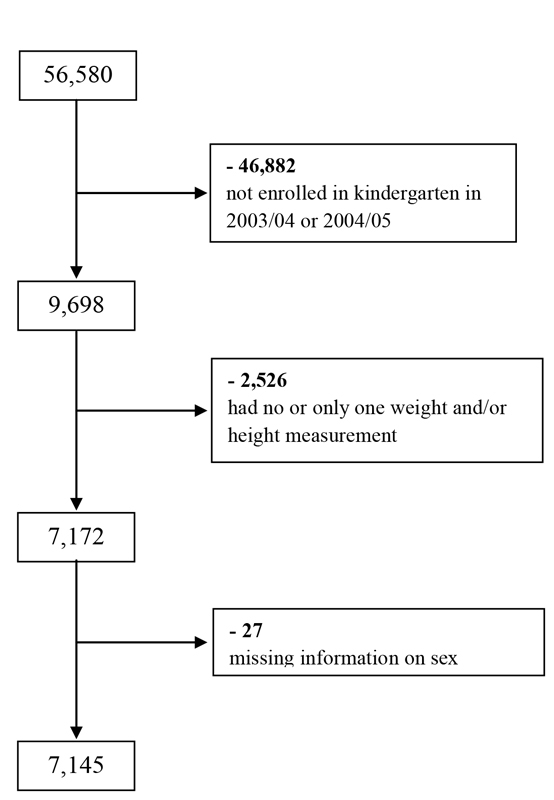
Figure 1 Number of subjects excluded from the study.
DOI: https://doi.org/10.4414/smw.2017.14501
Excess body weight is a major public health burden worldwide. More than two billion people are expected to be overweight or obese and the prevalence is still increasing in most countries [1]. Excess weight develops at a young age. Thus, besides adults, a large number of children and adolescents are affected [2]. In rapidly developing countries such as India or China, childhood obesity is on the rise [3] whereas in developed countries, there is currently a trend towards stagnation at a high level [4, 5].
Several factors, such as low physical activity [6], sedentary behaviour [7] and unfavourable eating habits [8, 9], probably influence the development of childhood obesity. Lifestyle behaviours are driven by individual and environmental factors, including age, gender, ethnicity and parental socioeconomic position [10], access to recreational facilities, vegetation density and traffic exposure [11].
Overweight children are much more likely than normal weight children to become overweight adults [12]. The early school years might be a critical time for the excess body mass index (BMI) gains. Datar et al. [13] found the largest BMI gains in a nationally representative cohort of children in the United States between 1st and 3rd school grades. In Switzerland, previous data also suggest that the school years might be a critical period for excess weight gain [14]. In this country, in 2012, 14.0% of individuals aged 6 to 12 years were overweight and 3.4% were obese according to the International Obesity Task Force (IOTF) criteria [15]. Data from the same time period for adolescents (average age: 14.7 years) showed that 15.9% were overweight and 4.9% were obese, with boys having higher rates of overweight and obesity combined than girls (23.1 vs 17.5%) [14]. However, as in most cases, in these studies there was no individual follow-up – the same individuals could not be tracked over time. Only individual longitudinal data allow proper study of critical periods and possible triggers for excess weight gain and thorough study of coincidence with sociodemographic, environmental and behavioural factors.
In order to define potential target groups, appropriate settings and life periods for preventive public health measures, it is essential to assess children who are already overweight/obese at school entry separately from those who gain excess weight during school years. In this study, we aimed to use routine data from medical examinations in the public schools of Zurich to track individual changes in BMI, to investigate the stability of children’s weight status and to examine the sociodemographic and environmental factors associated with excess weight gain and with overweight/obesity at school entry.
The study procedure was reviewed and classified as uncritical by the ethics committee of the canton of Zurich, Switzerland (Unbedenklichkeitserklärung-Nr. 18-2015).
Data were obtained from the routine medical examinations at public schools undertaken by physicians of the School Health Services of Zurich, the largest city in Switzerland. Examinations usually occur in kindergarten (children aged 5–6 years), grade 4 (10 years) and 8 (14 years) and are aimed at monitoring children’s development (including height and weight), examining function of the sensory organs and checking vaccination status. In addition, weight and height data from the first school grade (7 years) are used for the motor function examination of the Federal Institute of Technology (ETHZ). Also, because routine medical examinations are conducted only at public schools, children who switched to a baccalaureate school after grade 6 did not attend a medical examination at grade 8. Data were gathered between the school years 2003/04 and 2013/14. Only children who were enrolled in kindergarten in 2003/04 or 2004/05, who had more than one weight and height measurement and for whom information on sex was available were considered for analyses.
To ensure the validity of comparing the overweight/obesity prevalence between the kindergarten and the 8th grade, a subsample consisting of children who participated at least in the kindergarten and in the 8th grade examination was used for the analyses shown in table S1, figure 2 and figure 4. In all other analyses, the entire study sample was used. However, the number of children used for analyses leading to the result tables varies owing to the incompleteness of data regarding the variables included.
Different data sources were linked by the Statistics Office of the City of Zurich (SSZ). After linkage, identification information (date of birth, identification number, building and residence indicators) was removed from the data file prior to analysis to ensure the privacy of all examined subjects.
