
Figure 1 A refugee family currently living in Moria camp in front of their shelter. Photographer: Tricia Vannatter, health promoter; the photograph is published with the consent of the persons depicted.
DOI: https://doi.org/10.4414/smw.2020.20263
The national and international response to the corona virus disease 2019 (COVID-19) has reached an unprecedented level. It has become evident that the pandemic will have a long-lasting and substantial influence on our society, globally and locally, far beyond health. This outbreak of the new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) will also shed light on pre-existing challenges, such as the refugee crisis, which are converging with the pandemic [1]. It is now crucial that the unique needs of the refugee and migrant population are included in the global response to COVID-19 [2].
In 2019, approximately 123,700 refugees and migrants arrived via the three Mediterranean routes to Greece, Italy and Spain from North Africa and Turkey [3]. Whilst we read the staggering number of daily cases and deaths in Italy and Spain from COVID-19 [4], arrivals of refugees and migrants to the Mediterranean countries have continued, reaching over 15,000 in the first two months of 2020 [3]. In addition, the United Nations High Commissioner for Refugees (UNHCR) reports considerably higher number of migrant entries to the Western Balkan countries in recent months in contrast to decreasing numbers since 2015 [5].
COVID-19 – as a novel communicable disease – crosses all borders and spreads fast. However, in migrant and asylum shelters the proposed measures to flatten the curve of transmission by physical distancing and improving hand hygiene are not feasible (fig. 1 and 2 ).
Figure 1 A refugee family currently living in Moria camp in front of their shelter. Photographer: Tricia Vannatter, health promoter; the photograph is published with the consent of the persons depicted.

Figure 2 One of the streets in Moria camp. Photographer: Tricia Vannatter, health promoter.
Self-isolation in refugee camps is impossible: you cannot stay at home if you have no home (fig. 3).

Figure 3 Swiss activist raising awareness on the difficulties to implement COVID-19 prevention measures in refugee camps (pictures provided by Céline de Richoufftz, reproduced with permission).
As of April 5 2020, the first two refugee camps on mainland Greece have reported COVID-19 cases and started quarantine for 2 weeks [6]. So far no cases have been confirmed in the highly overcrowded refugee camps on the Greek islands, but according to the Greek migration minister Notis Mitarachi, any emergency response to a COVID-19 outbreak in this setting will be even more difficult.
The only way to efficiently tackle and prevent the spread of SARS-CoV-2 in refugees in European countries is therefore spacing out individuals. Experts in the field of humanitarian work call for “a sans frontiers solidarity” [7]. Such an approach may seem counter-intuitive, particularly as the first action of UNHCR and the International Organization for Migration (IOM) on 17 March 2020, was the suspension of the resettlement programme for refugees [8].
Citizens of many European countries have signed open letters to the European Parliament and national governments to start the evacuation of refugees [9, 10, 11]. The first unaccompanied minor refugees have been accepted in Germany and Luxemburg. However, to accommodate an estimated 42,000 refugees in the Mediterranean region requiring relocation, a pan-European coordination of prevention is needed [1, 9] (fig. 4).
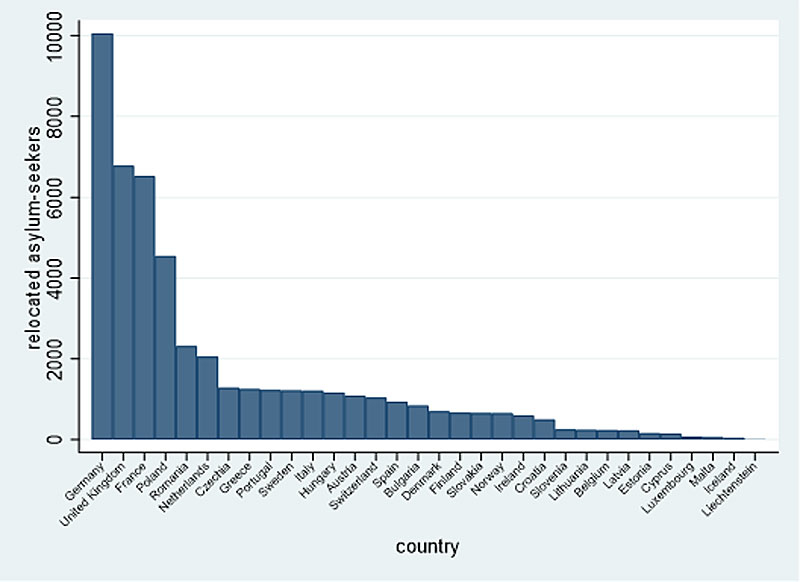
Figure 4 Number of asylum seekers the 32 European and associated countries are required to accommodate. Distribution was calculated based on population size and current death rates due to COVID-19. Countries with death rates below 20 per 100,000 receive 12 asylum-seekers per 100,000 inhabitants; those with death rates between 20 and 35 per 100,000 receive 10 asylum-seekers per 100,000 inhabitants and countries with death rates above 35 per 100 000 receive 2 asylum-seekers per 100,000 inhabitants. Graph adapted from the open letter to the European Parliament ([9], https://www.evacuate-moria.com/) with permission from Prof. Bozorgmehr. Mortality rates and population sizes were extracted from Eurostat on 16 April 2020.
