Figure 3 Proportion of main admission diagnosis according to the international disease classification (ICD) 10 for the non-asylum-seeking children (blue bars) and the asylum-seeking children (red bars).
* p-value < 0.05
DOI: https://doi.org/10.4414/smw.2020.20252
The United Nations High Commissioner for Refugees estimated that in 2017 there were 25.4 million refugees and 3.1 million asylum-seekers worldwide, of whom 52% were younger than 18 years [1]. Switzerland registered over 45,000 asylum requests in 2016 and 2017 [2–4], of which 43–46% were submitted by minors aged <18 years (personal communication, 31 July 2018, Sandra Binggeli, Swiss State Secretariat for Migration) [4]. Globally, an estimated 173,800 were unaccompanied minors and in Switzerland 2730 were registered, accounting for 6% of the total asylum requests [1].
Asylum-seeking children are among the most vulnerable groups in the migration crisis. Their health status is influenced by several factors including their health before leaving the country of origin, and conditions during the journey and in the host country. Many suffer from malnutrition, and communicable and mental health disorders, as they may have experienced exploitation, violence, war, separation from family and trauma [5]. In host countries asylum-seeking children face cultural and linguistic barriers, which have been shown to be a major risk factor for poor health [5, 6]. The World Health Organization (WHO) encourages local healthcare systems in host countries to adapt to the health needs and problems of refugees and asylum-seekers and underlines the importance to implement refugee and migrant health in public health programmes.
Studies about the healthcare and health needs of asylum-seeking children in high-income host countries in Europe are limited. Infectious diseases seem to be an important reason for hospital admission amongst asylum-seeking children [7, 8] and adults [9–11]. In 2015, a study from our institution found that mostly pathogens with a high prevalence in the local population were responsible for infections of admitted refugee children [12]. None of these studies, however, include detailed information on the further management of admitted asylum-seeking children and systematically compared this with the local population.
The aim of this study was therefore to analyse and compare the epidemiology and spectrum of diseases in asylum-seeking and non-asylum-seeking children admitted to our hospital and detail management differences between the two groups.
This was a retrospective cohort study comparing health data from recently arrived asylum-seeking and non-asylum-seeking children admitted to the University Children’s Hospital Basel between January 2016 and December 2017. Analysis of data from children who presented in the emergency department but were not admitted is part of a separate study [13].
Patients admitted between 1 January 2016 and 31 December 2017 were identified using administrative electronic records. The asylum-seeking status was systematically recorded for all children using the following criteria: (i) referral from one of the reception and processing centres run by the State Secretariat for Migration, (ii) presenting any document declaring the patient to be asylum seeking, or (iii) presenting an asylum-seeking identity card. To target only recently arrived asylum-seeking children, identified records were checked for any previous presentation using the unique identifier of the patient and excluded if a record from before January 2015 was detected. Non-asylum-seeking children were identified for the same period using the administrative electronic records. Only children admitted to the hospital were included for further analysis; records from outpatient departments and admissions to the short stay unit were excluded.
Administrative electronic records were used to extract the following variables: main diagnosis, country of origin, age, sex, country of birth, admission and discharge date, admission department, imaging done, treatment prescribed.
Electronic medical records were used to extract detailed information about the asylum-seeking patients including family structure, referring physician, pathogens detected, vaccination status and the use of interpreter services. Main diagnoses were coded using the International Classification of Diseases (ICD)-10 classification according to the WHO. An admission was defined as a documented presentation at our institution with overnight stay. Accounting-units were used for the analysis of prescribed medication. An account-unit was defined as a documented administration of a drug. Data were entered into a REDCap database (REDCap Software, version 6.9.4, 2018). Quality control of the REDCap data was done and records were locked before analysis.
STATA (Stata/IC Version 13.1 2013) was used for analysis and generation of graphs. Analyses were per patient (age, sex, country of origin) or per admission (main diagnosis, duration of admission, medication prescribed). Statistical comparisons were made using the chi-square test for categorical data and t-test for differences in means when data were normally distributed. If the distribution of data was not known, a Wilcoxon test was performed in parallel with the t-test and the t-test result only accepted if the results matched. A two-sample proportion test with a confidence interval (CI) of 95% was used to test differences in proportions. For CIs of medians, centiles with binomial interpolated confidence intervals were calculated. For CIs of proportions, the exact Clopper-Pearson CI was used.
Ethics approval (EKNZ 2017-01585) for this study was granted in October 2017 by the Ethics Committee of North-West Switzerland.
For the final analysis 11,794 admissions of 9407 patients were included. Of these, 1% of admissions (149/11,794) and 1% of patients (117/9407) were asylum-seeking children (fig. 1). In total, there were 9290 patients in the non-asylum-seeking and 117 patients in the asylum-seeking group. The median age in both groups was 4 years; the interquartile range was 0–13 and 0–11 years for asylum-seeking and non-asylum-seeking children, respectively. A total of 61% and 56% were male in the asylum-seeking and non-asylum-seeking children, respectively (table 1). Infants were the largest admitted age group (30%) in both groups. In addition, in the asylum-seeking group a second peak in the age distribution was seen in adolescence with 11% (17/149) being aged ≥15 compared with 5% (565/11’645) in the non-asylum-seeking group (fig. 2).