Body weight and height were measured by physicians or nurses during the medical examinations at schools with calibrated scales and fixed tape measures. Children’s weight was measured in light clothing and without shoes to the nearest of 100 g and height to the nearest of 0.5 cm. The protocol and equipment were standardised.
For each measurement point, BMI was calculated (kg/m2) and converted to the age- and sex-specific BMI z-scores by using the STATA “zanthro” command and to BMI percentiles by using the definition of the International Obesity Task Force (IOTF) [16, 17]. Individuals were classified according to Cole et al. [16, 17]: normal weight (equivalent to BMI <25 kg/m2 at age ≥18), overweight (25 kg/m2 ≤ BMI <30 kg/m2), obese (≥30 kg/m2). In light of the scope of this study (excess weight and not underweight), children with BMI <18.5 kg/m2 were classified as normal weight. The mean of the BMI percentiles for the observed children is indicated as mean BMI percentiles.
All children included in the study were classified into four groups of weight status trajectories: (1) children who were of normal weight most of the time i.e., these children were never or in only one examination overweight/obese (normal weight → normal weight); (2) children who were overweight/obese for most or all points of available examination (overweight/obese → overweight/obese); (3) children who were in the normal weight category at the first available measurement and became overweight/obese over time and whose their BMI percentile rose ≥10 percentiles (normal weight → overweight/obese); (4) children who changed weight status category from overweight/obese to normal weight over time and whose BMI percentile reduced ≥10 percentiles (overweight/obese → normal weight).Trajectories depend on the individually available measurements and therefore the length of observation time may vary between children.
Additionally, children were classified according to whether their BMI percentile increased over the school years studied by ≥20 percentiles and ended up ≥85th percentile (at last available measurement). The excess BMI gain was not included in multivariate models because there were no results that were statistically significant (lack of power due to the categorisation of variables).
The sociodemographic characteristics of the children were provided by the school department of the city of Zurich from their administrative databases and included sex, exact date of birth, nationality, main language, district of residence, type of secondary school, household size including the number of children in the household, father’s and mother’s marital status, parental year of birth and an indicator of taxable household income.
Migration background was based on the child’s nationality and his/her main language. Children with German as their main language and Swiss nationality at all existing measurement points were categorized as Swiss. In light of the small samples of specific nationalities, all other children were categorized according to their main language and their nationality at baseline into the following groups: northern and western Europe (including Germany), southern and eastern Europe and countries outside Europe.
Based on the rates found in adults living in Switzerland [18], nationality was dichotomised into; (1) Switzerland or northern and western Europe and (2) southern and eastern Europe and countries outside Europe. These two groups were used for regression analyses presented in table 4 and for the city maps.
The taxable family income was indicated by a letter (A–E). The letters were originally used to determine if a family is entitled to some subsidies for specific services from the city of Zurich and if so what the subsidised amount is. Therefore the income is not linearly distributed over the A–E groups. Families in the B–E groups received some subsidies for specific services from the city of Zurich, because they all had a low taxable income. Families in group A had a medium to high income and therefore do not receive any subsidies. The family income was dichotomised as low or high: the letter A was defined as high income, whereas the letters B–E were defined as low income.
In Zurich, secondary school comprises of grade 7 to 9. In secondary school, pupils are divided according to their capacities and career intentions in three school types: (1) upper level for students who aspire to a university education and entry to baccalaureate school; (2) intermediate level for students reaching an intermediate level of education and intending to pursue a trade or vocation; (3) lower level for students reaching a basic level of education and intending to pursue a trade or vocation.
Environmental data were available for 2010 from the Statistik Stadt Zurich (SSZ). Land use was categorised as buildings, land surrounding buildings, traffic, parks and sports grounds, meadows and farming, woodland and water bodies. The categories “parks and sports facilities” and “meadows and farming areas” and “woodland” were combined to form a new category “green area”. Proportions of land use categories were calculated for every city district.
For descriptive analyses, we calculated means, standard deviations and proportions. Cross-tabulation was used to investigate the changes in anthropometric variables over time. Differences between groups were detected in the independent samples t-test and Pearson’s chi-square test. In order to examine individual predictors for the existence of overweight/obesity at school entry, multiple logistic regression models were calculated and adjusted for sex, district of residence, family income and father’s marital status. Murer et al. [19] detected risk factors (such as parental nationality) that play an important role in the development of childhood obesity and showed that these risk factors affect boys and girls differently. In order to evaluate the role of these protective and risk factors in the potential target population, we stratified for sex and migration background. Three separate population groups were considered: (1) models including all examined children and separate models to look individually at children with (2) Western and Northern European background and (3) non-Western and non-Northern European background were calculated. Gain in BMI percentiles over time was examined with multiple linear regression models. The dependent variable was the difference in BMI percentile between the first and the last available measurement. Since the date of birth and examination date were available and the time spans between measurements were unequal, we used years (and not school period) as time metric. The multiple linear regression models were adjusted for time (in years) between the first and the last available BMI value and for age and BMI percentile at the first available measurement. The variables in the final models were selected with a stepwise procedure based on the Bayesian Information Criterion (BIC). As father’s and the mother’s marital status are alike in many cases (both married, both divorced…), including both in the models would induce a high danger of multicollinearity and not add much additional information to the model. For this reason, only one of the two variables was included in the model. Individuals with missing information were excluded from the respective analyses. In some analyses, samples are small (e.g., a sample of children with a Western and Northern European background, children living in district 1), precluding robust results. Data were analysed using Stata V.13.0 (StataCorp, Texas, USA). In all cases, the results were considered to be statistically significant if p <0.05.
