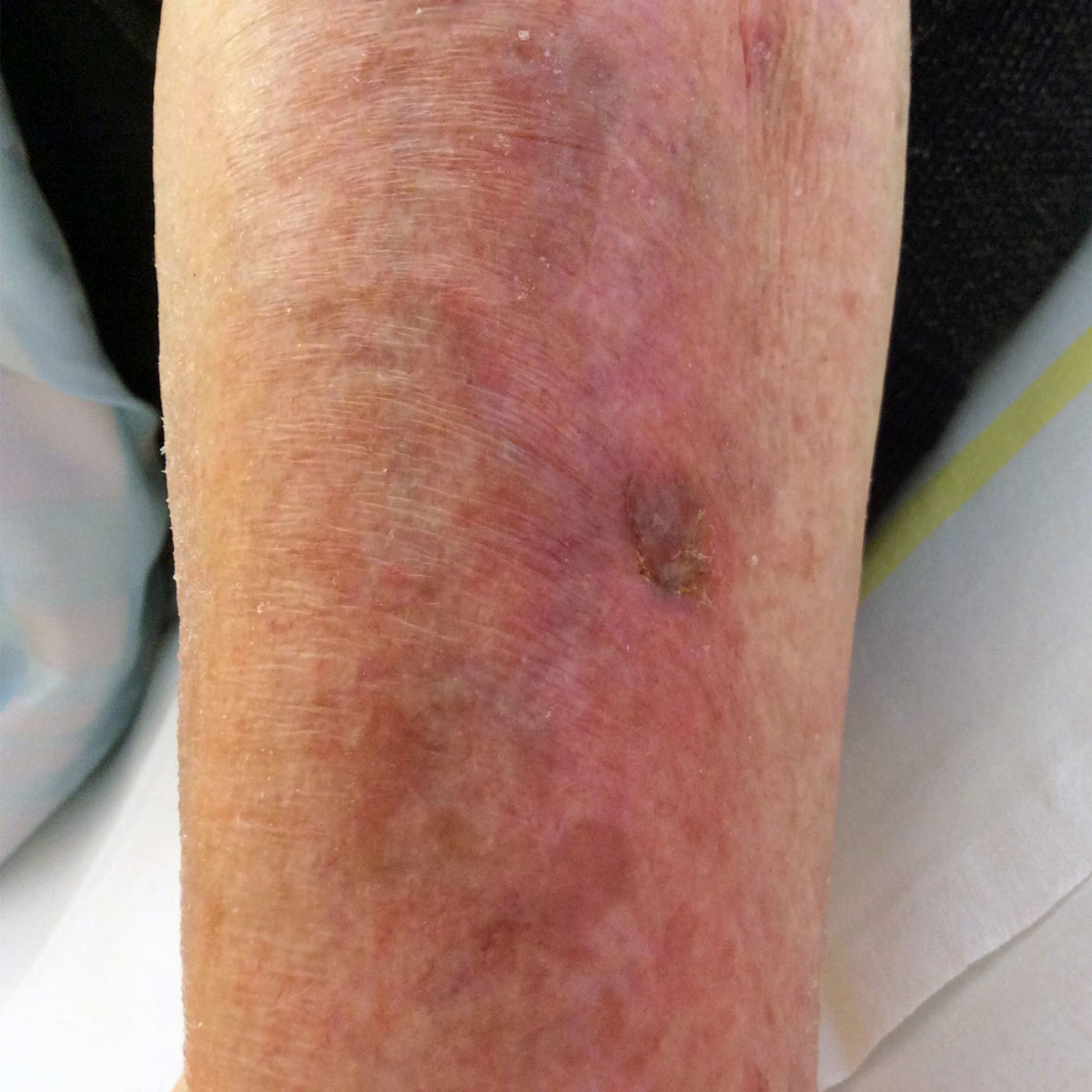
Figure 1 Initial aspect of the pretibial wound.
