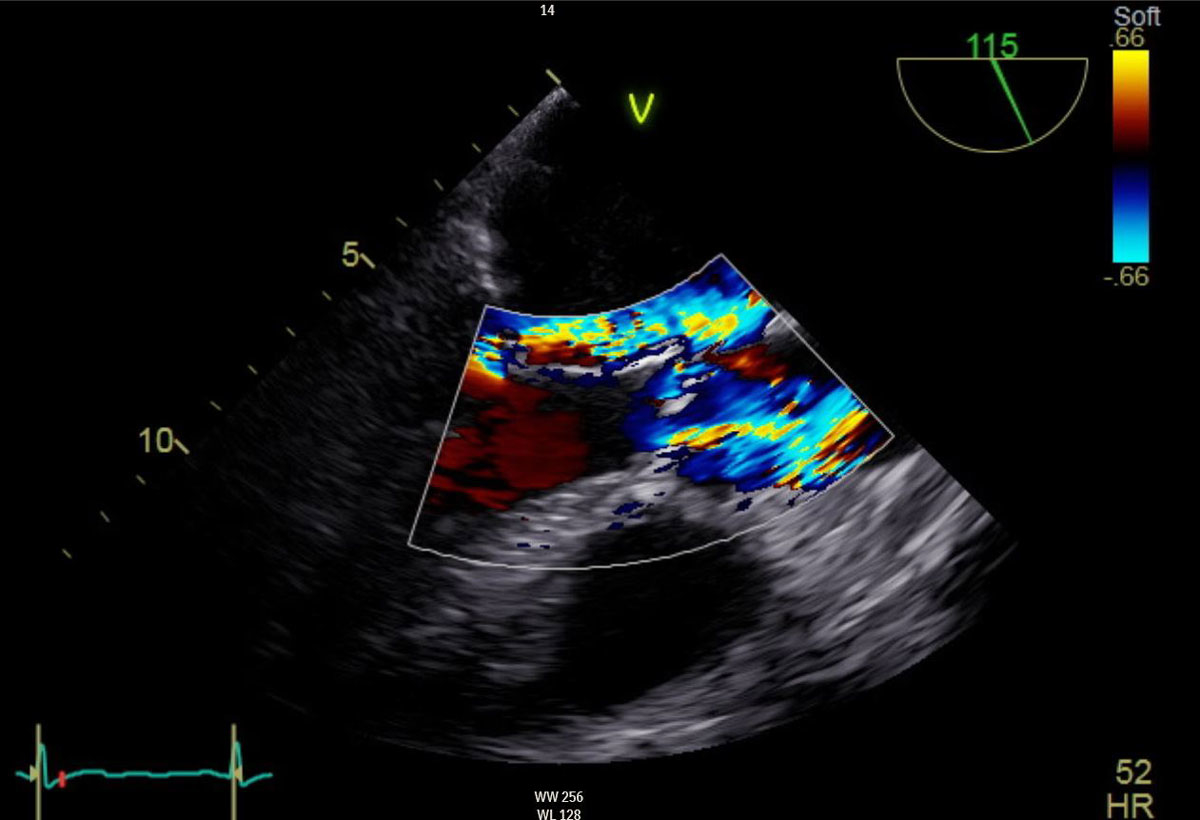
Figure 1 Severe mitral valve regurgitation with partial flail of the posterior mitral valve leaflet and moderate aortic valve stenosis. Preoperative transoesophageal echocardiography.
DOI: https://doi.org/10.4414/smw.2019.20168
Severe, symptomatic aortic valve stenosis and mitral valve regurgitation are an indication for surgical intervention according to the guidelines of the European Society of Cardiology and the European Association for Cardio-Thoracic Surgery [1]. Older and polymorbid patients comprise a special patient group, with significantly higher perioperative morbidity and mortality in the case of conventional surgical intervention. The continuous development of minimally invasive, transcatheter techniques has facilitated the treatment of such patients, through minimisation of the perioperative risk. We report the case of an 80-year-old, female, polymorbid patient with severe mitral valve regurgitation and moderate to severe aortic valve stenosis undergoing a concomitant transapical, transcatheter aortic valve implantation (transapical TAVI) and mitral valve reconstruction with the NeoChord system (NeoChord Inc, St. Louis Park, MN) [2], in an off-pump technique, on a beating heart and with a minimally invasive approach through a left anterolateral thoracotomy.