Figure 1 Flow chart – Study population
Table 1 Baseline characteristics, countries of origin, native country by asylum-seeking and non-asylum-seeking patients in 2016/17.
| Asylum-seeking | Non-asylum-seeking | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics |
Admissions
n = 149 |
Patients
n = 117 |
Admissions
n = 11,645 |
Patients
n = 9290 |
||||
| n | IQR/% | n | IQR/% | n | IQR/% | n | IQR/% | |
| Median age (years) 95% CI |
4 2–7 |
0–13 | 4 4–4 |
0–11 | ||||
| Male sex 95% CI |
71 | 60.7 0.51–0.70 |
5157 | 55.5 0.55–0.56 |
||||
| Countries of origin: | ||||||||
| Eritrea | 25 | 21.4 | Switzerland | 6057 | 65.2 | |||
| Afghanistan | 22 | 18.9 | Germany | 746 | 8.0 | |||
| Syria | 18 | 15.4 | Italy | 312 | 3.4 | |||
| Somalia | 10 | 8.6 | Turkey | 285 | 3.1 | |||
| Ethiopia | 8 | 6.8 | Kosovo | 253 | 2.7 | |||
| Iraq | 8 | 6.8 | Portugal | 168 | 1.8 | |||
| Other | 25 | 21.4 | Other | 1466 | 15.8 | |||
| ns | 1 | 0.85 | ns | 3 | 0.03 | |||
| Countries of birth: | ||||||||
| Switzerland | 40 | 34.1 | Switzerland | 8176 | 91.0 | |||
| Afghanistan | 17 | 15.3 | Germany | 268 | 3.0 | |||
| Syria | 14 | 12.0 | France | 54 | 0.6 | |||
| Eritrea | 13 | 11.1 | US | 41 | 0.5 | |||
| Iraq | 6 | 5.1 | Great Britain | 38 | 0.4 | |||
| Somalia | 5 | 4.2 | Italy | 30 | 0.3 | |||
| Other | 16 | 13.7 | Other | 372 | 4.0 | |||
| ns | 6 | 5.1 | ns | 311 | 3.3 | |||
| Mean duration of admission (days) | 4 | 2–7 | 3 | 2–6 | ||||
| Patients visited ED before | 96 | 64.9 | 7013 | 60.2 | ||||
| CI = confidence interval; ED = emergency department; ns = not specified | ||||||||
Figure 2 Histogram showing the age distribution of admissions from non-asylum-seeking and asylum-seeking children in the years 2016 and 2017.
In the asylum-seeking children the most frequent countries of origin were: Eritrea 21% (25/117); Afghanistan 19% (22/117) and Syria 15% (18/117). The most frequent countries of birth were Switzerland 36% (40/117), Afghanistan 15% (17/117) and Syria 13% (14/117). In the non-asylum-seeking children the most frequent countries of origin were Switzerland 65% (6057/9290), Germany 8% (746/9290) and Italy 3.4% (312/9290). The most frequent countries of birth were Switzerland 91% (8176/9290), Germany 3% (268/9290) and France 0.6% (54/9290).
In the asylum-seeking group, 16% of admissions were unaccompanied minors (24/149). In 63.8% of admissions (95/149), the child was accompanied by both parents, in 6.7% by one parent (10/149) and in one case by a caregiver who was not a parent (1/149; 0.7%). In 12.8% of admissions (19/149), data on the family structure were not available.
