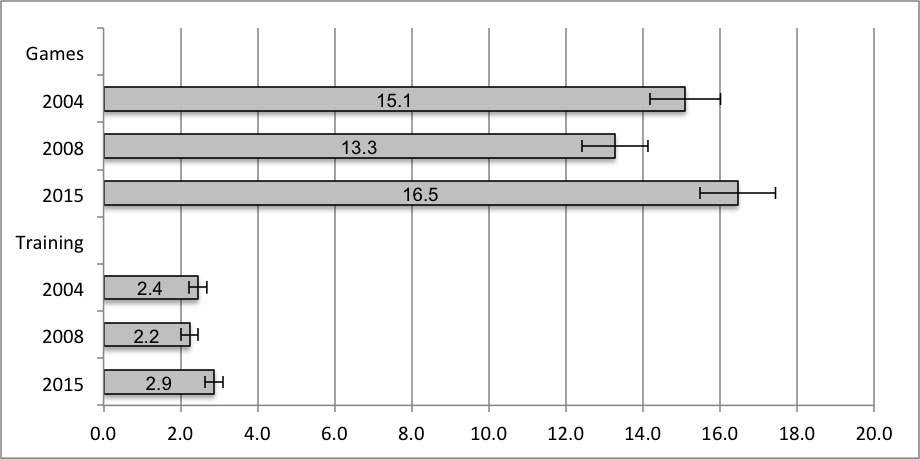
Figure 1 Injury incidence in amateur soccer per 1000 hours of playing during the previous 4 weeks (including 95% confidence intervals).
DOI: https://doi.org/10.4414/smw.2018.14690
The overall injury incidence in amateur soccer typically ranges from 5.2 to 12.4 per 1000 hours of play [1–4] and is higher during games than in training [5–7]. Previous studies of amateur soccer have reported injury incidences of 2.0 to 4.5 per 1000 hours for training and 12.3 to 24.7 per 1000 hours for match play [1, 2, 4, 8].
To our knowledge, studies addressing long-term changes in injury incidence in amateur soccer are scarce. Esquivel et al. [9] observed the estimated number of soccer-related injuries of people aged 5 to 49 years in the USA from 2000 to 2012. They concluded that the injury rate in youth soccer was increasing, despite a decline in participation. With respect to adult soccer, they reported an increase in the number of injuries that was higher than the increase in participation. In contrast, a decreased number of injuries per 100 players was found when data obtained by the Belgian Football Association from the seasons 1999/00 and 2009/10 were compared [10], although there was a higher percentage of severe injuries in the season 2009/10. However, no injury incidences were provided in the two above-mentioned studies. Junge et al. [8] compared injury incidences of Swiss amateur players between 2004 and 2008. They reported that teams performing the prevention programme “The 11” reduced the incidence of all game injuries by 17%, of noncontact game injuries by 27%, and of training injuries by 19% during this period. For other teams, injury rates during games remained stable, whereas injury rates during training increased by 9%. Unfortunately, this study only covered a short time period.
Only a few studies focusing on elite and professional club soccer provide more information about the long-term development of injury incidences [11–16]. Several studies analysing different periods between 1992 and 2010 found no changes with respect to the total injury incidence in professional soccer teams [11–15]. Training and game injury rates, as well as the incidence of severe injuries and muscle injuries, were also stable for top European male teams between 2001 and 2008 [14], but Dauty and Collon [13] concluded that the rate of muscle injuries had increased continuously in a French professional team between the seasons 1995/96 and 2009/10. Contrary to expectations, another study showed a decreasing tendency with regard to injury rates between 1993 and 2007 for professional soccer games in Japan [11].
Finally, one further study analysed the trend of injury incidence of male and female players in different world soccer tournaments between 1998 and 2012 [17]. The results suggest that the average number of injuries per game decreased in both men’s FIFA World Cups and the tournaments of the Olympic Games during this period, but increased for the corresponding female tournaments. The incidence of noncontact injuries remained stable; the trends mentioned above were mainly caused by changes in the frequency of contact injuries.
In Switzerland, 80,000 soccer-related injuries are recorded annually [18]. Consequently, injury prevention has been promoted in recent years. Between the years 2004 and 2011, all soccer coaches were instructed during their basic education and during refresher courses to implement “The 11” in their soccer training. Since 2011, another prevention programme called “Sports Basics” has been promoted and implemented in the education of coaches. Additionally, in 2007, fair play measures were launched in low-level amateur soccer leagues and junior leagues. More specifically, a penalty point system for red and yellow cards was implemented, which is of relevance for the final ranking of a team.