Of the 56 580 children who had ≥1 examination during the school years 2003/04 and 2013/14, 7145 fulfilled the inclusion criteria. A total of 49 408 children were either not enrolled in kindergarten in 2003/04 or 2004/05 or had no or only one weight and/or height measurement and were therefore excluded. In addition, 27 children were excluded because of incomplete information on sex (fig. 1).
Figure 1 Number of subjects excluded from the study.
Of the 7145 remaining children, 3542 participated at least in the kindergarten and in the 8th grade examination, 641 children left elementary school after the 6th grade and went to baccalaureate school, 1203 children moved into or away from the city of Zurich and 1759 had some missing data owing to school absence on the examination day (table 1).
Table 1 Study sample: participation of the children in the various examinations and reasons for missing data.
| Kindergarten | Grade 1 | Grade 4 | Grade 8 | Study sample* | Reasons for missing data |
|---|---|---|---|---|---|
| X | (x) | (x) | X | 3542 | |
| X | (x) | (x) | 2466 | 538 children switched to baccalaureate school after grade 6 563 children moved away from the City of Zurich after kindergarten 1365 children were absent from school or refused to participate at least in grade 8 |
|
| (x) | (x) | X | 848 | 501 children moved into the City of Zurich after kindergarten 347 children were absent from school or refused to participate at least in kindergarten |
|
| X | X | 289 | 103 children switched to baccalaureate school after grade 6 139 children moved into or away from the City of Zurich 47 were absent from school or refused to participate in kindergarten and in grade 8 |
||
| Total | 7145 |
x = children participating in the respective examination (x) = children participating either in the 1st grade examination or in the 4th grade examination or in both examinations * n = children participating in examination in the respective grade (kindergarten, 1, 4, 8)
The demographic characteristics of the 3542 children who participated at least in the kindergarten and in the 8th grade examinations are shown in table S1 (appendix 1). Equivalent data based on the entire analysed sample (n = 7145) is shown in table S2. Of the 3542 children who participated in the kindergarten and 8th grade examinations, 51.8% were male. At school entry, half of the children (50.3%) were foreign nationals. This proportion decreased over the school career. However, >60% of the children had a migration background.
In the same group of children, the mean BMI percentiles at grade 1 (+5.5, p <0.001), 4 (+8.9, p <0.001) and 8 (+12.8, p <0.001) were significantly higher than the mean percentiles at kindergarten. Accordingly, the number of children who were classified as overweight/obese increased significantly (p <0.001) from kindergarten (17.6%) to grade 8 (26.0%). The prevalence of overweight/obesity was higher for girls than boys in grade 1 (p = 0.035). In contrast, in grade 8, boys were more often overweight/obese than girls (p = 0.031; fig. 2). At all school grades, children with a migration background from southern and eastern Europe were more often overweight/obese than the Swiss children. The highest difference could be found at school entry, where 25.5% of children with southern and eastern European background were overweight/obese, as compared with 9.9% of the Swiss children. Over the school grades considered, overweight and obesity increased similarly among both nationality groups and amounted at grade 8 to 32.5% and 18.8%, respectively. Children with a northern and western European background (including Germany) had a prevalence of overweight/obesity comparable to that of Swiss children (12.6% in kindergarten; 16.8% in grade 8). Over the school grades, the number of overweight/obese children increased most among children with a migration background from outside Europe (15.4% in kindergarten; 27.9% in grade 8).
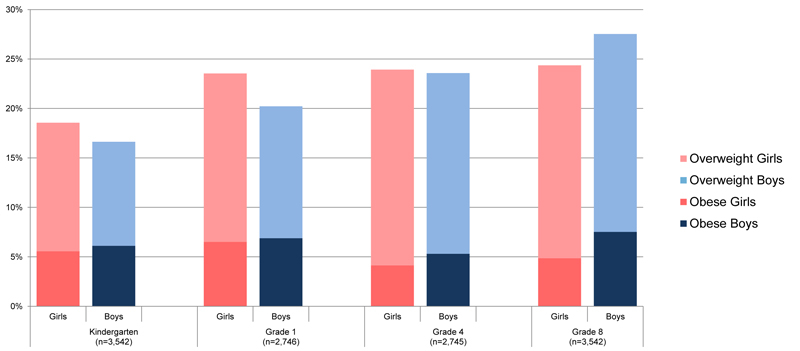
Figure 2 Prevalence of overweight/obesity in different school grades among boys and girls.