The 80-year-old female patient complained of dyspnoea on light exertion for almost a year, without orthopnoea or angina pectoris. After an episode of cardiac decompensation with pulmonary oedema requiring hospitalisation, the patient underwent an echocardiographic examination revealing severe mitral valve regurgitation because of rupture of tendinous cords with partial flail of the posterior mitral valve leaflet (fig. 1), as well as moderate aortic valve stenosis with a mean transvalvular gradient of 30 mm Hg on a tricuspid and severely calcified aortic valve. The left ventricular ejection fraction and dimensions were normal. Cardiac catheterisation showed no coronary artery disease and confirmed the above mentioned findings, showing an almost severe aortic valve stenosis with a mean transvalvular gradient of 36 mm Hg and with an indexed stroke volume of 42.6 ml/m2. Other comorbidities included chronic kidney disease (creatinine clearance 50 ml/min), status post invasive ductal carcinoma of the left breast with severe lymphoedema of the left arm, status post atrial flatter with conversion to sinus rhythm after treatment with amiodarone, arterial hypertension and severe obesity with a body mass index of 37.5 kg/m2. After interdisciplinary discussion in the heart team (cardiac surgery, cardiology and anaesthesiology) of our institution and because of the high calculated perioperative risk (EuroScore II 5.74%; STS score calculation not possible because of no support of combined mitral and aortic valve procedure) and frailty, it was decided to treat both valves concomitantly with a minimally invasive transcatheter procedure, through a left anterolateral thoracotomy, on a beating heart.
Figure 1 Severe mitral valve regurgitation with partial flail of the posterior mitral valve leaflet and moderate aortic valve stenosis. Preoperative transoesophageal echocardiography.
The procedure was performed through a left anterolateral thoracotomy with a 4 cm incision on the fifth intercostal space under the left breast. After preparation of the subcutaneous tissue and incision of the left pleura and the pericardium, felt-supported, purse string sutures were placed on the apex of the left ventricle (fig. 2). The apex of the left ventricle was then punctured and a guidewire placed through the aortic valve in the ascending aorta, under echocardiographic guidance. The sheath and the TAVI delivery system were introduced over the guidewire and positioned on the level of the aortic valve annulus. A 23-mm Edwards Sapien 3 valve (Edwards, Irvine, CA) was then implanted under rapid pacing with the subsequent intraoperative echocardiographic examination showing minimal paravalvular regurgitation. Afterwards, the TAVI deliver system was removed and the NeoChord system introduced (fig. 3). Subsequently, three neochords were implanted in the P2 segment under echocardiographic examination and the initially severe mitral valve regurgitation was decreased to a moderate one (fig. 4).

Figure 2 Left anterolateral thoracotomy under the left breast after incision of the pericardium and placement of purse string sutures on the apex of the left ventricle.
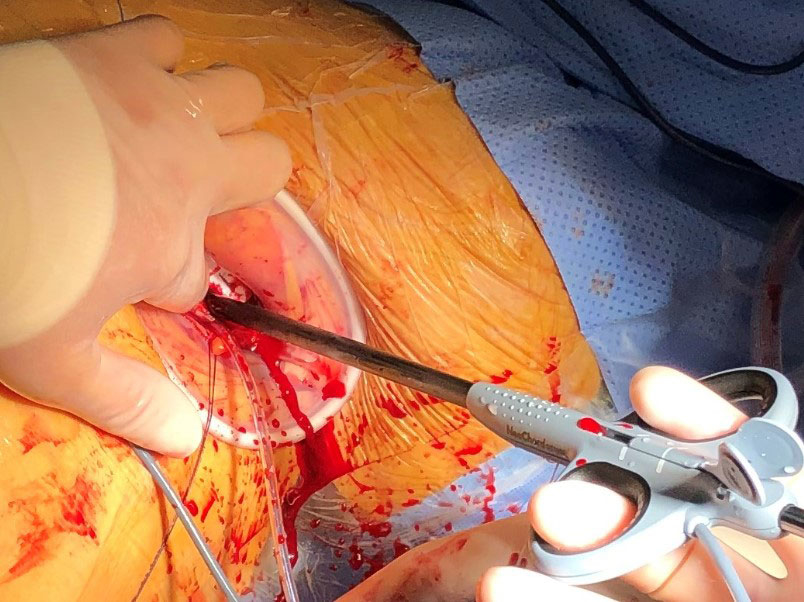
Figure 3 Introduction of the NeoChord system through the apex of the left ventricle.
