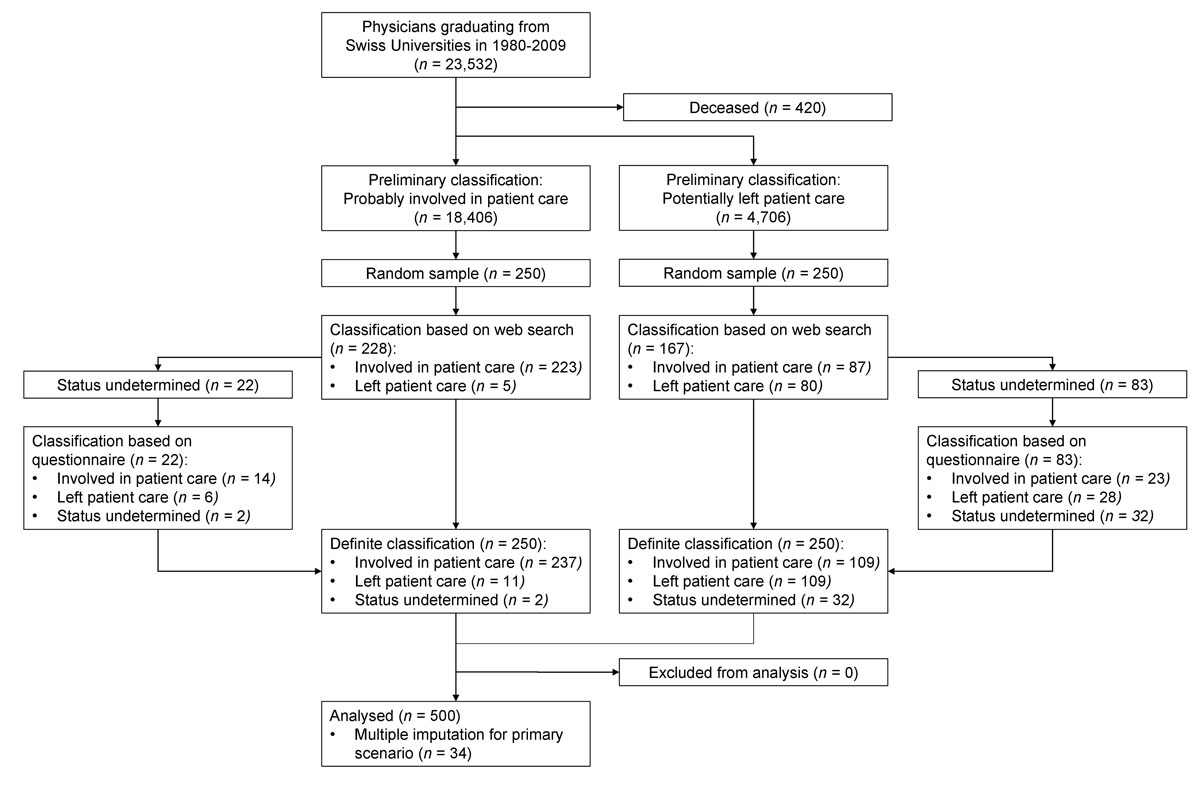
Figure 1 Inclusion and classification of the physicians.
DOI: https://doi.org/10.4414/smw.2019.20116
Physician shortage is an increasing problem in many countries. Too few young physicians enter the profession, and many practicing physicians leave patient care. There is much debate over why physicians leave practice, and reasons may differ across countries and healthcare systems. As the medical profession has become more feminised [1], media and politicians have often assumed a causal link between feminisation and physician attrition. A politician in the UK recently warned that “female doctors are putting a strain on the NHS” [2]. A US study speculated that female physicians are less productive because they work fewer hours [3]. In contrast, a systematic review in 2014 found that women physicians spent more time with their patients and that any negative effect feminisation has on the workforce is probably small [4].
Healthcare professionals often claim that physician dissatisfaction is the main reason for leaving patient care. In the US, it is commonly argued that the electronic health record (EHR) mandate [5] made record-keeping burdensome and reduced physicians’ time with patients [6], so that young doctors gain less clinical experience and waste more time on unnecessary clerical work [7]. In Switzerland, a hospital physician spends about 35% of their time directly caring for patients [8]. Physicians who face work-family conflicts may also withdraw from patient care, and such conflicts may be more common for women than men [9]. In 2015, the Swiss Association of residents and senior physicians (VSAO) speculated, without data, that between 14 and 21% of women physicians left patient care either temporarily or permanently [10].
