
Figure 1 Classification of caregiving groups.
DOI: https://doi.org/10.4414/smw.2017.14552
Burnout is a stress-induced illness and can be described as a psychological syndrome comprising physical and psychological fatigue as well as exhaustion [1]. It often occurs in human service professionals including physicians, psychiatrists, nurses, teachers as well as social workers [2] and results in adverse individual health outcomes such as psychosomatic disorders as well as negative work-related attitudes such as job dissatisfaction, poor performance, absenteeism and turnover [3]. Predictors of burnout are adverse and emotionally demanding working environments [1] as well as long-lasting work stressors [4]. Burnout may not only emerge from work-specific stressors but also from inter-role conflicts between work and private life [5, 6]. Stress resulting from these competing demands between work and private life may carry over from work to private life or in the opposite direction – from private life to work. This work-privacy conflict is considered as an indicator of general psychological stress. As burnout is conceptually the result of adverse working conditions [4], work-specific stressors can theoretically be expected to be more strongly associated with burnout than work-privacy conflict. Despite this theoretical reasoning, the work-privacy conflict was found to be a stronger predictor in a study directly comparing the effect of a work-specific stressor and work-privacy conflict on burnout [6].
Population ageing has led to an increase in the demand for healthcare services and consequently for healthcare professionals. These “formal” caregivers are exposed to many occupational stressors [7] that result in stress and subsequently burnout [8]. Healthcare professionals are among the professions that are especially vulnerable to burnout [9], with burnout rates varying between healthcare occupations [6, 9–11]. Studies have repeatedly shown high rates of burnout in nurses [12, 13] and physicians [14, 15] with a higher proportion of persons at increased burnout risk among physicians than among other hospital staff [6]. However most studies on burnout in healthcare settings focus on single occupational groups and neglect to directly compare different healthcare professions. A U.S. study reported that more than 50% of physicians show symptoms of professional burnout and estimated an increase in the prevalence of physician burnout of 10% from 2011 to 2014 [9]. Burnout in healthcare settings is not only a threat to patients' safety [16] but diminishes the quality of care [9] and the continuity of care due to high turnover [17].
Not only has the demand for formal professional healthcare risen, but so has the need for informal caregiving [8] especially in view of a possibly under-resourced healthcare system in Switzerland in the future [18]. Informal caregivers provide voluntarily unpaid care in their leisure time. Similarly to formal caregivers, informal caregivers are confronted with various physical and mental health problems [19, 20]. They have higher stress hormone levels [21], perceive more stress [22], and report lower psychological wellbeing [23] than non-caregivers. While the link between informal caregiving and stress is well documented, evidence for the association between informal caregiving and burnout is less investigated.
Health professionals providing informal care are called double-duty caregivers. We may distinguish between double-duty caregivers providing informal care to dependent children (double-duty child caregivers) or to parents, older relatives or other dependent adults (double-duty adult caregivers) and those who are sandwiched between informal caregiving roles and their formal caregiving role (triple-duty caregivers) (fig. 1). Although increasingly prevalent [19, 20, 24, 25], double- and triple-duty caregivers remain an understudied workforce population [20]. Whereas double- and triple-duty caregivers are associated with negative health outcomes [19, 24] and more work-family conflict than non-caregivers [19, 20, 26, 27], evidence for a link between double- and triple-duty caregivers and burnout is scarce. However, the link between emotional exhaustion, which is a component of burnout, has been documented for double-duty caregivers in the Netherlands [19, 26] and double- and triple-duty caregivers in the U.S [27–29]. Studies assessing burnout risk of double- and triple-duty caregivers neglect to differentiate between healthcare professions, despite differences in burnout risk [6, 9–11]. Moreover, to our knowledge studies considering work-privacy conflict as a mediator in the relationship between caregiving situation and burnout are currently lacking.
Figure 1 Classification of caregiving groups.
Role theory provides two opposing hypotheses as to how caregiving can affect burnout through stress: role strain and role enhancement. The role strain hypothesis postulates negative effects for informal caregivers as such additional roles compete for a finite set of resources and hence lead to role overload and/or time scarcity [30]. According to the role strain hypothesis, double-duty caregivers have higher and triple-duty caregivers the highest stress levels and hence burnout risk compared to formal caregivers only. Conversely, the role enhancement suggests positive effects of additional roles (such as informal caregiving) due to status security and enhancement, role privileges and personality enrichment [31]. According to the role enhancement hypothesis, double- and triple-duty caregivers are expected to have a comparable or even lower risk of burnout than formal caregivers only.
In view of the relatively high burnout rate of healthcare professionals [3] and the higher susceptibility to medical errors of “burnt out” healthcare professionals [32], it is crucial to disentangle the mechanisms behind formal and informal caregiving roles and burnout. While the associations between formal caregiving [3] and to some extent informal caregiving and burnout [19, 26–29] have been established, we aim to investigate the effect of informal caregiving roles on burnout in the hospital setting and to assess whether work-privacy conflict mediates this relationship in different health professions (fig. 2).