DOI: https://doi.org/10.4414/smw.2020.20220
An 83-year-old immunocompetent woman with Alzheimer disease presented to our emergency department in July 2018 with a 2-day history of fever without other complaints. Nine days before she reported a small wound on the right pretibial region that occurred during gardening. In the days immediately following the minor injury, the patient visited her neighbour and bathed in their open-air swimming pool. She did not take any specific pharmacological treatment, and denied regular contacts with animals and trips outside of Switzerland in the last year. Physical examination revealed a body temperature of 39.2°C, blood pressure of 153/67 mm Hg, heart rate of 87 bpm and poor general clinical condition. On the right pretibial region she had a wound of about 1 centimetre in diameter with a localised warm surrounding non-necrotic erythematous reaction without a defined margin (fig. 1). Blood tests revealed an increase in C-reactive protein (155 mg/l, reference <5 mg/l) and leucocytosis (10.4 × 109/l). No masses or infiltrations of the lung were described on the chest X-rays. Right leg radiography did not show any fracture or sign of periosteal reaction. After the blood draw for blood cultures, the patient started empirical therapy with amoxicillin/clavulanic acid 1.2 g three times a day intravenously. In the first 48 hours we noted persistent fever and further increase of the inflammatory markers (C-reactive protein up to 159 mg/l). Renal function, creatine phosphokinase and transaminases were normal. The treatment was modified to piperacillin/tazobactam 4.5 g every 8 hours intravenously. Blood cultures were positive (four of four bottles) for Chromobacterium violaceum susceptible to piperacillin/tazobactam, ciprofloxacin and trimethoprim/sulfamethoxazole. After 8 days of the initial antibiotic therapy, the clinical course was favourable with defervescence, healing of the skin lesion and normalisation of inflammation parameters. We changed the antibiotic therapy to ciprofloxacin 500 mg every 12 hours orally to be continued for 3 weeks, and the patient was discharged from our clinic.
Figure 1 Initial aspect of the pretibial wound.
C. violaceum is a rare gram-negative facultative anaerobe bacillus associated with serious waterborne infections of non-intact skin in tropical and subtropical regions, mostly in Southeast Asia. The clinical presentation usually starts with a localised cutaneous lesion and lymphadenitis after contact with stagnant water. C. violaceum is considered an emerging pathogen and it can generally be isolated from water and soil of tropical and subtropical regions [1, 2]. Its pathogenicity was described for the first time at the start of the twentieth century from an infection in a bull, which led to the death of the animal. The first human clinical case was described in Malaysia in 1927 [3]. Since then, various clinical cases have been described in Asia, Africa, South America, North America and, recently, in Europe [4–7]. C. violaceum can cause opportunistic infections in humans and in some animals, occurring at first as a cutaneous lesion and later as a septic dissemination with multiple abscesses in organs such brain, liver, spleen and lung, potentially causing a fatal septicaemia with a case-fatality rate of up to 60% [2, 6, 8]. In the literature, urinary infections, ocular infections, cellulitis and also a case of a patient affected by chronic granulomatosis are reported [9, 10]. The number of case reports of C. violaceum is fewer than 200 worldwide, described in Vietnam, Taiwan, India, Nepal, Singapore, Sri Lanka, Japan, Australia, Cuba, Argentina, Brazil, United States, Nigeria, Senegal and Congo [4–6].
After the isolation of C. violaceum from the blood culture of our patient in the microbiology laboratory, we asked the laboratory managers of the principal hospitals over the whole Switzerland, searched similar published case reports and searched in Swiss clinical databases, such anresis.ch [11], without founding any record of previous similar episodes. To our knowledge, this is the first case of C. violaceum infection in Switzerland. Furthermore, there are only three previous clinical cases of such infection in Europe. The first case report was in 2011, when a 14-year-old patient, who was born in Guinea and who had lived in Italy for 7 years, presented lymphadenopathies with increased inflammatory markers in the blood [7]. Then, a case report in 2019 from the Czech Republic described a 54-year-old man who died of septic shock with ischaemic necrosis of all extremities and multiple organ failure after contracting C. violaceum during a holiday in Thailand [12]. Unlike the first two cases, which could have been imported infections, a third article in 2019 from Poland described an autochthonous case of C. violaceum sepsis in a 55-year-old patient, who recovered from the infection but was referred to the haemodialysis programme because of kidney insufficiency [13]. Our patient had not recently travelled out of Switzerland and had no contact with anyone who had been in endemic regions. She was probably infected during the summer of 2018 in a local private swimming pool in a village of the Lepontine Alps. Therefore, to our knowledge, this is the second autochthonous infection by C. violaceum in Europe.
