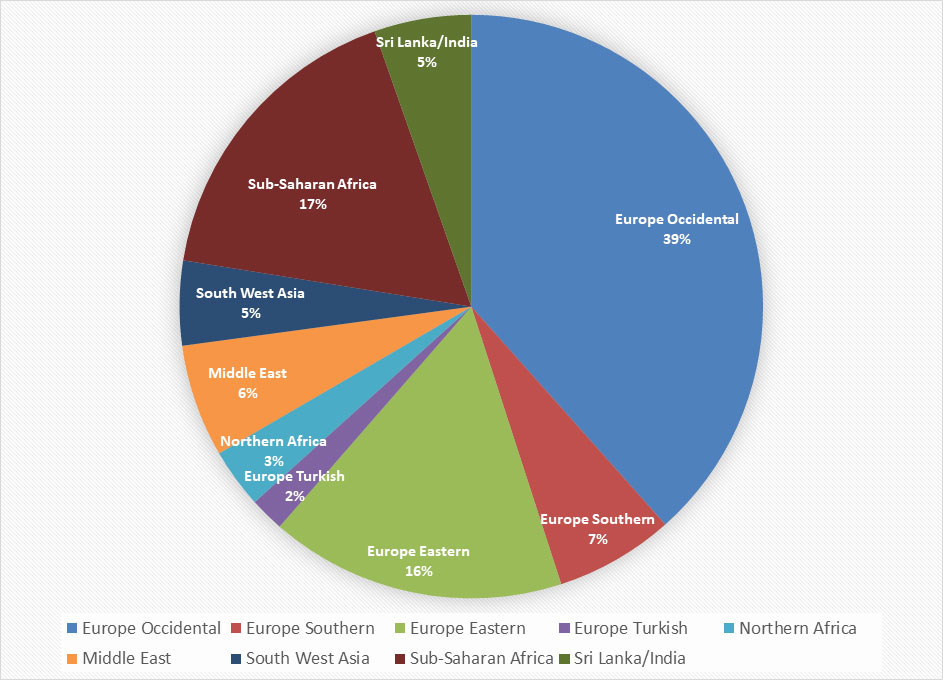
Figure 1 Distribution of the population studied according to their ethnic origin.
DOI: https://doi.org/10.4414/smw.2020.20238
Vitamin D is best known as a vitamin of the calcium and bone metabolism. More recently, vitamin D has been shown to have many other roles in human physiology. Indeed, vitamin D receptors are found in most of an organism’s cells, including white blood cells, and may play a role in cell proliferation and differentiation and affect the immune system or insulin secretion and sensitivity [1]. Furthermore, recent reports indicate an association between low vitamin D levels and an increased risk of developing pregnancy complications such as disorders of placental implantation, pre-eclampsia, fetal growth retardation, gestational hypertension, impaired glucose tolerance and gestational diabetes, preterm birth, caesarean section, and other adverse conditions [2–5]. Recent studies report a higher incidence of postpartum depression in cases of vitamin D deficiency [6]. As a long-term consequence of vitamin D deficiency, women are at risk of developing severe osteoporosis [1]. A low vitamin D level in the mother can result in maternal hypocalcaemia, which in turn is a factor that promotes the development of neonatal seizures.
Negative effects of maternal vitamin D deficiency have also been reported in the newborn and for the offspring’s development: long-term consequences for the child may range from rickets, increased susceptibility to respiratory illness, autoimmune diseases like Crohn’s disease or diabetes mellitus type I, or even cancer, since vitamin D also has a modulatory action on the immune system [7–9]. Lower neonatal vitamin D status is related to autism spectrum disorder, and a link to developmental delay has recently been shown in the CHARGE case-control study [10].
There is emerging evidence that genetic and epigenetic factors may influence vitamin D status, and that the gene expression profiles of healthy pregnant women change during the course of pregnancy, suggesting that maternal vitamin D levels influence transcriptional profiles. These alterations of the maternal transcriptome may contribute to fetal immune imprinting and reduce allergic sensitisation in early life [11, 12]. New data suggest that there are indeed direct genomic alterations induced by the vitamin D administered during pregnancy that can alter birth outcomes [13–15].
Vitamin D is the only vitamin that can be synthesised by the body itself, with the help of ultraviolet B (UVB) irradiation. Nevertheless, vitamin D deficiency is quite common. In Switzerland, the prevalence of vitamin D deficiency has been shown to be 60% for the general population, with seasonal variability [16]. There is no published data on the prevalence of vitamin D deficiency in pregnant women in Switzerland.
There is no consensus among health experts on the optimal serum level of vitamin D to guarantee sufficient long-term bone mineralisation and to support the proper functioning of the whole organism. In the literature, most experts (IOM, WHO, NIH, EFSA) regard serum levels of 25(OH)D between 50 and 75 nmol/l as sufficient [17–21].
Treatment of vitamin D deficiency consists of consequent supplementation. There are several different supplementation protocols among different countries and health institutions [22]. Unfortunately, there is currently a lack of evidence concerning the best way to supplement vitamin D and the efficacy of vitamin D supplementation to improve pregnancy and neonatal outcomes. The current literature has clearly demonstrated that vitamin D supplementation is safe at up to 4000 IU/d, and to date, there are no reports of adverse events [4, 5, 21, 23–25].
The primary aim of this study was to determine the prevalence of vitamin D deficiency among the population of pregnant women receiving prenatal care and giving birth in our clinic. Furthermore, we aimed to assess baseline vitamin D levels, as well as the prevalence and degree of severity of vitamin D deficiency among the pregnant population receiving care at our clinic in Switzerland. We also aimed to compare our data to the existing data for the general population and to compare our results to the current Swiss guidelines, which recommend a routine supplementation of 600 IU of vitamin D to every pregnant women, without a prior assessment of their vitamin D levels. Prior assessment of vitamin D levels is only recommended if risk factors are present [16]. We further wanted to identify in our sub-population groups and confirm the known risk factors for vitamin D deficiency among pregnant women. We also wanted to study the influence of vitamin D on various pregnancy outcomes and to suggest how an optimised management strategy for vitamin D supplementation in pregnancy might look if our results are confirmed in further studies.
In 2012, following the release of the Swiss guidelines on vitamin D deficiency by the Federal Commission for Nutrition, we started collecting the baseline vitamin D levels of pregnant subjects to rectify the lack of data on baseline vitamin D levels in pregnant women and the unknown prevalence of vitamin D deficiency in pregnant women in Switzerland.
We now intend to provide, for the first time, data on baseline vitamin D levels in pregnant women in Switzerland, and to explore possible associations of these levels with adverse pregnancy outcomes. This retrospective, observational cross-sectional study was performed at the Department of Obstetrics and Gynaecology of the University Hospital Bern in Switzerland.
The study was approved by the ethics committee of the University of Bern (Ref.-Nr. KEK-BE: 330/2015; Basec: 2015-00063) and was registered on ClinicalTrial.gov. (Identifier: NCT02904720).
Following the Swiss Federal Act on research involving human beings (Human Research Act, HRA) of 30 September 2011 (Status as of 1 January 2014), Art. 33–35, written informed consent for further use of non-genetic health-related personal data is not necessary.