Figure 3a shows the proportions of all included children in the study (n = 7145) with excess BMI gain by city district. Overall, in 7.5% the BMI percentiles increased over the school years considered by >20 percentiles and ended up ≥85th percentile. Districts coloured dark red had the highest prevalence of excess BMI gain, whereas districts in the lightest colour had the lowest. Differences in districts were compared also among other variables such as the proportion of children with a migration background from southern and eastern Europe or a country outside Europe (fig. 3b), low income of the parents (fig. 3c), low education level of the children (fig. 3d) and environmental characteristics (fig 3e, 3f, 3g). District 4 showed the highest proportion of children with excess BMI gain as well as the highest proportion of children with a migration background from southern and eastern Europe or a country outside Europe, low income of the parents and low education levels of the children. In addition, this district had a low proportion of green areas and a relatively high proportion of traffic and buildings.

Figure 3a-g Maps of the City of Zurich with excess BMI gain, sociodemographic characteristics and environment data in different districts (intensity of the colour symbolises the quantity of proportion; dark = high proportion, light = low proportion) (n = 7145).
Table 2 presents the prevalence of the four groups of weight status trajectories in all children included in the study (n = 7145) and in the important sociodemographic subpopulation. Most of the children remained in the same weight category over the school grades studied. One-tenth of the children showed an ascending trajectory, whereas only 3% were found in the descending trajectory. Differences in the weight status trajectories were observed with respect to the migration background of the children, the age of the parents at childbirth and the taxable income. No sex differences were observed.
Table 2 Weight status trajectories in all children (n = 7145) and in specific strata.
| normal weight → normal weight | overweight/obese → overweight/obese | normal weight → overweight/obese | overweight/obese → normal weight | ||
|---|---|---|---|---|---|
| All children | 5130 (71.8%) | 1027 (14.4%) | 774 (10.8%) | 214 (3.0%) | |
| Sex | Girls | 2514 (71.8%) | 496 (14.2%) | 364 (10.4%) | 129 (3.7%) |
| Boys | 2616 (71.8%) | 531 (14.6%) | 410 (11.3%) | 85 (2.3%) | |
| Migration background | None | 2662 (81.1%) | 272 (8.3%) | 284 (8.7%) | 64 (1.9%) |
| Northern and western Europe (incl. Germany) | 255 (81.5%) | 29 (9.3%) | 21 (6.7%) | 8 (2.6%) | |
| Southern and eastern Europe | 1529 (60.6%) | 559 (22.1%) | 326 (12.9%) | 111 (4.4%) | |
| Outside Europe | 684 (66.8%) | 166 (16.2%) | 143 (14.0%) | 31 (3.0%) | |
| Missing data (n) | 1 | ||||
| Age of mother at child’s birth | <25 | 819 (64.6%) | 245 (19.3%) | 160 (12.6%) | 44 (3.5%) |
| >25 | 4311 (73.4%) | 781 (13.3%) | 614 (10.5%) | 170 (2.9%) | |
| Missing data (n) | 1 | ||||
| Age of father at child’s birth | <25 | 305 (63.0%) | 96 (19.8%) | 68 (14.1%) | 15 (3.1%) |
| >25 | 4825 (72.4%) | 931 (14.0%) | 706 (10.6%) | 199 (3.0%) | |
| Taxable income | Low | 1929 (68.1%) | 459 (16.2%) | 358 (12.6%) | 88 (3.1%) |
| High | 2697 (74.8%) | 458 (12.7%) | 344 (9.5%) | 107 (3.0%) | |
| Missing data (n) | 504 | 110 | 72 | 19 |
Trajectories depend on the individually available measurements and may vary therefore between children in time length.
To examine the proportion of children who changed weight categories between kindergarten and grade 8, weight status categories were cross-tabulated. Among the children who had normal weight in kindergarten, the weight status was relatively stable over the 8 school years (fig. 4). Most children (83.8%) with normal weight remained in that category between kindergarten and grade 8. Only 16.2% of the children who were not overweight/obese in kindergarten changed weight category to overweight/obese. Larger changes occurred among the overweight/obese children. Of the 415 children who were overweight in kindergarten, nearly 40% were classified as normal weight 8 years later, whereas 14.5% had become obese. Among those who were obese in kindergarten only 7.3% moved into the normal weight category. However, nearly 50% changed to the overweight category.
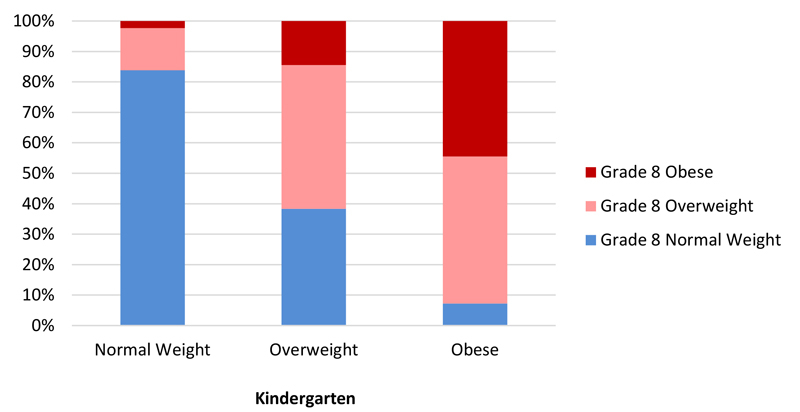
Figure 4 Prevalence of changes in weight status categories from kindergarten to grade 8 (n = 3542).