Although detailed information about changes of injury incidence with respect to level of play, injury causes and injury characteristics can make an important contribution to improving injury prevention, thus far little is known about the long-term development of injury incidences in amateur soccer. Therefore, the purpose of the present study was to compare injury incidences in Swiss amateur soccer between the years 2004, 2008 and 2015. More specifically, the present article focuses on the following three research questions. (1) How has injury incidence changed in amateur soccer? (2) How has injury incidence changed in different amateur soccer leagues? (3) How have injury characteristics and injury causes changed in amateur soccer?
In May 2004, May 2008 and May 2015, three representative samples of Swiss amateur soccer coaches were interviewed about the frequency and characteristics of injuries in their teams. Detailed information about study design and samples of 2004 and 2008 have been provided by Junge et al. [8]. In 2004, 1029 amateur coaches were interviewed, whereas 1015 coaches participated in the 2008 survey.
For the latest survey, a random sample of 1260 coaches was contacted by telephone. The sample was drawn from a complete list provided by the Swiss Football Association (SFV) of 5719 coaches who were engaged either in male amateur leagues (including 2nd–5th amateur league, juniors 14–20 years and 30+/40+ leagues) or in female leagues (all levels). Of the selected coaches, 1008 were willing to take part in the survey (80.0% response rate). The 252 (20.0%) nonresponses were due to the following: no longer coaching a soccer team (n = 64), not coaching an amateur team (n = 22), could not be contacted because of unavailability (did not answer the telephone call repeatedly) (n = 50), incorrect telephone numbers (n = 37, and other reasons (n = 21) such as language problems. Additionally, 58 coaches refused to be interviewed.
The computer-assisted, fully structured telephone interviews were conducted by the LINK Institute, which specialises in this kind of survey. On average, an interview took 21 minutes to complete. In Switzerland, the ethics committee approval is not mandatory for anonymised surveys as documented by Art. 2 HRA (Human Research Act) and Art. 25 HRO (Human Research Ordinance). Nevertheless, the study followed the ethical principles described in the Declaration of Helsinki.
The content of the 2015 telephone interviews was almost identical to the survey carried out in 2008, which was developed by Junge et al. [8] and followed the consensus statement of Fuller et al. [19] (the survey used in the 2015 telephone interviews is available on request in German and French language from the corresponding author). First, the coaches had to answer some questions about their team (league, team size, training frequency, etc.). Second, they had to report the number of games played by their team during the previous 4 weeks and to describe all injuries that happened during these games. To achieve the highest level of accuracy with respect to the injury reports, the interviewers strictly guided the coaches. The coaches were instructed to remember the last game and the opposing team. Then they were asked to report the injuries that occurred (for their players) during this specific game. For each injury, the coaches were asked to provide detailed information (body region, type, contact, foul play, severity, medical attention). This procedure was repeated for all games that took place during the previous 4 weeks. Third, the coaches were asked about the number of training injuries that had occurred during the previous 4 weeks, and were invited to provide detailed information about each injury. Finally, the coaches were asked to respond to some questions about their personal background (age, gender, experience as a coach).
Based on the answers of the coaches, injury incidences were calculated as injuries per 1000 hours of game play and as injuries per 1000 hours of training. For the calculation of injury incidence during games, a maximum of five games was considered, in order to reduce recall bias. With respect to games, total exposure time was defined as the product of the number of games, the duration of a game (1.5 hours) and the number of players (11 players); for training exposure, time was calculated as the product of the average number of training sessions per week, the average duration of a training session, the average number of players per training session, the number of weeks for this study period (4 weeks) and the number of teams involved.
Data were analysed using the Statistical Package for the Social Sciences software (version 22.0; SPSS Inc). Descriptive data are presented as percentages, means including standard deviations (SDs), and means including bias-corrected and accelerated 95% confidence intervals (BCa 95% CIs) calculated by bootstrapping with 1000 replications [20]. Differences between the three surveys with respect to the distribution of coaches by league and with respect to team characteristics were tested with χ2 statistics and t-tests, respectively. To avoid alpha error inflation, Bonferroni correction was applied. Thus, differences were considered significant at p <0.017. Injury incidence was calculated with Excel 2011 for Mac (Microsoft, Redmond, WA, USA) and defined as the number of injuries divided by the total person-time at risk. To establish the significance of the difference between injury incidences, 95% confidence intervals (95% CIs) were calculated with the following formula [21]:
Incidence rate ± 1.96 * √(number of injuries) / (person-time at risk)
The criterion for statistical significance was set according to Field [20] who states that a moderate overlap between the bars of the 95% confidence intervals (no more than half of each bar) represents a p-value of ≈0.05.