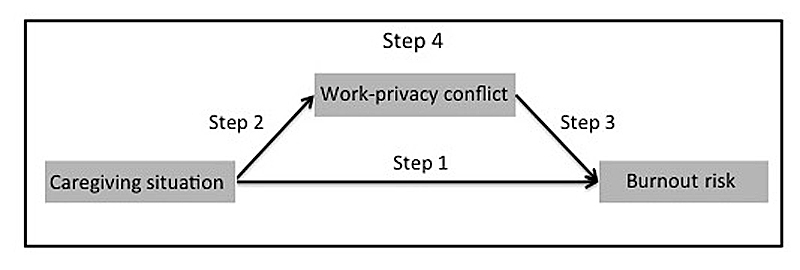
Figure 2 Analytical framework to investigate the effect of caregiving of burnout risk: four-step mediation analyses.
Hence we aimed to answer the following research questions:
Data stemmed from an anonymous employee survey on working conditions and health of hospital employees in German-speaking Switzerland (n = 1406). The questionnaire contained 100 questions concerning working conditions, satisfaction and wellbeing at work, personal resources, multiple roles, health and general wellbeing (see appendix 1). It was sent to all permanent employees of the six hospitals including a university hospital, a cantonal hospital, two district hospitals and two rehabilitation clinics. Hospitals varied not only regarding size ranging from 473 to 2182 permanent employees, but also regarding the degree of specialisation and urbanisation of catchment area. The employees had four weeks to return the questionnaire with the enclosed postage-paid envelope to the University of Zurich. A reminder was sent to all employees three weeks after initial distribution.
Burnout risk was assessed with the validated German version of the personal burnout scale [33] from the Copenhagen Burnout Inventory (CBI) [1]. This scale contained six questions (e.g., “How often are you physically exhausted?”) concerning the prolonged physical and psychological fatigue with five answer categories ranging from “always” (100), “often” (75), “sometimes” (50), “seldom” (25) to “never/almost never” (0). The sum score of the items was divided by the number of items answered whereas at least three items had to be answered in order to be included in the analyses. Hence a burnout score of 50 and above indicated having an increased risk or developing burnout. In the original Danish validation study of the CBI, the average burnout score was 33 [34] whereas the reference score of the German validation study was 42 [35].
We categorised the study population into four caregiving groups depending on the additional informal caregiving roles (see fig 1). Questions about informal caregiving roles stemmed from the national module of unpaid work, which is included every third year in the Swiss Labour Force Survey (SAKE). Our reference group of formal caregivers was defined by having no informal caregiving role for dependent children or adults. Participants who reported living with at least one minor (i.e., under 18 years old) in the same household were classified as double-duty child caregivers (DDCC). Individuals reporting to provide informal care to a related adult or another adult living outside of the household or living in the same household with an adult person in need of care were categorised as double-duty adult caregivers (DDAC). Study participants facing both of these informal caregiving roles i.e., living in a household with at least one underage child and providing informal adult care, were classified as triple-duty caregivers (TDC).
Due to small numbers of cases, the following professional categories were formed: nursing professionals (including midwives), medical doctors and other health professionals (including medical-therapeutic experts, medical-technical experts, academic staff).
For work-privacy conflict, we used the work-privacy conflict scale (WPC) from the German version of the Copenhagen Psychosocial Questionnaire (COPSOQ) [33], which is an adapted version of the work-family conflict scale [36] measuring inter-role conflict between private life and work. Despite this bidirectional concept, the WPC scale measures solely the conflict between work and private life, and not the other direction. It consists of five items (e.g., “The demands of my work interfere with my private and family life,” with answer categories ranging from “I totally agree” (100), “I agree” (75), “neither agree nor disagree” (50), “I disagree” (25), to “I totally disagree” (0). The sum score of all items was divided by the number of items answered. At least three items had to be answered in order for the value to be considered. The higher the score on WPC, the greater the conflict between work and private life.
We used descriptive statistics to characterise the study population according to burnout risk. We assessed the effect of the caregiving situation on burnout risk and tested WPC as a potential mediator in this association by using a four-step mediation analyses [37] (see fig. 2). According to Baron and Kenny [37], mediation will take place if the following conditions are fulfilled: the independent variable had a significant effect on the dependent variable (step 1) and on the mediator (step 2), the mediator had a significant effect on the dependent variable (step 3) and the effect of the independent variable on the dependent variable diminished when the mediator was included in the analysis (step 4). Hence, in step 1 we estimated the effect of the caregiving situation on burnout risk. In a second step (step 2), we investigated the effect of the caregiving situation on WPC as the dependent variable. This step was necessary to test whether the initial variable caregiving situation was associated with the potential mediator. Next, we analysed the effect of the potential mediator WPC on burnout risk (step 3). In step 4, we included WPC in the initial analyses that assessed the effect of the caregiving situation on burnout risk. In all steps, we controlled for age, sex, marital status, education and work volume. We performed linear mixed regression models with fixed effects for caregiving groups and random effects for hospitals to allow for clustering of results within each hospital. For our third research question, we performed linear mixed regression models stratified for professional group with the same four-step approach to test for mediation [37]. Akaike’s Information Criterion indicated a better model fit for linear mixed models compared to linear regression as well as best model fit for step 4.