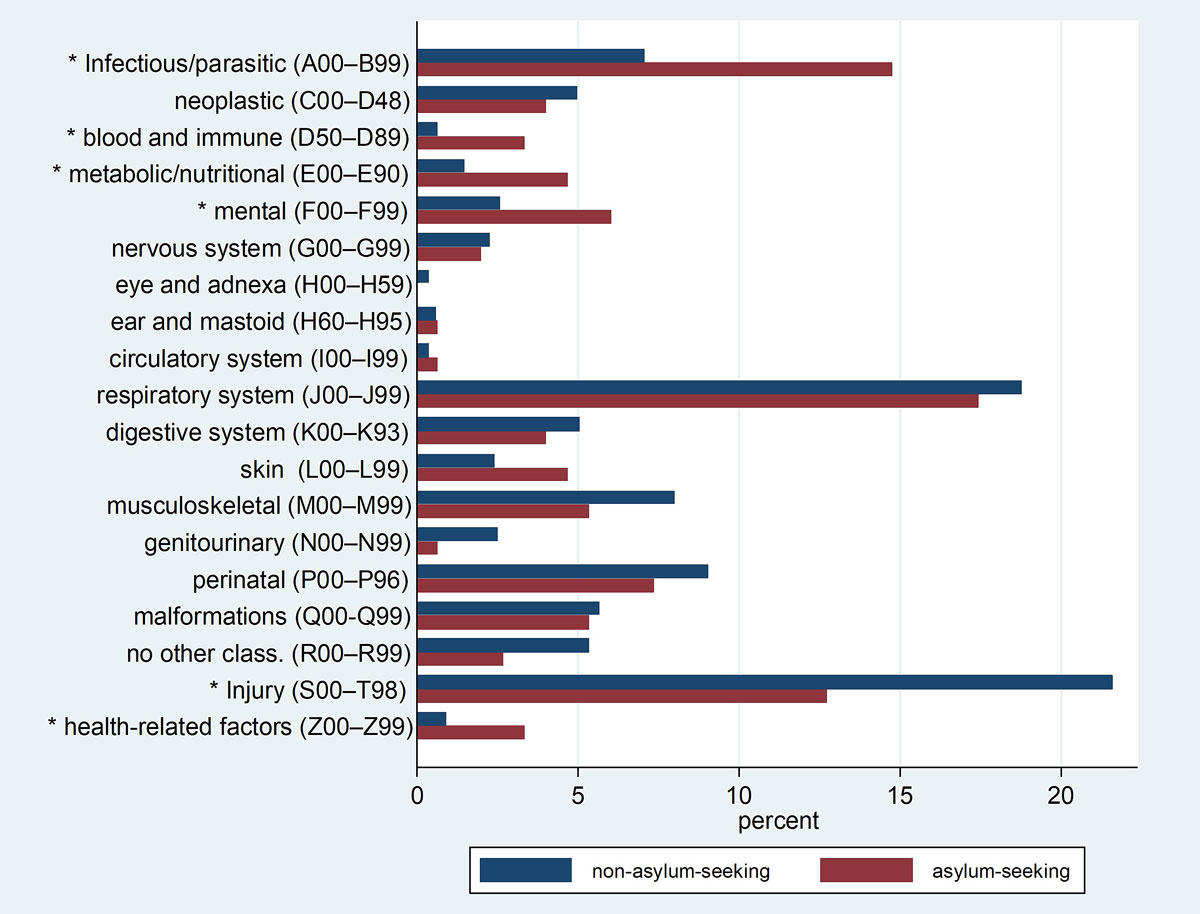
The main admission diagnosis in the asylum-seeking children were: diseases of the respiratory system (ICD-10 codes J00–J99) 17% (26/149), certain infectious and parasitic diseases (ICD-10 codes A00–B99) 15% (22/149) and injury, poisoning and other consequences of external causes (ICD-10 codes S00–T98) 13% (19/149). In the non-asylum-seeking group the most frequent reasons for admission were injury, poisoning and other consequences of external causes 22% (2517/11,645), diseases of the respiratory system 19% (2187/11,645) and conditions originating in the perinatal period (ICD-10 codes P00–P96) 9% (1057/11,645). Mean duration of admission was 4 days in the asylum-seeking and 3 days in the non-asylum-seeking children (table 1). Further diseases and details can be found in table 2 and supplementary table S1 in appendix 1.
Table 2 Top five of main IC-10 category with top five of main admission diagnosis. 95% CI: Confidence Interval for the proportion of the ICD-10 category.
| Asylum-seeking | Non-asylum-seeking | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ICD-10 coding | n | % | ICD-10 coding | n | % | |||||
| Diseases of the respiratory system (J00-J99) | 26 | 17 | Injury, poisoning, other consequences of ext. causes (S00-T98) | 2517 | 22 | |||||
| 95% CI | 0.12–0.25 | 95% CI | 0.21–0.22 | |||||||
| J06 | Acute upper respiratory infections of multiple and unspecified sites | 9 | 6.0 | S06 | Intracranial injury | 871 | 7.5 | |||
| J20/21 | Acute bronchitis/bronchiolitis | 4 | 2.6 | S00 | Superficial injury of head | 380 | 3.4 | |||
| J10 | Influenza due to identified seasonal influenza virus | 2 | 1.3 | S52 | Fracture of forearm | 225 | 1.9 | |||
| J12 | Viral pneumonia, not elsewhere classified | 2 | 1.3 | S42 | Fracture of shoulder and upper arm | 110 | 0.9 | |||
| J18 | Pneumonia, organism unspecified | 2 | 1.3 | T78 | Adverse effects, not elsewhere classified | 84 | 0.7 | |||
| Certain infectious and parasitic diseases (A00-B99) | 22 | 15 | Diseases of the respiratory system (J00–J99) | 2187 | 19 | |||||
| 95% CI | 0.09–0.21 | 95% CI | 0.18–0.20 | |||||||
| B50/51 | Plasmodium falciparum and vivax malaria | 5 | 2.7 | J20 | Acute bronchitis | 528 | 4.5 | |||
| A09 | Other gastroenteritis and colitis of infectious and unspecified origin | 3 | 2.0 | J35 | Chronic diseases of tonsils and adenoids | 422 | 3.6 | |||
| A15 | Respiratory tuberculosis, bact. and histol. confirmed | 3 | 2.0 | J06 | Acute upper respiratory infections of multiple and unspecified sites | 396 | 3.4 | |||
| B86 | Scabies | 3 | 2.0 | J21 | Acute bronchiolitis | 297 | 2.6 | |||
| A38 | Scarlet fever | 2 | 1.3 | J10 | Influenza due to identified seasonal influenza virus | 85 | 0.7 | |||
| Injury, poisoning, other consequences of external causes (S00-T98) | 19 | 13 | Certain conditions originating in the perinatal period (P00–P96) | 1057 | 9.1 | |||||
| 95% CI | 0.08–0.19 | 95% CI | 0.09–0.10 | |||||||
| S00 | Superficial injury of head | 3 | 2.0 | P22 | Respiratory distress of newborn | 424 | 3.6 | |||
| S06 | Intracranial injury | 3 | 2.0 | P39 | Other infections specific to the perinatal period | 117 | 1.0 | |||
| T81 | Complications of procedures, not elsewhere classified | 2 | 1.3 | P92 | Feeding problems of newborn | 112 | 1.0 | |||