In 2004, 2008 and 2015 almost all interviewed coaches were male (99%). On average, they were about 40 years old (2004: mean 40.3, SD 9.2; 2008: mean 41.6, SD 9.6; 2015: mean 40.6, SD 10.7) and had more than 10 years of experience as soccer coaches (2004: mean 10.4, SD 7.8; 2008: mean 11.9, SD 7.9; 2015: mean 11.0, SD 8.9). A majority of all coaches was responsible for a male soccer team. However, the percentage of respondents coaching female teams increased from 3.3% in 2004 to 9.8% in 2015 (χ2[1, 2035] = 35.302, p <0.001). The representation of the other leagues did not differ significantly between the years 2004 and 2015 and the years 2008 and 2015.
There were only some slight changes from 2004 to 2015 with respect to team characteristics (table 1). However, due to the large sample sizes, differences in all team characteristics (with the exception of training duration) were statistically significant. In 2015, the average number of players per team was 1.4 players more than in 2004, whereas the average number of players participating per training session increased by nearly one player. In contrast, the average number of reported games played during the previous 4 weeks was slightly lower in 2015, whereas training load (number of training sessions per week and training duration) remained relatively stable across the examined time period.
Table 1 Team and exposure characteristics (arithmetic mean and bias-corrected and accelerated 95% confidence intervals).
| 2004 | 2008 | 2015 | |
|---|---|---|---|
| Team size | 18.6 (18.4–18.9) | 19.3 (19.0–19.5)‡ | 20.0 (19.7–20.2)*† |
| No. of games (previous 4 weeks) | 4.3 (4.2–4.3) | 4.4 (4.3–4.4) | 4.0 (4.0–4.1)*† |
| No. of training sessions per week | 2.0 (2.0–2.0) | 2.1 (2.0–2.1) ‡ | 2.1 (2.0–2.1)* |
| Duration of training (in minutes) | 92.0 (91.2–92.9) | 91.0 (90.4–91.5) | 91.0 (90.1–91.5) |
| No. of players per training session | 13.6 (13.4–13.8) | 14.1 (13.9–14.2)‡ | 14.4 (14.2–14.6)*† |
| No. of interviewed coaches | 1028 | 1015 | 1007 |
Significant difference (t-test, p <0.017): * between 2015 and 2004, † between 2015 and 2008, ‡ between 2008 and 2004.
The survey of 2015 referred to 1076 injuries that happened during 3964 amateur soccer games and to 525 injuries that occurred during 8338 training sessions. Additionally, an exposure time of 182,961 training hours was considered for the calculations. As illustrated in figure 1, the number of injuries per 1000 hours of competitive playing significantly decreased from 2004 to 2008 by 11.9%. However, from 2008 to 2015, an increase in injury incidence of 3.2 injuries per 1000 hours was observed during competitive games. The incidence of training injuries increased by 20.8% from 2004 to 2015 and by 31.8% from 2008 to 2015.
Figure 1 Injury incidence in amateur soccer per 1000 hours of playing during the previous 4 weeks (including 95% confidence intervals).
For the incidence of game injuries, the trend to a decrease between the years 2004 and 2008 followed by an increase between the years 2008 and 2015 was observable across all leagues (table 2). On a descriptive level, in each league the incidence of game and training injuries was higher in 2015 than 2004. Nevertheless, differences across time rarely reached statistical significance in the various subgroups.
Table 2 Injury incidence during amateur soccer games and training per 1000 hours of playing during the previous 4 weeks, by league (including 95% confidence intervals).
| 2004 | 2008 | 2015 | |
|---|---|---|---|
| Games | |||
| Male 2nd–3rd amateur league | 16.3 (13.9–18.7) | 14.0 (11.8–16.2) | 17.2 (14.5–19.9) |
| Male 4th–5th amateur league | 17.1 (15.1–19.0) | 16.5 (14.4–18.6) | 19.0 (16.8–21.3) |
| Male 16–20 years | 12.2 (10.4–13.9) | 12.1 (10.5–13.8) | 14.4 (12.4–16.4) |
| Male 14–15 years | 10.1 (8.4–11.7) | 8.5 (7.0–10.1) | 12.5 (10.7–14.3)* |
| Male 30+/40+ league | 22.7 (19.7–25.6) | 18.0 (14.9–21.1)‡ | 24.2 (20.5–27.8)* |
| Female all levels | 13.8 (9.0–18.5) | 11.9 (8.6–15.2) | 14.3 (11.4–17.2) |
| Training | |||
| Male 2nd–3rd amateur league | 2.6 (2.1–3.2) | 2.1 (1.6–2.6) | 2.8 (2.2–3.4) |
| Male 4th–5th amateur league | 2.7 (2.2–3.2) | 3.1 (2.6–3.7) | 3.5 (2.9–4.1) |
| Male 16–20 years | 2.3 (1.8–2.7) | 1.9 (1.5–2.3) | 2.7 (2.2–3.2)* |
| Male 14–15 years | 1.7 (1.3–2.0) | 1.3 (1.0–1.7) | 2.1 (1.7–2.5)* |
| Male 30+/40+ league | 4.9 (3.6–6.3) | 6.0 (4.3–7.7) | 5.0 (3.6–6.4) |
| Female all levels | 1.1 (0.3–2.0) | 1.6 (0.8–2.3) | 2.3 (1.6–3.0) |
Significant difference (95% confidence intervals, p ≤0.05): * between 2015 and 2008, ‡ between 2008 and 2004.