Potential effects of the global climate change include new geographical distributions of infectious diseases. Clinicians must be aware and promptly recognise these entities because a delay in adequate treatment is associated with high fatality rates.
No financial support and no other potential conflict of interest relevant to this article was reported.
1 Okada M , Inokuchi R , Shinohara K , Matsumoto A , Ono Y , Narita M , et al. Chromobacterium haemolyticum-induced bacteremia in a healthy young man. BMC Infect Dis. 2013;13(1):406. doi:.https://doi.org/10.1186/1471-2334-13-406
2 Bottieau E , Mukendi D , Kalo JR , Mpanya A , Lutumba P , Barbé B , et al. Fatal Chromobacterium violaceum bacteraemia in rural Bandundu, Democratic Republic of the Congo. New Microbes New Infect. 2015;3:21–3. doi:.https://doi.org/10.1016/j.nmni.2014.10.007
3 Sneath PHA , Singh RB , Whelan JPF , Edwards D . Fatal infection by Chromobacterium violaceum. Lancet. 1953;262(6780):276–7. doi:.https://doi.org/10.1016/S0140-6736(53)91132-5
4 Parajuli NP , Bhetwal A , Ghimire S , Maharjan A , Shakya S , Satyal D , et al. Bacteremia caused by a rare pathogen - Chromobacterium violaceum: a case report from Nepal. Int J Gen Med. 2016;9:441–6. doi:.https://doi.org/10.2147/IJGM.S125183
5 Kaniyarakkal V , Orvankundil S , Lalitha SK , Thazhethekandi R , Thottathil J . Chromobacterium violaceum Septicaemia and Urinary Tract Infection: Case Reports from a Tertiary Care Hospital in South India. Case Rep Infect Dis. 2016;2016:6795743. doi:.https://doi.org/10.1155/2016/6795743
6 de Siqueira IC , Dias J , Ruf H , Ramos EA , Maciel EA , Rolim A , et al. Chromobacterium violaceum in siblings, Brazil. Emerg Infect Dis. 2005;11(9):1443–5. doi:.https://doi.org/10.3201/eid1109.050278
7 Arosio M , Raglio A , Ruggeri M , Serna Ortega P , Morali L , De Angelis C , et al. Chromobacterium violaceum lymphadenitis successfully treated in a Northern Italian hospital. New Microbiol. 2011;34(4):429–32.
8 Ansari S , Paudel P , Gautam K , Shrestha S , Thapa S , Gautam R . Chromobacterium violaceum Isolated from a Wound Sepsis: A Case Study from Nepal. Case Rep Infect Dis. 2015;2015:181946. doi:.https://doi.org/10.1155/2015/181946
9 Meher-Homji Z , Mangalore RP , D R Johnson P , Y L Chua K . Chromobacterium violaceum infection in chronic granulomatous disease: a case report and review of the literature. JMM Case Rep. 2017;4(1):e005084. doi:.https://doi.org/10.1099/jmmcr.0.005084
10 Ray P , Sharma J , Marak RS , Singhi S , Taneja N , Garg RK , et al. Chromobacterium violaceum septicaemia from north India. Indian J Med Res. 2004;120(6):523–6.
11Anresis.ch. [Internet]. Bern: Swiss Centre for Antibiotic resistance; c2020 [cited 2020 Jan 27]. Available from: https:// www.anresis.ch/.
12 Dzupova O , Benes J . Serious imported infections: A focus on Chromobacterium violaceum. Bratisl Lek Listy. 2019;120(10):730–3. doi:.https://doi.org/10.4149/BLL_2019_121
13 Jędruszczak A , Węgrzyn-Bąk M , Budzyńska-Nosal R , Maciejewski M , Marczewski K . Sepsis caused by Chromobacterium violaceum - probably the first case in Europe, or <i>Macbeth</i> read anew. Ann Agric Environ Med. 2019;26(3):508–10. doi:.https://doi.org/10.26444/aaem/99295
No financial support and no other potential conflict of interest relevant to this article was reported.