We set out to estimate the percentage of physicians who left patient care in Switzerland, and to determine whether gender was associated with the decision to leave patient care.
This cross-sectional study nested in a national registry used two random samples drawn from the target population of all physicians who graduated between 1980 and 2009 from one of the five Swiss university medical schools.
In June 2015, we used the National Registry of Medical Professions (Medreg) in Switzerland, a public database that captures all newly graduated physicians from the five Swiss university medical schools, to identify all physicians who graduated in Switzerland between 1980 and 2009. This time window captured the largest number of physicians who had finished their postgraduate training and had not yet retired. We excluded physicians who died during or after 2015. Data collected from the registry included name, gender, year of medical school graduation, graduating university, and the language region the university was in (German vs French or Italian). These data were linked to data from the membership database of the Swiss Medical Association (FMH), which included current work addresses, email addresses, and phone numbers for physicians who consented to make this information publicly available. The FMH used their data on physician working status to classify physicians employed by hospitals, working in private practice or in postgraduate training as “probably involved in patient care”. The rest were classified as “potentially left patient care”. We selected an unrestricted random sample of 250 individuals from each category. The study was reviewed for compliance with Swiss data protection and privacy laws and approved by the boards of FMH and VSAO. Since no health-related data were collected, our study did not need additional approval by the research ethics committee. Randomly selected physicians were mailed an information letter signed by the Presidents of FMH and VSAO that explained the rationale and design of the study and its confidential nature.
Between 15 July and 4 August 2015, one of us (SC), who was unaware of the preliminary classification, searched professional directories such as www.medreg.admin.ch, www.doktor.ch, and www.doctorfmh.ch, and social media websites such as www.linkedin.com, www.facebook.com, and www.google.ch to determine the working status of each physician. If a physician was clinically active (i.e. in direct contact with patients) in a private practice or hospital, we definitively classified them as involved in patient care whether or not they were board certified. If a web search uncovered a current description of professional activity that ruled out involvement in patient care, we definitely classified the individual as having left patient care. If we could not make a definitive determination we classified the status of the physician as undetermined. Between 10 and 23 August 2015, physicians whose status was undetermined and who had a known email or postal address were invited to complete an online questionnaire about their working status in German or French. All non-responders were sent a reminder letter by postal mail a week after the initial invitation; this letter included a postal questionnaire.
To determine the feasibility of the search and help us determine sample size, we performed a pilot study in unrestricted random samples of 30 physicians from the FMH’s preliminary classification of physicians into those who were either probably involved in patient care or have potentially left patient care. One of us (SC) performed the searches described above and classified individuals as “involved in patient care”, “left patient care” or “status undetermined”. Another investigator (SS) checked two random samples of 15 individuals each. We came to agreement on all 30 classifications. In the random sample of those the FMH had classified as probably involved in patient care, 27 were definitely classified as involved in patient care (90%) and 3 remained undetermined (10%). Among those the FMH classified as potentially left patient care, 19 were clinically active (63%), 5 had left patient care (17%) and the status of 6 remained undetermined (20%).
Based on data from the pilot study, we estimated that 16% of physicians had left patient care (95% confidence interval [CI] 7–26%) after taking the sampling strategy into account. Assuming percentages of physicians who had left patient care of this approximate magnitude, a sample size of 250 physicians per stratum would result in widths of two-sided 95% CIs around 5% after accounting for the stratified random sampling strategy.
We first calculated the proportion of physicians who had left patient care and 95% CI, using the svy family of commands in Stata that appropriately took the complex sampling design of the study into account. The number of physicians who graduated between 1980 and 2009 and had left patient care by August 2015 was calculated by multiplying the point estimate and 95% CIs of the proportion with the total number of physicians of 23,112 who had graduated during this period and were alive in August 2015. As the length of follow-up varied depending on the year of graduation, we used Poisson regression to calculate rates, and univariable and multivariable Cox proportional hazards models adjusted for all three covariates to calculate hazards ratios (HRs) for the association of leaving patient care with gender (women vs men), language region (German- vs Italian-/French-speaking parts of Switzerland) and year of graduation (1995–009 vs 1980–1994 as a reference group). Rates were estimated for 5-year bands of graduation. The period from 1995–2009 was deemed to represent the current generation of 30- to 45-year-olds, who were most likely to be actively engaged in family planning.
