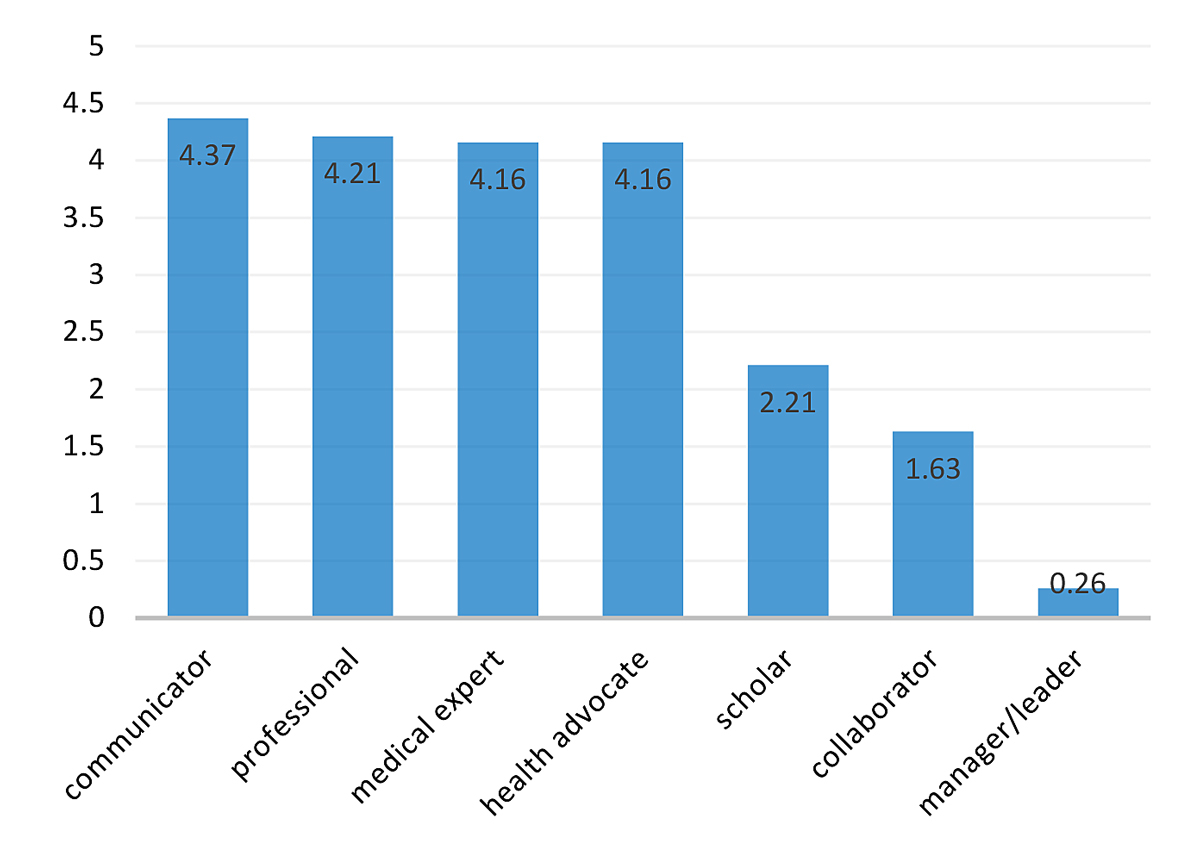
Figure 2 Residents’ ranking of their perceived proficiency of each CanMEDS role. Values correspond to the average score of the rankings (19 observations): 6 = best mastered role; 0 = least mastered role.
Large majorities of residents considered themselves capable of accurately carrying out a medical history (98.3%), identifying clinical signs (84.7%) and dealing with ethical and confidentiality problems (91.5%). Senior physicians confirmed that these skills are well-mastered by junior residents (table 3, questions 3, 5, 6, 20) and that residents’ knowledge base is adapted for entering postgraduate training (table 3, question 1). The focus groups corroborated these statements:
Regarding their ability in developing differential diagnoses, residents considered themselves more competent than their supervisors assume (fig. 1). Adjustments for gender and clinical setting do not show statistically significant differences.
