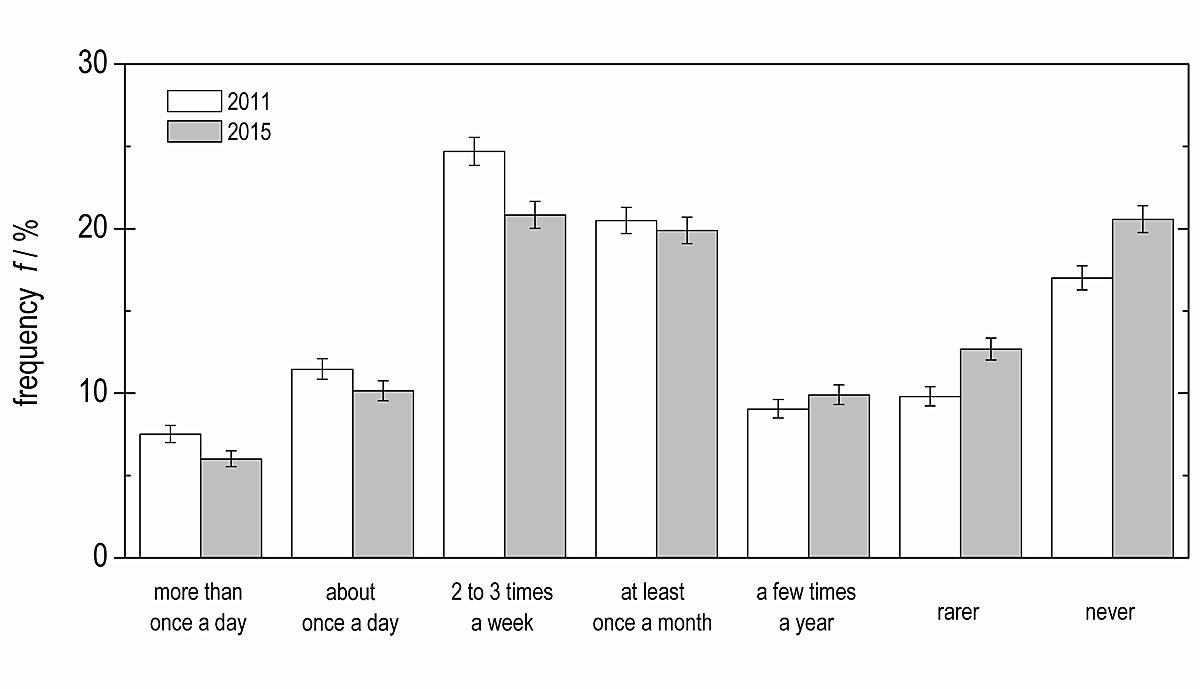
Figure 1 Prevalence of energy drink consumption among young Swiss men in the data sets from 2010/11 (“2011”) and 2014/15 (“2015”) with 95% confidence intervals (bars).
DOI: https://doi.org/10.4414/smw.2020.20243
The health risks of energy drink consumption have been hotly debated over the past decade. Detractors have focused on their high caffeine content and the risks of excessive use [1–3]. In Switzerland, energy drinks typically have a volume of between 0.25 dm3 and 0.36 dm3 and a caffeine concentration of ∼0.32 g dm-3. Studies have found that most healthy adults can consume single caffeine doses of up to 0.2 g or intake caffeine at a rate of up to 0.4 g d-1 without adverse effects [4–7]. For this rate of caffeine intake, other common constituents of energy drinks are not reported to affect their safety at the concentrations usually found in such beverages (4.0 g dm-3 for taurine and 2.4 g dm-3 for D-glucurono-gamma-lactone) [4]. Consuming this much caffeine from energy drinks would require ingesting about 1 dm3 d-1 of energy drinks (approximately four typical energy drinks per day). Drinking more than about four energy drinks per day could result in excessive caffeine consumption, which can cause adverse health effects like caffeine-intoxication, depression, insomnia and headache (for details see [6–10]). More than once a day energy drink use in combination with the consumption of other sources of caffeine risks exceeding the safe caffeine intake rate and poses an important public health challenge. For energy drinks in general, however, questions remain on the acute or long-term effects of excessive and/or chronic consumption [1, 11, 12].
Although data on chronic high energy drink consumption in young adults is scarce, surveys suggest that they comprise a significant subgroup. A population-based survey conducted in 16 countries of the European Union [12] found that 13.3% of young adult energy drink users were “high chronic” consumers (using energy drinks at least 4-5 days per week). A survey-based study from Poland [13] reported that 3.2% of adolescent boys and young adult men consumed energy drinks daily, and that the average caffeine intake rate among daily consumers of energy drinks was more than 0.5 g d-1. The energy drinks supplied more than 0.2 g caffeine, which suggests that those who drank energy drinks more than once a day were at a high risk of consuming excessive amounts of caffeine. A population-based Danish study [14] reported that 0.9% of young adult men consumed more than one energy drink a day and that moderate (weekly) energy drink consumption had a significant positive association with being male, having a low level of education, being employed (vs being a student), being overweight, smoking and consuming alcohol. Other studies have found that energy drink users are more likely to initiate nonmedical use of prescription painkillers [15] and to have used tranquilizers than energy drink non-users [16].