In total, 1844 questionnaires were returned (41%). In order to have a study population of formal caregivers, we restricted the study to health professionals (n = 1441) with complete information on all variables of interest (n = 1406), resulting in a study population of 1232 women (88%) and 174 men (12%) (table 1). Most participants were nurses (61%), followed by other health professionals (23%) and medical doctors (16%). The majority of the participants were formal caregivers only (60%), DDCCs (32%) were the second largest caregiving group followed by DDACs (6%) and TDCs (2%). The average burnout risk score was 40.3 in females and 37.4 in males. With the exception of male DDACs (only 4 participants), all caregiving groups had a mean burnout score below the cut-off point at score 50 for an increased burnout risk. No clear burnout risk pattern for the caregiving groups was found. Whereas female TDCs had a higher unadjusted mean burnout score compared to formal caregivers only, the unadjusted means for female DDCCs and DDACs were lower compared to the formal caregivers only. In the male study population DDACs had a higher mean burnout score compared to the formal caregivers only (but based on only four participants and statistically not significant), whereas DDCCs had a comparable burnout risk score to the formal caregivers only.
Table 1 Average burnout risk score for women and men, unadjusted.
| Women | Men | |||||
|---|---|---|---|---|---|---|
| N | Burnout risk (0–100) | N | Burnout risk (0–100) | |||
| Total study population | 1232 | 40.2 | (39.3–41.2) | 174 | 37.4 | (34.5–40.3) |
| Age | ||||||
| Under 25 | 82 | 45.5 | (42.3–48.7) | 4 | 40.6 | (18.7–62.5) |
| 25–34 | 386 | 41.7 | (40.1–43.3) | 39 | 38.2 | (31.7–44.8) |
| 35–44 | 313 | 42.0 | (40.2–43.8) | 46 | 40.1 | (34.2–45.9) |
| 45–54 | 288 | 37.5 | (35.6–39.3) | 58 | 34.6 | (29.8–39.5) |
| 55+ | 163 | 35.8 | (33.3–38.5) | 27 | 34.9 | (27.7–42.1) |
| Marital status | ||||||
| Married | 592 | 38.5 | (37.1–39.7) | 102 | 35.6 | (31.8–39.4) |
| Single | 518 | 42.8 | (41.4–44.2) | 58 | 40.1 | (35.1–45.0) |
| Divorced/widowed | 122 | 37.6 | (34.7–40.5) | 14 | 35.2 | (25.6–44.7) |
| Education | ||||||
| Primary | 31 | 39.7 | (32.8–46.5) | 1 | 20.8 | – |
| Secondary | 385 | 38.9 | (37.2–40.5) | 22 | 33.5 | (24.9–42.2) |
| Tertiary | 816 | 40.9 | (39.8–41.9) | 151 | 37.7 | (34.6–40.7) |
| Work volume | ||||||
| 100% | 376 | 43.0 | (41.3–44.6) | 122 | 36.0 | (32.6–39.5) |
| 80–99% | 323 | 39.6 | (37.9–41.3) | 36 | 39.4 | (33.4–45.3) |
| 50–79% | 328 | 39.0 | (37.1–41.8) | 13 | 40.4 | (26.4–54.3) |
| 30–49% | 166 | 39.4 | (36.9–41.8) | 1 | 33.3 | – |
| under 30% | 39 | 32.4 | (27.7–37.1) | 2 | 39.6 | – |
| Professional category | ||||||
| Nursing professionals | 807 | 39.6 | (38.5–40.7) | 47 | 35.4 | (29.2–38.5) |
| Medical doctors | 148 | 42.9 | (40.4–45.5) | 83 | 38.7 | (34.5–42.9) |
| Other health professionals | 277 | 40.6 | (38.6–42.6) | 44 | 37.4 | (30.9–43.9) |
| Caregiving group | ||||||
| Formal caregiver | 747 | 40.4 | (39.2–41.6) | 102 | 36.2 | (32.6–39.8) |
| Double–duty child caregiver | 379 | 39.9 | (38.3–41.5) | 66 | 37.4 | (32.6–42.2) |
| Double–duty adult caregiver | 78 | 36.9 | (33.9–39.9) | 4 | 52.1 | (4.7–99.4) |
| Triple duty caregiver | 28 | 46.6 | (40.1–51.2) | 2 | 39.6 | – |
| Work Privacy Conflict score | ||||||
| Lowest quartile | 353 | 30.1 | (28.6–31.5) | 47 | 25.5 | 21.6–29.3 |
| Second lowest quartile | 356 | 38.8 | (37.3–40.2) | 44 | 31.0 | 25.8–36.1 |
| Second highest quartile | 228 | 43.6 | (41.8–45.4) | 42 | 42.0 | 38.0–48.3 |
| Highest quartile | 295 | 51.4 | (49.7–53.2) | 41 | 51.9 | 46.9–59.7 |
We found a steep and consistent gradient for the association between WPC score and burnout risk score in both sexes that reflected the relatively low unadjusted mean burnout score for the lowest WPC quartiles and the elevated mean burnout score for the highest WPC quartile.