Residents reported a mismatch between the subject matter taught during studies and the knowledge relevant for clinical practice:
The ability to propose appropriate therapeutic strategies, in particular drug prescription, was described as poorly mastered (49.2% of residents, 60% of senior physicians). In this area, residents considered the teaching received as very specific but not sufficiently practice-oriented:
Similarly, when considering the reality of everyday clinical practice, they lamented that the undergraduate curriculum emphasises rare conditions at the expense of common diseases:
Important skills for everyday practice, such as correct interpretation of X-rays or of ECGs, also seem to be poorly mastered. Similarly, residents reported a lack of structured and systematic training concerning invasive procedures, with this training instead occurring opportunistically, mostly during the final-year internships:
Internships were considered a key step in training, where a learned topic finally takes on its full meaning. They were nevertheless described as too disparate in quality, too opportunistic, and too dependent on the training site or the abilities and goodwill of the designated supervisor. Residents suggested a more active involvement of the medical school in the governance of the learning objectives and in the various hospitals which provide internships. Moreover, despite being offered the opportunity to be personally in charge of patients, interns often assumed a relatively passive, “student” role.
All these points could explain why only 54.2% (95% confidence interval 40.8-67.3) of residents considered undergraduate training to have prepared them adequately for postgraduate practice.
According to the CanMEDS definition, “as collaborators, physicians work effectively in a health care team to provide optimal patient care”. This competence was described as seldom formally imparted during medical studies, and many participants felt underprepared in collaborating with nurses (69.5%) or with other health professionals (53.4%). They stressed how an incomplete knowledge of the roles and competences of other health professionals could lead to difficulties in collaboration:
In general, residents considered themselves well-prepared in this field. The teaching of communication with patients was unanimously judged as one of the strengths of our university. Simulation-based, hands-on teaching about communication in difficult situations, such as a “motivational interview” or “breaking bad news”, were deemed particularly useful. Difficulties were, however, found in concisely and coherently summarising a patient encounter to the supervisor or in writing a discharge letter (fig. 1):
The SCLO states that “as scholars, physicians demonstrate a lifelong commitment to reflective learning, as well as the creation, dissemination, application and translation of medical knowledge” [14]. In this area, participants considered the undergraduate curriculum deficient in preparing them for searching and critically appraising the literature (fig. 1 and fig. 2). The mandatory master’s thesis research project was mentioned as one of the rare opportunities for the student to independently search for information and develop critical thinking skills. The prevalence of classroom lectures was perceived as preventing the autonomy that students need when seeking new knowledge at postgraduate level:
Residents’ difficulties in managing their workload within the allotted time were widely reported, both by senior physicians and by the residents themselves (fig. 1 and fig. 2). The program’s neglect of administrative skills despite their importance in practice reportedly leads to anxiety and frustration:
Half of the resident respondents reported feeling overwhelmed. The first three months of residency were described as particularly difficult and distressing. Residents reported a lack of self-confidence, which was also associated with a sense of anxiety and a fear of making mistakes. Moreover, fear and stress seem to be taboo topics of discussion in the hospital setting:
Working in emergency wards and night shifts were described as particularly stressful and associated with anxiety. Residents become responsible for decisions they must take with little or no supervision. They felt unprepared and lacked the self-confidence for this. In the first month of residency, these negative feelings persist even at home:
This cross-sectional, mixed-methods study describes the perceptions of preparedness for practice of junior residents and of their supervisors after a major curriculum change. This study also illustrates the strengths and weaknesses of the curriculum and the reforms undertaken at the Lausanne School of Medicine. Our results highlight six major areas of perceived underpreparedness. Junior residents felt insufficiently prepared to manage daily clinical work, to communicate with colleagues, to work efficiently within an interprofessional team, and to engage in critical inquiry and self-directed learning. They argued that instructional approaches do not align well with the postgraduate learning environment. The first few months of work were often associated with negative emotions.