Most energy drink studies have focused on specific and often socially homogenous groups like students [13, 15–19], so we do not yet know the prevalence, sociodemographic distribution, and health behaviour-related factors of chronic heavy consumption of energy drinks in broader populations. We thus set out to analyse the data sets of the “Young Adult Survey Switzerland” (YASS), which began in 2010 and has collected data every four years since then. We (i) quantified the prevalence of chronic heavy energy drink use (consuming energy drinks more than once a day) and (ii) explored associations with sociodemographic and health behaviour-related factors (e.g., use of painkillers and tranquilizers) among young Swiss men.
We analysed data from the 2010/11 (32,424 men) and 2014/15 (28,705 men) cross-sectional “Young Adult Survey Switzerland” (YASS), which is repeated every four years. Throughout, we refer to these datasets as “2011” and “2015”. All data was collected from Swiss men during compulsory recruitment at the six national military recruiting centres in Switzerland, so our sample represented Swiss male citizens between 18 and 21 years old, whether fit or unfit for military service, and whether or not they opted for civilian alternative service. The survey, based only on self-reports, was administered as a paper-and-pencil questionnaire in a classroom.
A supplementary questionnaire on health-relevant behaviours (including a question on energy drink use) and sport [20, 21] was administered to a randomly selected subsample of about one third of the participants. We analysed the data from these participants (10,345 in 2011 and 9761 in 2015). The samples covered the three main language regions in Switzerland (German, French, Italian), urban and rural areas, and all socio-economic strata, so they also included men with no post-mandatory education and men who were unemployed (table 1 below shows the sample characteristics). The survey design and the process of translating the questionnaire into Switzerland’s main languages are published elsewhere [22–24].
The outcome variable was the reported frequency of energy drink consumption over the last year, assessed by the question, “How often have you consumed energy drinks in the last 12 months?” Possible answers were more than once a day/about once a day/2–3 times a week/at least once a month/a few times a year/less often/never. For statistical analysis, we dichotomised energy drink consumption into (I) “more than once a day” or (II) “once a day or less” (see table 1 for categories, frequencies and missing values of variables).
Age was categorised by years old: (I) 18, (II) 19, (III) 20 or (IV) 21. Educational level was based on the International Standard Classification of Education and categorised by the highest level achieved in school [25]: (I) mandatory, (II) vocational or (III) grammar school or higher. Employment status was categorised as (I) employed (including apprentices), (II) student or (III) unemployed. We used criteria defined by the Swiss Federal Office of Public Health to determine migration background [26], and classified migration background as (I) yes or (II) no.
Current smoking status was dichotomised into (I) daily smoking or (II) less than daily smoking or not smoking. Alcohol consumption was calculated from self-reports of average consumption of standard units on weekdays and weekends. The standard units are: 0.3 dm3 for beer; 0.1 dm3 for wine; and 0.02 dm3 for liquor. We defined more than two units per day as the meaningful distinction between (I) low- and (II) high-risk alcohol consumption, based on the low-risk drinking guidelines published by the Swiss Federal Commission for Alcohol Questions [27]. We coded “high-risk drinking” as consuming 15 or more standard units per week, in line with other published international low risk drinking guidelines for men [28]. We assessed use of “tranquilizers or sleeping pills” and “painkillers” on the same scale as energy drink consumption, based on these questions: “How often have you consumed tranquilizers or sleeping pills in the last 12 months?” and, “How often have you consumed the painkillers in the last 12 months?” These questions did not distinguish between prescription and non-prescription drugs and did not ask if they were taken medical purposes. Answers were dichotomised into (I) “once a day or more often” and (II) “less than once a day or never”. We based our categorisation on accumulated evidence of clinically significant adverse effects in chronic use of over-the-counter painkillers [29] and on expert opinion [30] that suggests that only very frequent use of these painkillers (≥15 days per month for >3 months) will induce analgesic-overuse headaches. Sports activity was assessed with the question, “Do you engage in sports” (yes/no) and we divided respondents into two categories: (I) doing sports and (II) not doing sports. Body mass index (BMI) was calculated from self-reported height and weight and grouped into (I) BMI <25 kg/m2 (underweight/normal weight), (II) BMI 25–30 kg/m2 (overweight) and (III) BMI >30 kg/m2 (obese).
We performed multivariable logistic regressions to examine the associations between chronic heavy energy drink consumption (consuming energy drinks more than once a day) and socio-demographic variables (age, educational level, employment status and migrant background) as well as health behaviour-related variables (daily smoking, high-risk alcohol consumption, daily use of tranquilizers/sleeping pills, daily use of painkillers, doing sports and BMI). Because the number of cases was relatively low in some categories, we combined the data sets from 2011 and 2015 to create a larger sample. However, we introduced a binary variable to indicate the wave of data within the model. We also fitted interaction terms to identify which variables varied temporally in their odds ratios (ORs). Because only two variables (daily smoking and high-risk alcohol consumption) had more than 5% missing values (6.03% and 6.67% respectively), we did not expect any bias from using only the valid cases for the analysis. To provide full information, additional regressions were performed for the 2011 and 2015 data sets separately. Chi2 test statistics were calculated for differences in chronic heavy energy drink consumption rates in 2011 and 2015. We considered results significant when p <0.05; Stata 14 software [31] was used for the analyses.
Figure 1 shows the basic distribution of energy drink consumption among Swiss men in 2011 and 2015. The prevalence of the group which forms the focus of this study (“energy drink use more than once a day”) was 7.51% in 2011 and 6.00% in 2015 (chi2 = 17.70, p <0.001). Distributions of “more than once a day energy drink use” according to sociodemographic characteristics and health behaviours are depicted in table 1.