For the calculation of rates and HRs, we used two different scenarios. For scenario 1, we used the full length of follow-up from graduation to August 2015 for physicians who had stayed involved in patient care, and assumed the time of event occurrence for physicians who had left patient care to be at 50% of the time elapsed between graduation and August 2015. As the length of follow-up depended on the year of graduation, this scenario would likely overestimate the difference in rates between physicians who graduated late (1995–2009) and physicians who graduated early (1980–1994). In a conservative and probably more realistic scenario (scenario 2), we therefore censored the follow-up of physicians who had stayed involved in patient care at 10 years, and assumed that the time of event in physicians who had left patient care had occurred between 5 and 10 years after graduation, using a uniform distribution for the event probability between 5 and 10 years. For all analyses, we used multiple imputation to account for undetermined status, with stratum, gender, region of origin and year of graduation included in the imputation model to create 20 datasets. All analyses were done in STATA version 15.1 (STATA corporation, College Station, TX, USA) and accounted for the stratified random sampling strategy.
In the National Registry of Medical Professionals, we identified 23,532 individuals who graduated between 1980 and 2009 (fig. 1). We excluded 420 physicians (1.8%) who had died. Of the remaining 23,112 physicians, preliminary classification identified 18,406 (79.6%) who were probably involved in patient care and 4706 (20.4%) who had potentially left patient care.
Figure 1 Inclusion and classification of the physicians.
Of the 250 physicians classified as probably involved in patient care, we found that 223 (89.2%) were involved in patient care and 5 (2.0%) had left patient care. After searching the web, we could not determine the status of 22 (8.8%). Twenty of these responded to our questionnaire; 14 were involved in patient care and 6 had left patient care. Of the 250 physicians classified as having potentially left patient care, we found that 87 (34.8%) were involved in patient care and 80 (32.0%) had left patient care, whereas 83 (33.2%) remained undetermined. Of the 83 physicians with undetermined status, 51 responded to our questionnaire: 23 were involved in patient care and 28 had left patient care. Table 1 shows a cross-tabulation of baseline characteristics by type of classification (definitive or preliminary). There was no evidence for associations between baseline characteristics and definite status for physicians probably involved in patient care or those who had potentially left patient care (p-values between 0.29 and 1.00).
Table 1 Cross-tabulation of baseline characteristics with the definitive classification of physicians stratified by the preliminary classification.
| Characteristics, n (%) | Definitive classification | p-value* | ||
|---|---|---|---|---|
|
Involved in patient care
(n = 346) |
Left patient care
(n = 120) |
Status undetermined
(n = 34) |
||
| Preliminary classification: probably involved in patient care | ||||
| n = 237 | n = 11 | n =2 | ||
| Women | 94 (39.7) | 4 (36.4) | 2 (100) | 0.29 |
| German-speaking origin | 158 (66.7) | 7 (63.6) | 1 (50.0) | 1.00 |
| Year of graduation between 1995 and 2009 | 109 (46.0) | 5 (45.5) | 2 (100) | 0.38 |
| Preliminary classification: potentially left patient care | ||||
| n = 109 | n = 109 | n = 32 | ||
| Women | 56 (51.4) | 51 (46.8) | 19 (59.4) | 0.44 |
| German-speaking origin | 80 (73.4) | 81 (74.3) | 23 (71.9) | 0.96 |
| Year of graduation between 1995 and 2009 | 70 (64.2) | 67 (61.5) | 23 (71.9) | 0.56 |
* Fisher’s exact test for those probably involved in patient care, chi-square test for those who had potentially left patient care.
For all graduation years, 1980 to 2009 combined, we estimated that an average of 13.6% had left patient care (95% CI 11.1–16.1%). For physicians who had graduated between 1980 and 1994, the estimate was 11.3% (95% CI 7.9–14.7%); for those who graduated between 1995 and 2009, the estimate was 15.9% (95% CI 12.2–19.6%). Based on these numbers, a total of 3149 physicians were estimated to have left patient care by August 2015 (95% CI 2575–3722).