Whereas the burnout risk score (ranging from 0–100) for DDCCs and DDACs did not significantly differ from the formal caregivers only, TDCs had a higher mean burnout score compared to the formal caregivers only (tables 1 and 2 ). In a multivariate linear mixed regression analysis (table 2), TDCs had an 8.39 (CI 2-29–14.49) higher mean burnout score than formal caregivers only (step 1).
Table 2 Burnout risk for caregiving groups: four-step mediation analyses*.
| N | Step 1 | Step 2 (WPC) | Step 3 | Step 4 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Coef. | CI (95%) | Coef. | CI (95%) | Coef. | CI (95%) | Coef. | CI (95%) | ||
| Caregiving group | |||||||||
| Formal caregivers† | 849 | 0 | 0 | 0 | |||||
| DDCC | 445 | 0.65 | −1.78–3.08 | 3.65 | 0.10–7.19 | −0.69 | −2.76–1.39 | ||
| DDAC | 82 | −0.17 | −3.90–3.56 | 4.58 | −0.85–10.02 | −1.82 | −5.001–1.36 | ||
| TDC | 30 | 8.39 | 2.29–14.49 | 6.53 | −2.36–15.42 | 5.98 | 0.78–11.19 | ||
| Work-Privacy Conflict score (0–100) | 1406 | 0.36 | 0.33–0.39 | 0.36 | 0.33–0.39 | ||||
CI = confidence interval; Coef. = coefficient; DDAC = double-duty adult caregivers; DDCC = double-duty child caregivers; TDC = triple-duty caregivers * Adjusted for age, sex, marital status, education and work volume † Without informal caregiving roles
Only DDCCs had a significantly higher WPC score compared to the formal caregivers only (step 2 in table 2). The regression of WPC on burnout risk (step 3) revealed a significant positive association: with every unit increase on the WPC scale ranging from 0–100, the mean burnout score increased by 0.36 (CI 0.33–0.39). Although the inclusion of WPC in step 4 lowered the coefficient of TDCs, TDCs still had a significantly higher mean burnout score 5.98 (CI 0.78–11.19) compared to the formal caregivers only, and WPC was a predictor for burnout score.
Whereas nurse DDCCs and DDACs did not significantly differ in their burnout score from the formal caregivers only, TDCs had a significantly higher mean burnout score of 7.5 (CI 0.45–14.57) compared to formal caregivers only (step 1 in table 3). DDCCs, DDACs and TDCs did not differ significantly in their WPC from formal caregivers only (step 2). WPC was a predictor for nursing professionals’ burnout score (step 3). The adjustment for WPC in step 4 suggested that nurse TDCs had a higher mean burnout score of 6.9 (CI 0.90–12.90) compared to formal caregivers only, with WPC also playing a significant role.
Table 3 Burnout risk for caregiving groups of nursing professionals: four-step mediation analyses*.
| N | Step 1 | Step 2 (WPC) | Step 3 | Step 4 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Coef. | CI (95%) | Coef. | CI (95%) | Coef. | CI (95%) | Coef. | CI (95%) | ||
| Caregiving group | |||||||||
| Formal caregivers† | 512 | 0 | 0 | 0 | |||||
| DDCC | 269 | −0.26 | −3.25–2.73 | 0.43 | −3.85–4.71 | −0.41 | −2.95–2.13 | ||
| DDAC | 52 | −2.42 | −6.94–2.09 | 2.77 | −3.70–9.24 | −3.47 | −7.31–0. 7 | ||
| TDC | 21 | 7.51 | 0.45–14.57 | 1.39 | −8.72–11.51 | 6.90 | 0.90–12.90 | ||
| Work-Privacy Conflict score (0–100) | 854 | 0.37 | 0.33–0.41 | 0.37 | 0.33–0.41 | ||||
CI = confidence interval; Coef. = coefficient; DDAC = double-duty adult caregivers; DDCC = double-duty child caregivers; TDC = triple-duty caregivers * Adjusted for age, sex, marital status, education and work volume † Without informal caregiving roles
The caregiving situation did not have an effect on burnout score nor on WPC (step 1 and 2 in table 4). WPC significantly predicted medical doctors’ burnout score (step 3). The caregiving groups did not differ in their burnout score when additionally adjusted for WPC (step 4). However WPC had a significant effect on the burnout score of medical doctors.