Among areas of perceived proficiency, junior residents and heads of hospital departments both mentioned the knowledge bases and basic clinical skills (history taking, clinical examination, communication with patients). Commenting on curricular choices, however, residents regretted the overemphasis on rare diseases at the expense of conditions more frequently encountered in their daily activities. This created a sense of frustration and discomfort when facing difficulties in the management of common diseases. Difficulties were also reported in important and very practical aspects of daily patient care, such as prescribing specific pharmacological treatments, interpreting electrocardiograms and radiological investigations, managing emergency situations, setting and following priorities, and working within an interprofessional team. Our findings are in line with those of a recent systematic review where junior graduates perceived skills such as prescribing, decision making, treatment planning, managing stress in the workplace, team-working, interpersonal skills and performing clinical procedures as lacking [13]. In a survey of 640 German junior physicians, Ochsmann et al. reported that 60% of them felt ill-prepared in the first two years of postgraduate training [6]. Illing et al. compared the perceptions of graduates from three UK medical schools with very different curricula and highlighted very similar areas of underpreparedness in the management of acute situations, in drug prescribing, and in workload management [24]. The difficulties highlighted in these studies, including ours, are probably not so much due to a lack of knowledge, but rather due to curricula that are unable to involve students in the application of knowledge in concrete situations [25] and to engage them in relevant “whole task” activities [26]. In a recent analysis of the curricula of 11 medical schools in the United States, Irby et al. drew up a list of the main weaknesses of current training programs, such as a lack of standardisation, flexibility and student-centeredness, a poor integration between formal knowledge and experiential learning, and inadequate attention paid to the skills required for interprofessional and team work [27]. These problems were also found at the Lausanne School of Medicine.
As highlighted in previous studies [12, 13, 28], some residents also reported difficulties in managing administrative and other nonclinical tasks that are part of residents’ daily work, a major cause of workplace dissatisfaction [29]. Although somewhat unavoidable, the reported discomfort and anxiety arising during the first months of postgraduate training are concerning. If experienced chronically, these could lead to burnout [30]. Shanafelt et al. showed how burnout is common among resident physicians and is associated with self-reported suboptimal patient care practices [31].
To our knowledge, this is the first Swiss study exploring the preparedness of residents for postgraduate practice. While the number of senior physicians who responded is relatively low, the fact that nearly half of the students filled in the questionnaire despite a heavy workload means it gives a fair illustration of their opinions. Our response rate corresponds with what is usually found among physicians in online surveys [32]. In addition, the mixed-methods approach allowed us to illustrate some of the findings of the questionnaire. Lastly, by surveying first-year residents with around six months of practice experience, we selected the optimal representative population of this transition phase.
Our study has several limitations. The first is that we report on the measurement of perceptions and not of objective outcomes of preparedness, a challenge that has already been mentioned in a previous publication [33]. Another limitation is the relatively low number of senior respondents to the surveys, and the low number of residents who attended the FGs. Third, the data date from 2013, and the situation may have changed since then. However, as no major changes to the curriculum have been undertaken since 2013, we think the results are still valid. The inclusion of students graduating from the same medical school may limit the generalisability of our results. Nevertheless, generalisations can be made to all medical schools similar to Lausanne’s, including those beyond Switzerland.
Two actions can be taken to address the weaknesses identified in our study. The first is to translate them into specific learning objectives and to ensure that the learning methods match the desired training outcomes. One of the most promising ways to describe learning objectives reflecting “real-life” clinical activities is the development of entrustable professional activities (EPAs) [34]. EPAs are easily observable tasks reflecting day-to-day clinical work that trainees are entrusted to perform without supervision when they have attained sufficient competence [34]. The EPAs provide guidance both on teaching and on evaluation methods. The new Swiss framework for undergraduate medical education (PROFILES) [19], edited in 2018, provides a set of nine EPAs. This framework also emphasises clinical and personal competences such as self-assurance and autonomy in dealing with common clinical circumstances and lists a series of situations encompassing the most frequent health care needs of patients. The publication of PROFILES triggered new collaborations between Swiss medical schools, one of which recently led to the publication of a joint document on measures to be implemented in order to comply with the new training objectives [35].