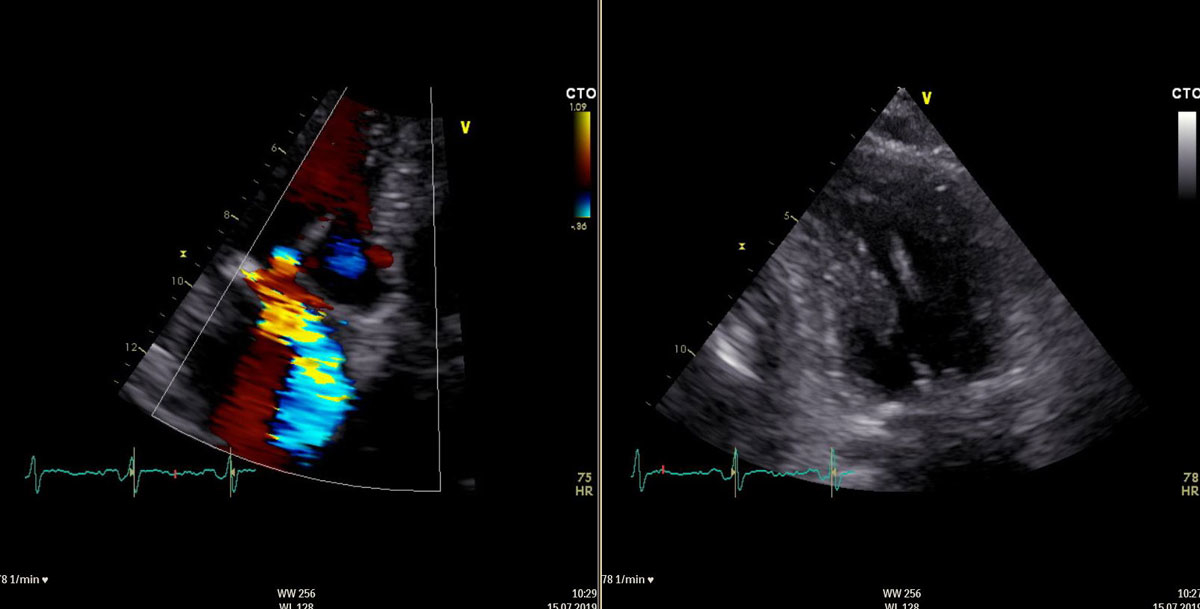
Figure 4 Moderate mitral valve regurgitation and implanted neochords. Postoperative transoesophageal echocardiography.
The postoperative course was uncomplicated except for a transient left bundle branch and first-grade atrioventricular block, a urinary tract infection, an activated arthrosis of the acromioclavicular joint and a left-sided pleural effusion requiring thoracentesis. The postoperative echocardiographic examination showed a good function of the implanted aortic valve with minimal paravalvular regurgitation and moderate regurgitation of the reconstructed mitral valve. The patient was discharged from hospital and referred for rehabilitation on the eighth postoperative day. Follow-up examination at 1 month postoperatively showed an unchanged echocardiographic result with minimal paravalvular regurgitation of the aortic valve and moderate mitral regurgitation, as well as a marked improvement of the functional status of the patient from New York Heart Association (NYHA) class III to NYHA class II.
The concomitant treatment of severe symptomatic aortic valve stenosis and mitral valve regurgitation is associated with high morbidity and mortality, with a reported in-hospital mortality of 5.4% for combined aortic valve replacement and mitral valve repair, and of 7% for double valve replacement [3]. In this article, we present the case of an 80-year-old female, polymorbid patient with high-grade symptomatic aortic valve stenosis and mitral valve regurgitation. Because of the high calculated perioperative risk, as well as her frailty, the interdisciplinary heart team decided to treat both valves concomitantly, using a minimally invasive transcatheter approach through a left anterolateral thoracotomy, on a beating heart. Because of the unfavourable mitral valve anatomy, with insufficient tissue for mechanical capping of the mitral valve leaflets, the mitral valve was deemed not amenable for MitraClip repair (Abbott, Abbott Park, IL).
The decision of the heart team to treat the aortic valve stenosis concomitantly with the mitral valve regurgitation, instead of a two-staged intervention, was taken in order to avoid any risk of cardiac decompensation after treatment of the mitral valve regurgitation and before the aortic valve intervention. Furthermore, a two-stage approach may increase the perioperative risk for the second operation because of pericardial adhesions and use of the same access route through the apex of the left ventricle. In addition, a two-stage procedure with a transapical aortic valve implantation following the transapical mitral valve reconstruction may cause a rupture of neochords or distortion of the delivery system causing malfunction of the reconstructed mitral valve. Even though the aortic valve stenosis was formally moderate, we decided to treat it because of a high mean transvalvular gradient of 36 mm Hg and because of concomitant surgery on the mitral valve though the same transapical access.
Interdisciplinary decision-making involving both cardiac surgeons and cardiologists is of great importance for the best treatment of complex cases, as shown here. Interdisciplinary heart teams are patient-oriented and aim at offering the best treatment through optimisation of the postoperative results and minimisation of the perioperative risk. The importance of their role has increased in recent years [4].