Table 4 Burnout risk for caregiving groups of medical doctors: four-step mediation analyses*.
| N | Step 1 | Step 2 (WPC) | Step 3 | Step 4 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Coef. | CI (95%) | Coef. | CI (95%) | Coef. | CI (95%) | Coef. | CI (95%) | ||
| Caregiving group | |||||||||
| Formal caregivers† | 138 | 0 | 0 | 0 | |||||
| DDCC | 79 | −1.22 | −7.85–5.57 | 5.07 | −3.53–13.67 | −3.63 | −8.58–1.32 | ||
| DDAC | 9 | 1.00 | −11.43–11.56 | 6.63 | −9.01–21.72 | −2.02 | −10.86–6.83 | ||
| TDC | 5 | 1.42 | −14.02–18.57 | −0.43 | −21.85–20.99 | 1.63 | −10.68–13.94 | ||
| Work-Privacy Conflict score (0–100) | 231 | 0.47 | 0.40–0.54 | 0.48 | 0.40–0.55 | ||||
CI = confidence interval; Coef. = coefficient; DDAC = double-duty adult caregivers; DDCC = double-duty child caregivers; TDC = triple-duty caregivers * Adjusted for age, sex, marital status, education and work volume † Without informal caregiving roles
TDCs had a significantly higher mean burnout score (coef. 21.55, CI 4.28–38.82) compared to formal caregivers only (step 1 in table 5). The caregiving situation did not predict WPC in other health professionals (step 2) with the exception of TDCs. TDCs had a significantly higher WPC compared to formal caregivers only (coef. 23.68, CI 0.30–47.06). WPC predicted burnout score in other health professionals (step 3). The inclusion of WPC lowered the regression coefficient of TDCs burnout risk (coef. 12.86, CI -2.01–27.83) and their burnout score was not significantly higher compared to the formal caregivers only (step 4). WPC was a predictor for burnout score in other health professionals.
Table 5 Burnout risk for caregiving groups of other health professionals: four-step mediation analyses*.
| N | Step 1 | Step 2 (WPC) | Step 3 | Step 4 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Coef. | CI (95%) | Coef. | CI (95%) | Coef. | CI (95%) | Coef. | CI (95%) | ||
| Caregiving group | |||||||||
| Formal caregivers† | 199 | 0 | 0 | 0 | |||||
| DDCC | 97 | 3.30 | −2.13–8.72 | 5.49 | −1.84–12.81 | 1.36 | −3.34–6.06 | ||
| DDAC | 21 | 6.49 | −1.42–14.41 | 10.24 | −0.45–20.94 | 2.71 | −4.17–9.58 | ||
| TDC | 4 | 21.55 | 4.28–38.82 | 23.68 | 0.30–47.06 | 12.86 | −2.01–27.83 | ||
| Work-Privacy Conflict score (0–100) | 321 | 0.38 | 0.31–0.45 | 0.37 | 0.30–0.44 | ||||
CI = confidence interval; Coef. = coefficient; DDAC = double-duty adult caregivers; DDCC = double-duty child caregivers; TDC = triple-duty caregivers * Adjusted for age, sex, marital status, education and work volume † Without informal caregiving roles
We found that, among health professionals, informal adult caregiving in combination with being a parent (TCDs) had a negative impact on burnout risk. WPC only mediated the relationship between TDCs and burnout risk in “other health professionals”.
The results of the analyses regarding our first research question showed that not all informal caregiving roles were associated with an elevated burnout risk compared to formal caregivers only. In contrast to other studies [19, 26], we did not find an elevated burnout risk for DDACs compared to formal caregivers only. There was evidence for TDCs having an increased risk of burnout compared to the formal caregivers only. This association has been found previously for TDCs and emotional exhaustion, which is a component of burnout [27–29]. Role strain resulting from informal and formal caregiving roles is expected due to energy scarcity [27]. However, as no dose-response relationship was found, the role strain hypothesis cannot explain why only TDCs revealed a higher burnout risk compared to the formal caregivers only. As DDCCs and DDACs did not have an increased burnout risk compared to formal caregivers only, we assumed that there may be a threshold for when additional caregiving roles cause role strain. Moreover, TDCs were found to struggle to manage professional and informal caregiving role boundaries [24]. Further risk factors for physical and mental health are the time demands of the multiple roles and the inability to separate work and life domains [25].