Between the years 2004 and 2015, a considerable increase of 109.1% was observed for training injury incidence among female players. However, this change was not statistically significant owing to a limited number of injuries. With regard to injury incidence during competitive games, a significant increase occurred from 2008 to 2015 for 14- to 15-year-old males (47.1%) and males playing in the 30+/40+ leagues (34.4%), and there was a significant decrease of injury incidence in male 30+/40+ league players from 2004 to 2008. For training injuries, a 42.1% increase was found in young male players (14–15 years), and a 61.5% increase among 16- to 20-year-old male players.
Furthermore, a remarkably high injury incidence was observed during games in male 30+/40+ leagues. Across all three time-points, this group had the highest injury incidence rates, during both competitive games and training.
With regard to injury severity, there were no significant differences in game (table 3) and training (table 4) injury incidence between the years 2004 and 2015. Only the incidence of injuries leading to medical attention significantly increased from 2004 to 2015 (game 20.0%, training 37.5%). However, in 2015, a higher incidence for light (1–7 days lay-off, 40.6%) and severe (>28 days lay-off, 29.2%) game injuries and a higher incidence for moderate (8–28 days lay-off, 33.3%) training injuries, compared with 2008, were found.
Table 3 Injury incidence in amateur soccer games per 1000 hours of playing during the previous 4 weeks, by causes and characteristics (including 95% confidence intervals).
| Games | 2004 | 2008 | 2015 |
|---|---|---|---|
| Time loss§ | |||
| No days | 1.8 (1.5–2.1) | 1.2 (0.9–1.4)‡ | 1.5 (1.2–1.8) |
| 1–7 days | 4.2 (3.7–4.6) | 3.2 (2.8–3.6)‡ | 4.5 (4.0–5.0)† |
| 8–28 days | 5.9 (5.3–6.5) | 5.8 (5.2–6.4) | 6.7 (6.0–7.3) |
| >28 days | 2.6 (2.2–3.0) | 2.4 (2.1–2.8) | 3.1 (2.6–3.5)† |
| Had to stop soccer | 0.1 (0.0–0.2) | 0.1 (0.0–0.2) | 0.1 (0.0–0.2) |
| Medical attention | 6.0 (5.4–6.5) | 5.8 (5.3–6.4) | 7.2 (6.5–7.8)*† |
| Injury situation | |||
| Contact | 4.7 (4.2–5.2) | 4.4 (3.9–4.9) | 5.6 (5.0–6.2)*† |
| Noncontact | 10.3 (9.6–11.1) | 8.6 (7.9–9.3)‡ | 10.7 (9.9–11.5)† |
| Foul play¶ | 3.1 (2.6–3.5) | 2.8 (2.4–3.2) | 3.5 (3.0–4.0)† |
| Body region | |||
| Ankle | 3.5 (3.1–3.9) | 3.6 (3.2–4.1) | 3.9 (3.4–4.4) |
| Thigh | 3.5 (3.1–4.0) | 2.9 (2.5–3.3)‡ | 3.7 (3.3–4.2)† |
| Knee | 2.1 (1.8–2.5) | 1.9 (1.6–2.2) | 2.9 (2.4–3.3)*† |
| Lower leg, Achilles tendon | 1.3 (1.1–1.6) | 1.1 (0.9–1.4) | 1.3 (1.0–1.6) |
| Upper limb | 0.6 (0.4–0.8) | 0.9 (0.7–1.1) | 1.1 (0.9–1.4)* |
| Other, don’t know | 4.0 (3.5–4.5) | 2.8 (2.4–3.2)‡ | 3.5 (3.1–4.0) |
| Injury type | |||
| Strain, muscle rupture, tear | 4.5 (4.0–5.0) | 3.0 (2.6–3.4)‡ | 4.3 (3.8–4.8)† |
| Ligament injury, sprain | 3.2 (2.8–3.6) | 3.4 (3.0–3.8) | 4.1 (3.6–4.6)*† |
| Contusion, hematoma | 4.1 (3.6–4.5) | 3.1 (2.7–3.5)‡ | 3.8 (3.3–4.2)† |
| Bone fracture, bone injury | 0.5 (0.3–0.7) | 0.6 (0.4–0.8) | 0.9 (0.7–1.1)* |
| Other, don’t know | 2.8 (2.4–3.2) | 3.1 (2.7–3.5) | 3.3 (2.9–3.8) |
| No. of injuries | 1049 | 914 | 1076 |
Significant difference (95% confidence intervals, p ≤0.05): * between 2015 and 2004, † between 2015 and 2008, ‡ between 2008 and 2004. § The information is based on the medical diagnosis (provided that the player consulted a physician) and on the assessment of the player and the coach. ¶ Foul play was determined as a combination of the referee’s and the coach’s opinion for game injuries and of the coach’s opinion for training injuries. Foul play is a sub-category of contact injuries.