All pregnant women who had their serum vitamin D levels measured during the first or second trimester of their pregnancy and who took prenatal care and had their deliveries at our institution between 2012 and 2015 were included. Vitamin D levels were routinely checked at the first antenatal visit by women taking prenatal care at our clinic. All data were retrieved retrospectively from the patients` electronic files.
In our antenatal clinic, we recommend maternal multivitamin supplementation with Elevit® Pronatal, Bayer, containing 500 IU of vitamin D, to every patient. Additional vitamin D is added according to their individual vitamin D needs. The pregnant subjects were reviewed every 5–6 weeks and their history of adherence was taken. Compliance was reported to be usually quite good. The costs of vitamin D testing and supplementation were covered by the Swiss health insurance system.
In our clinic, supplementation of at least 1000 IU/d was administered orally throughout the pregnancy in cases of deficiency. Women with adequate vitamin D levels were routinely supplemented with 600 IU/d orally, following the Swiss Federal Commission for Nutrition’s recommendations [16]. A follow-up measurement of the vitamin D level was not routinely performed, as it was assumed that vitamin D levels were adequately restored after the course of the treatment.
Using blood samples obtained from a standard venipuncture at admission, a quantitative laboratory analysis of 25-hydroxycholecalciferol (25(OH)D), the precursor form of bioactive vitamin D, was performed in our Center of Laboratory Medicine, Inselspital, University Hospital Bern using chemiluminescent immunoassays (CLIA) on a Liaison XL (Diasorin).
For 25(OH)D, total internal quality control was performed using the LIAISON by Diasorin 25 OH vitamin D total control set (REF 310601), level 1 and 2 in each series, as well as after calibration. The external quality control was done by round robin tests four times a year by the Swiss Centre for Quality Control.
For our study, we established that a sufficient 25(OH)D level was indicated by a value >50 nmol/l. A mild deficiency was present when values were between 25–49 nmol/l, and a severe deficiency was present if levels were below 25 nmol/l [17–20].
We retrospectively reviewed the electronic files of the 1382 selected patients. Relevant data such as body mass index (BMI), origin, season of testing, smoking status, pregnancy outcomes including the occurrence of complications (see below), mode of birth and gestational age at birth, and the neonatal outcomes of birth weight and length were extracted and anonymised.
The adverse pregnancy variables added to the multivariate analysis were selected after reviewing the relevant literature, especially existing reviews and meta-analyses [24, 26–32]. The most frequently studied maternal and fetal adverse outcomes were selected.
Preeclampsia was defined as systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg at two separate times (at least 4 hours apart) in a previously normotensive patient, whether or not associated with the presence of a proteinuria ≥300 mg/24h.
Gestational diabetes mellitus (GDM) was defined following the WHO 2013 criteria (fasting plasma glucose ≥5.1 mmol/l, 1h plasma glucose ≥10 mmol/l, or 2h plasma glucose ≥ 8.5 mmol/l after a standard 75g oral glucose tolerance test performed around the 28th week of gestation).
Postpartum haemorrhage (PPH) was diagnosed in all vaginal deliveries with a blood loss ≥500 ml.
Placental retention was diagnosed when the placenta had not undergone expulsion within 30 minutes after the delivery.
Preterm birth was defined as a delivery which took place before completing the 37th week of gestation.
Postdate pregnancy was defined as a delivery which took place after the 40th week of gestation.
Miscarriage was defined as a clinically recognised pregnancy loss before the 20th week of gestation or as the extraction of an embryo or fetus weighing ≤500 g, following the WHO criteria.
Intrauterine growth restriction (IUGR) was diagnosed when a fetus failed to achieve its growth potential, in the case of progressive deviation from its growth curve or in the case of SGA (fetus with weight <10th percentile) combined with signs of placental insufficiency such as oligohydramnios or abnormal umbilical artery Doppler.
Bacterial vaginosis was diagnosed in the case of clinical symptoms of colpitis associated with a positive vaginal smear test or following the Amsel criteria.
The mode of delivery was classified as vaginal birth or caesarean section.
The primary endpoint, the prevalence of vitamin D deficiency, was analysed with an empirical estimation of the proportion of interest and with a score-type confidence interval.
To identify the risk factors (BMI, ethnicity, religion, smoking status, season at testing) for the numerical primary outcome, a linear regression model was performed. The linear regression analysis was performed by modelling the numerical outcome of vitamin D status. As this was log-normally rather than normally distributed, a log transformation was applied to the outcome.
A backward selection modelling method was chosen because there were many potential risk factors for vitamin D deficiency. Two-way interactions were also considered in order not to miss any important effects. No adjustments were made for potential factors due to the retrospective nature of this study.
A correlation analysis was performed because associations between several perinatal outcomes and the primary outcome were of interest. These outcomes could not be included in the regression model since they could not be seen as predictors of vitamin D status.
For the analysis associations between the numerical primary endpoint and several outcomes, measurements of associations were computed. Numerical outcomes (weight, length and gestational age at birth) were analysed with Pearson’s correlation coefficient.
For the analysis of categorical outcomes (preeclampsia, gestational diabetes, abortion, postpartum haemorrhage, etc.), the numerical primary endpoint was split into two categories describing whether a value was regarded as deficient or not. Following this, odds ratios (ORs) in the case of a dichotomous variable and chi-square tests in the case of a nominally scaled variable were performed.
For all association measures, a confidence interval (CI) and a p-value for the null of no association were also computed. No correction for multiple testing was applied due to the explorative nature of this retrospective observational study. The level of significance was set to 0.05.
All calculations for the statistical analysis were done with R, version 3.2.2. (The R Project for Statistical Computing, Vienna, Austria).
Out of the 1382 women who had vitamin D testing at our clinic, 229 were lost to follow-up. For the assessment of the prevalence of vitamin D deficiency among pregnant Swiss women, all 1382 women who had their vitamin D levels tested were included.
For the second part of this study, which analysed the associations between vitamin D levels and adverse pregnancy outcomes, only the 1153 women for whom we conducted a complete follow-up until the delivery at our clinic were included. The baseline characteristics of the population studied are presented in figure 1 and table 1.
Figure 1 Distribution of the population studied according to their ethnic origin.
Table 1 Baseline characteristics of the population studied.
| Patients with 25(OH)D testing | 1382 | |
| Testing period from April to September (%) | 677 (48.99) | |
| Testing period from October to March (%) | 705 (51.01) | |
| Patients with 25(OH)D testing and follow-up until birth | 1153 | |
| Median maternal age at testing (years) | 30 (IQR 22–38) | |
| Median gestational age at testing (weeks) | 12 (IQR 8–16) | |
| Median BMI (kg/m2) | 23 (IQR 16–30) | |
| Smoking mothers (%) | 70 (6.17) | |
| Ethnic origin (%) | European: | 730 (63.31) |
| - Occidental | - 443 (38.42) | |
| - Southern | - 76 (6.59) | |
| - Eastern | - 189 (16.39) | |
| - Turkish | - 22 (1.91) | |
| Northern Africa | 38 (3.30) | |
| Middle East | 72 (6.24) | |
| South West Asia | 54 (4.68) | |
| Sub-Saharan Africa | 197 (17.09) | |
| Sri Lanka/India | 62 (5.38) | |
Among the 1382 women who had their 25(OH)D serum level tested, only 26.77% had a sufficient vitamin D level (≥50 nmol/l). Mild deficiency, defined as 25(OH)D levels between 25 and 50 nmol/l, was present in 38.93%, while severe deficiency, defined as 25(OH)D levels below 25 nmol/l, was present in 34.2% of all the women tested, which gives an overall rate of vitamin D deficiency (25(OH)D < 50 nmol/l) of 73.23%. These results are presented in table 2.