Figure 1 Prevalence of energy drink consumption among young Swiss men in the data sets from 2010/11 (“2011”) and 2014/15 (“2015”) with 95% confidence intervals (bars).
Table 1 Prevalence of more than once a day energy drink consumption in the subgroups defined by the socio-demographic and health behaviour-related variables. The data in the columns “2011” is from the Young Adult Survey Switzerland conducted in 2010/11; “2015” refers to survey years 2014/15. f = frequency per row.
| More than once a day energy drink use | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2011 (n = 10,345) | 2015 (n = 9761) | ||||||||||
| Variable | Yes | No | Total | Yes | No | Total | |||||
| n | f (%) | f (%) | n | n | f (%) | f (%) | n | ||||
| Energy drink use | More than once a day | 746 | 7.51 | 9182 | 92.49 | 9928 | 569 | 6.00 | 8920 | 94.00 | 9489 |
| Missing values | 417 | 272 | |||||||||
| Age (years) | 18 | 170 | 6.52 | 2436 | 93.48 | 2606 | 166 | 5.45 | 2879 | 94.55 | 3045 |
| 19 | 332 | 7.16 | 4308 | 92.84 | 4640 | 262 | 6.04 | 4077 | 93.96 | 4339 | |
| 20 | 183 | 8.85 | 1884 | 91.15 | 2067 | 111 | 6.92 | 1492 | 93.08 | 1603 | |
| 21 | 61 | 9.9 | 554 | 90.1 | 615 | 30 | 6.0 | 472 | 94.0 | 502 | |
| Missing values | 0 | 0 | |||||||||
| Educational level | Mandatory | 132 | 16.9 | 647 | 83.1 | 779 | 101 | 14.7 | 588 | 85.3 | 689 |
| Vocational | 493 | 8.65 | 5205 | 91.35 | 5698 | 354 | 7.06 | 4660 | 92.94 | 5014 | |
| Grammar school or higher | 95 | 2.9 | 3186 | 97.1 | 3281 | 76 | 2.4 | 3132 | 97.6 | 3208 | |
| Missing values | 170 | 578 | |||||||||
| Employment status | Employed | 598 | 8.56 | 6391 | 91.44 | 6989 | 466 | 7.18 | 6028 | 92.82 | 6494 |
| Unemployed | 69 | 11 | 557 | 89 | 626 | 37 | 6.3 | 555 | 93.7 | 592 | |
| Student | 47 | 2.4 | 1900 | 97.6 | 1947 | 40 | 2.0 | 1864 | 98.0 | 1904 | |
| Missing values | 366 | 499 | |||||||||
| Migrant background | Yes | 281 | 9.88 | 2562 | 90.12 | 2843 | 212 | 6.60 | 3000 | 93.40 | 3212 |
| No | 438 | 6.43 | 6377 | 93.57 | 6815 | 347 | 5.66 | 5780 | 94.34 | 6127 | |
| Missing values | 270 | 150 | |||||||||
| Daily smoking | Yes | 464 | 15.7 | 2485 | 84.3 | 2949 | 362 | 14.7 | 2098 | 85.3 | 2460 |
| No | 255 | 3.80 | 6457 | 96.20 | 6712 | 148 | 2.43 | 5935 | 97.57 | 6083 | |
| Missing values | High-risk alcohol consumption | ||||||||||
| Yes | 213 | 11.3 | 1678 | 88.7 | 1891 | 122 | 9.54 | 1157 | 90.46 | 1279 | |
| No | 450 | 5.96 | 7106 | 94.04 | 7556 | 360 | 4.91 | 6972 | 95.09 | 7332 | |
| Missing values | 481 | 878 | |||||||||
| Daily use of tranquilizers/sleeping pills | Yes | 66 | 43 | 87 | 57 | 153 | 60 | 45 | 74 | 55 | 134 |
| No | 673 | 6.92 | 9051 | 93.08 | 9724 | 501 | 5.39 | 8798 | 94.61 | 9299 | |
| Missing values | 51 | 56 | |||||||||
| Daily use of painkillers | Yes | 76 | 46 | 88 | 54 | 164 | 59 | 43 | 79 | 57 | 138 |
| No | 659 | 6.83 | 8988 | 93.17 | 9647 | 492 | 5.33 | 8744 | 94.67 | 9236 | |
| Missing values | 117 | 115 | |||||||||
| Doing sports | Yes | 528 | 6.46 | 7644 | 93.54 | 8172 | 383 | 4.97 | 7330 | 95.03 | 7713 |
| No | 206 | 12.4 | 1458 | 87.6 | 1664 | 177 | 10.3 | 1539 | 89.7 | 1716 | |
| Missing values | 92 | 60 | |||||||||
| Body mass index (BMI)* (kg/m2) | >30 | 50 | 12 | 367 | 88 | 417 | 42 | 11 | 347 | 89 | 389 |
| 25–30 | 124 | 7.57 | 1513 | 92.43 | 1637 | 100 | 6.33 | 1480 | 93.67 | 1580 | |
| <25 | 508 | 6.98 | 6775 | 93.02 | 7283 | 401 | 5.54 | 6835 | 94.46 | 7236 | |
| Missing values | 591 | 284 | |||||||||
* BMI >30: obese; 25–30: overweight; <25: underweight/normal weight
Table 2 presents the results from our multivariate logistic regression analysis, which assessed associations between chronic heavy energy drink use (consuming energy drinks more than once a day) and both sociodemographic and health behaviour-related factors. These data are plotted in figure 2. The influences of the variables were stable between datasets, except for “daily smoking” (interaction term p-value = 0.038) and “migration background” (p = 0.006). The OR of the former variable increased, whereas that of the latter decreased (see table 2 for OR by year).