Table 4 Injury incidence in amateur soccer training per 1000 hours of playing during the previous 4 weeks, by causes and characteristics (including 95% confidence intervals).
| Training | 2004 | 2008 | 2015 |
|---|---|---|---|
| Time loss§ | |||
| No days | 0.3 (0.2–0.3) | 0.2 (0.2–0.3) | 0.3 (0.2–0.3) |
| 1–7 days | 0.7 (0.6–0.9) | 0.6 (0.5–0.8) | 0.8 (0.7–1.0) |
| 8–28 days | 1.0 (0.9–1.2) | 0.9 (0.7–1.0) | 1.2 (1.1–1.4)† |
| >28 days | 0.4 (0.3– 0.5) | 0.4 (0.3–0.4) | 0.4 (0.3–0.5) |
| Had to stop soccer | 0.0 | 0.0 | 0.0 |
| Medical attention | 0.8 (0.7–1.0) | 0.8 (0.7–1.0) | 1.1 (1.0–1.3)*† |
| Injury situation | |||
| Contact | 0.6 (0.4–0.7) | 0.5 (0.4–0.6) | 0.6 (0.5–0.7) |
| Noncontact | 1.8 (1.6–2.0) | 1.7 (1.5–1.9) | 2.2 (2.0–2.4)*† |
| Body region | |||
| Ankle | 0.6 (0.5–0.8) | 0.7 (0.5–0.8) | 0.8 (0.6–0.9) |
| Thigh | 0.6 (0.5–0.7) | 0.5 (0.4–0.7) | 0.6 (0.5–0.7) |
| Knee | 0.3 (0.2–0.4) | 0.3 (0.2–0.4) | 0.4 (0.3–0.5) |
| Lower leg, Achilles tendon | 0.2 (0.1–0.2) | 0.2 (0.1–0.2) | 0.2 (0.1–0.2) |
| Upper limb | 0.2 (0.1–0.2) | 0.1 (0.0–0.1) | 0.2 (0.1–0.3) |
| Other, don’t know | 0.6 (0.5–0.7) | 0.5 (0.4–0.6) | 0.7 (0.6–0.8)† |
| Injury type | |||
| Strain, muscle rupture, tear | 0.7 (0.5–0.8) | 0.7 (0.5–0.8) | 0.7 (0.6–0.8) |
| Ligament injury, sprain | 0.7 (0.6–0.8) | 0.6 (0.5–0.7) | 0.8 (0.7–1.0)† |
| Contusion, hematoma | 0.5 (0.4–0.6) | 0.4 (0.3–0.5) | 0.5 (0.4–0.6) |
| Other, don’t know | 0.6 (0.5–0.7) | 0.5 (0.4–0.7) | 0.8 (0.7–1.0)*† |
| No. of injuries | 417 | 403 | 525 |
Significant difference (95% confidence intervals, p≤0.05): * between 2015 and 2004, † between 2015 and 2008. § The information is based on the medical diagnosis (provided that the player consulted a physician) and on the assessment of the player and the coach. Foul play was determined as a combination of the referee’s and the coach’s opinion for game injuries and of the coach’s opinion for training injuries. Foul play is a sub-category of contact injuries. Even in training, (unintentional) foul play can occur, for example, when duels are practiced or when two teams play against each other.
During competitive games, the incidence of contact injuries increased by 19.1% from 2004 to 2015, whereas the incidence of noncontact injuries and foul play injuries did not vary significantly between these years. The increase of game injury incidence from 2008 to 2015 can be explained by a higher frequency of both contact and noncontact injuries. Between the years 2008 and 2015, the incidence of foul play injuries in games increased by 25.0%. With regard to training injuries, the total increase from 2004 to 2015 was mainly due to a 22.2% higher rate of noncontact injuries.
There were also significant differences across time with respect to injury characteristics. More injuries to the knee (38.1% higher injury incidence), injuries to the upper limb (83.3%), sprains (28.1%) and bone fractures (80.0%) were observed during competitive games in 2015 compared with 2004. The incidence of injuries such as strains and contusions was significantly reduced in 2008. For training injuries, the changes of injury characteristics between the years 2004, 2008 and 2015 were of less relevance.