| S42 | Fracture of shoulder and upper arm | 1 | 0.7 | P59 | Neonatal jaundice from other and unspecified causes | 73 | 0.6 | |||
| S52 | Fracture of forearm | 1 | 0.7 | P28 | Other respiratory conditions originating in the perinatal period | 72 | 0.6 | |||
| Certain conditions originating in the perinatal period (P00-P96) | 11 | 7.4 | Diseases of the musculoskeletal system/connective tissue (M00–M99) | 930 | 8.0 | |||||
| 95% CI | 0.04–0.13 | 95% CI | 0.08–0.08 | |||||||
| P22 | Respiratory distress of newborn | 7 | 4.7 | M21 | Other acquired deformities of limbs | 244 | 2.1 | |||
| P28 | Other respiratory conditions originating in the perinatal period | 1 | 0.7 | M41 | Scoliosis | 125 | 1.1 | |||
| P39 | Other infections specific to the perinatal period | 1 | 0.7 | M24 | Other specific joint derangements | 102 | 0.9 | |||
| P55 | Haemolytic disease of fetus and newborn | 1 | 0.7 | M23 | Internal derangement of knee | 58 | 0.5 | |||
| P92 | Feeding problems of newborn | 1 | 0.7 | M84 | Disorders of continuity of bone | 52 | 0.5 | |||
| Mental and behavioural disorders (F00-F99) | 9 | 6.0 | Certain infectious and parasitic diseases (A00–B99) | 824 | 7.1 | |||||
| 95% CI | 0.03–0.11 | 95% CI | 0.07–0.08 | |||||||
| F43 | Reaction to severe stress, and adjustment disorders | 5 | 3.4 | A08 | Viral and other specifies intestinal infections | 273 | 2.3 | |||
| F32 | Depressive episode | 3 | 2.0 | A09 | Other gastroenteritis and colitis of infectious and unspecified origin | 256 | 2.2 | |||
| F10 | Mental and behavioural disorders due to use of alcohol | 1 | 0.7 | B34 | Viral infection of unspecified site | 70 | 0.6 | |||
| A87 | Viral meningitis | 26 | 0.2 | |||||||
| A04 | Other bacterial intestinal infections | 24 | 0.2 | |||||||
The frequency of admission for diseases of the respiratory system was comparable in both asylum-seeking and non-asylum-seeking groups at 17% (26/149) and 19% (2187/11,645), respectively (difference in proportions 0.02, 95% CI −0.08 to 0.04; p = 0.73; fig. 3). Admissions for certain infectious and parasitic diseases were more frequent in the asylum-seeking than the non-asylum-seeking children at 15% (22/149) and 7% (824/11,645), respectively (difference in proportions 0.08, 95% CI 0.02 to 0.14; p <0.001). In the asylum-seeking children, 3% of the admissions were caused by malaria (5/149), intestinal infections (4/149) and active tuberculosis (4/149). In the non-asylum-seeking children malaria or active tuberculosis were very rare accounting for <0.1% of admissions (2/11,645 and 4/11,645, respectively).
Figure 3 Proportion of main admission diagnosis according to the international disease classification (ICD) 10 for the non-asylum-seeking children (blue bars) and the asylum-seeking children (red bars).
* p-value < 0.05
Admissions for injury, poisoning and certain other consequences of external causes were more frequent in non-asylum-seeking children at 22% (2517/11,645) compared with 13% (19/149) (difference in proportions 0.09, 95% CI 0.04 to 0.14; p <0.01). Within this category head injuries were the most frequent reason for admission, with intracranial injury being more frequent in asylum-seeking than non-asylum-seeking children 2% (3/149) and 7.5% (871/11,645), respectively, (p = 0.01) (table 2).