Figure 2 shows the estimated rates of physicians who left patient care by 5-year bands of graduation. Panel A shows the rate of physicians who left patient care for scenario 1, based on year of graduation, with 95% CI. Across the entire period from 1980 to 2009, the rate of physicians who left patient care was 0.7 per 100 physicians/year (95% CI 0.6–0.8). For physicians who graduated between 1980 and 1994, we estimated a rate of 0.4 per 100 physicians/year (95% CI 0.3–0.6). For those who graduated between 1995 and 2009, we estimated a rate of 1.3 per 100 physicians/year (95% CI 1.0–1.7).
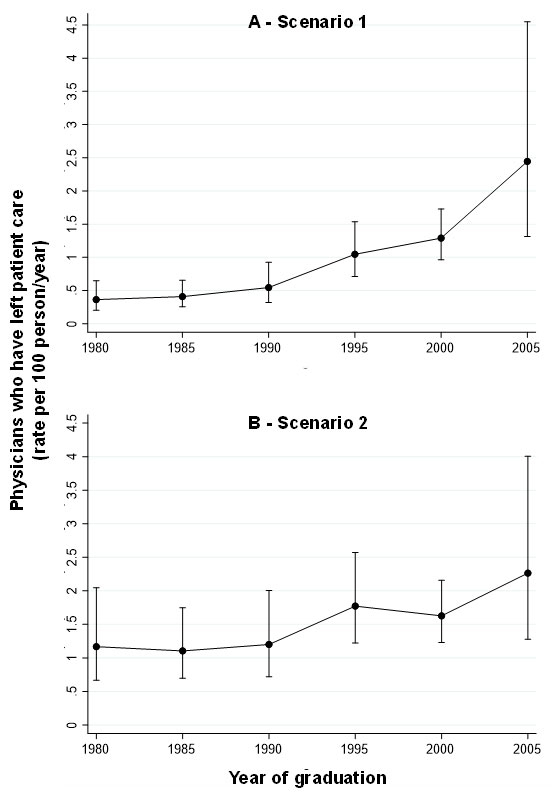
Figure 2 Rates of physicians leaving patient care by year of graduation and scenario.
Figure 2 panel B shows the rate of physicians who left patient care based on scenario 2. In the period between 1980 and 2009, the rate of physicians who had left patient care was 1.5 per 100 physicians/year (95% CI 1.2–1.8). For physicians who graduated between 1980 and 1994 we estimated a rate of 1.2 per 100 physicians/year (95% CI 0.9–1.6); for those who graduated between 1995 and 2009, we estimated a rate of 1.8 per 100 physicians/year (95% CI 1.4–2.3).
Table 2 shows the result of the subgroup analysis. In univariable (left) and multivariable Cox regression models (right), there was evidence for an association of leaving patient care only with period of graduation. According to scenario 1, the HR comparing physicians who graduated late (1995–2009) with physicians who graduated early (1980–1994) was 2.50 in the univariable analysis (95% CI 1.67–3.74) and 2.52 in the adjusted analysis (95% CI 1.68–3.78). According to the more realistic scenario 2, the HR was 1.72 in the univariable analysis (95% CI 1.11–2.67) and 1.74 in the adjusted analysis (95% CI 1.12–2.70).
Table 2 Hazard ratios of leaving patient care for the association with gender (women versus men), region (German speaking part of Switzerland versus French and Italian speaking part of Switzerland) and year of graduation (1995–2009 versus 19801994) for scenarios 1 and 2.
| Factor |
Hazard ratios of having left patient care
(with 95% confidence interval) |
||||
|---|---|---|---|---|---|
| Univariable analysis | p-value | Multivariable analysis | p-value | ||
| Scenario 1 | Women | 1.24 (0.80–1.91) | 0.33 | 1.17 (0.76–1.82) | 0.47 |
| German-speaking region of origin | 1.16 (0.71–1.89) | 0.55 | 1.27 (0.77–2.09) | 0.35 | |
| Graduation 1995–2009 | 2.50 (1.67–3.74) | <0.001 | 2.52 (1.68–3.78) | <0.001 | |
| Scenario 2 | Women | 1.17 (0.76–1.80) | 0.48 | 1.11 (0.72–1.71) | 0.63 |
| German-speaking region of origin | 1.21 (0.74–1.96) | 0.45 | 1.28 (0.79–2.09) | 0.32 | |
| Graduation 1995–2009 | 1.72 (1.11–2.67) | 0.015 | 1.74 (1.12–2.70) | 0.014 | |
See methods section for a description of the two scenarios. Reading help for the last line of the table: the hazard ratio of having left patient care comparing those graduating 1995–2009 with those graduating 1980–1994 is 1.72 in the univariable analysis of the more realistic scenario 2, corresponding to a 72% relative increase in the risk of leaving patient care during the later as compared with the earlier period. The association was still found in the multivariable analysis after adjustment for gender and language origin, with a hazard ratio of 1.74, corresponding to a 74% relative increase.