The aim of the present study was to compare injury incidences in Swiss amateur soccer between the years 2004, 2008 and 2015 with respect to leagues, and injury causes and characteristics. One main finding was that the rate of training injuries increased significantly from 2004 to 2015, whereas the injury rate during competitive games increased significantly from 2008 to 2015. On this basis, it can be concluded that the injury incidence in Swiss amateur soccer has increased in the past years. This finding is in line with a previous study analysing soccer-related injuries of children and adults in the USA [9].
A more detailed analysis of the injury situations showed that the above-mentioned changes in injury incidence may be attributable to various causes. Compared with 2004, the incidence of contact injuries during games in 2015 was higher. Additionally, the incidence of foul play injuries during games increased from 2008 to 2015. These findings suggest that competitive amateur soccer in Switzerland may have become more physical. In contrast, the higher incidence of training injuries in 2015 was mainly due to an increased rate of noncontact injuries. This indicates that the intensity of playing may have increased during amateur soccer training.
The long-term development of injury incidence in the different amateur soccer leagues provides important insights for the improvement of prevention strategies. A comparison of the 2004 and 2015 data points towards a tendency for injury incidence to increase across all leagues. From 2008 to 2015, significant increases were observed among junior (both training and game) [9] and veteran soccer players (only game). Although not statistically significant, the increased injury incidence during female soccer training is worth noting. As Junge and Dvorak [17] concluded, the playing style of women has become more intense in top tournaments. Although speculative, it can be assumed that this trend also pertains to female soccer training, and both to youth and veteran soccer.
In line with previous research [22], remarkably high levels of injury incidences were identified during competitive games and training sessions in male 30+/40+ leagues. Our data support previous research showing that injury risk increases with age [23–25]. As a consequence, male 30+/40+ league players should be a main target group for injury prevention. Although Hammes et al. [5] were unable to find a preventive effect of “FIFA 11+” among veteran soccer players, this might be as result of the low frequency of training sessions. Thus, more concerted efforts are needed to find out how injury prevention can be implemented successfully among older amateur players.
During both games and training, the incidence of medical attention injuries increased significantly between 2004 and 2015. This may be related to the fact that players had a lower threshold for consulting a physician. It might also be an indication that injuries in Swiss amateur soccer have become more severe. The latter assumption is supported by the fact that, on a descriptive level, moderate (time loss of 8–28 days) and severe (time loss of >28 days) game injuries increased between 2004 and 2015. The development of severe injuries sustained during competitive games between 2008 and 2015 is of particular concern. Furthermore, significant differences regarding injury characteristics were in line with the assumption that injury severity may has increased over time. Compared with 2004, injuries to the knee, injuries to the upper limb, sprains and bone fractures were more frequently observed during competitive games in 2015. The changes in injury severity and injury characteristics corroborate the notion that amateur soccer in Switzerland may have become more intensive, including higher speeds and forces, which leads to a higher number of serious falls and severe injuries such as bone fractures.
Possible limitations of the present study design such as memory effects and reporting bias have been discussed previously by Junge et al. [8]. Since these effects were similar across all three years the data should be comparable and changes in injury incidence should be conclusive. However, the generalisability of the calculated injury incidences is limited due to the study design. In general, injury data collected by sports coaches are likely to underestimate injury incidence [26]. Nevertheless, the incidences of game and training injuries were comparable to those reported for amateur players in other studies [1, 2, 4]. Additionally, a game duration of 90 minutes and a number of 11 players was used as a basic assumption when calculating the total exposure time. However, for a few junior teams (male and female 14–15 years), as well as for a few veteran teams, play time was shorter (e.g., 80 minutes) and fewer players are engaged on the field (7 or 9 players). As a consequence, injury incidence may have been underestimated in these leagues. All in all, we assume that these few cases should not have an impact on our data. Furthermore, we acknowledge that our study does not provide real longitudinal data, in which the same individuals are followed-up over time. Rather, changes observed over time are based on potentially different individuals (that is, different coaches who may refer to different players). Finally, as described in the methods section, the coaches were asked to report injuries during games when they were present. With regard to the training sessions the question was formulated in a more general way. That is, coaches were asked about the number of training injuries that had occurred during the previous 4 weeks. Moreover, coaches were invited to provide details about each injury. Since coaches might not have been present at each individual training session, it is plausible that coaches may not be aware of some minor injuries that have occurred during training. Accordingly, it is possible that we underestimated the incidence of minor injury during training sessions in the current study.
During the past years, injury prevention programmes and fair play measures have been successfully implemented in Swiss amateur soccer [8]. Additionally, the international literature supports a positive effect of prevention programmes in youth soccer [27–29], female soccer [30–32] and amateur soccer in general [30, 33, 34]. Nevertheless, the present study shows that, despite these measures, there was an increase of incidence from 2004 to 2015 in contact injuries during games, noncontact injuries during training and medical attention injuries. We therefore suggest that the development, scientific evaluation and implementation of appropriate preventive strategies in amateur soccer need to remain a top priority for policy makers. Furthermore, there is a continued need for studies monitoring the development of injury incidence in amateur soccer across time.