Table 2 Distribution of vitamin D status among the 1382 patients with vitamin D testing (total = 1382).
| Sufficiency (%) | 370 (26.77) |
| Mild deficiency (%) | 538 (38.93) |
| Severe deficiency (%) | 474 (34.30) |
| Mean serum level of 25(OH)D (nmol/l) | 36.72 (SD 19.6) |
The mean 25(OH)D serum level was 36.72 nmol/l (SD 19.6).
Known risk factors for vitamin D deficiency were confirmed by our findings and are presented in table 3.
Table 3 Linear model for vitamin D status and risk factors*.
| Variable | Estimate | Std error | t value | p-value |
|---|---|---|---|---|
| (Intercept) | 3.8366 | 0.125895 | 30.4750 | <0.0001 |
| Ethnicity | 0.6418 | 0.0372 | 17.2320 | <0.0001 |
| BMI | −0.0220 | 0.0035 | −6.2870 | <0.0001 |
| Smoking | −0.0045 | 0.0615 | −0.0730 | 0.9419 |
| Season at testing | −0.1950 | 0.0349 | −5.5880 | <0.0001 |
| Gestational age at testing | 0.0047 | 0.0030 | 1.5850 | 0.1133 |
* The modelled outcome was the numerical vitamin D status
Patients who had blood samples taken during the period from October to March were more likely to have a vitamin D deficiency than those who were tested between April and September (p <0.0001). Patients with higher BMI values were significantly more likely to suffer from vitamin D deficiency (p <0.0001). Smoking was not found to be a risk factor for vitamin D deficiency (p = 0.0924).
The statistical analysis demonstrated that subjects of European descent (including western + eastern + southern Europe and Turkey) and those from North Africa, the Middle East and Asia, i.e., people with lighter skin, are significantly less likely to show a vitamin D deficiency compared to Africans or Sri Lankans/Indians (p <0.0001), i.e., people with darker skin living in Switzerland. The results for the various ethnic groups are summarised in figures 2 and 3 .
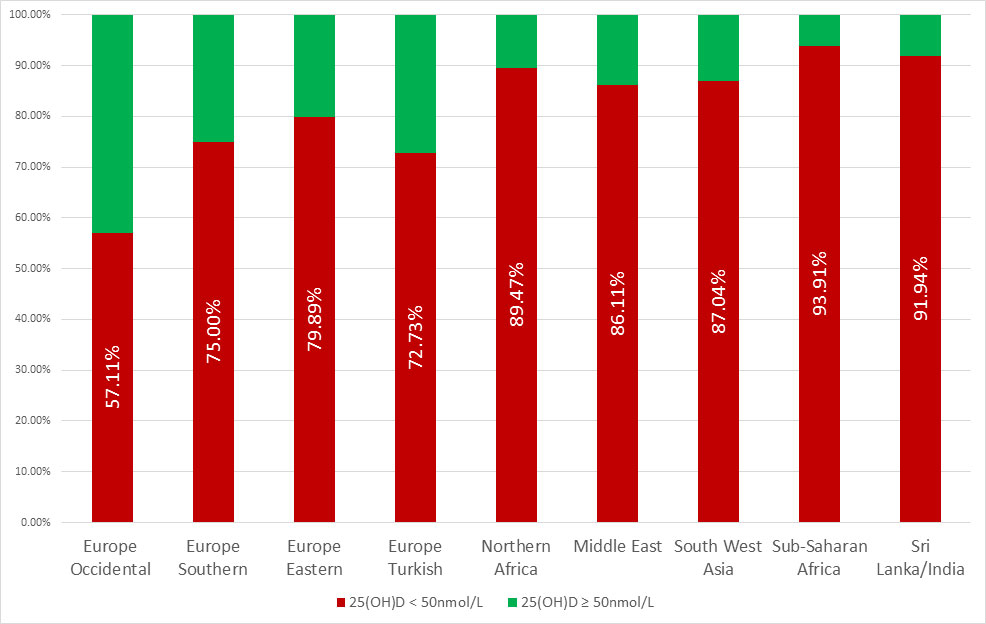
Figure 2 Vitamin D status among the various ethnic origins.
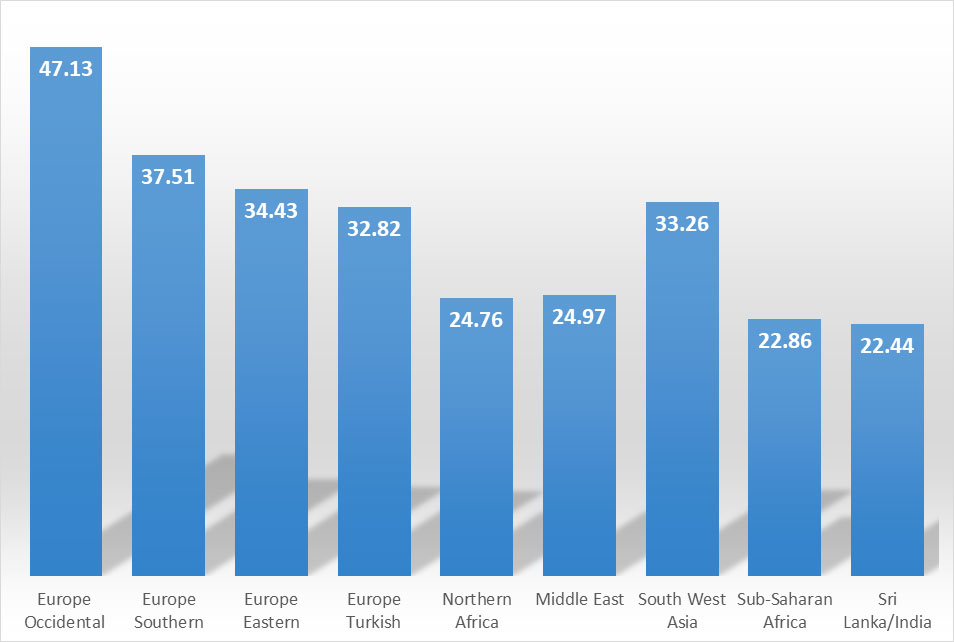
Figure 3 Mean value of 25(OH)D according to the various ethnic origins.
A statistically significant association with vitamin D deficiency was found only for the development of gestational diabetes (p = 0.0116; OR = 0.5932, 95%CI 0.3872–0.8826). Postpartum haemorrhage and placental retention, which can be regrouped under “abnormalities of third stage of labour”, were found to be less likely in patients with a lower vitamin D status (p = 0.0188 and p = 0.0277).
No significant association could be observed between the vitamin D status and the occurrence of:
Interestingly, gestational age at birth was closely negatively correlated with vitamin D level (correlation coefficient −0.0978, 95%CI −0.1498 to −0.0453; p = 0.0003). This means that low vitamin D levels were not associated with preterm births, but on the contrary, the lower the vitamin D level, the higher the gestational age at birth. No significant correlations were found concerning newborn weight (p = 0.2006) or length (p = 0.5808).