About one in seven physicians who graduated in Switzerland between 1980 and 2009 had left patient care. Our multivariable analysis of both scenarios showed that physicians who had graduated between 1995 and 2009 were less likely to participate in patient care than those who graduated before 1995. Our analyses revealed no evidence for gender differences or an association with language region.
Few studies are comparable to ours (table 3). Studies usually focus on “intention to leave patient care”, which varies widely and depends on setting and the physicians sampled. The few studies in table 3 that assessed departure from patient care also varied widely, from 3% to 17%. Degen and colleagues’ systematic review found that the percentage of physicians who intended to leave patient care ranged from 3% to 54% in Finland, France, Germany, the UK, and the US [11]. When physicians were asked about their intention to leave ‘direct patient care within 5 years’, answers from four of the studies in the review ranged from 11.8% to 22%. In a prospective cohort study, Hann et al. [12] established a causal link between intention and subsequent departure from patient care. The investigators asked 1174 GPs in the UK about their intention to leave patient care and followed them up 5 years later. They found 1 in 6 GPs left patient care within 5 years; intention to leave (measured 5 years earlier) was the strongest predictor.
Table 3 Intention and effectively leaving patient care in different samples of physicians across countries.
| Country | Type of physicians analysed | Intention to leave patient care | Left patient care in their country | Source/year |
|---|---|---|---|---|
| Germany | Different specialties, from inpatient and outpatient care in Munich | 54% | Bornschein et al. 2006 | |
| Germany | Hospital physicians working in surgical fields (surgery, gynaecology, obstetrics) | 21% | von dem Knesebeck et al. 2010 | |
| Germany | Different specialities, junior physicians in their first or second postgraduate year in Bavaria | 52% | Ochsmann 2012 | |
| France | Different specialities in French hospitals | 17% | Estryn-Behar et al. 2011 | |
| United Kingdom | Family physicians <50 years | 17% | Hann et al. 2010 | |
| United Kingdom | Different specialities | 23% | Davidson et al. 1998 | |
| United Kingdom | Different specialities | 52% | Davidson et al. 2001 | |
| United Kingdom | Different specialities, 5 years after graduation (excluding emigration) | 5–9% | cited in "The Supply of Physician Services in OECD Countries" page 37 | |
| United States | Different specialities, physicians practicing in urban settings in California | 5% | 4% | Rittenhouse et al. 2004 |
| United States | Different specialities, in primary and secondary care physicians | 19% | Williams et al. 2001 | |
| United States | Physicians aged ≥50years | 38% | Hawkins, 2000, (cited in "The Supply of Physician Services in OECD Countries" page 38) | |
| United States | Different specialities, with symptoms of burnout | 54% | Tait D. Shanafelt 2016 | |
| United States | Different specialities, physicians in Atlanta | 50% | Jackson Healthcare, 2012 | |
| United States | Different specialities | 55% | Joanne Finnegan, 2016 | |
| Canada | Full sample of all physicians in Canada | 3% | Scott’s Medical Database, 2016, Canadian Institute for Health Information |
Contrary to prevalent opinion in Switzerland, women were no more likely to leave patient care than men. Mache and colleagues’ 2015 study of work-family conflicts and other studies also found that gender was not associated with leaving patient care [13–15]. Men and women were equally likely to report work-family conflicts, and these conflicts were tentatively associated with the decision to leave patient care [9]. Other studies did find gender differences [16–18]. For example, Adám et al. surveyed a cross-section of 123 Hungarian physicians. In in-depth interviews, they found that female physicians reported more work-family conflicts and “less parental, spousal and peer support” than men [16]. This suggests that lack of social support, rather than the feminisation of the profession, could explain why physicians leave patient care.