Admission for mental health disorders (F00–F99) were more frequent in the asylum-seeking children than the non-asylum-seeking children at 6% (9/149) and 2.6% (304/11,645), respectively (difference in proportions 0.03, 95% CI −0.04 to 0.07; p = 0.01). Severe stress and adjustment disorders, depressive episodes and behavioural disorder due to psychoactive substance use were most common in the asylum-seeking children and eating disorders, depressive episodes in the non-asylum-seeking children.
A total of 75,722 accounting-units of the most common analgesics including paracetamol, nonsteroidal anti-inflammatory drugs (NSAIDs) and opioids were prescribed (table 3 and supplementary tables S2 and S3 in appendix 1). With 3.4 (506/149) accounting-units per admission in asylum-seeking children, analgesic prescription was lower compared with non-asylum-seeking children with 6.5 (75,216/11,645) accounting-units per admission.
Table 3 Prescribed analgesic and antibiotic medication in asylum-seeking and non-asylum-seeking children admitted to the hospital.
| Type of medication | Administration route | Asylum-seeking | Non-asylum-seeking | ||
|---|---|---|---|---|---|
| Accounting units | Unit/hosp. | Accounting units | Unit/hosp. | ||
| Paracetamol | Oral | 85 | 0.57 | 20370 | 1.75 |
| Rectal | 55 | 0.37 | 7751 | 0.67 | |
| i.v. | 32 | 0.21 | 12015 | 1.03 | |
| Total | 172 | 0.15 | 40136 | 3.45 | |
| Non-steroidal anti-inflammatory drugs (NSAID) |
Oral | 230 | 1.54 | 20803 | 1.79 |
| Rectal | 2 | 0.01 | 833 | 0.07 | |
| i.v. | 47 | 0.32 | 5463 | 0.47 | |
| Total | 279 | 1.87 | 27099 | 2.33 | |
| Opioids | Oral | 0 | 0 | 1044 | 0.09 |
| i.v. | 55 | 0.37 | 6801 | 0.58 | |
| Others | 0 | 0 | 16 | 0.001 | |
| Total | 55 | 0.37 | 7861 | 0.68 | |
| Total, analgesics | 506 | 3.39 | 75096 | 6.45 | |
| Amoxicillin – clavulanic acid | Oral | 54 | 0.36 | 3749 | 0.32 |
| i.v. | 55 | 0.37 | 4390 | 0.38 | |
| Total | 109 | 0.73 | 8139 | 0.7 | |
| Cephalosporins | Oral | 0 | 0 | 326 | 0.03 |
| i.v. | 15 | 0.1 | 2019 | 0.17 | |
| Total | 15 | 0.1 | 2345 | 0.2 | |
| Total, antibiotics | 124 | 0.83 | 10484 | 0.9 | |
i.v. = intra venous; unit/hosp. = unit per hospitalisation
NSAIDs were most frequently prescribed, with a total of 2.3 (27,378/11,794) accounting-units per admission, and a frequency of 1.87 (279/149) accounting-units per admission in the asylum-seeking versus 2.33 (27,099/11,645) in the non-asylum-seeking children. Opioids were rarely used in either group, in total 0.67 (7916/11,794) accounting-units per admission, with 0.37 (55/149) accounting-units per admission in the asylum-seeking and 0.69 (7861/11,645) accounting-units per admission in the non-asylum-seeking children.
Amoxicillin-clavulanic acid and cephalosporins were the most commonly prescribed antibiotics overall with 0.9 (10,608/11,794) accounting-units per admission. Prescription of amoxicillin-clavulanic acid was comparable in both groups with 0.7 accounting-units per admission in the asylum-seeking children (109/149) and in non-asylum-seeking children (8139/11,645). Cephalosporins were less frequently prescribed with 0.1 (15/149) and 0.2 (2345/11645) accounting-units per admission in asylum-seeking and non-asylum-seeking children, respectively.
This study analysing the spectrum of diseases of asylum-seeking children admitted to a tertiary care hospital found respiratory infections to be common in both groups, but rare infectious diseases to be more frequent in asylum-seeking children and injuries more frequent in non-asylum-seeking children. The strength of this study lies in its comparison of admitted asylum-seeking with non-asylum-seeking children in the same institution.
The age distribution in both groups shows striking similarity in younger children but a remarkably higher proportion in the adolescent asylum-seeking group. This is because adolescents and young adults have become an important refugee group in all European countries over the past few years [14]. This age group includes unaccompanied minor refugees with special health needs. Their vulnerability leads to an increased susceptibility to disease, malnutrition and physical injury and their dependence requires qualified special care to support physical and psychological needs, and social well-being [15, 16].
Our study showed a high number of asylum-seeking children admitted with respiratory diseases. This is in accordance with other studies reporting a high prevalence of respiratory tract diseases in asylum-seeking children [8, 12, 17–19]. Importantly, admission for respiratory tract infections is also very common in non-asylum-seeking children. Several other studies reported acute respiratory infections, including pneumonia [20–22] and influenza [23], to be among the most prevalent diseases of children all over the world – in developing as well as in developed countries.