The results concerning the associations between low vitamin D levels and pregnancy outcomes/complications are presented in tables 4 and 5 .
Table 4Associations between vitamin D status and pregnancy outcomes.
| Outcome | n (%) | % with vitamin D deficiency | Mean vitamin D (nmol/l) | SD | OR | 95% confidence interval | p-value |
|---|---|---|---|---|---|---|---|
| Gestational diabetes | 167 (14.5) | 81.44 | 36.31 | 19.59 | 0.5932 | 0.3872–0.8826 | 0.0116 |
| Bacterial vaginosis | 36 (3.1) | 77.78 | 40.62 | 19.41 | 0.6912 | 0.2730–1.5181 | 0.4420 |
| Preeclampsia | 24 (2.1) | 87.50 | 33.46 | 19.37 | 0.4042 | 0.0914–1.1900 | 0.1606 |
| SGA/IUGR | 109 (9.5) | 77.06 | 38.05 | 19.45 | 0.7961 | 0.4911–1.2473 | 0.3695 |
| Prematurity | 85 (7.4) | 68.24 | 41.63 | 19.70 | 1.2769 | 0.7855–2.0322 | 0.3154 |
| Miscarriage | 46 (4) | 84.78 | 36.56 | 19.54 | 0.5050 | 0.2030–1.0768 | 0.0892 |
| Delivery by caesarean section | 388 (33.7) | 75.52 | 39.12 | 19.65 | 1.1968 | 0.9154–1.5744 | 0.1992 |
| Prolonged pregnancy | 129 (153) | 74.42 (74.51) | 41.99 (27.29) | 19.64 | 0.9292 | 0.6056–1.3930 | 0.7558 |
| Placental retention | 46 (4) | 58.70 | 46.73 | 19.39 | 1.9841 | 1.0709–3.6044 | 0.0277 |
| Postpartum haemorrhage | 90 (7.8) | 62.22 | 46.34 | 19.60 | 1.7349 | 1.1023–2.6935 | 0.0188 |
IUGR = intrauterine growth restriction; OR = odds ratio; SD = standard deviation; SGA = small for gestational age
Table 5 Associations for numerical outcomes.
| Outcome | Mean value | Standard deviation | Correlation coefficient | Confidence interval | p-value |
|---|---|---|---|---|---|
| Weight of neonate at birth | 3337.3g | 1148.16 | 0.0434 | −0.0231 to 0.1095 | 0.2006 |
| Length of neonate at birth | 49.3cm | 2.83 | −0.0189 | −0.0858 to 0.0482 | 0.5808 |
| Gestational age at birth | 39th 2/7 | 2.35 | −0.0978 | −0.1498 to −0.0453 | 0.0003 |
Our study is the first large cross-sectional cohort study of 25(OH)D level measurements in pregnant women in Switzerland, showing that three quarters of them are vitamin D deficient and over one third are severely vitamin D deficient. This corresponds to our primary hypothesis that pregnant women have a much higher prevalence of severe vitamin D deficiency compared to the rate for the general population in Switzerland stated in the Swiss Federal Commission for Nutrition report [16]. This finding has consequences for vitamin D supplementation recommendations in Switzerland. Currently, supplementation of 600 IU is recommended for all pregnant and breastfeeding women. For women with a severe vitamin D deficiency, supplementation of 1500–2000 IU is recommended, as stated in the Swiss Federal Commission guidelines. However, general serum measurements are not currently recommended.
The effect of the supplementation of 600 IU vitamin D on 25(OH)D levels can be estimated using the dose–response calculations proposed by Heaney. The administration of 400 IU is expected to increase 25(OH)D concentrations by about 10.0 nmol/l [33]. This means that even if 800 IU vitamin D were to be supplemented to all pregnant women, over a third would not reach the recommended minimum threshold level of 50 nmol/l. There are recent publications of RCTs highlighting the fact that a 600 IU daily supplement is insufficient to prevent vitamin D deficiency, and that higher dosing of vitamin D is required to establish sufficiency [4, 21, 23].
The current literature contains conflicting evidence regarding the association between vitamin deficiency and adverse pregnancy outcomes. A recent Cochrane review of 30 randomised and quasi-randomised trials concluded that supplementing pregnant women with vitamin D alone probably reduces the risk of preeclampsia, gestational diabetes and low birthweight, and may reduce the risk of severe postpartum haemorrhage [34]. However, additional rigorous, high-quality and larger randomised trials are required to evaluate the effects of vitamin D supplementation in pregnancy, particularly in relation to the risk of maternal adverse events. This is in accordance with the conclusions of many other studies and meta-analyses, with a wide heterogeneity of populations studied and applied methodologies for both vitamin D substitution and assessment, on the relationship between maternal vitamin D status and pregnancy outcomes [35–37].
In line with general clinical practice, we measured only total 25(OH)D. However, there are recent data indicating that free 25(OH)D might be superior to routine total 25(OH)D as a characteristic of vitamin D status in pregnancy [38].
Our findings regarding the prevalence of vitamin D deficiency are in line with several published studies from all over the world. One of them, conducted in northern Italy, observed a prevalence of vitamin D deficiency of 70.6% [39]. In a 2018 study from Saudi Arabia, the prevalence was as high as 82.5% [40]. A Chinese study obtained almost the same result, with a prevalence of 82.6% [6]. On the contrary, a recently published Australian study reported a much lower percentage of pregnant women with a vitamin D deficiency, but that difference can be easily explained by differences in sun exposure [41]. We found two recently published Swiss studies that reported slightly lower prevalences of vitamin D deficiency. The first one included 204 patients and focused on differences in the rates of vitamin D deficiency detected in pregnant women depending on their skin color. It found that overall, 63% of these women were vitamin D deficient [42]. The second study included 305 patients and obtained a prevalence of vitamin D deficiency of 53.4% [43].
Our study confirms most of the risk factors for vitamin D deficiency reported in the literature (winter season, BMI, ethnic groups with darker skin, smoking status). Indeed, our results show the presence of a significant seasonal variability of vitamin D status. We also found an inverse relationship between vitamin D status and BMI, which is explained by a smaller skin surface area for vitamin D synthesis in comparison to the total body volume [44]. Our results do not confirm smoking as a risk factor for vitamin D [45]. Like several others [39, 42, 46–48], our study confirms that populations from Southeast Asia and Africa have a significantly higher risk of vitamin D deficiency than the occidental population. This difference between the various ethnic groups has been explained in the literature: it is due to the degree of skin pigmentation, which influences the ability of the body to absorb sunlight for the synthesis of vitamin D [1]. This is of increasing interest in view of current global migration patterns.
Like numerous others, our study confirms the association between low vitamin D levels and the occurrence of gestational diabetes mellitus (GDM) [40, 41, 46, 49]. An Australian study from 2014 [46] reported a seven-fold increase in the likelihood of developing GDM if the women were vitamin D deficient during the early stages of pregnancy. Another Australian study, published in 2018, observed a 53% decreased risk for gestational diabetes mellitus in women with high (> 81 nmol/l) "standardised" vitamin D status when compared to moderate to high (63−81 nmol/l) [41]. In a multiethnic cohort of 745 pregnant women from Norway, a higher proportion of women from ethnic minorities had GDM (p <0.01) and low 25(OH)D levels (p <0.01), compared to European women. However, after adjustments for confounding factors, in particular ethnicity, vitamin D deficiency was not associated with GDM [50].