Our study was not designed to assess the reasons why physicians leave patient care, but early studies found a variety of causes, from family or personal problems, to dissatisfaction with the work load, healthcare reforms that burdened them with administrative tasks, less opportunity for direct patient contact, and rising patient expectations [19–21]. Petterson et al. analysed a cohort of 80,000 US physicians and found that about 11% of those over 55 had started to participate in activities other than patient care late in their careers (i.e., administration, teaching and research) [22]. Physicians also leave patient care because they get burned out. Pantenburg et al. identified a cross-sectional association between the desire to leave patient care and burnout in a sample of about 2400 German physicians: 30% of physicians with burnout wanted to permanently leave patient care, but only 16% of those without burnout felt similarly [23].
Our study has several limitations. First, we were unable to identify the working status of 34 out of 500 (6.8%) of the physicians sampled. We therefore used multiple imputation to account for the undetermined status of these physicians in all analyses. Second, the length of follow-up in our study varied depending on the year of graduation. We therefore used Poisson regression to calculate rates, and Cox proportional hazards to determine the association of having left patient care with gender, language region and period of graduation. As our design prevented collection of the specific time when physicians had left patient care, we performed analyses using two different scenarios. For scenario 1, we used the full length of follow-up from graduation to August 2015 for physicians who had stayed involved in patient care. As the length of follow-up depended on the year of graduation, this scenario would likely overestimate the difference between physicians who graduated late and physicians who graduated early. We therefore developed a conservative and more realistic scenario 2, in which we censored the follow-up of physicians who had stayed involved in patient care at 10 years, and assumed that the time of event in physicians who had left patient care had occurred between 5 and 10 years after graduation. The two scenarios are likely to cover the full range of plausible differences in rates of having left patient care between physicians who graduated late and physicians who graduated early. Finally, the power of our study was low to detect smaller associations, and there is a possibility of residual confounding. Strengths of the study include its innovative design with efficient use of existing data sources and surveys in random samples representative of physicians who graduated in Switzerland during a 30-year period, and its novelty, as this is the first conducted study to estimate the percentage of physicians who actually left patient care in Switzerland.
As the population ages, medical specialisation and the shortage of general practitioners must be reversed and the healthcare system must retain physicians in the clinical workforce. Future studies should ask why Swiss physicians leave patient care, with an eye toward designing and testing effective interventions that address preventable and solvable problems that cause physicians to turn away from clinical practice and that discourage them from returning.
Approximately one in seven physicians in Switzerland who graduated between 1980 and 2009 left patient care. Leaving patient care was not associated with gender, but the probability of leaving patient care was increased considerably in physicians who graduated more recently. Interventions that aim at keeping physicians in the work force and encourage their return to practice are sorely needed.
We thank the Swiss Medical Association (FMH), especially Esther Kraft, and the Swiss Association of residents and senior physicians (VSAO) for their support to conduct this study. We also thank Sophie Mantelli for helping us produce table 3 of this paper.
This project was funded by Swiss Medical Association (FMH) and the Swiss Association of resident and senior physicians (VSAO). FMH and VSAO helped define the aims of this study and consented to the method used but did not help analyse or interpret the data.
The authors declare no conflict of interest.
1 Kraft E , Hersperger M . Ärzteschaft in der Schweiz – die Feminisierung der Medizin. Schweiz Arzteztg. 2009;90(47):1823–5. doi:https://doi.org/10.4414/saez.2009.14776
2Dominiczak P. Female doctors who work part-time after having children put NHS under strain. The Telegraph. 2013 June 5
3 Petterson SM , Liaw WR , Tran C , Bazemore AW . Estimating the residency expansion required to avoid projected primary care physician shortages by 2035. Ann Fam Med. 2015;13(2):107–14. doi:.https://doi.org/10.1370/afm.1760
4 Hedden L , Barer ML , Cardiff K , McGrail KM , Law MR , Bourgeault IL . The implications of the feminization of the primary care physician workforce on service supply: a systematic review. Hum Resour Health. 2014;12(1):32. doi:.https://doi.org/10.1186/1478-4491-12-32
5Krauthammer C. Why doctors quit. The Washington Post. 2015 May 28.
6 Detsky AS , Gropper MA . WHy physician leaders of health care organizations should participate in direct patient care. Ann Intern Med. 2016;165(7):519–20. doi:.https://doi.org/10.7326/M16-0820
7Lister S. Ministers take doctor's battle to Europe. The Times. 2010.