As regards our second research question, namely whether the effect of informal caregiving on burnout risk was mediated by WPC, we found evidence that WPC did not mediate this relationship. As only TDCs reveal an elevated burnout risk compared to formal caregivers only, we focused on the mediation in this significant relationship between TDCs and burnout. WPC did not mediate the relationship between TDCs and burnout risk because TDCs did not have a significantly higher WPC compared to formal caregivers only, which is a mandatory condition for mediation. However, the inclusion of WPC in step 4 lowered their burnout risk but TDCs had a higher burnout risk compared to the formal caregivers only. Nevertheless, work-related stress measured as WPC failed to explain the elevated burnout risk of TDCs. Therefore the triple caregiving situation itself or work-specific stressors as well as other factors such as time constraints [25], perceived schedule control [27], partner support or family-to-work conflict [29, 38] may be important in this relationship. As WPC lowered the burnout risk in TDCs, employer-based programs such as flexible working arrangements could help employees cope with their emotionally demanding caregiving situation [25]. Further interventions to facilitate the combination of work, caregiving duties and social activities, such as an adult day care service for adults in need of care, has been proven to reduce informal caregivers’ stress and increase wellbeing [39].
Further, as regards our third research question, our results suggest that the effect of WPC as a mediator in the relationship between caregiving situation and burnout risk differs between medical doctors, nursing professionals and other health professionals. The stratified analyses for medical doctors revealed no significant difference in burnout risk between the caregiving groups. TDCs working as other health professionals and nursing professionals showed a significantly higher burnout risk compared to formal caregivers only. WPC mediated this relationship in other health professionals, as all mandatory conditions for mediation were fulfilled. Hence stress resulting from the inter-role conflict between work and private life explained the higher burnout risk of TDCs among other health professionals. On the contrary, WPC did not mediate the same relationship in nursing professionals because TDCs working as nurses do not have a higher WPC score compared to formal caregivers only. Hence, WPC failed to explain the effect of the caregiving situation on burnout risk among nurses. Our findings were not in line with a previous study finding stronger associations between WPC and burnout in nurses, technical care and emergency staff, whereas work-related stressors are more strongly associated with burnout in medical doctors, therapists and medical-technical staff [6]. In contrast to this study, we found that WPC was more strongly associated with burnout in medical doctors than in nursing professionals.
To our knowledge this is the first study to assess the influence of the combination of formal and informal caregiving roles on burnout risk for different professional groups in the healthcare setting. Also, we considered WPC as a mediator in the relationship between caregiving situation and burnout risk. This study is innovative because it investigates an emerging topic in a study population with an elevated burnout risk.
There were several limitations of this study. Although we considered the caregiving situation as well as the stressor WPC as predictors for burnout risk, our data is cross-sectional and hence does not allow causal inferences. Despite the bidirectional concept of inter-role conflicts between work and private life, WPC only measures the conflict between work and private life. Further, the response rate of 41% may have resulted in selection bias. Due to the small number of participants in some caregiving groups, the confidence intervals were large. Moreover, the low number of some professional groups required the merging of some categories, despite different working conditions. Further, our categorisation of the caregiving situation was based on roles and not controlled for intensity or duration. As the questions to categorise our study population into caregiving groups stemmed from the national module on unpaid work from the Swiss Labour Force Survey, the double- and triple-duty caregiving measure does not fully correspond to other measures used for DDCCs, DDACs and TDCs in international studies. This reduces the comparability with previous studies in this field.
Considering the high burnout rate among health professionals and informal caregivers and the evidence of its adverse effects on hospitals' performance, quality of care, patient safety, satisfaction and turnover rate [9, 24], these results have major implications not only for healthcare professionals’ wellbeing but also for patients and society at large. Larger-scale studies focusing on the combination of informal caregiving roles among health professionals are required to better understand these mechanisms. Moreover, a commonly agreed, valid and reliable measure of informal caregiving is crucial to increase the comparability of studies.
The questionnaire is available as a separate file for downloading at https://smw.ch/en/article/doi/smw.2017.14552/
This study was funded by Swiss National Accident Insurance Fund (SUVA), Federal Office of Public Health (FOPH), State Secretariat for Economic Affairs (SECO).
We declare no conflict of interest as the funding sources were not involved in conceiving this study, analysing data, interpreting results or drafting of the manuscript.
1 Kristensen TS , Hannerz H , Høgh A , Borg V . The Copenhagen Psychosocial Questionnaire--a tool for the assessment and improvement of the psychosocial work environment. Scand J Work Environ Health. 2005;31(6):438–49. doi:.https://doi.org/10.5271/sjweh.948
2Bakker AB, Schaufeli WB, Van Dierendonck D. Burnout: prevalentie, risicogroepen en risicofactoren (Burnout: Prevalence, groups at risk and risk factors). In: Houtman IL, Schaufeli WB, Taris T, editors. Psychische vermoeidheid en werk. The Netherlands: Samsom; 2000. p. 65–82.