The second action is to incorporate the desired training objectives into a programmatic assessment [36]. This should encompass frequent and comprehensive formative assessments, including of those aspects for which residents feel less prepared. As all health care institutions receiving medical students will have to adopt the concept of EPAs and the corresponding assessment methods, it will be necessary to develop a systematic faculty development program for clinical teachers.
Even if these measures are properly implemented, it is difficult to predict to what extent it is possible to mitigate the "transition shock" (as described by Duchscher [21]) and to better prepare medical graduates to assume their responsibilities in the clinical ward. Indeed, besides curricular aspects, preparedness requires confidence and the ability to adapt to future work [37–39], and depends on internal factors, attributable to the trainee’s personality or behaviors, as well as on external factors such as the support received, the workplace organisation and the workplace culture [21].
Finally, but of paramount importance, the successful implementation of these curricular changes will require the development of an effective academic governance to ensure that all these steps and decisions are taken, implemented and monitored [40].
A small majority of junior residents consider medical school to have prepared them adequately for entering postgraduate training. We highlighted underpreparedness in six critical areas of practice, which limits residents’ autonomy and self-confidence in dealing with their daily clinical practice. The first months of residency are associated with anxiety and fear of making mistakes. By highlighting areas of underperformance, their underlying reasons and their potential repercussions, our study can inform medical schools and program directors about specific actions which can be taken in order to better prepare students and to facilitate their transition to postgraduate practice. Although no formal recommendations can be drawn from this study, it will provide a basis for comparison with larger studies on the impact of the new framework.
Our thanks go to Professor Pedro Manuel Marques-Vidal of the Internal Medicine Service of the University Hospital of Lausanne (Switzerland) for his central contribution to the statistical analysis of the questionnaires.
No conflict of interest relevant to this article was reported.
1 Ten Cate O . What is a 21st-century doctor? Rethinking the significance of the medical degree. Acad Med. 2014;89(7):966–9. doi:.https://doi.org/10.1097/ACM.0000000000000280
2 Morrow G , Johnson N , Burford B , Rothwell C , Spencer J , Peile E , et al. Preparedness for practice: the perceptions of medical graduates and clinical teams. Med Teach. 2012;34(2):123–35. doi:.https://doi.org/10.3109/0142159X.2012.643260
3 Frank JR, Jr , Mungroo R , Ahmad Y , Wang M , De Rossi S , Horsley T . Toward a definition of competency-based education in medicine: a systematic review of published definitions. Med Teach. 2010;32(8):631–7. doi:.https://doi.org/10.3109/0142159X.2010.500898
4 Hawkins RE , Welcher CM , Holmboe ES , Kirk LM , Norcini JJ , Simons KB , et al. Implementation of competency-based medical education: are we addressing the concerns and challenges? Med Educ. 2015;49(11):1086–102. doi:.https://doi.org/10.1111/medu.12831
5 Goldacre MJ , Lambert T , Evans J , Turner G . Preregistration house officers’ views on whether their experience at medical school prepared them well for their jobs: national questionnaire survey. BMJ. 2003;326(7397):1011–2. doi:.https://doi.org/10.1136/bmj.326.7397.1011
6 Ochsmann EB , Zier U , Drexler H , Schmid K . Well prepared for work? Junior doctors’ self-assessment after medical education. BMC Med Educ. 2011;11(1):99. doi:.https://doi.org/10.1186/1472-6920-11-99
7 Hyppölä H , Kumpusalo E , Virjo I , Mattila K , Neittaanmäki L , Halila H , et al. Improvement in undergraduate medical education: a 10-year follow-up in Finland. Med Teach. 2002;24(1):52–6. doi:.https://doi.org/10.1080/00034980120103487
8 Byrne D , O’Connor P , Lydon S , Kerin MJ . Preparing new doctors for clinical practice: an evaluation of pre-internship training. Ir Med J. 2012;105(10):328–30.