Many of the non-Mediterranean European countries, including Switzerland, currently have underused asylum centres to allow physical distancing and hygiene.
Access to health information, diagnostic testing and medical care is excellent in our setting and will be vital to reduce the impact of this pandemic [12]. We also need to ensure that, when seeking health care or being included in contact tracing for COVID-19, refugees and migrants will not face any sanctions when engaging with state authorities.
Urgent measures are required to ensure that these refugees and migrants – not only residents, tourists and international travellers – are included in our response to COVID-19. We are obliged to protect their health and human rights, particularly in these extraordinary times.
No financial support and no other potential conflict of interest relevant to this article was reported.
1 Bozorgmehr K , Saint V , Kaasch A , Stuckler D , Kentikelenis A . COVID and the convergence of three crises in Europe. Lancet Public Health. 2020;S2468-2667(20)30078-5. doi:.https://doi.org/10.1016/S2468-2667(20)30078-5
2 Brandenberger J , Tylleskär T , Sontag K , Peterhans B , Ritz N . A systematic literature review of reported challenges in health care delivery to migrants and refugees in high-income countries - the 3C model. BMC Public Health. 2019;19(1):755. doi:.https://doi.org/10.1186/s12889-019-7049-x
3The UN Refugee Agency. Operational portal refugee situations - Mediterranean route. 2020. Available at: https://data2.unhcr.org/en/situations/mediterranean
4Tableau Publique. COVID19 Trend Tracker. 2020. https://public.tableau.com/profile/stevie.soler#!/vizhome/TrendTracker-COVID19/TrendTracker-COVID19
5The UN Refugee Agency. Operational portal on refugee situations - western Balkans. 2020. Available at: https://data2.unhcr.org/en/situations/westbalkans.
6Renee M. Greece quarantines second migrant camp after COVID-19 case confirmed. In: Reuters, editor. Athens: Reuters; 2020.
7Lugli M. To truly beat COVID-19, we need "sans frontières" solidarity. The New Hunanitarian. 13 April 2020. Available at: http://www.thenewhumanitarian.org/opinion/2020/04/13/global-coronavirus-public-health-solidarity.
8The UN Refugee Agency. IOM, UNHCR announce temporary suspension of resettlement travel for refugees. 17 March 2020. https://www.unhcr.org/news/press/2020/3/5e7103034/iom-unhcr-announce-temporary-suspension-resettlement-travel-refugees.html (accessed 2020 March 31)
9Bozorgmehr K, Biddle L, Jahn R, Wahedi K, McKee M. Evacuate.Moria.Now. Open letter to the European Commission and the European Emergency Response Coordinator. 27 March 2020. Available at: https://www.evacuate-moria.com/.
10evakuierenJETZT. Wir fordern den Bundesrat und das Parlament auf: Handelt jetzt! 2020. https://evakuieren-jetzt.ch/ (accessed 2020 April 17)
11Amnesty International Switzerland. Die Schweiz muss dringend Flüchtlinge aufnehmen. https://www.amnesty.ch/de/laender/europa-zentralasien/griechenland/dok/2020/fluechtlinge-griechenland/online (accessed 2020 April 27)
12 Brandenberger J , Gmünder M , Pohl C , Buser S , Ritz N . Reasons for admission in asylum-seeking and non-asylum-seeking patients in a pediatric tertiary care centre. Swiss Med Wkly. 2020;150:w20252 [in print]
No financial support and no other potential conflict of interest relevant to this article was reported.