This is the first case in Switzerland of a concomitant transapical transcatheter aortic valve implantation and mitral valve reconstruction with the NeoChord system, in off-pump technique, on a beating heart and with a minimally invasive approach through a left anterolateral thoracotomy. Postoperatively, we showed a complete elimination of the aortic valve stenosis and an improvement of the initially severe mitral valve regurgitation to moderate.
The concomitant transapical, transcatheter intervention on the aortic and mitral valve is not widespread, with only four cases in three published articles reported in the literature [5–7]. The indication for the intervention was severe aortic valve stenosis and severe mitral valve regurgitation in two cases, moderate aortic valve stenosis and severe mitral valve regurgitation in one case and severe aortic valve regurgitation and severe mitral valve regurgitation in the fourth case. All four patients underwent transapical transcatheter aortic valve implantation first, followed by mitral valve reconstruction with the NeoChord system. After an uneventful postoperative course, echocardiographic examination showed good function of both valves in all cases, showcasing the safety and the efficacy of the concomitant transapical, transcatheter intervention in selected patient groups. Another two, two-stage cases are also reported in the literature, with the indication being severe aortic valve stenosis and severe mitral valve regurgitation. The patients underwent firstly a transapical transcatheter aortic valve implantation followed by a mitral valve repair using the MitraClip device (Abbott, Abbott Park, IL) in a second stage [8, 9]. The postoperative echocardiographic examination showed a good function of both valves also in these cases.
Our case emphasises the possibility of minimally invasive concomitant procedures on older and polymorbid patients with multivalvular heart disease, as these patients exhibit a high perioperative morbidity and mortality when treated with conventional surgery. As increasingly old and polymorbid patients will be presenting with a need for cardiac surgery in the future, it is of great importance that heart surgeons and especially residents become familiar with these minimally invasive techniques, in order to be able to provide the best possible treatment to this patient-group.
No financial support and no other potential conflict of interest relevant to this article was reported.
1 Baumgartner H , Falk V , Bax JJ , De Bonis M , Hamm C , Holm PJ , et al.; ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739–91. doi:.https://doi.org/10.1093/eurheartj/ehx391
2 Colli A , Zucchetta F , Torregrossa G , Manzan E , Bizzotto E , Besola L , et al. Transapical off-pump mitral valve repair with Neochord Implantation (TOP-MINI): step-by-step guide. Ann Cardiothorac Surg. 2015;4(3):295–7. doi:.https://doi.org/10.3978/j.issn.2225-319X.2015.05.01
3 Gillinov AM , Blackstone EH , Cosgrove DM, 3rd , White J , Kerr P , Marullo A , et al. Mitral valve repair with aortic valve replacement is superior to double valve replacement. J Thorac Cardiovasc Surg. 2003;125(6):1372–85. doi:.https://doi.org/10.1016/S0022-5223(02)73225-X
4 Zheng Z , Rao C , Du J . Is the era of the heart team coming? J Thorac Cardiovasc Surg. 2015;150(6):1664–5. doi:.https://doi.org/10.1016/j.jtcvs.2015.07.091
5 Zierer AF , Kammler J , Blessberger H , Ay M , Steinwender C . First in Man: Off-Pump Transapical Transcatheter Aortic Valve Implantation and Mitral Valve Repair. Ann Thorac Surg. 2019;107(4):e249–50. doi:.https://doi.org/10.1016/j.athoracsur.2018.07.062
6 Gerosa G , D’Onofrio A , Manzan E , Besola L , Bizzotto E , Zucchetta F , et al. One-stage off-pump transapical mitral valve repair and aortic valve replacement. Circulation. 2015;131(19):e430–4. doi:.https://doi.org/10.1161/CIRCULATIONAHA.114.014023
7 Stelzmueller M-E , Zilberszac R , Heinrich N , Mora B , Laufer G , Wisser W . Concomitant Transapical Transcatheter Aortic Valve Implantation and Transapical Mitral Valve Repair with NeoChord Implantation. Innovations (Phila). 2019:1556984519871905. Epub ahead of print. doi:.https://doi.org/10.1177/1556984519871905
8 Madder RD , Safian RD , Gallagher M , Senter SR , Hanzel GS . The first report of transcatheter aortic valve implantation and percutaneous mitral valve repair in the same patient. JACC Cardiovasc Interv. 2011;4(7):824. doi:.https://doi.org/10.1016/j.jcin.2011.05.009
9 Chan PH , Alegria-Barrero E , Patterson T , Davies S , Di Mario C , Franzen OW , et al. Successful dual-valve transcatheter therapy for severe aortic stenosis and mitral regurgitation. Int J Cardiol. 2012;157(2):e35–7. doi:.https://doi.org/10.1016/j.ijcard.2011.09.067
No financial support and no other potential conflict of interest relevant to this article was reported.