3Schaufeli WB. Burnout in health care. In: Handbook of human factors and ergonomics in health care and patient safety. 2007. p. 217–32.
4 Maslach C , Leiter MP . Early predictors of job burnout and engagement. J Appl Psychol. 2008;93(3):498–512. doi:.https://doi.org/10.1037/0021-9010.93.3.498
5 Kozak A , Kersten M , Schillmöller Z , Nienhaus A . Psychosocial work-related predictors and consequences of personal burnout among staff working with people with intellectual disabilities. Res Dev Disabil. 2013;34(1):102–15. doi:.https://doi.org/10.1016/j.ridd.2012.07.021
6 Hämmig O , Brauchli R , Bauer GF . Effort-reward and work-life imbalance, general stress and burnout among employees of a large public hospital in Switzerland. Swiss Med Wkly. 2012;142:w13577.
7 McVicar A . Workplace stress in nursing: a literature review. J Adv Nurs. 2003;44(6):633–42. doi:.https://doi.org/10.1046/j.0309-2402.2003.02853.x
8Reinhard SC, Feinberg LF, Choula R, Houser A. Valuing the Invaluable: 2015 Update: Undeniable Progress, but Big Gaps Remain [Internet]. AARP Public Policy Institute. Washington DC; 2015. Available from: http://www.aarp.org/content/dam/aarp/ppi/2015/valuing-the-invaluable-2015-update-new.pdf
9 Shanafelt TD , Hasan O , Dyrbye LN , Sinsky C , Satele D , Sloan J , et al. Changes in Burnout and Satisfaction With Work-Life Balance in Physicians and the General US Working Population Between 2011 and 2014. Mayo Clin Proc. 2015;90(12):1600–13. doi:.https://doi.org/10.1016/j.mayocp.2015.08.023
10 Bennett S , Plint A , Clifford TJ . Burnout, psychological morbidity, job satisfaction, and stress: a survey of Canadian hospital based child protection professionals. Arch Dis Child. 2005;90(11):1112–6. doi:.https://doi.org/10.1136/adc.2003.048462
11 Ramirez AJ , Graham J , Richards MA , Gregory WM , Cull A . Mental health of hospital consultants: the effects of stress and satisfaction at work. Lancet. 1996;347(9003):724–8. doi:.https://doi.org/10.1016/S0140-6736(96)90077-X
12 Aiken LH , Sermeus W , Van den Heede K , Sloane DM , Busse R , McKee M , et al. Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ. 2012;344(mar20-2):e1717. doi:.https://doi.org/10.1136/bmj.e1717
13 Bakker AB , Killmer CH , Siegrist J , Schaufeli WB . Effort-reward imbalance and burnout among nurses. J Adv Nurs. 2000;31(4):884–91. doi:.https://doi.org/10.1046/j.1365-2648.2000.01361.x
14 Arigoni F , Bovier PA , Mermillod B , Waltz P , Sappino AP . Prevalence of burnout among Swiss cancer clinicians, paediatricians and general practitioners: who are most at risk? Support Care Cancer. 2009;17(1):75–81. doi:.https://doi.org/10.1007/s00520-008-0465-6
15 Goehring C , Bouvier Gallacchi M , Künzi B , Bovier P . Psychosocial and professional characteristics of burnout in Swiss primary care practitioners: a cross-sectional survey. Swiss Med Wkly. 2005;135(7-8):101–8.
16 Welp A , Meier LL , Manser T . Emotional exhaustion and workload predict clinician-rated and objective patient safety. Front Psychol. 2015;5(JAN):1573.