9 Tokuda Y , Goto E , Otaki J , Jacobs J , Omata F , Obara H , et al. Undergraduate educational environment, perceived preparedness for postgraduate clinical training, and pass rate on the National Medical Licensure Examination in Japan. BMC Med Educ. 2010;10(1):35. doi:.https://doi.org/10.1186/1472-6920-10-35
10 Tallentire VR , Smith SE , Wylde K , Cameron HS . Are medical graduates ready to face the challenges of Foundation training? Postgrad Med J. 2011;87(1031):590–5. doi:.https://doi.org/10.1136/pgmj.2010.115659
11 Byrne D , O’Connor P , Lydon S , Kerin MJ . Preparing new doctors for clinical practice: an evaluation of pre-internship training. Ir Med J. 2012;105(10):328–30.
12 Illing JC , Morrow GM , Rothwell nee Kergon CR , Burford BC , Baldauf BK , Davies CL , et al. Perceptions of UK medical graduates’ preparedness for practice: a multi-centre qualitative study reflecting the importance of learning on the job. BMC Med Educ. 2013;13(1):34. doi:.https://doi.org/10.1186/1472-6920-13-34
13 Alexander C , Millar J , Szmidt N , Hanlon K , Cleland J . Can new doctors be prepared for practice? A review. Clin Teach. 2014;11(3):188–92. doi:.https://doi.org/10.1111/tct.12127
14CIMS-SMIFK. Swiss Catalogue of Learning Objectives for Undergraduate Medical Training- 2nd edition, http://sclo.smifk.ch/sclo2008 in http://sclo.smifk.ch/sclo2008/, Editor. 2008, http://sclo.smifk.ch/sclo2008/.
15 Berendonk C , Schirlo C , Balestra G , Bonvin R , Feller S , Huber P , et al. The new final Clinical Skills examination in human medicine in Switzerland: Essential steps of exam development, implementation and evaluation, and central insights from the perspective of the national Working Group. GMS Z Med Ausbild. 2015;32(4):Doc40. doi:.https://doi.org/10.3205/zma000982
16 Michaud PA , e.a., The “Profiles” document: a modern revision of the objectives of undergraduate medical studies in Switzerland. Swiss Med Wkly. 2016. 146:w14270.
17 RCPSC CanMEDS Framework. http://www.royalcollege.ca/rcsite/canmeds/canmeds-framework-e.
18 Michaud PA . Reforms of the pre-graduate curriculum for medical students: the Bologna process and beyond. Swiss Med Wkly. 2012;142:w13738. doi:.https://doi.org/10.4414/smw.2012.13738
19CIMS-SMIFK. PROFILES - Principal Relevant Objectives and Framework for Integrative Learning and Education in Switzerland for the training of medical students. 2017 [cited 2020; Available from: https://www.profilesmed.ch/.
20 Schifferdecker KE , Reed VA . Using mixed methods research in medical education: basic guidelines for researchers. Med Educ. 2009;43(7):637–44. doi:.https://doi.org/10.1111/j.1365-2923.2009.03386.x
21 Duchscher JE . Transition shock: the initial stage of role adaptation for newly graduated registered nurses. J Adv Nurs. 2009;65(5):1103–13. doi:.https://doi.org/10.1111/j.1365-2648.2008.04898.x
22 Braun V , Clarke V . Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:.https://doi.org/10.1191/1478088706qp063oa
23 Redwood-Campbell L , Pakes B , Rouleau K , MacDonald CJ , Arya N , Purkey E , et al. Developing a curriculum framework for global health in family medicine: emerging principles, competencies, and educational approaches. BMC Med Educ. 2011;11(1):46. doi:.https://doi.org/10.1186/1472-6920-11-46
24Illing JEA How prepared are medical graduates to begin practice? A comparison of three diverse UK medical schools. 2008. Available from: http://dro.dur.ac.uk/10561/
25Bandaranayake RC. Integrated Learning, in A practical guide for medical teachers, H.R. Dent JA, Hunt D, Editor. 2017, Elsevier. p. 122-127.