A meta-analysis from 2014, based on 20 observational studies and regrouping up to 9200 patients, also indicated a consistent association between vitamin D deficiency and an increased risk of GDM [51]. A meta-analysis of 29 observational studies conducted in 2018, which included 28,982 participants of whom 4634 were diagnosed with gestational diabetes, showed that maternal vitamin D insufficiency was associated with a significant increase in the risk of gestational diabetes of 39% (pooled OR 1.39, 95%CI 1.20−1.60), with moderate heterogeneity (I2 50.2%; p = 0.001) [52].
Another meta-analysis of 26 studies found that vitamin D deficiency among mothers in general may be related to an increased risk of gestational diabetes (OR 1.18, 95%CI 1.01−1.35; p <0.001). Subgroup analysis showed that the results concerning this association may vary with study design but do not change with country of origin [53].
Gestational diabetes is strongly associated with an adverse pregnancy outcome, as well as with long-term adverse effects on the offspring, which likely occur due to epigenetic modifications of the fetal genome (fetal programming), which is exposed to altered conditions in diabetic mothers. The impact of gestational diabetes in pregnancy and on the offspring’s future shows a need to find efficient prevention and intervention strategies. A question that should be raised is whether vitamin D supplementation is helpful in preventing the development of gestational diabetes, a condition that develops in about 2–5% of all pregnant women and has become considerably more common during the last decade [54].
To our knowledge, three recently published double-blind RCTs presented positive data regarding the effect of vitamin D supplementation on GDM. Vitamin D supplementation during the first and second trimesters of pregnancy was effective in reducing GDM and controlling the glucose tolerance test [55]. A high dose of vitamin D supplementation (50,000 IU every 2 weeks) significantly improved insulin resistance in pregnant women with GDM [56], and supplementation among pregnant women with GDM resulted in a decrease in the occurrence of maternal polyhydramnios and infant hyperbilirubinemia compared with a placebo [57].
Surprisingly, our results show a significant inverse relationship between vitamin D status and the occurrence of both postpartum haemorrhage and placental retention. We do not have an explanation for this finding and very few existing publications address this subject. A case-control study found that women with uterine atony had a significantly lower mean of vitamin D concentration than those without uterine atony, which could be explained by the fact that low vitamin D can result in muscle weakness. Another study [46] did not find any such association.
Similar to our study, there have been observational studies [46, 47] which showed negative results for any association between vitamin D levels and preeclampsia. A meta-analysis of 12 studies from 2014 [58] suggested that low maternal serum 25(OH)D concentrations increase the risk of preeclampsia and that vitamin D supplementation lowers this risk. However, the quality of evidence was insufficient to determine a causal association. Another study [59], based on data from up to 700 patients who developed preeclampsia, concluded that vitamin D deficiency may be a risk factor for severe preeclampsia, but that it is not associated with preeclampsia overall or its mild subtypes. A recently updated meta-analysis of 23 studies found that vitamin D deficiency (25(OH)D <20 ng/ml = <50 nmol/l) was significantly associated with a risk of preeclampsia (fixed p <0.0001; random p = 0.0029; fixed OR = 1.33; random OR = 1.54) and that this association can be specific up to 90% at a 10.60 ng/ml cut-off [60]. The findings on the relationship between vitamin D deficiency and preeclampsia in the literature are therefore inconclusive, possibly because, according to Hollis and Wagner, supplementation should occur prior to placentation [21].
Yet again, in agreement with our study, there are published results showing a lack of any significant association between vitamin D and SGA and/or low birth weight. However, many observational studies [3, 61] have shown that women with lower vitamin D levels are more likely to give birth to SGA fetuses, and pregnant women who deliver SGA fetuses have lower vitamin D levels. This has been explained by the action of vitamin D on bone formation and the known fact that birth weight is directly correlated with skeletal growth.
Our results did not demonstrate any association between vitamin D status and the occurrence of bacterial vaginosis, pregnancy losses or prematurity.
Several observational studies [3, 51] have found that women with a lower vitamin D status have a higher risk of bacterial vaginosis. The underlying mechanism is possibly related to the role that calcitriol plays in the immune system. By reducing susceptibility to infections, vitamin D could also be a protective factor against the premature rupture of the membranes and prevent prematurity.
Few studies concerning the connection between vitamin D and prematurity are available. We found only one study with significant results, a retrospective case–control study [62] which concluded that vitamin D levels were significantly lower in women who delivered at preterm compared to in those who delivered at full term.
As an immune modulator, vitamin D also plays a role in maternal immunosuppression, without which the fetus could not survive. Therefore, vitamin D deficiency has been implicated as a risk factor for recurrent pregnancy losses. There is limited data available concerning this last outcome. However, a recent study from Denmark reported that concentrations of 25(OH)D <50 nmol/l were associated with a greater than two-fold increase in the adjusted hazard ratio for first-semester miscarriage [63]. A recent review of the literature on recurrent pregnancy loss included 11 studies which reported a high prevalence of vitamin D insufficiency/deficiency in women with recurrent pregnancy loss and suggested that this could be associated with immunological dysregulation and consequently with recurrent pregnancy loss. However, there is currently no evidence concerning the benefits of supplementation on this outcome [64].
Few studies have assessed the mode of delivery. However, most of those that have are similar to ours in the sense that they did not demonstrate any significant association between vitamin D and delivery by caesarean section [3, 46, 65]. In a cross-sectional study by Merewood et al. in 2009 [66], delivery by caesarean section was almost four times more common in women with vitamin D levels < 37.5 nmol/l compared to those with levels over 80 nmol/l. Similar to the ideas around uterine atony, the theory is that low vitamin D can result in muscle weakness and negatively affect the stages of labour.
This study is one of the first large studies presenting data on the vitamin D status of pregnant women in the first trimester in Switzerland. The data highlight the magnitude of the problem and raise awareness of this global health issue. Our data also show that vitamin D deficiency is not a problem restricted to developing countries, but also affects pregnant women in developed countries.
These data also contribute to establishing a possible link between vitamin D deficiency and gestational diabetes mellitus.
This study has two further major strengths. The first is the large number of included subjects. The second is that the study population was not a selective cohort of typical Swiss women, but a longitudinal sample of the overall population living in a modern Swiss city, which is much more representative of the daily practice.
Limitations of this analysis result firstly from the retrospective nature of the study and the difficulty in recalling past events. This may contribute to possible biases in the study.
As we only included the most frequently studied adverse maternal and fetal outcomes after a narrative review of the literature, less frequent adverse events like hypercalcemia of newborns were not included.
There are several parameters, like dietary and lifestyle habits, sunshine exposure and clothing preferences, which would have been of interest. However, we were unable to obtain the data to allow us to include them in the analysis.
It would have also been quite interesting to incorporate the follow-up results of the vitamin D levels from the second and third trimesters. However, no results were available for this population as we assumed that vitamin D levels would, by then, have returned to the normal range. Nevertheless, we now recognise that it would have been of value to check the vitamin D levels. Therefore, we have subsequently introduced a follow-up check of vitamin D levels in the second trimester.