8 Hehli S . Mediziner versinken in der Papierflut. Neue Zür Ztg. 2016 January 6
9 Mache S , Bernburg M , Vitzthum K , Groneberg DA , Klapp BF , Danzer G . Managing work-family conflict in the medical profession: working conditions and individual resources as related factors. BMJ Open. 2015;5(4):e006871. doi:.https://doi.org/10.1136/bmjopen-2014-006871
10 Hehli S . Wenn Ärztinnen ihren Kittel an den Nagel hängen. Neue Zür Ztg. 2015 February 5
11 Degen C , Li J , Angerer P . Physicians’ intention to leave direct patient care: an integrative review. Hum Resour Health. 2015;13(1):74. doi:.https://doi.org/10.1186/s12960-015-0068-5
12 Hann M , Reeves D , Sibbald B . Relationships between job satisfaction, intentions to leave family practice and actually leaving among family physicians in England. Eur J Public Health. 2011;21(4):499–503. doi:.https://doi.org/10.1093/eurpub/ckq005
13 Hill EJ . Work-Family Facilitation and Conflict, Working Fathers and Mothers, Work-Family Stressors and Support. J Fam Issues. 2005;26(6):793–819. doi:.https://doi.org/10.1177/0192513X05277542
14 Yavas U , Babakus E , Karatepe OM . Attitudinal and behavioral consequences of work‐family conflict and family‐work conflict: Does gender matter? Int J Serv Ind Manage. 2008;19(1):7–31. doi:.https://doi.org/10.1108/09564230810855699
15 Fuß I , Nübling M , Hasselhorn H-M , Schwappach D , Rieger MA . Working conditions and Work-Family Conflict in German hospital physicians: psychosocial and organisational predictors and consequences. BMC Public Health. 2008;8(1):353. doi:.https://doi.org/10.1186/1471-2458-8-353
16 Treister-Goltzman Y , Peleg R . Female Physicians and the Work-Family Conflict. Isr Med Assoc J. 2016;18(5):261–6.
17 Dumelow C , Littlejohns P , Griffiths S . Relation between a career and family life for English hospital consultants: qualitative, semistructured interview study. BMJ. 2000;320(7247):1437–40. doi:.https://doi.org/10.1136/bmj.320.7247.1437
18 Adám S . Magas a munkahelyi és a családi szerepek közötti konfliktus prevalenciája az orvosnok körében: a társas támogatás hiánya mint lehetséges rizikótényezo [High prevalence of work-family conflict among female physicians: lack of social support as a potential antecedent]. Orv Hetil. 2009;150(50):2274–81. In Hungarian. doi:.https://doi.org/10.1556/OH.2009.28583
19 Young R , Leese B , Sibbald B . Imbalances in the GP Labour Market in the UK: Evidence from a Postal Survey and Interviews with GP Leavers. Work Employ Soc. 2001;15(4):699–719. doi:.https://doi.org/10.1177/095001701400438161
20 Scott A , Gravelle H , Simoens S , Bojke C , Sibbald B . Job Satisfaction and Quitting Intentions: A Structural Model of British General Practitioners. Br J Ind Relat. 2006;44(3):519–40. doi:.https://doi.org/10.1111/j.1467-8543.2006.00511.x
21 Bornschein S , Erbas B , Borelli S , Emminger C , Hesse J , Pilz J , et al. Arbeitszeit und Arbeitszufriedenheit angestellter und beamteter Arzte in München. Ergebnisse einer anonymen Befragung [Working hours and job satisfaction among physicians in hospitals and general practice in Munich. Results of an anonymous questionnaire]. Gesundheitswesen. 2006;68(8-9):535–44. In German. doi:.https://doi.org/10.1055/s-2006-927070
22 Petterson SM , Rayburn WF , Liaw WR . When Do Primary Care Physicians Retire? Implications for Workforce Projections. Ann Fam Med. 2016;14(4):344–9. doi:.https://doi.org/10.1370/afm.1936
23 Pantenburg B , Luppa M , König HH , Riedel-Heller SG . Burnout among young physicians and its association with physicians’ wishes to leave: results of a survey in Saxony, Germany. J Occup Med Toxicol. 2016;11(1):2. doi:.https://doi.org/10.1186/s12995-016-0091-z
Contributed equally
This project was funded by Swiss Medical Association (FMH) and the Swiss Association of resident and senior physicians (VSAO). FMH and VSAO helped define the aims of this study and consented to the method used but did not help analyse or interpret the data.
The authors declare no conflict of interest.