No financial support and no other potential conflict of interest relevant to this article was reported.
1 Hägglund M , Waldén M , Ekstrand J . Injury recurrence is lower at the highest professional football level than at national and amateur levels: does sports medicine and sports physiotherapy deliver? Br J Sports Med. 2016;50(12):751–8. doi:.https://doi.org/10.1136/bjsports-2015-095951
2 Hammes D , Aus Der Fünten K , Kaiser S , Frisen E , Dvorák J , Meyer T . Injuries of veteran football (soccer) players in Germany. Res Sports Med. 2015 a;23(2):215–26. doi:.https://doi.org/10.1080/15438627.2015.1005295
3 Roos KG , Wasserman EB , Dalton SL , Gray A , Djoko A , Dompier TP , et al. Epidemiology of 3825 injuries sustained in six seasons of National Collegiate Athletic Association men’s and women’s soccer (2009/2010-2014/2015). Br J Sports Med. 2017;51(13):1029–34.
4 van Beijsterveldt AM , Stubbe JH , Schmikli SL , van de Port IG , Backx FJ . Differences in injury risk and characteristics between Dutch amateur and professional soccer players. J Sci Med Sport. 2015;18(2):145–9. doi:.https://doi.org/10.1016/j.jsams.2014.02.004
5 Hammes D , Aus der Fünten K , Kaiser S , Frisen E , Bizzini M , Meyer T . Injury prevention in male veteran football players - a randomised controlled trial using "FIFA 11+". J Sports Sci. 2015 b;33(9):873–81. doi:.https://doi.org/10.1080/02640414.2014.975736
6 Sousa P , Rebelo A , Brito J . Injuries in amateur soccer players on artificial turf: a one-season prospective study. Phys Ther Sport. 2013;14(3):146–51. doi:.https://doi.org/10.1016/j.ptsp.2012.05.003
7 van Beijsterveldt AM , Steffen K , Stubbe JH , Frederiks JE , van de Port IG , Backx FJ . Soccer injuries and recovery in Dutch male amateur soccer players: results of a prospective cohort study. Clin J Sport Med. 2014;24(4):337–42. doi:.https://doi.org/10.1097/JSM.0000000000000028
8 Junge A , Lamprecht M , Stamm H , Hasler H , Bizzini M , Tschopp M , et al. Countrywide campaign to prevent soccer injuries in Swiss amateur players. Am J Sports Med. 2011;39(1):57–63. doi:.https://doi.org/10.1177/0363546510377424
9 Esquivel AO , Bruder A , Ratkowiak K , Lemos SE . Soccer-Related Injuries in Children and Adults Aged 5 to 49 Years in US Emergency Departments From 2000 to 2012. Sports Health. 2015;7(4):366–70. doi:.https://doi.org/10.1177/1941738115579854
10 Mufty S , Bollars P , Vanlommel L , Van Crombrugge K , Corten K , Bellemans J . Injuries in male versus female soccer players: epidemiology of a nationwide study. Acta Orthop Belg. 2015;81(2):289–95.
11 Aoki H , O’Hata N , Kohno T , Morikawa T , Seki J . A 15-year prospective epidemiological account of acute traumatic injuries during official professional soccer league matches in Japan. Am J Sports Med. 2012;40(5):1006–14. doi:.https://doi.org/10.1177/0363546512438695
12 Carling C , Orhant E , LeGall F . Match injuries in professional soccer: inter-seasonal variation and effects of competition type, match congestion and positional role. Int J Sports Med. 2010;31(4):271–6. doi:.https://doi.org/10.1055/s-0029-1243646
13 Dauty M , Collon S . Incidence of injuries in French professional soccer players. Int J Sports Med. 2011;32(12):965–9. doi:.https://doi.org/10.1055/s-0031-1283188
14 Ekstrand J , Hägglund M , Waldén M . Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med. 2011;45(7):553–8. doi:.https://doi.org/10.1136/bjsm.2009.060582
15 Hägglund M , Waldén M , Ekstrand J . Exposure and injury risk in Swedish elite football: a comparison between seasons 1982 and 2001. Scand J Med Sci Sports. 2003;13(6):364–70. doi:.https://doi.org/10.1046/j.1600-0838.2003.00327.x
16 Mohib M , Moser N , Kim R , Thillai M , Gringmuth R . A four year prospective study of injuries in elite Ontario youth provincial and national soccer players during training and matchplay. J Can Chiropr Assoc. 2014;58(4):369–76.