Table 2 Odds ratios (OR) of the listed variables, estimated with multivariate logistic regression, for more than once a day energy drink consumption in “2011” (survey years 2010/11), “2015” (survey years 2014/15) and for the combination of the two data sets. Numbers in brackets refer to the 95% confidence interval (CI) of the OR. Ref.= Reference category.
| Variable | 2011 and 2015 combined | 2011 | 2015 | ||||
|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | OR (95% CI) | p-value | ||
| Age (years) | 0.825 | 0.802 | 0.945 | ||||
| 21 | 1.00 (0.73–1.37) | 1.07 (0.72–1.58) | 0.90 (0.53–1.53) | ||||
| 20 | 1.03 (0.83–1.26) | 1.10 (0.84–1.44) | 0.94 (0.67–1.32) | ||||
| 19 | 0.94 (0.79–1.13) | 0.97 (0.77–1.24) | 0.92 (0.71–1.21) | ||||
| 18 (Ref.) | |||||||
| Educational level | <0.001 | <0.001 | <0.001 | ||||
| Mandatory | 3.53 (2.62–4.76) | 3.29 (2.26–4.79) | 4.04 (2.46–6.64) | ||||
| Vocational | 1.96 (1.54–2.50) | 1.85 (1.36–2.51) | 2.24 (1.48–3.39) | ||||
| Grammar school or higher (Ref.) | |||||||
| Employment status | 0.012 | 0.012 | 0.243 | ||||
| Employed | 1.55 (1.13–2.12) | 1.84 (1.23–2.76) | 1.17 (0.70–1.95) | ||||
| Unemployed | 1.23 (0.83–1.84) | 1.62 (0.98–2.69) | 0.79 (0.41–1.52) | ||||
| Student (Ref.) | |||||||
| Migrant background | Yes | 1.32 (1.13–1.53) | <0.001 | 1.57 (1.29–1.91) | <0.001 | 1.02 (0.80–1.30) | 0.873 |
| No (Ref.) | |||||||
| Daily smoking | Yes | 4.25 (3.64–4.97) | <0.001 | 3.71 (3.04–4.53) | <0.001 | 5.21 (4.05–6.71) | <0.001 |
| No (Ref.) | |||||||
| High-risk alcohol consumption | Yes | 1.18 (1.00–1.40) | 0.049 | 1.18 (0.96–1.46) | 0.121 | 1.19 (0.91–1.57) | 0.209 |
| No (Ref.) | |||||||
| Daily use of tranquilizers/sleeping pills | Yes | 4.07 (2.66–6.25) | <0.001 | 3.10 (1.71–5.63) | <0.001 | 5.38 (2.89–10.02) | <0.001 |
| No (Ref.) | |||||||
| Daily use of painkillers | Yes | 5.23 (3.51–7.79) | <0.001 | 5.45 (3.24–9.17) | <0.001 | 5.27 (2.81–9.89) | <0.001 |
| No (Ref.) | |||||||
| Doing sports | Yes | 0.73 (0.62–0.86) | <0.001 | 0.76 (0.61–0.95) | 0.016 | 0.68 (0.53–0.87) | 0.002 |
| No (Ref.) | |||||||
| Body mass index (BMI)* (kg/m2) | 0.147 | 0.458 | 0.136 | ||||
| >30 | 1.12 (0.84–1.50) | 0.96 (0.65–1.42) | 1.39 (0.90–2.15) | ||||
| 25–30 | 0.85 (0.70–1.03) | 0.86 (0.67–1.09) | 0.84 (0.61–1.14) | ||||
| <25 (Ref.) | |||||||
| Year | 2015 | 0.80 (0.69–0.93) | 0.003 | ||||
| 2011 (Ref.) | |||||||
* BMI >30: obese; 25–30: overweight; <25: underweight/normal weight
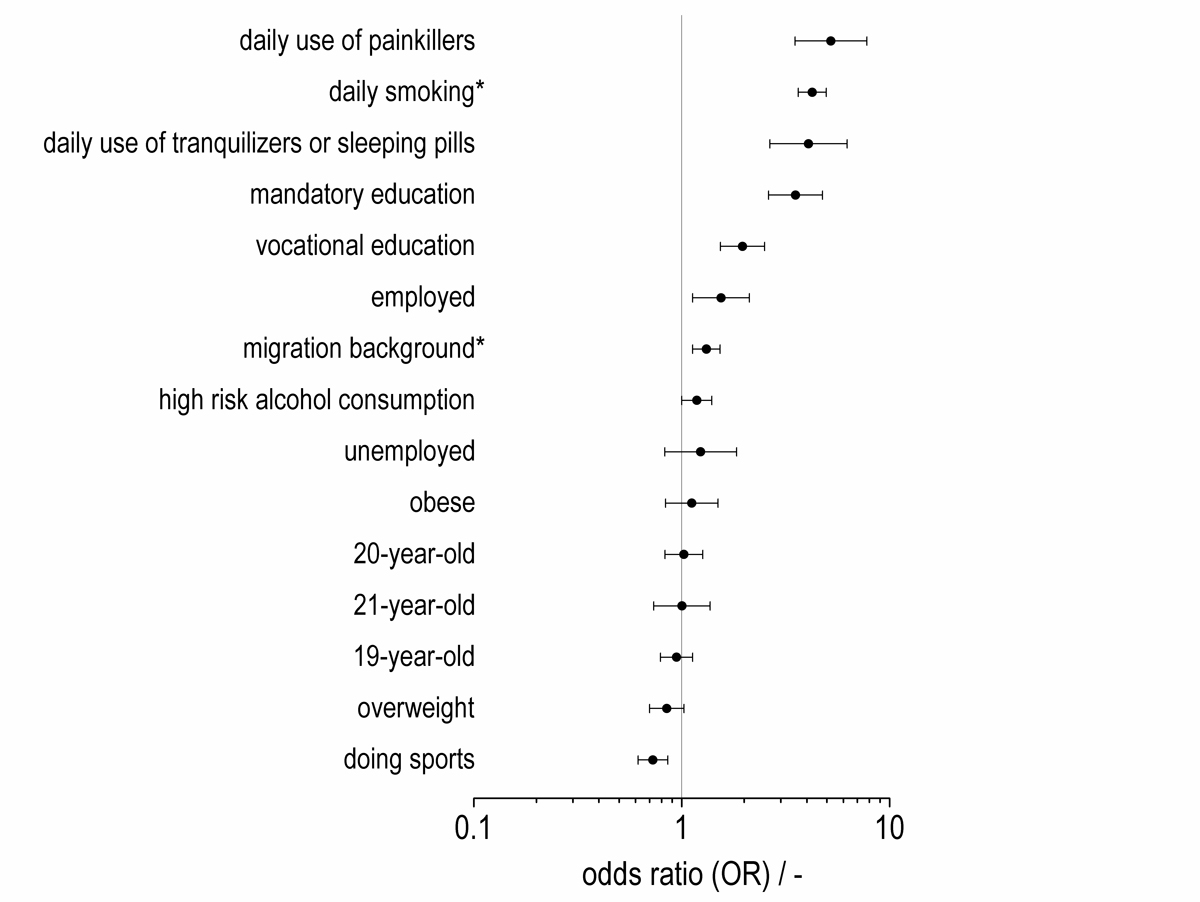
Figure 2 Odds ratios (ORs) and 95% confidence intervals from the multivariate logistic regression performed on the combination of the data sets from 2010/11 and 2014/15 for chronic heavy energy drink consumption (consuming energy drinks more than once a day) from the multivariate logistic regression performed on the combination of the data sets from 2010/11 and 2014/15. An asterisk indicates a statistically significant difference of OR between the two waves. Data from table 2 (“2011 and 2015 combined”).