A multivariate logistic regression analysis found that the odds ratio of being overweight/obese at school entry is strikingly elevated in children with a migration background compared with Swiss children after adjustment for sex, district of residence, family income and father’s marital status (table 3). Analyses were also stratified by migration background. In children with a migration background from southern and eastern Europe or a country outside Europe, there was a significant association between district of residence and weight status in kindergarten. In children with a western and northern European background, girls had a greater risk of being overweight/obese at school entry than boys (table 3). No sex differences were found among children with a non-western and non-northern European background.
Table 3 Odds ratios (95% confidence intervals) for children being overweight/obese at school entry, based on sociodemographic variables and stratified for migration background.
| All Children |
Migration background:
southern, eastern and outside Europe* |
Migration background:
western and northern Europe** |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| n = 5199 | n = 2597 | n = 2598 | |||||||
| OR | 95% CI | p-value | OR | 95% CI | p-value | OR | 95% CI | p-value | |
| Sex1 | |||||||||
| Girls | 1.15 | 0.99–1.34 | 0.064 | 1.03 | 0.86–1.24 | 0.745 | 1.44 | 1.10–1.89 | 0.008 |
| Migration background2 | |||||||||
| Northern and western Europe (incl. Germany) | 1.60 | 1.02–2.49 | 0.040 | – | 1.67 | 1.08–2.66 | 0.026 | ||
| Southern and eastern Europe | 3.39 | 2.81–4.09 | <0.001 | – | – | ||||
| Outside Europe | 1.95 | 1.49–2.55 | <0.001 | 0.60 | 0.47–0.77 | <0.001 | – | ||
| Taxable income4 | |||||||||
| Low | 1.00 | 0.85–1.18 | 0.956 | 0.89 | 0.73–1.08 | 0.225 | 1.33 | 0.97–1.77 | 0.062 |
| Father's marital status5 | |||||||||
| Unmarried | 1.05 | 0.69–1.59 | 0.818 | 0.67 | 0.28–1.63 | 0.378 | 1.18 | 0.74–1.93 | 0.492 |
| Divorced/separated/widowed | 1.04 | 0.77–1.40 | 0.804 | 1.24 | 0.83–1.84 | 0.295 | 0.78 | 0.56–1.47 | 0.311 |
| District of residence3 | |||||||||
| District 1 | 1.18 | 0.34–4.10 | 0.796 | – | 1.43 | 0.40–5.23 | 0.585 | ||
| District 3 | 1.55 | 1.04–2.33 | 0.033 | 1.66 | 0.94–2.92 | 0.079 | 1.57 | 0.87–2.85 | 0.133 |
| District 4 | 1.35 | 0.86–2.12 | 0.188 | 1.45 | 0.81–2.60 | 0.208 | 2.18 | 0.81–5.91 | 0.125 |
| District 5 | 2.19 | 1.33–3.63 | 0.002 | 2.91 | 1.52–5.57 | 0.001 | 1.02 | 0.36–2.87 | 0.973 |
| District 6 | 1.74 | 1.12–2.71 | 0.014 | 2.58 | 1.37–4.87 | 0.003 | 1.20 | 0.64–2.27 | 0.569 |
| District 7 | 1.42 | 0.89–2.25 | 0.138 | 1.15 | 0.54–2.44 | 0.716 | 1.58 | 0.87–2.86 | 0.134 |
| District 8 | 0.90 | 0.48–1.67 | 0.731 | 1.49 | 0.64–3.45 | 0.350 | 0.51 | 0.19–1.42 | 0.188 |
| District 9 | 1.57 | 1.05–2.34 | 0.028 | 1.77 | 1.02–3.09 | 0.044 | 1.40 | 0.76–2.60 | 0.290 |
| District 10 | 1.50 | 0.97–2.32 | 0.065 | 1.64 | 0.88–3.03 | 0.117 | 1.42 | 0.77–2.62 | 0.264 |
| District 11 | 1.29 | 0.87–1.90 | 0.209 | 1.51 | 0.87–2.60 | 0.143 | 1.05 | 0.58–1.90 | 0.878 |
| District 12 | 1.43 | 0.95–2.14 | 0.084 | 1.51 | 0.87–2.63 | 0.146 | 1.64 | 0.87–3.10 | 0.126 |
Reference categories: 1Boys, 2Swiss, 3District 2, 4High taxable income, 5Married * Reference category for migration background: Southern and Eastern European background ** Reference category: Swiss Figures adjusted for all other listed variables Bold indicates significant results.
Table 4 shows the results of the linear regression analysis for all children and stratified by sex. The increase in BMI percentile was strongly associated with migration background. Children with a migration background from southern and eastern Europe or a country outside Europe gained on average 1.66 or 1.97 percentiles, respectively, more per year than Swiss children. In addition, the difference in BMI percentiles was significantly associated with sex, indicating a greater gain in BMI percentiles in boys than girls. Boys with southern and eastern European background showed the greatest gain in BMI percentiles. In girls, we found no differences between the nationality groups, but the school type significantly influenced excess weight gain.