Other types of infection including malaria, active tuberculosis and scabies were rare in admitted patients and almost exclusively in asylum-seeking children. This finding is in contrast to other studies. For example, a prospective cross-sectional study in Germany including unaccompanied asylum-seeking adolescents found infectious and parasitic diseases, including intestinal parasites, scabies and hepatitis B, in almost 50% [24]. Another German study reporting screening results that detected intestinal parasite infections in 22% of unaccompanied minors [25]. This discrepancy might be explained by the fact that intestinal parasitic infections are usually not severe and, generally, affected children do not require admission to hospital. Also, we did not consistently screen our patients on admission.
Surprisingly, trauma and injury were less frequently the cause of admission in asylum-seeking children than the non-asylum-seeking children. A limited number of trauma- and injury-related admissions were also seen in our previous study; however at that time we were unable to compare results with the local population. One explanation for this finding might be that asylum-seeking children are less likely to be admitted for trauma and injury as these occur less commonly. Alternatively, the injuries are equally common but asylum-seeking children potentially experience barriers to presenting to an emergency department, including lack of information about the local health care system, worries about high charges or language barriers [26–28].
In the current study, mental disorders were the fifth most common reason of admission and the incidence was increased compared with our previous study [12]. Mental health disorders have been identified as one of the most important issues for asylum-seeking children in other studies, particularly in young adults and unaccompanied minor refugees [29–34]. A literature search showed that screening and intervention for post-traumatic stress disorder in minor refugees are rare. About 25% of asylum-seeking children might develop this disorder, but few are being diagnosed and treated [35]. A Danish study found a higher prevalence of mental health disorders in unaccompanied than in accompanied asylum-seeking children [31]. In our study, only a few patients were admitted because of mental health disorders, in contrast to a Norwegian study where 48% of unaccompanied adolescent asylum-seekers met the diagnostic criteria [36]. One possible explanation is that these disorders were underestimated in our study as we only analysed the main diagnosis for admission and underlying mental health disorders was not included in the analysis. In addition, patients might have been referred directly to a psychiatric clinic. Nevertheless, healthcare workers in host countries should be aware of mental health disorder in asylum-seeking children; however it remains controversial if routine screening should be used [37].
A further important finding was the difference in prescriptions for asylum-seeking and non-asylum-seeking admitted patients. Lower rates of analgesic prescription in the asylum-seeking patients may result from fewer admissions due to injuries. However, a possible other explanation is the language barrier, preventing asylum-seeking patients and their families from verbalising discomfort and pain.
This study has several limitations. First, only data of patients at our institution were included, so applicability to other regions in Switzerland and Europe might be limited. Second, the systematic registration as asylum-seeking patients may have been missed at the registration desk, and therefore a potential underestimation of the number of asylum-seeking children cannot be excluded. Third, the retrospective collection of data from a large number of patients presents potential sources of reporting bias and missing data, which limited in depth analysis. For example, data on vaccination status and interpreter use was not systematically recorded, and further data regarding factors influencing pain medication use were not recorded at all.
Asylum-seeking children represent a small number of total admissions in a tertiary hospital in Switzerland. Respiratory infectious were among the most common admission diagnoses in asylum-seeking and non-asylum-seeking children. In addition, rare infections and mental health disorders are important diseases in asylum-seeking children, and require special attention and training of staff working with paediatric asylum-seekers. In non-asylum-seeking children, injuries and neonatal diseases are also frequent. Asylum-seeking children received half as much analgesics as non-asylum-seeking children which may result from language barriers.
The appendix is available as a separate file at https://smw.ch/article/doi/smw.2020.20252.
We would like to thank kindly Robert Kopf (Controlling), Matthias Tschudin (Application and Services) and Angelika Fix (Accounting) for their support.
We do not have any funding source for this study.
The authors declare that they have no conflict of interest.
1United Nations High Commissioner for Refugees. Global trends 2017. 2018. Available from: http://www.unhcr.org/globaltrends2017/.
2Statssekretariat für Migration. Asylstatistik Übersichten 1986-2018. Available from: https://www.sem.admin.ch/sem/de/home/publiservice/statistik/asylstatistik/uebersichten.html.
3Staatssekretariat für Migration. Asylstatistik 2017. 2018. Available from: https://www.sem.admin.ch/sem/de/home/aktuell/news/2018/2018-01-22.html.
4Staatssekretariat für Migration. Statistik UMA 2017. 2018. Available from: https://www.sem.admin.ch/dam/data/sem/publiservice/statistik/asylstatistik/statistiken_uma/uma-2017-d.pdf.
5 ISSOP Migration Working Group. ISSOP position statement on migrant child health. Child Care Health Dev. 2018;44(1):161–70. doi:.https://doi.org/10.1111/cch.12485
6 Williams B , Cassar C , Siggers G , Taylor S . Medical and social issues of child refugees in Europe. Arch Dis Child. 2016;101(9):839–42. doi:.https://doi.org/10.1136/archdischild-2016-310657
7 Güngör A , Çatak AI , Çuhaci Çakir B , Öden Akman A , Karagöl C , Köksal T , et al. Evaluation of Syrian refugees who received inpatient treatment in a tertiary pediatric hospital in Turkey between January 2016 and August 2017. Int Health. 2018;10(5):371–5. doi:.https://doi.org/10.1093/inthealth/ihy034
8 Bucak IH , Almis H , Benli S , Turgut M . An overview of the health status of Syrian refugee children in a tertiary hospital in Turkey. Avicenna J Med. 2017;7(3):110–4.