Every sociodemographic factor except “age” was significantly associated with the use of energy drinks more than once a day. Chronic heavy energy drink consumption showed a consistent gradient pattern for education: men with mandatory or vocational education were more likely to report consuming energy drinks more than once a day than men with higher education. Chronic heavy energy drink consumption was also more common in employed men than in students. Unemployment was not associated with consuming more than one energy drink a day. Respondents with a migrant background were more likely to report chronic heavy energy drink use (vs non-migrant background) in 2011, but not in 2015.
Daily painkiller use, smoking and tranquilizer use were strongly associated with consuming more than one energy drink a day. Less pronounced associations of chronic heavy energy drink use were found for high-risk alcohol consumption; doing sport showed an inverse effect. We did not find that BMI was a relevant factor in chronic heavy energy drink consumption, because neither obesity nor being overweight were associated with multiple daily energy drink use. To qualify the significance of the results, we performed regressions with two alternative categorisations of the outcome variable (more than once a day energy drink use vs. “never consume energy drinks” and “rare to about once a day energy drink consumers”). The largest ORs were found for the same variables as reported above (data not shown). Thus, our results appear to be robust for different categorisations of the dependent variable.
We found strong associations between chronic heavy energy drink consumption (consuming energy drinks more than once a day) and unhealthy substance use in our large and socially diverse sample of young adult men. The rate of chronic heavy energy drinks varied slightly between 2011 and 2015. Based on our data, it is difficult to draw any conclusions about the reason for this variation. Future studies will show if this variation reflects a short-term fluctuation or indicates a long-term trend.
Our study revealed high rates of multiple daily energy drink consumption among men in Switzerland: 7.51% in 2011 (eight times higher than in a 2010 survey of 16–24 year-old men in Denmark [14]) and 6.00% (six times higher than in the survey) in 2015. Although this difference might be attributable in part to different age groups and study designs, this is unlikely to explain away the large difference in consumption rate. Our finding supports existing evidence of wide variation in heavy energy drink use across countries: an earlier study found that the prevalence of “high chronic” energy drink consumption (using energy drinks 4–5 days per week or more) among adult energy drink consumers varied between 5% in Italy and Hungary to 21% in the UK [12].