26 Yardley S , Teunissen PW , Dornan T . Experiential learning: AMEE Guide No. 63. Med Teach. 2012;34(2):e102–15. doi:.https://doi.org/10.3109/0142159X.2012.650741
27 Irby DM , Cooke M , O’Brien BC . Calls for reform of medical education by the Carnegie Foundation for the Advancement of Teaching: 1910 and 2010. Acad Med. 2010;85(2):220–7. doi:.https://doi.org/10.1097/ACM.0b013e3181c88449
28Wenger E. Communities of Practice: Learning, Meaning, and Identity. 1999, Cambridge: Cambridge University Press.
29 Wenger N , Méan M , Castioni J , Marques-Vidal P , Waeber G , Garnier A . Allocation of Internal Medicine Resident Time in a Swiss Hospital: A Time and Motion Study of Day and Evening Shifts. Ann Intern Med. 2017;166(8):579–86. doi:.https://doi.org/10.7326/M16-2238
30 Maslach C. , Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. 2016. 15(2): p. 103-111. doi: https://doi.org/10.1002/wps.20311
31 Shanafelt TD , Bradley KA , Wipf JE , Back AL . Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136(5):358–67. doi:.https://doi.org/10.7326/0003-4819-136-5-200203050-00008
32 Cunningham CT , Quan H , Hemmelgarn B , Noseworthy T , Beck CA , Dixon E , et al. Exploring physician specialist response rates to web-based surveys. BMC Med Res Methodol. 2015;15(1):32. doi:.https://doi.org/10.1186/s12874-015-0016-z
33 Goldacre MJ , Taylor K , Lambert TW . Views of junior doctors about whether their medical school prepared them well for work: questionnaire surveys. BMC Med Educ. 2010;10(1):78. doi:.https://doi.org/10.1186/1472-6920-10-78
34 Ten Cate O , Chen HC , Hoff RG , Peters H , Bok H , van der Schaaf M . Curriculum development for the workplace using Entrustable Professional Activities (EPAs): AMEE Guide No. 99. Med Teach. 2015;37(11):983–1002. doi:.https://doi.org/10.3109/0142159X.2015.1060308
35 Sohrmann M , Berendonk C , Nendaz M , Bonvin R ; Swiss Working Group For Profiles Implementation. Nationwide introduction of a new competency framework for undergraduate medical curricula: a collaborative approach. Swiss Med Wkly. 2020;150:w20201. doi:.https://doi.org/10.4414/smw.2020.20201
36 Schuwirth LW , Van der Vleuten CP . Programmatic assessment: From assessment of learning to assessment for learning. Med Teach. 2011;33(6):478–85. doi:.https://doi.org/10.3109/0142159X.2011.565828
37 Goldacre MJ , Taylor K , Lambert TW . Views of junior doctors about whether their medical school prepared them well for work: questionnaire surveys. BMC Med Educ. 2010;10(1):78. doi:.https://doi.org/10.1186/1472-6920-10-78
38 Junod Perron N , Audetat MC , Mazouri S , Schindler M , Haller DM , Sommer J . How well are Swiss French physicians prepared for future practice in primary care? BMC Med Educ. 2018;18(1):65. doi:.https://doi.org/10.1186/s12909-018-1168-4
39 Wiener-Ogilvie S , Bennison J , Smith V . General practice training environment and its impact on preparedness. Educ Prim Care. 2014;25(1):8–17. doi:.https://doi.org/10.1080/14739879.2014.11494236
40 Casiro O , Regehr G . Enacting Pedagogy in Curricula: On the Vital Role of Governance in Medical Education. Acad Med. 2018;93(2):179–84. doi:.https://doi.org/10.1097/ACM.0000000000001774
Monti M. and Brunet L. are co-first authors
No conflict of interest relevant to this article was reported.