Table 4 Results of a linear regression model for differences in BMI percentile over school time, based on sociodemographic variables, total and by sex.
|
All children
n = 6089 |
Boys
n = 3117 |
Girls
n = 2972 |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Coef. | 95% CI | p-value | Coef. | 95% CI | p-value | Coef. | 95% CI | p-value | |
| Sex1 | |||||||||
| Girls | ˗1.90 | ˗3.00 – ˗0.80 | 0.001 | – | – | – | – | ||
| Migration background2 | |||||||||
| Northern and Western Europe (incl. Germany) | ˗1.85 | ˗4.65–0.96 | 0.197 | ˗1.60 | ˗5.61–2.40 | 0.432 | ˗2.09 | ˗6.03–1.85 | 0.298 |
| Southern and Eastern Europe | 1.67 | 0.29–3.04 | 0.017 | 2.30 | 0.33–4.28 | 0.023 | 1.00 | ˗0.91–2.91 | 0.306 |
| Outside Europe | 1.98 | 0.10–3.86 | 0.040 | 1.63 | ˗1.02–4.27 | 0.228 | 2.41 | ˗0.27–5.09 | 0.078 |
| Taxable income4 | |||||||||
| Low | 0.38 | ˗0.83–1.59 | 0.533 | 0.39 | ˗1.36–2.14 | 0.662 | 0.29 | ˗1.38–1.96 | 0.734 |
| Father's marital status5 | |||||||||
| Unmarried | ˗2.43 | ˗5.05–0.18 | 0.069 | ˗1.53 | ˗5.32–2.26 | 0.430 | ˗3.15 | ˗6.77–0.46 | 0.087 |
| Divorced/separated/widowed | ˗1.34 | ˗3.38–0.71 | 0.200 | ˗2.16 | ˗5.15–0.83 | 0.156 | ˗0.47 | ˗3.26–2.32 | 0.739 |
| School type6 | |||||||||
| Intermediate level | 4.92 | 2.14–7.69 | 0.001 | 2.02 | ˗2.05–6.10 | 0.330 | 7.56 | 3.77–11.35 | <0.001 |
| Lower level | 8.40 | 5.37–11.43 | <0.001 | 4.03 | ˗0.40–8.45 | 0.075 | 12.98 | 8.82–17.13 | <0.001 |
| Unknown | 3.71 | 1.61–5.81 | 0.001 | 4.43 | 1.32–7.54 | 0.005 | 2.66 | ˗0.18–5.50 | 0.066 |
| District of residence3 | |||||||||
| District 1 | 1.54 | ˗5.80–8.87 | 0.681 | 4.10 | ˗7.12–15.33 | 0.474 | ˗0.67 | ˗10.29–8.95 | 0.891 |
| District 2 | 5.37 | 2.55–8.18 | <0.001 | 5.13 | 1.04–9.23 | 0.014 | 5.78 | 1.91–9.65 | 0.003 |
| District 3 | 5.55 | 3.01–8.10 | <0.001 | 4.93 | 1.22–8.63 | 0.009 | 6.04 | 2.56–9.52 | 0.001 |
| District 4 | 7.59 | 4.56–10.63 | <0.001 | 7.56 | 3.25–11.87 | 0.001 | 7.62 | 3.34–11.89 | <0.001 |
| District 5 | 1.56 | ˗2.15–5.26 | 0.411 | 2.77 | ˗2.39–7.92 | 0.293 | ˗0.17 | ˗5.55–5.21 | 0.950 |
| District 7 | 1.92 | ˗0.84–4.69 | 0.173 | 0.05 | ˗3.99–4.09 | 0.981 | 3.58 | ˗0.19–7.36 | 0.063 |
| District 8 | 1.23 | ˗2.35–4.82 | 0.500 | 1.51 | ˗3.47–6.49 | 0.552 | 0.90 | ˗4.31–6.11 | 0.734 |
| District 9 | 6.38 | 3.85–8.90 | <0.001 | 7.12 | 3.42–10.82 | <0.001 | 5.61 | 2.16–9.05 | 0.001 |
| District 10 | 1.78 | ˗0.92–4.48 | 0.196 | 2.74 | ˗1.23–6.70 | 0.176 | 0.93 | ˗2.73–4.60 | 0.617 |
| District 11 | 7.30 | 4.90–9.70 | <0.001 | 7.91 | 4.44–11.39 | <0.001 | 6.65 | 3.35–9.95 | <0.001 |
| District 12 | 6.34 | 3.75–8.92 | <0.001 | 6.97 | 3.25–10.70 | <0.001 | 5.86 | 2.29–9.44 | 0.001 |
Reference categories: 1Boys, 2Swiss, 3District 6, 4High taxable income, 5Married, 6Upper level Adjusted for time (in years) between the first and the last available BMI-value and for age and BMI-percentile at the first available measurement Bold indicates significant results
The aim of this study was to examine trajectories in children’s weight status and to investigate sociodemographic and environmental factors associated with overweight/obesity at school entry, as well as with excess weight gain over school years. The results suggest that children’s weight status was relatively stable over the eight school years considered. Among those who were obese in kindergarten, only 7.3% changed to the normal weight category, highlighting that weight status at school entry predicts weight status during childhood and adolescence. The study showed a strong association between migration background and overweight/obesity at school entry (kindergarten): compared with Swiss children, children with a migration background in southern and eastern Europe, in northern and western Europe, and outside Europe had higher odds of being overweight/obese.