Associations between multiple daily energy drink use and sociodemographic and health behaviour-related factors were mostly stable over time. Among the strongest and most intriguing positive associations with chronic heavy energy drink use was “heavy use of painkillers and tranquilizers or sleeping pills”, which warrants attention because of the risk of pharmacokinetic interactions between over-the-counter or prescription drugs and dietary caffeine [8, 32, 33], and because painkiller use is increasingly prevalent (15.1% in 2017) among young adult men in Switzerland [34]. Unfortunately, the datasets could not tell us why young men consumed energy drinks, or whether the painkillers and tranquilizers they took were prescribed. Since long-term excessive caffeine consumption is linked to headaches [9], chronic heavy energy drink use might cause headaches, increasing the likelihood that young men will take painkillers. This could explain the high proportion of heavy analgesic users among the chronic heavy energy drink consumers. Consuming energy drinks more than once a day was also associated with daily smoking and high-risk alcohol consumption, in line with previous findings that have linked smoking, alcohol consumption, and energy drink use [14, 17, 18, 35–39]. Heavier cigarette consumption increases coffee intake [40], and may also increase consumption of caffeinated beverages like energy drinks, encouraging daily smokers to consume energy drinks in excess.
The associations between chronic heavy use of energy drinks and the other unhealthy behaviours substantiated in this study suggest that high use may be part of a social pattern in health lifestyles [41, 42], since health lifestyles “comprise patterns of health-related behaviour, values, and attitudes adapted by groups of individuals in response to their social, cultural and economic environment” [41]. Single health behaviours tend to cluster but are also influenced by social characteristics like status and class, so it makes sense that chronic heavy energy drink use was strongly associated both with other health-relevant behaviours and also with social determinants like education. Other researchers have identified negative relationships between unhealthy behaviours and educational resources in young adult Swiss men [22, 43–45]. Our results complement European data which indicated that education was one of the strongest socio-demographic predictors of energy drink use [14]. If we had not analysed energy drink use in a socially diverse sample, we might have missed the social gradient in chronic heavy energy drink consumption. We found that consuming energy drinks excessively and chronically was linked to employment status and migration background. Employed respondents were more likely than students to consume energy drinks more than once a day. Both occupational conditions and migration background may indicate health contexts which shape the healthiness of the participants’ lifestyles. Chronic heavy consumption of energy drinks may be a facet of the health lifestyles of young men – valuable information for those who want to design prevention measures.
Our study has some limitations. First, all of our variables were based on self-reports, which have been shown to be susceptible to social desirability biases. Thus, underreporting may have occurred in some of the health behaviour-related variables, such as smoking or alcohol use. Second, local administrative records do not include the number of men the army recruitment centres processed each day, so we cannot know the exact response rate, but field staff reported that recruits rarely refused to fill in the questionnaire. A study that used a very similar sampling procedure in two of those recruitment centres reported their response rate as 95% [43]. Third, the sampling procedure in the recruitment centres excluded women and non-citizens, so our results cannot be generalised beyond Swiss men aged 18-21. Future studies should examine patterns of chronic heavy energy drink consumption in large and socially diverse samples of girls and women. Fourth, the measure of energy drink use was based on a single question about the frequency of energy drink consumption, but did not assess the amount consumed. To determine the exact proportion of people exceeding the safe caffeine intake rate, and thus at risk of adverse health effects caused by chronic heavy energy drink use, we would need to collect new data on consumption levels, and we suggest future researchers do so. Fifth, there was no definition of energy drinks in the questionnaire, so some men may have included sports drinks (e.g., high mineral drinks) in their tally, which would have resulted in an overestimation of consumption.
Our nation-wide survey on energy drink use among young Swiss men revealed remarkably high rates of chronic heavy energy drink consumption: 7.51% in 2011 and 6.00% in 2015. The study identified a strong link between chronic heavy energy drink consumption and unhealthy behaviours, especially substance use (heavy use of painkillers, tranquilizers and daily smoking). The chances a young Swiss man would be a chronic heavy energy drink consumer were roughly four to five times higher if he also used painkillers or tranquilizers daily. The co-occurrence of chronic heavy energy drink consumption and unhealthy behaviours and their association with social characteristics suggest lifestyle plays a central role in the emergence and distribution of energy drink consumption. If multiple daily energy drink consumption is an expression of a general pattern of unhealthy behaviour, then measures that address associated lifestyles may help prevent substance use in chronic heavy energy drink consumers.
We thank Dr Kali Tal for her editorial suggestions.
The authors received no external funding for this project and have no conflicts of interest to declare.
1German Federal Institute for Risk Assessment. Kinder und Jugendliche: Übermässiger Konsum von Energy Drinks erhöht Gesundheitsrisiko für Herz und Kreislauf. Stellungnahme Nr. 018/2019 des BfR vom 27. Mai 2019. 2019 [cited 2019 July 2019]. Available from https://www.bfr.bund.de/cm/343/kinder-und-jugendliche-uebermaessige-konsum-von-energy-drinks-erhoeht-gesundheitsrisiko-fuer-herz-und-kreislauf.pdf.
2 Breda JJ , Whiting SH , Encarnação R , Norberg S , Jones R , Reinap M , et al. Energy drink consumption in europe: a review of the risks, adverse health effects, and policy options to respond. Front Public Health. 2014;2:134. doi:.https://doi.org/10.3389/fpubh.2014.00134
3 Wassef B , Kohansieh M , Makaryus AN . Effects of energy drinks on the cardiovascular system. World J Cardiol. 2017;9(11):796–806. doi:.https://doi.org/10.4330/wjc.v9.i11.796
4 EFSA Panel on Dietetic Products. Nutrition and Allergies. Scientific Opinion on the safety of caffeine. EFSA J. 2015;13(5):4102.