Due to the retrospective nature of the study, no structured data on the vitamin D supplementation could be provided. The pregnant subjects were reviewed every 5–6 weeks and the history of adherence was taken, with compliance good overall.
Low levels of vitamin D appear to be associated with both positive and negative outcomes. Therefore, the resulting available evidence needs to be interpreted with caution. However, it remains unclear whether this association is causal, owing to the observational design of the study.
We are aware that our findings must be interpreted with caution and that further research is needed to provide more evidence on this topic and to promote a change in the guidelines.
Despite the many important health benefits of vitamin D, there is controversy regarding the definition of vitamin D deficiency and what the vitamin D requirement should be. In addition, critical windows of exposure to adequate vitamin D levels during fetal maturation remain to be defined [67].
Our study shows a high prevalence of severe vitamin D deficiency in pregnant women. Furthermore, the data suggest that vitamin D deficiency is linked to gestational diabetes.
In our opinion, the current recommendations of vitamin D supplementation of 600 IU in pregnant women are insufficient to establish an adequate vitamin D level. Novel strategies such as general 25(OH)D measurement in pregnancy and adjusted supplementation of vitamin D should be evaluated in further studies, potentially leading to improved maternal health and benefits to children’s long-term health in Switzerland and worldwide. Pre-conception supplementation of vitamin D, as is recommended for folic acid, may even be considered as part of a novel approach, so that women begin their pregnancy with already sufficient levels of vitamin D, especially as there are no negative effects to be expected from starting supplementation earlier.
Further well-designed studies are required to assess the efficacy of targeted, 25(OH)D level-adjusted vitamin D supplementation during pregnancy on vitamin D levels in newborns and, finally, on clinical outcomes. This is of utmost importance, as ensuring a sufficient supply of vitamin D in both the mother and the child has great potential for the prevention of birth complications and significantly affects the health of the child throughout his/her life.
The authors acknowledge the hospital, the gynaecologist-obstetricians, the midwives and the patients who permitted the realisation of this study. We would also like to acknowledge G. Fischer for his statistical analysis.
The study was supported by a grant of the Research Fund, Department of Obstetrics and Gynaecology, University Hospital Bern, Switzerland.
The authors have no conflicts of interest to declare.
1 Wacker M , Holick MF . Vitamin D - effects on skeletal and extraskeletal health and the need for supplementation. Nutrients. 2013;5(1):111–48. doi:.https://doi.org/10.3390/nu5010111
2 Kaushal M , Magon N . Vitamin D in pregnancy: A metabolic outlook. Indian J Endocrinol Metab. 2013;17(1):76–82. doi:.https://doi.org/10.4103/2230-8210.107862
3 Aghajafari F , Nagulesapillai T , Ronksley PE , Tough SC , O’Beirne M , Rabi DM . Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: systematic review and meta-analysis of observational studies. BMJ. 2013;346(mar26 4):f1169. doi:.https://doi.org/10.1136/bmj.f1169
4 Dawodu A , Saadi HF , Bekdache G , Javed Y , Altaye M , Hollis BW . Randomized controlled trial (RCT) of vitamin D supplementation in pregnancy in a population with endemic vitamin D deficiency. J Clin Endocrinol Metab. 2013;98(6):2337–46. doi:.https://doi.org/10.1210/jc.2013-1154
5 Rostami M , Tehrani FR , Simbar M , Bidhendi Yarandi R , Minooee S , Hollis BW , et al. Effectiveness of Prenatal Vitamin D Deficiency Screening and Treatment Program: A Stratified Randomized Field Trial. J Clin Endocrinol Metab. 2018;103(8):2936–48. doi:.https://doi.org/10.1210/jc.2018-00109
6 Fu CW , Liu JT , Tu WJ , Yang JQ , Cao Y . Association between serum 25-hydroxyvitamin D levels measured 24 hours after delivery and postpartum depression. BJOG. 2015;122(12):1688–94. doi:.https://doi.org/10.1111/1471-0528.13111
7 McGrath J . Does ‘imprinting’ with low prenatal vitamin D contribute to the risk of various adult disorders? Med Hypotheses. 2001;56(3):367–71. doi:.https://doi.org/10.1054/mehy.2000.1226
8 Ponsonby AL , Lucas RM , Lewis S , Halliday J . Vitamin D status during pregnancy and aspects of offspring health. Nutrients. 2010;2(3):389–407. doi:.https://doi.org/10.3390/nu2030389
9 Roth DE , Leung M , Mesfin E , Qamar H , Watterworth J , Papp E . Vitamin D supplementation during pregnancy: state of the evidence from a systematic review of randomised trials. BMJ. 2017;359:j5237. doi:.https://doi.org/10.1136/bmj.j5237
10 Schmidt RJ , Niu Q , Eyles DW , Hansen RL , Iosif AM . Neonatal vitamin D status in relation to autism spectrum disorder and developmental delay in the CHARGE case-control study. Autism Res. 2019;12(6):976–88. doi:.https://doi.org/10.1002/aur.2118
11 Al-Garawi A , Carey VJ , Chhabra D , Mirzakhani H , Morrow J , Lasky-Su J , et al. The Role of Vitamin D in the Transcriptional Program of Human Pregnancy. PLoS One. 2016;11(10):e0163832. doi:.https://doi.org/10.1371/journal.pone.0163832
12 Olsen SF , Secher NJ . A possible preventive effect of low-dose fish oil on early delivery and pre-eclampsia: indications from a 50-year-old controlled trial. Br J Nutr. 1990;64(3):599–609. doi:.https://doi.org/10.1079/BJN19900063
13 Goldring ST , Griffiths CJ , Martineau AR , Robinson S , Yu C , Poulton S , et al. Prenatal vitamin d supplementation and child respiratory health: a randomised controlled trial. PLoS One. 2013;8(6):e66627. doi:.https://doi.org/10.1371/journal.pone.0066627
14 Mirzakhani H , Litonjua AA , McElrath TF , O’Connor G , Lee-Parritz A , Iverson R , et al. Early pregnancy vitamin D status and risk of preeclampsia. J Clin Invest. 2016;126(12):4702–15. doi:.https://doi.org/10.1172/JCI89031
15 Bahrami A , Sadeghnia HR , Tabatabaeizadeh SA , Bahrami-Taghanaki H , Behboodi N , Esmaeili H , et al. Genetic and epigenetic factors influencing vitamin D status. J Cell Physiol. 2018;233(5):4033–43. doi:.https://doi.org/10.1002/jcp.26216
16Nutrition ESFCf. Vitamin D deficiency: Evidence, safety, and recommendations for the Swiss Population. 2012, Swiss Federal Office for Public Health.
17World Health Organization. Guidelines: Vitamin D supplementation in pregnant women. Geneva: WHO; 2012.