Although a vast majority (>80%) of the children had a stable weight status over their school career, the mean BMI percentile changed over time. This indicator increased from kindergarten to grade 8 (+12.8 BMI percentiles) and so did the prevalence of overweight/obesity (from 17.6 to 26.0%). The increase was associated with male sex, migration background (southern and eastern Europe or outside Europe), school type and the city district of residence, but not with environmental data such as proportions of green areas, traffic and buildings.
The results of general weight status stability and tracking over school years are consistent with other research [20–22]. Comparing the prevalence of overweight/obesity with other high-income countries with high levels of migration the results are similar [23, 24].
Regarding sex the results are inconsistent. Wheaton et al. reported, in line with our results, a higher prevalence of overweight/obesity in boys [22], but others did not find an increased risk for excess weight gain in boys than in girls [20, 21]. However, these studies did not follow individuals until adolescence. A cross-sectional study including other urban and rural regions of Switzerland [14] also showed a higher prevalence of overweight/obesity for girls than boys in kindergarten and a catch up in excess BMI in boys, finally resulting in higher prevalence in boys at the end of the school career. In our study, the boys gained on average 1.9 BMI percentiles more per year than girls after full adjustment. It can be speculated whether girls pay more attention to their body image and make more efforts to combat weight gain [25]. Sex differences further increased with increasing age. In Switzerland in 2012, adult overweight/obesity prevalence was 50.5% in men and 32.0% in women [26].
Differences in the prevalence of overweight/obesity and in excess BMI gain depend on the migration background. Cross-sectional European studies showed a north-south gradient in childhood obesity [27, 28], with a lower prevalence in northern than in southern European countries. Our findings corroborated such a north-south gradient. The explanations for higher rates in children with a migration background in southern or eastern Europe compared with those with western or northern European background could be explained by variations in health behaviour, education, socioeconomic position and cultural values [29].
Several studies found an inverse relationship between income and/or education and obesity risk [30, 31]. However, socioeconomic status is complex and comprises various dimensions, including income, education and occupation. In this study, only family income was available, and this dimension was not associated with variations in excess weight gain. Faeh et al. [31] pointed out that education, in comparison with income and occupational class, was the strongest predictor of overweight/obesity in adults, especially in women. As shown in table 4, lower school type was strongly associated with excess weight gain in girls, suggesting that this gradient is rooted at a young age. Moreover, our results show that children from more socially deprived city districts had higher risks of being or becoming overweight/obese compared with those living in more attractive and wealthy districts. In line with this result, Guessous et al. [32] showed that individual BMI is associated with the mean BMI in the neighbourhood. These BMI clusters were spatially dependent and influenced by neighbourhood-level income [32, 33]. In addition, Moser et al. [34] showed that life expectancy is strongly associated with the social standing of neighbourhoods in Switzerland.
The fact that overweight/obesity were already largely prevalent in kindergarten suggests that interventions aimed at preventing overweight/obesity must impact before school entry. This is supported by others, who showed that gestation [35, 36] and early childhood [37] are critical periods. Educating (future) parents may affect their children’s development of food- and activity-related behaviours [38].
Migrants from southern and eastern Europe are an important target group for interventions, but difficult to reach with general prevention programs [39]. To meet this challenge, interventions need to be targeted and culturally adapted. Furthermore, appropriate language and intercultural education of public health professionals are important. Structural public health measures probably impact on the entire population, including families with migration background. Institutional organisations (e.g., public day nurseries, leisure centres, schools) must provide a healthy environment, promoting a healthy behaviour in everyday life, such as physical activity, and fruit and vegetable consumption. At the school level, there should be a focus on boys with a southern and eastern European background and girls in a lower-level school type. Furthermore, city planners and politicians ought to be aware of (childhood) obesity in order to adapt built, social, political and legislative environments accordingly. Longitudinal data from routine medical examinations at school are crucial for monitoring childhood obesity and for the identification of potential determinants and specific target groups as well as of ideal life course periods for interventions. It is, therefore, worthwhile to invest in and improve these time- and cost-effective examinations.
The major strength of this study is the large and quite complete study sample from an economically highly developed country. Data were assessed up to four times over eight school years so that individual changes in measured BMI could be tracked. Besides BMI, a wide range of potential determinants of various routine data sources could be considered.
The study has several limitations. First, the completeness of data varied over the study period. Children who changed to baccalaureate school after grade 6 could not be followed until grade 8. Also, children attending private schools could not be included. However, these groups can be considered at “low-risk” for excess BMI gain and therefore not relevant for targeted public health interventions. Expectedly, 10% of pupils refused the medical examination at school and were attended to by their family doctor. In addition, children who moved into or away from Zurich could not be followed up over all school grades. Second, in longitudinal analyses considering the entire school grade range, children finally attaining a higher education level were underrepresented, because those who go to a baccalaureate school missed the final examination. This is likely to lead to an overestimation of overweight/obesity and possibly to a misestimation of determinants. A study in Swiss conscripts showed that 26% of unskilled workers were overweight versus 13% of students that attended baccalaureate school, and 12% of unskilled workers were obese against 2% of students [40].