5 Higdon JV , Frei B . Coffee and health: a review of recent human research. Crit Rev Food Sci Nutr. 2006;46(2):101–23. doi:.https://doi.org/10.1080/10408390500400009
6 Wikoff D , Welsh BT , Henderson R , Brorby GP , Britt J , Myers E , et al. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem Toxicol. 2017;109(Pt 1):585–648. doi:.https://doi.org/10.1016/j.fct.2017.04.002
7 Nawrot P , Jordan S , Eastwood J , Rotstein J , Hugenholtz A , Feeley M . Effects of caffeine on human health. Food Addit Contam. 2003;20(1):1–30. doi:.https://doi.org/10.1080/0265203021000007840
8 Temple JL , Bernard C , Lipshultz SE , Czachor JD , Westphal JA , Mestre MA . The Safety of Ingested Caffeine: A Comprehensive Review. Front Psychiatry. 2017;8:80. doi:.https://doi.org/10.3389/fpsyt.2017.00080
9 Espinosa Jovel CA , Sobrino Mejía FE . Cafeína y cefalea: consideraciones especiales [Caffeine and headache: specific remarks]. Neurologia. 2017;32(6):394–8. doi:.https://doi.org/10.1016/j.nrl.2014.12.016
10Flanagan RJ, Braithwaite RA, Brown SS, Widdop B, de Wolff FA. Basic analytical toxicology. Geneva: World Health Organization;1995.
11 Seifert SM , Schaechter JL , Hershorin ER , Lipshultz SE . Health effects of energy drinks on children, adolescents, and young adults. Pediatrics. 2011;127(3):511–28. doi:.https://doi.org/10.1542/peds.2009-3592
12 Zucconi S , Volpato C , Adinolfi F , Gandini E , Gentile E , Loi A , et al. Gathering consumption data on specific consumer groups of energy drinks. External Scientific Report for European Safety Authority. 2013;10(3):1–190. doi:.https://doi.org/10.2903/sp.efsa.2013.EN-394
13 Nowak D , Jasionowski A . Analysis of the Consumption of Caffeinated Energy Drinks among Polish Adolescents. Int J Environ Res Public Health. 2015;12(7):7910–21. doi:.https://doi.org/10.3390/ijerph120707910
14 Friis K , Lyng JI , Lasgaard M , Larsen FB . Energy drink consumption and the relation to socio-demographic factors and health behaviour among young adults in Denmark. A population-based study. Eur J Public Health. 2014;24(5):840–4. doi:.https://doi.org/10.1093/eurpub/cku003
15 Arria AM , Caldeira KM , Kasperski SJ , O’Grady KE , Vincent KB , Griffiths RR , et al. Increased alcohol consumption, nonmedical prescription drug use, and illicit drug use are associated with energy drink consumption among college students. J Addict Med. 2010;4(2):74–80. doi:.https://doi.org/10.1097/ADM.0b013e3181aa8dd4
16 Polak K , Dillon P , Koch JR , Miller WG, Jr , Thacker L , Svikis D . Energy drink use is associated with alcohol and substance use in eighth, tenth, and twelfth graders. Prev Med Rep. 2016;4:381–4. doi:.https://doi.org/10.1016/j.pmedr.2016.06.019
17 Attila S , Çakir B . Energy-drink consumption in college students and associated factors. Nutrition. 2011;27(3):316–22. doi:.https://doi.org/10.1016/j.nut.2010.02.008
18 Miller KE . Energy drinks, race, and problem behaviors among college students. J Adolesc Health. 2008;43(5):490–7. doi:.https://doi.org/10.1016/j.jadohealth.2008.03.003
19 Marczinski CA . Alcohol mixed with energy drinks: consumption patterns and motivations for use in U.S. college students. Int J Environ Res Public Health. 2011;8(8):3232–45. doi:.https://doi.org/10.3390/ijerph8083232
20Young Adult Survey Switzerland. Main and supplementary questionnaire 2010/11. 2010 [cited 2019 Feb 20]. Available from https://chx.mazzehosting.ch/sites/default/files/downloads/chx_yass-fb2010-2011_b_gesundheit-und-sport_d.pdf
21Young Adult Survey Switzerland. Main and supplementary questionnaire 2014/15. 2014 [cited 2019 Feb 20] Available from: https://chx.mazzehosting.ch/sites/default/files/downloads/02_chx_2014-15_b_gesundheit_deutsch.pdf
22 Abel T , Hofmann K , Schori D . Social and regional variations in health status and health behaviours among Swiss young adults. Swiss Med Wkly. 2013;143:w13901. doi:.https://doi.org/10.4414/smw.2013.13901
23 Hofmann K , Schori D , Abel T . Self-reported capabilities among young male adults in Switzerland: Translation and psychometric evaluation of a German, French and Italian version of a closed survey instrument. Soc Indic Res. 2013;114(2):723–38. doi:.https://doi.org/10.1007/s11205-012-0170-1
24Huber SG, ed. Young Adult Survey Switzerland. Bern: BBL/OFCL/UFCL;2016.
25UNESCO. International Standard Classfication of Education. ISCED 2011. Montreal, Quebec: UNESCO Institute for Statistics;2012.