18 Ross AC , Manson JE , Abrams SA , Aloia JF , Brannon PM , Clinton SK , et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab. 2011;96(1):53–8. doi:.https://doi.org/10.1210/jc.2010-2704
19 Bischoff-Ferrari HA , Giovannucci E , Willett WC , Dietrich T , Dawson-Hughes B . Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr. 2006;84(1):18–28. doi:.https://doi.org/10.1093/ajcn/84.1.18
20 EFSA Panel on Dietetic Products. Dietary reference values for vitamin D. EFSA J. 2016;14(10):e04547. doi:.https://doi.org/10.2903/j.efsa.2016.4547
21 Hollis BW , Wagner CL . Vitamin D supplementation during pregnancy: Improvements in birth outcomes and complications through direct genomic alteration. Mol Cell Endocrinol. 2017;453:113–30. doi:.https://doi.org/10.1016/j.mce.2017.01.039
22 Bouillon R . Comparative analysis of nutritional guidelines for vitamin D. Nat Rev Endocrinol. 2017;13(8):466–79. doi:.https://doi.org/10.1038/nrendo.2017.31
23 Enkhmaa D , Tanz L , Ganmaa D , Enkhtur S , Oyun-Erdene B , Stuart J , et al. Randomized trial of three doses of vitamin D to reduce deficiency in pregnant Mongolian women. EBioMedicine. 2019;39:510–9. doi:.https://doi.org/10.1016/j.ebiom.2018.11.060
24 Hollis BW , Johnson D , Hulsey TC , Ebeling M , Wagner CL . Vitamin D supplementation during pregnancy: double-blind, randomized clinical trial of safety and effectiveness. J Bone Miner Res. 2011;26(10):2341–57. doi:.https://doi.org/10.1002/jbmr.463
25 Wolsk HM , Chawes BL , Litonjua AA , Hollis BW , Waage J , Stokholm J , et al. Prenatal vitamin D supplementation reduces risk of asthma/recurrent wheeze in early childhood: A combined analysis of two randomized controlled trials. PLoS One. 2017;12(10):e0186657. doi:.https://doi.org/10.1371/journal.pone.0186657
26 Thorp JM , Camargo CA , McGee PL , Harper M , Klebanoff MA , Sorokin Y , et al.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Vitamin D status and recurrent preterm birth: a nested case-control study in high-risk women. BJOG. 2012;119(13):1617–23. doi:.https://doi.org/10.1111/j.1471-0528.2012.03495.x
27 Abedi P , Mohaghegh Z , Afshary P , Latifi M . The relationship of serum vitamin D with pre-eclampsia in the Iranian women. Matern Child Nutr. 2014;10(2):206–12. doi:.https://doi.org/10.1111/mcn.12058
28 Bennett SE , McPeake J , McCance DR , Manderson JG , Johnston P , McGalliard R , et al. Maternal vitamin D status in Type 1 diabetic pregnancy: Impact on neonatal vitamin D status and association with maternal glycaemic control. Pregnancy Hypertens. 2014;4(3):235–6. doi:.https://doi.org/10.1016/j.preghy.2014.03.020
29 Mutlu N , Esra H , Begum A , Fatma D , Arzu Y , Yalcin H , et al. Relation of maternal vitamin D status with gestational diabetes mellitus and perinatal outcome. Afr Health Sci. 2015;15(2):523–31. doi:.https://doi.org/10.4314/ahs.v15i2.27
30 Kiely ME , Zhang JY , Kinsella M , Khashan AS , Kenny LC . Vitamin D status is associated with uteroplacental dysfunction indicated by pre-eclampsia and small-for-gestational-age birth in a large prospective pregnancy cohort in Ireland with low vitamin D status. Am J Clin Nutr. 2016;104(2):354–61. doi:.https://doi.org/10.3945/ajcn.116.130419
31 Wagner CL , McNeil RB , Johnson DD , Hulsey TC , Ebeling M , Robinson C , et al. Health characteristics and outcomes of two randomized vitamin D supplementation trials during pregnancy: a combined analysis. J Steroid Biochem Mol Biol. 2013;136:313–20. doi:.https://doi.org/10.1016/j.jsbmb.2013.01.002
32 Jefferson KK , Parikh HI , Garcia EM , Edwards DJ , Serrano MG , Hewison M , et al. Relationship between vitamin D status and the vaginal microbiome during pregnancy. J Perinatol. 2019;39(6):824–36. doi:.https://doi.org/10.1038/s41372-019-0343-8
33 Heaney RP . The Vitamin D requirement in health and disease. J Steroid Biochem Mol Biol. 2005;97(1-2):13–9. doi:.https://doi.org/10.1016/j.jsbmb.2005.06.020
34 Palacios C , Kostiuk LK , Peña-Rosas JP . Vitamin D supplementation for women during pregnancy. Cochrane Database Syst Rev. 2019;7:CD008873. doi:.https://doi.org/10.1002/14651858.CD008873.pub4
35 von Websky K , Hasan AA , Reichetzeder C , Tsuprykov O , Hocher B . Impact of vitamin D on pregnancy-related disorders and on offspring outcome. J Steroid Biochem Mol Biol. 2018;180:51–64. doi:.https://doi.org/10.1016/j.jsbmb.2017.11.008
36 Roth DE , Leung M , Mesfin E , Qamar H , Watterworth J , Papp E . Vitamin D supplementation during pregnancy: state of the evidence from a systematic review of randomised trials. BMJ. 2017;359:j5237. doi:.https://doi.org/10.1136/bmj.j5237
37 Reichetzeder C , Chen H , Föller M , Slowinski T , Li J , Chen YP , et al. Maternal vitamin D deficiency and fetal programming--lessons learned from humans and mice. Kidney Blood Press Res. 2014;39(4):315–29. doi:.https://doi.org/10.1159/000355809
38 Tsuprykov O , Chen X , Hocher CF , Skoblo R , Lianghong Yin , Hocher B . Why should we measure free 25(OH) vitamin D? J Steroid Biochem Mol Biol. 2018;180:87–104. doi:.https://doi.org/10.1016/j.jsbmb.2017.11.014
39 Cadario F , Savastio S , Magnani C , Cena T , Pagliardini V , Bellomo G , et al. High Prevalence of Vitamin D Deficiency in Native versus Migrant Mothers and Newborns in the North of Italy: A Call to Act with a Stronger Prevention Program. PLoS One. 2015;10(6):e0129586. doi:.https://doi.org/10.1371/journal.pone.0129586
40 Al-Ajlan A , Al-Musharaf S , Fouda MA , Krishnaswamy S , Wani K , Aljohani NJ , et al. Lower vitamin D levels in Saudi pregnant women are associated with higher risk of developing GDM. BMC Pregnancy Childbirth. 2018;18(1):86. doi:.https://doi.org/10.1186/s12884-018-1723-3
41 Wilson RL , Leviton AJ , Leemaqz SY , Anderson PH , Grieger JA , Grzeskowiak LE , et al. Vitamin D levels in an Australian and New Zealand cohort and the association with pregnancy outcome. BMC Pregnancy Childbirth. 2018;18(1):251. doi:.https://doi.org/10.1186/s12884-018-1887-x
42 Richard A , Rohrmann S , Quack Lötscher KC . Prevalence of Vitamin D Deficiency and Its Associations with Skin Color in Pregnant Women in the First Trimester in a Sample from Switzerland. Nutrients. 2017;9(3):260. doi:.https://doi.org/10.3390/nu9030260
43 Krieger JP , Cabaset S , Canonica C , Christoffel L , Richard A , Schröder T , et al. Prevalence and determinants of vitamin D deficiency in the third trimester of pregnancy: a multicentre study in Switzerland. Br J Nutr. 2018;119(3):299–309. doi:.https://doi.org/10.1017/S0007114517003634
44 Lagunova Z , Porojnicu AC , Lindberg F , Hexeberg S , Moan J . The dependency of vitamin D status on body mass index, gender, age and season. Anticancer Res. 2009;29(9):3713–20.