9 van Loenen T , van den Muijsenbergh M , Hofmeester M , Dowrick C , van Ginneken N , Mechili EA , et al. Primary care for refugees and newly arrived migrants in Europe: a qualitative study on health needs, barriers and wishes. Eur J Public Health. 2018;28(1):82–7. doi:.https://doi.org/10.1093/eurpub/ckx210
10 Bloch-Infanger C , Bättig V , Kremo J , Widmer AF , Egli A , Bingisser R , et al. Increasing prevalence of infectious diseases in asylum seekers at a tertiary care hospital in Switzerland. PLoS One. 2017;12(6):e0179537. doi:.https://doi.org/10.1371/journal.pone.0179537
11 Aldridge RW , Nellums LB , Bartlett S , Barr AL , Patel P , Burns R , et al. Global patterns of mortality in international migrants: a systematic review and meta-analysis. Lancet. 2018;392(10164):2553–66. doi:.https://doi.org/10.1016/S0140-6736(18)32781-8
12 Pohl C , Mack I , Schmitz T , Ritz N . The spectrum of care for pediatric refugees and asylum seekers at a tertiary health care facility in Switzerland in 2015. Eur J Pediatr. 2017;176(12):1681–7. doi:.https://doi.org/10.1007/s00431-017-3014-9
13 Brandenberger J , Bozorgmehr K , Vogt F , Tylleskär T , Ritz N . Preventable admissions and emergency-department-visits in pediatric asylum-seeking and non-asylum-seeking patients. Int J Equity Health. 2020;19(1):58. doi:.https://doi.org/10.1186/s12939-020-01172-w
14World Health Organization Europe. Report on the health of refugees and migrants in the WHO European Region. 2018. Available from: http://www.euro.who.int/__data/assets/pdf_file/0004/392773/ermh-eng.pdf?ua=1.
15United Nations High Commissioner for Refugees. Refugee Children: Guidelines on Protection and Care: Refugee Children: Guidelines on Protection and Care; 1994. Available from: https://www.unhcr.org/3b84c6c67.pdf.
16United Nations Children’s Fund. A child is a child 2017 [Available from: https://www.unicef.org/publications/files/UNICEF_A_child_is_a_child_May_2017_EN.pdf.
17 Pfeil J , Kobbe R , Trapp S , Kitz C , Hufnagel M . [Recommendations for the diagnosis and prevention of infectious diseases in pediatric and adolescent refugees in Germany : Statement of the German Society of Pediatric Infectious Diseases, the Society of Tropical Pediatrics and International Child Health, and the Professional Association of Pediatricians]. Internist (Berl). 2016;57(5):416–33. doi:.https://doi.org/10.1007/s00108-016-0040-z
18 Alberer M , Wendeborn M , Löscher T , Seilmaier M . [Spectrum of diseases occurring in refugees and asylum seekers: data from three different medical institutions in the Munich area from 2014 and 2015]. Dtsch Med Wochenschr. 2016;141(1):e8–15.
19 Abbott KL , Woods CA , Halim DA , Qureshi HA . Pediatric care during a short-term medical mission to a Syrian refugee camp in Northern Jordan. Avicenna J Med. 2017;7(4):176–81. doi:.https://doi.org/10.4103/ajm.AJM_100_17
20 El Baroudy NR , Refay ASE , Hamid TAA , Hassan DM , Soliman MS , Sherif L . Respiratory Viruses and Atypical Bacteria Co-Infection in Children with Acute Respiratory Infection. Open Access Maced J Med Sci. 2018;6(9):1588–93. doi:.https://doi.org/10.3889/oamjms.2018.332
21 Walker CLF , Rudan I , Liu L , Nair H , Theodoratou E , Bhutta ZA , et al. Global burden of childhood pneumonia and diarrhoea. Lancet. 2013;381(9875):1405–16. doi:.https://doi.org/10.1016/S0140-6736(13)60222-6
22 Bhuiyan MU , Snelling TL , West R , Lang J , Rahman T , Granland C , et al. The contribution of viruses and bacteria to community-acquired pneumonia in vaccinated children: a case-control study. Thorax. 2019;74(3):261–9. doi:.https://doi.org/10.1136/thoraxjnl-2018-212096
23 Lafond KE , Nair H , Rasooly MH , Valente F , Booy R , Rahman M , et al.; Global Respiratory Hospitalizations—Influenza Proportion Positive (GRIPP) Working Group. Global Role and Burden of Influenza in Pediatric Respiratory Hospitalizations, 1982-2012: A Systematic Analysis. PLoS Med. 2016;13(3):e1001977. doi:.https://doi.org/10.1371/journal.pmed.1001977
24 Laukamp A , Prüfer-Krämer L , Fischer F , Krämer A . Health of Syrian unaccompanied asylum seeking adolescents (UASA) at first medical examination in Germany in comparison to UASA from other world regions. BMC Int Health Hum Rights. 2019;19(1):5. doi:.https://doi.org/10.1186/s12914-019-0192-8