17 Junge A , Dvorak J . Injury surveillance in the World Football Tournaments 1998-2012. Br J Sports Med. 2013;47(12):782–8. doi:.https://doi.org/10.1136/bjsports-2013-092205
18Beratungsstelle für Unfallverhütung (bfu) [Swiss Competence Centre for Accident Prevention]. STATUS 2017: Statistik der Nichtberufsunfälle und des Sicherheitsniveaus in der Schweiz, Strassenverkehr, Sport, Haus und Freizeit. Available at: https://www.bfu.ch/de/forschung-und-statistik/statistik
19 Fuller CW , Ekstrand J , Junge A , Andersen TE , Bahr R , Dvorak J , et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med. 2006;40(3):193–201. doi:.https://doi.org/10.1136/bjsm.2005.025270
20Field A. Discovering Statistics Using IBM SPSS Statistics. Fourth edition. London: SAGE Publications Ltd; 2013. p. 27.
21 Knowles SB , Marshall SW , Guskiewicz KM . Issues in estimating risks and rates in sports injury research. J Athl Train. 2006;41(2):207–15.
22 Herrero H , Salinero JJ , Del Coso J . Injuries among Spanish male amateur soccer players: a retrospective population study. Am J Sports Med. 2014;42(1):78–85. doi:.https://doi.org/10.1177/0363546513507767
23 Arnason A , Sigurdsson SB , Gudmundsson A , Holme I , Engebretsen L , Bahr R . Risk factors for injuries in football. Am J Sports Med. 2004;32(1, Suppl):5–16. doi:.https://doi.org/10.1177/0363546503258912
24 Dvorak J , Junge A . Football injuries and physical symptoms. A review of the literature. Am J Sports Med. 2000;28(5, Suppl):3–9. doi:.https://doi.org/10.1177/28.suppl_5.s-3
25 Fuller CW , Junge A , Dvorak J . Risk management: FIFA’s approach for protecting the health of football players. Br J Sports Med. 2012;46(1):11–7. doi:.https://doi.org/10.1136/bjsports-2011-090634
26 Ekegren CL , Gabbe BJ , Finch CF . Injury surveillance in community sport: Can we obtain valid data from sports trainers? Scand J Med Sci Sports. 2015;25(3):315–22. doi:.https://doi.org/10.1111/sms.12216
27 Emery CA , Meeuwisse WH . The effectiveness of a neuromuscular prevention strategy to reduce injuries in youth soccer: a cluster-randomised controlled trial. Br J Sports Med. 2010;44(8):555–62. doi:.https://doi.org/10.1136/bjsm.2010.074377
28 Junge A , Rösch D , Peterson L , Graf-Baumann T , Dvorak J . Prevention of soccer injuries: a prospective intervention study in youth amateur players. Am J Sports Med. 2002;30(5):652–9. doi:.https://doi.org/10.1177/03635465020300050401
29 Rössler R , Donath L , Verhagen E , Junge A , Schweizer T , Faude O . Exercise-based injury prevention in child and adolescent sport: a systematic review and meta-analysis. Sports Med. 2014;44(12):1733–48. doi:.https://doi.org/10.1007/s40279-014-0234-2
30 Barengo NC , Meneses-Echávez JF , Ramírez-Vélez R , Cohen DD , Tovar G , Bautista JE . The impact of the FIFA 11+ training program on injury prevention in football players: a systematic review. Int J Environ Res Public Health. 2014;11(11):11986–2000. doi:.https://doi.org/10.3390/ijerph111111986
31 Soligard T , Myklebust G , Steffen K , Holme I , Silvers H , Bizzini M , et al. Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. BMJ. 2008;337(dec09 2):a2469. doi:.https://doi.org/10.1136/bmj.a2469
32 Steffen K , Emery CA , Romiti M , Kang J , Bizzini M , Dvorak J , et al. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: a cluster randomised trial. Br J Sports Med. 2013;47(12):794–802. doi:.https://doi.org/10.1136/bjsports-2012-091886
33 Thorborg K , Krommes KK , Esteve E , Clausen MB , Bartels EM , Rathleff MS . Effect of specific exercise-based football injury prevention programmes on the overall injury rate in football: a systematic review and meta-analysis of the FIFA 11 and 11+ programmes. Br J Sports Med. 2017;51(7):562–71. doi:.https://doi.org/10.1136/bjsports-2016-097066
34 Al Attar WSA , Soomro N , Pappas E , Sinclair PJ , Sanders RH . Adding a post-training FIFA 11+ exercise program to the pre-training FIFA 11+ injury prevention program reduces injury rates among male amateur soccer players: a cluster-randomised trial. J Physiother. 2017;63(4):235–42. doi:.https://doi.org/10.1016/j.jphys.2017.08.004
No financial support and no other potential conflict of interest relevant to this article was reported.