45 Banihosseini SZ , Baheiraei A , Shirzad N , Heshmat R , Mohsenifar A . The effect of cigarette smoke exposure on vitamin D level and biochemical parameters of mothers and neonates. J Diabetes Metab Disord. 2013;12(1):19. doi:.https://doi.org/10.1186/2251-6581-12-19
46 Davies-Tuck M , Yim C , Knight M , Hodges R , Doery JC , Wallace E . Vitamin D testing in pregnancy: Does one size fit all? Aust N Z J Obstet Gynaecol. 2015;55(2):149–55. doi:.https://doi.org/10.1111/ajo.12278
47 Flood-Nichols SK , Tinnemore D , Huang RR , Napolitano PG , Ippolito DL . Vitamin D deficiency in early pregnancy. PLoS One. 2015;10(4):e0123763. doi:.https://doi.org/10.1371/journal.pone.0123763
48 van der Meer IM , Karamali NS , Boeke AJ , Lips P , Middelkoop BJ , Verhoeven I , et al. High prevalence of vitamin D deficiency in pregnant non-Western women in The Hague, Netherlands. Am J Clin Nutr. 2006;84(2):350–3, quiz 468–9. doi:.https://doi.org/10.1093/ajcn/84.2.350
49 Xu C , Ma HH , Wang Y . Maternal Early Pregnancy Plasma Concentration of 25-Hydroxyvitamin D and Risk of Gestational Diabetes Mellitus. Calcif Tissue Int. 2018;102(3):280–6. doi:.https://doi.org/10.1007/s00223-017-0346-4
50 Eggemoen AR , Waage CW , Sletner L , Gulseth HL , Birkeland KI , Jenum AK . Vitamin D, Gestational Diabetes, and Measures of Glucose Metabolism in a Population-Based Multiethnic Cohort. J Diabetes Res. 2018;2018:8939235. doi:.https://doi.org/10.1155/2018/8939235
51 Zhang MX , Pan GT , Guo JF , Li BY , Qin LQ , Zhang ZL . Vitamin D Deficiency Increases the Risk of Gestational Diabetes Mellitus: A Meta-Analysis of Observational Studies. Nutrients. 2015;7(10):8366–75. doi:.https://doi.org/10.3390/nu7105398
52 Hu L , Zhang Y , Wang X , You L , Xu P , Cui X , et al. Maternal Vitamin D Status and Risk of Gestational Diabetes: a Meta-Analysis. Cell Physiol Biochem. 2018;45(1):291–300. doi:.https://doi.org/10.1159/000486810
53 Amraei M , Mohamadpour S , Sayehmiri K , Mousavi SF , Shirzadpour E , Moayeri A . Effects of Vitamin D Deficiency on Incidence Risk of Gestational Diabetes Mellitus: A Systematic Review and Meta-analysis. Front Endocrinol (Lausanne). 2018;9:7. doi:.https://doi.org/10.3389/fendo.2018.00007
54 Monteiro LJ , Norman JE , Rice GE , Illanes SE . Fetal programming and gestational diabetes mellitus. Placenta. 2016;48(Suppl 1):S54–60. doi:.https://doi.org/10.1016/j.placenta.2015.11.015
55 Shahgheibi S , Farhadifar F , Pouya B . The effect of vitamin D supplementation on gestational diabetes in high-risk women: Results from a randomized placebo-controlled trial. J Res Med Sci. 2016;21(1):2. doi:.https://doi.org/10.4103/1735-1995.175148
56 Zhang Q , Cheng Y , He M , Li T , Ma Z , Cheng H . Effect of various doses of vitamin D supplementation on pregnant women with gestational diabetes mellitus: A randomized controlled trial. Exp Ther Med. 2016;12(3):1889–95. doi:.https://doi.org/10.3892/etm.2016.3515
57 Asemi Z , Karamali M , Esmaillzadeh A . Favorable effects of vitamin D supplementation on pregnancy outcomes in gestational diabetes: a double blind randomized controlled clinical trial. Horm Metab Res. 2015;47(8):565–70.
58 Hyppönen E , Cavadino A , Williams D , Fraser A , Vereczkey A , Fraser WD , et al. Vitamin D and pre-eclampsia: original data, systematic review and meta-analysis. Ann Nutr Metab. 2013;63(4):331–40. doi:.https://doi.org/10.1159/000358338
59 Bakacak M , Serin S , Ercan O , Köstü B , Avci F , Kılınç M , et al. Comparison of Vitamin D levels in cases with preeclampsia, eclampsia and healthy pregnant women. Int J Clin Exp Med. 2015;8(9):16280–6.
60 Akbari S , Khodadadi B , Ahmadi SAY , Abbaszadeh S , Shahsavar F . Association of vitamin D level and vitamin D deficiency with risk of preeclampsia: A systematic review and updated meta-analysis. Taiwan J Obstet Gynecol. 2018;57(2):241–7. doi:.https://doi.org/10.1016/j.tjog.2018.02.013
61 Olmos-Ortiz A , Avila E , Durand-Carbajal M , Díaz L . Regulation of calcitriol biosynthesis and activity: focus on gestational vitamin D deficiency and adverse pregnancy outcomes. Nutrients. 2015;7(1):443–80. doi:.https://doi.org/10.3390/nu7010443
62 Thota C , Menon R , Fortunato SJ , Brou L , Lee JE , Al-Hendy A . 1,25-Dihydroxyvitamin D deficiency is associated with preterm birth in African American and Caucasian women. Reprod Sci. 2014;21(2):244–50. doi:.https://doi.org/10.1177/1933719113493513
63 Andersen LB , Jørgensen JS , Jensen TK , Dalgård C , Barington T , Nielsen J , et al. Vitamin D insufficiency is associated with increased risk of first-trimester miscarriage in the Odense Child Cohort. Am J Clin Nutr. 2015;102(3):633–8. doi:.https://doi.org/10.3945/ajcn.114.103655
64 Gonçalves DR , Braga A , Braga J , Marinho A . Recurrent pregnancy loss and vitamin D: A review of the literature. Am J Reprod Immunol. 2018;80(5):e13022. doi:.https://doi.org/10.1111/aji.13022
65 Gernand AD , Klebanoff MA , Simhan HN , Bodnar LM . Maternal vitamin D status, prolonged labor, cesarean delivery and instrumental delivery in an era with a low cesarean rate. J Perinatol. 2015;35(1):23–8. doi:.https://doi.org/10.1038/jp.2014.139
66 Merewood A , Mehta SD , Chen TC , Bauchner H , Holick MF . Association between vitamin D deficiency and primary cesarean section. J Clin Endocrinol Metab. 2009;94(3):940–5. doi:.https://doi.org/10.1210/jc.2008-1217
67 Hossein-nezhad A , Holick MF . Vitamin D for health: a global perspective. Mayo Clin Proc. 2013;88(7):720–55. doi:.https://doi.org/10.1016/j.mayocp.2013.05.011