26Swiss Federal Office of Public Health. [Key features to measure migration background in Swiss health surveys] Schlüsselmerkmale zur Erfassung des Migrationshintergrundes in schweizerischen Gesundheitsdatenerhebungen. 2016 [cited 2018 Nov 12]. Available from https://www.bag.admin.ch/dam/bag/de/dokumente/nat-gesundheitsstrategien/nat-programm-migration-und-gesundheit/forschung-migration-und-gesundheit/schluesselmerkmale-zur-erfassung-des-migrationshintergrunds/schluesselmerkmale-migrationshintergrund.pdf.download.pdf/schluesselmerkmale-migrationshintergrund.pdf.
27Swiss Federal Commission for Alcohol Questions. [Guidelines for alcohol consumption – 2018] Orientierungshilfe zum Alkoholkonsum - 2018. 2018 [cited 2019 Feb 14]. Available from https://www.newsd.admin.ch/newsd/message/attachments/53054.pdf
28 Bondy SJ , Rehm J , Ashley MJ , Walsh G , Single E , Room R . Low-risk drinking guidelines: the scientific evidence. Can J Public Health. 1999;90(4):264–70. doi:.https://doi.org/10.1007/BF03404129
29 McCrae JC , Morrison EE , MacIntyre IM , Dear JW , Webb DJ . Long-term adverse effects of paracetamol - a review. Br J Clin Pharmacol. 2018;84(10):2218–30. doi:.https://doi.org/10.1111/bcp.13656
30 Headache Classification Committee of International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. 2013;33(9):629–808. doi:.https://doi.org/10.1177/0333102413485658
31Stata Corp. Stata Statistical Software: Release 14. StataCorp LP, College Station, TX;2015.
32 Carrillo JA , Benitez J . Clinically significant pharmacokinetic interactions between dietary caffeine and medications. Clin Pharmacokinet. 2000;39(2):127–53. doi:.https://doi.org/10.2165/00003088-200039020-00004
33 Cameron MD , Wen B , Roberts AG , Atkins WM , Campbell AP , Nelson SD . Cooperative binding of acetaminophen and caffeine within the P450 3A4 active site. Chem Res Toxicol. 2007;20(10):1434–41. doi:.https://doi.org/10.1021/tx7000702
34Swiss Federal Statistical Office. [Consumption of single drugs] Konsum einzelner Medikamente, excel file. 2019 [cited 2019 Mar 4]. Available from https://www.bfs.admin.ch/bfs/de/home/aktuell/neue-veroeffentlichungen.assetdetail.7567000.html
35 Mann MJ , Smith ML , Kristjansson AL . Energy drink consumption and substance use risk in middle school students. Prev Med Rep. 2016;3:279–82. doi:.https://doi.org/10.1016/j.pmedr.2016.03.014
36 Terry-McElrath YM , OʼMalley PM , Johnston LD . Energy drinks, soft drinks, and substance use among United States secondary school students. J Addict Med. 2014;8(1):6–13. doi:.https://doi.org/10.1097/01.ADM.0000435322.07020.53
37 Arria AM , Caldeira KM , Kasperski SJ , Vincent KB , Griffiths RR , O’Grady KE . Energy drink consumption and increased risk for alcohol dependence. Alcohol Clin Exp Res. 2011;35(2):365–75. doi:.https://doi.org/10.1111/j.1530-0277.2010.01352.x
38 Larson N , Laska MN , Story M , Neumark-Sztainer D . Sports and energy drink consumption are linked to health-risk behaviours among young adults. Public Health Nutr. 2015;18(15):2794–803. doi:.https://doi.org/10.1017/S1368980015000191
39 O’Brien MC , McCoy TP , Rhodes SD , Wagoner A , Wolfson M . Caffeinated cocktails: energy drink consumption, high-risk drinking, and alcohol-related consequences among college students. Acad Emerg Med. 2008;15(5):453–60. doi:.https://doi.org/10.1111/j.1553-2712.2008.00085.x
40 Bjørngaard JH , Nordestgaard AT , Taylor AE , Treur JL , Gabrielsen ME , Munafò MR , et al. Heavier smoking increases coffee consumption: findings from a Mendelian randomization analysis. Int J Epidemiol. 2017;46(6):1958–67. doi:.https://doi.org/10.1093/ije/dyx147
41 Abel T . Measuring health lifestyles in a comparative analysis: theoretical issues and empirical findings. Soc Sci Med. 1991;32(8):899–908. doi:.https://doi.org/10.1016/0277-9536(91)90245-8
42 Cockerham WC . Health lifestyle theory and the convergence of agency and structure. J Health Soc Behav. 2005;46(1):51–67. doi:.https://doi.org/10.1177/002214650504600105
43 Dermota P , Wang J , Dey M , Gmel G , Studer J , Mohler-Kuo M . Health literacy and substance use in young Swiss men. Int J Public Health. 2013;58(6):939–48. doi:.https://doi.org/10.1007/s00038-013-0487-9
44 Schori D , Hofmann K , Abel T . Social inequality and smoking in young Swiss men: intergenerational transmission of cultural capital and health orientation. Int J Public Health. 2014;59(2):261–70. doi:.https://doi.org/10.1007/s00038-013-0537-3
45 Charitonidi E , Studer J , Gaume J , Gmel G , Daeppen JB , Bertholet N . Socio-economic status and substance use among young Swiss men. BMC Public Health. 2016;16:333. doi:.https://doi.org/10.1186/s12889-016-2949-5
The authors received no external funding for this project and have no conflicts of interest to declare.