17 Heinen MM , van Achterberg T , Schwendimann R , Zander B , Matthews A , Kózka M , et al. Nurses’ intention to leave their profession: a cross sectional observational study in 10 European countries. Int J Nurs Stud. 2013;50(2):174–84. doi:.https://doi.org/10.1016/j.ijnurstu.2012.09.019
18Jaccard Ruedin H, Weaver F. Ageing Workforce in an Ageing Society - How many health professionals will the Swiss healthcare system need by 2030? [Internet]. 2009. (Careum Working Paper 1). Available from: http://www.obsan.admin.ch/sites/default/files/publications/2015/wp_ageing-workforce_e.pdf
19 Boumans NP , Dorant E . Double-duty caregivers: healthcare professionals juggling employment and informal caregiving. A survey on personal health and work experiences. J Adv Nurs. 2014;70(7):1604–15. doi:.https://doi.org/10.1111/jan.12320
20 DePasquale N , Davis KD , Zarit SH , Moen P , Hammer LB , Almeida DM . Combining formal and informal caregiving roles: The psychosocial implications of double- and triple-duty care. J Gerontol B Psychol Sci Soc Sci. 2016;71(2):201–11. doi:.https://doi.org/10.1093/geronb/gbu139
21 Vitaliano PP , Zhang J , Scanlan JM . Is caregiving hazardous to one’s physical health? A meta-analysis. Psychol Bull. 2003;129(6):946–72. doi:.https://doi.org/10.1037/0033-2909.129.6.946
22 Pinquart M , Sörensen S . Differences between caregivers and noncaregivers in psychological health and physical health: a meta-analysis. Psychol Aging. 2003;18(2):250–67. doi:.https://doi.org/10.1037/0882-7974.18.2.250
23 Berglund E , Lytsy P , Westerling R . Health and wellbeing in informal caregivers and non-caregivers: a comparative cross-sectional study of the Swedish general population. Health Qual Life Outcomes. 2015;13(1):109. doi:.https://doi.org/10.1186/s12955-015-0309-2
24 Ward-Griffin C , Brown JB , St-Amant O , Sutherland N , Martin-Matthews A , Keefe J , et al. Nurses negotiating professional-familial care boundaries: striving for balance within double duty caregiving. J Fam Nurs. 2015;21(1):57–85. doi:.https://doi.org/10.1177/1074840714562645
25Duxbury L, Higgins C. Balancing Work, Childcare and Eldercare: A view from the trenches [Internet]. Ottawa; 2013. Available from: http://sprott.carleton.ca/wp-content/uploads/Duxbury-BalancingWorkChildcareEldercare-ExecSummary-1.pdf
26 Dorant E , Boumans NP . Positive and negative consequences of balancing paid work and informal family care: A survey in two different sectors. Int J Heal Psychol Res. 2016;4(1):16–33.
27 DePasquale N , Zarit SH , Mogle J , Moen P , Hammer LB , Almeida DM . Double- and Triple-Duty Caregiving Men: An Examination of Subjective Stress and Perceived Schedule Control. J Appl Gerontol. 2016:0733464816641391. doi:.https://doi.org/10.1177/0733464816641391
28 DePasquale N , Mogle J , Zarit SH , Okechukwu C , Kossek EE , Almeida DM . The Family Time Squeeze: Perceived Family Time Adequacy Buffers Work Strain in Certified Nursing Assistants With Multiple Caregiving Roles. Gerontologist. 2017;0(0):gnw191. doi:.https://doi.org/10.1093/geront/gnw191
29 DePasquale N , Polenick CA , Davis KD , Berkman LF , Cabot TD . A bright side to the work-family interface: Husbands’ support as a resource in double-and-triple-duty caregiving wives’ work lives. Gerontologist. 2017; Epub ahead of print.
30 Goode WJ . A Theory of Role Strain. Am Sociol Rev. 1960;25(4):483–96. Available at: http://www.jstor.org/stable/2092933.
31 Sieber SD . Toward a Theory of Role Accumulation. Am Sociol Rev. 1974;39(4):567–78. doi:.https://doi.org/10.2307/2094422
32 Crane M . Why burned-out doctors get sued more often. Med Econ. 1998;75(10):210–2, 215–8.
33 Nübling M , Stößel U , Hasselhorn H-M , Michaelis M , Hofmann F . Measuring psychological stress and strain at work - Evaluation of the COPSOQ Questionnaire in Germany. Psychosoc Med. 2006;3:Doc05.
34Borritz M, Kristensen TS. Copenhagen Burnout Inventory. Copenhagen Denmark: National Institute of Occupational Health; 1999.
35Nübling M, Stößel U, Hasselhorn H-M, Michaelis M, Hofmann F. Methoden zur Erfassung psychischer Belastungen - Erprobung eines Messinstrumentes (COPSOQ). Bremerhaven: Wirtschaftsverlag NW; 2005. 142 p.
36 Netemeyer RG , Boles JS , McMurrian R . Development and validation of work–family conflict and family–work conflict scales. J Appl Psychol. 1996;81(4):400–10. doi:.https://doi.org/10.1037/0021-9010.81.4.400
37 Baron RM , Kenny DA . The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–82. doi:.https://doi.org/10.1037/0022-3514.51.6.1173
38 DePasquale N , Polenick C , Davis KD , Moen P , Hammer LB , Almeida DM . The Psychosocial Implications of Managing Work and Family Caregiving Roles: Gender Differences Among Information Technology Professionals. J Fam Issues. 2017;38(11):1495–519.
39 Zarit SH , Stephens MA , Townsend A , Greene R . Stress reduction for family caregivers: effects of adult day care use. J Gerontol B Psychol Sci Soc Sci. 1998;53B(5):S267–77. doi:.https://doi.org/10.1093/geronb/53B.5.S267
This study was funded by Swiss National Accident Insurance Fund (SUVA), Federal Office of Public Health (FOPH), State Secretariat for Economic Affairs (SECO).
We declare no conflict of interest as the funding sources were not involved in conceiving this study, analysing data, interpreting results or drafting of the manuscript.