25 Mockenhaupt FP , Barbre KA , Jensenius M , Larsen CS , Barnett ED , Stauffer W , et al. Profile of illness in Syrian refugees: A GeoSentinel analysis, 2013 to 2015. Euro Surveill. 2016;21(10):30160. doi:.https://doi.org/10.2807/1560-7917.ES.2016.21.10.30160
26 Chiarenza A , Dauvrin M , Chiesa V , Baatout S , Verrept H . Supporting access to healthcare for refugees and migrants in European countries under particular migratory pressure. BMC Health Serv Res. 2019;19(1):513. doi:.https://doi.org/10.1186/s12913-019-4353-1
27 Brandenberger J , Sontag K , Duchêne-Lacroix C , Jaeger FN , Peterhans B , Ritz N . Perspective of asylum-seeking caregivers on the quality of care provided by a Swiss paediatric hospital: a qualitative study. BMJ Open. 2019;9(9):e029385. doi:.https://doi.org/10.1136/bmjopen-2019-029385
28 Brandenberger J , Tylleskär T , Sontag K , Peterhans B , Ritz N . A systematic literature review of reported challenges in health care delivery to migrants and refugees in high-income countries - the 3C model. BMC Public Health. 2019;19(1):755. doi:.https://doi.org/10.1186/s12889-019-7049-x
29 Gadeberg AK , Montgomery E , Frederiksen HW , Norredam M . Assessing trauma and mental health in refugee children and youth: a systematic review of validated screening and measurement tools. Eur J Public Health. 2017;27(3):439–46. doi:.https://doi.org/10.1093/eurpub/ckx034
30 Hodes M , Vasquez MM , Anagnostopoulos D , Triantafyllou K , Abdelhady D , Weiss K , et al. Refugees in Europe: national overviews from key countries with a special focus on child and adolescent mental health. Eur Child Adolesc Psychiatry. 2018;27(4):389–99. doi:.https://doi.org/10.1007/s00787-017-1094-8
31 Norredam M , Nellums L , Nielsen RS , Byberg S , Petersen JH . Incidence of psychiatric disorders among accompanied and unaccompanied asylum-seeking children in Denmark: a nation-wide register-based cohort study. Eur Child Adolesc Psychiatry. 2018;27(4):439–46. doi:.https://doi.org/10.1007/s00787-018-1122-3
32 Reavell J , Fazil Q . The epidemiology of PTSD and depression in refugee minors who have resettled in developed countries. J Ment Health. 2017;26(1):74–83. doi:.https://doi.org/10.1080/09638237.2016.1222065
33United Nations Children’s Fund. Unaccompanied minors from Afghanistan: Problems and protection in the European Union 2016 [Available from: https://www.unicef-irc.org/article/1389-unaccompanied-minors-from-afghanistan-problems-and-protection-in-the-european-union.html.
34 Vervliet M , Meyer Demott MA , Jakobsen M , Broekaert E , Heir T , Derluyn I . The mental health of unaccompanied refugee minors on arrival in the host country. Scand J Psychol. 2014;55(1):33–7. doi:.https://doi.org/10.1111/sjop.12094
35 Horlings A , Hein I . Psychiatric screening and interventions for minor refugees in Europe: an overview of approaches and tools. Eur J Pediatr. 2018;177(2):163–9. doi:.https://doi.org/10.1007/s00431-017-3027-4
36 Wittkowski A , Patel S , Fox JR . The Experience of Postnatal Depression in Immigrant Mothers Living in Western Countries: A Meta-Synthesis. Clin Psychol Psychother. 2017;24(2):411–27. doi:.https://doi.org/10.1002/cpp.2010
37 Pottie K , Greenaway C , Feightner J , Welch V , Swinkels H , Rashid M , et al.; coauthors of the Canadian Collaboration for Immigrant and Refugee Health. Evidence-based clinical guidelines for immigrants and refugees. CMAJ. 2011;183(12):E824–925. doi:.https://doi.org/10.1503/cmaj.090313
Shared authorship
MG: conceived the study, performed data analysis, drafted the initial manuscript, and approved the final manuscript as submitted. JB: conceived the study, performed data analysis, reviewed the manuscript, and approved the final manuscript as submitted. SB: conceived the study, reviewed the manuscript, and approved the final manuscript as submitted. CP: Reviewed the manuscript, and approved the final manuscript as submitted. NR: conceived the study, supervised analysis, reviewed and revised the manuscript, and approved the final manuscript as submitted.
We do not have any funding source for this study.
The authors declare that they have no conflict of interest.