Third, the database does not include information on the occupational and educational level of parents precluding a more detailed and complete examination of the role of socioeconomic status. Moreover, we used broad definitions for socioeconomic and migration background precluding to analyse associations between these two characteristics. In addition, we can't make any hypotheses why Switzerland is one of the countries with the lowest overall prevalence of overweight in childhood and adolescence. Switzerland has a large variability of ethnicities which do not allow to explain the differences in other countries by individual or genetic factors.
Overweight/obesity at school entry is associated with migration background and tracks strongly through childhood and adolescence. Boys with migration background in Southern and Eastern Europe and girls following lower-level school trajectories are mostly at risk for excess weight gain over school years. Since almost one-fifth of the children in this study were overweight or obese already in kindergarten, routine gathering of relevant data of children and of their parents prior to school entry should be focused on.
Table S1 Demographic characteristics of the children who participated at least in kindergarten and in grade 8 (n = 3542).
| Kindergarten | Grade 1 | Grade 4 | Grade 8 | |||||
|---|---|---|---|---|---|---|---|---|
| Nationality Swiss | 1759 (49.7%) | 2128 (77.6%) | 2925 (82.7%) | |||||
| Missing (n) | 0 | 150 | 10 | |||||
| Migration background | ||||||||
| None | 1391 (39.3%) | |||||||
| Southern and eastern Europe | 1540 (43.5%) | |||||||
| Northern and western Europe (incl. Germany) | 95 (2.7%) | |||||||
| Outside Europe | 512 (14.5%) | |||||||
| Missing (n) | 4 | |||||||
| Secondary school type | ||||||||
| Upper level | 538 (13.2%)* | |||||||
| Intermediate level | 2104 (51.6%) | |||||||
| Lower level | 1379 (33.8%) | |||||||
| Unknown | 59 (1.4%) | |||||||
| Place of residence | ||||||||
| District 1 | 18 (0.5%) | 10 (0.4%) | 14 (0.5%) | 18 (0.5%) | ||||
| District 2 | 251 (7.1%) | 152 (5.5%) | 187 (6.8%) | 251 (7.1%) | ||||
| District 3 | 440 (12.4%) | 325 (11.8%) | 362 (13.2%) | 440 (12.4%) | ||||
| District 4 | 259 (7.3%) | 226 (8.2%) | 193 (7.0%) | 259 (7.3%) | ||||
| District 5 | 113 (3.2%) | 86 (3.1%) | 87 (3.2%) | 113 (3.2%) | ||||
| District 6 | 246 (7.0%) | 198 (7.2%) | 179 (6.5%) | 246 (7.0%) | ||||
| District 7 | 202 (5.7%) | 126 (4.6%) | 147 (5.4%) | 202 (5.7%) | ||||
| District 8 | 101 (2.9%) | 71 (2.6%) | 83 (3.0%) | 101 (2.9%) | ||||
| District 9 | 480 (13.6%) | 313 (11.4%) | 364 (13.3%) | 480 (13.6%) | ||||
| District 10 | 269 (7.6%) | 223 (8.1%) | 208 (7.6%) | 269 (7.6%) | ||||
| District 11 | 665 (18.8%) | 576 (21.0%) | 528 (19.2%) | 665 (18.8%) | ||||
| District 12 | 496 (14.0%) | 439 (16.0%) | 393 (14.3%) | 496 (14.0%) | ||||
| Missing (n) | 12 | 1875 | 160 | 50 | ||||
| Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | |
| No. | 1835 (51.8%) | 1707 (48.2%) | 1425 (51.9%) | 1321 (48.1%) | 1413 (51.5%) | 1332 (48.5%) | 1835 (51.8%) | 1707 (48.2%) |
| Age (years) | 5.9 | 5.9 | 7.2 | 7.1 | 10.1 | 10.1 | 14.2 | 14.1 |
| Height (cm) | 117.4 | 116.2 | 125.1 | 123.7 | 141.5 | 140.8 | 167.1 | 161.5 |
| Weight (kg) | 22.3 | 21.5 | 26.2 | 25.5 | 36.8 | 36.4 | 59.8 | 56.5 |
| BMI percentiles | 53.8 | 50.7 | 59.7 | 55.7 | 63.8 | 58.4 | 66.2 | 64.0 |
* children participated in kindergarten, but not in grade 8
Table S2 Demographic characteristics of all children included in the study (n = 7145).
| Kindergarten | Grade 1 | Grade 4 | Grade 8 | |||||
|---|---|---|---|---|---|---|---|---|
| Nationality Swiss | 3598 (56.0%) | - | 4798 (76.9%) | 3673 (80.2%) | ||||
| Missing (n) | 721 | 909 | 2567 | |||||
| Migration background | ||||||||
| None | 3282 (45.9%) | |||||||
| Southern and eastern Europe | 2525 (35.3%) | |||||||
| Northern and western Europe (incl. Germany) | 313 (4.4%) | |||||||
| Outside Europe | 1024 (14.3%) | |||||||
| Missing (n) | 1 | |||||||
| Secondary school type | ||||||||
| Upper level | 641 (9.0%) | |||||||
| Intermediate level | 2686 (37.6%) | |||||||
| Lower level | 1793 (25.1%) | |||||||
| Unknown | 2025 (28.3%) | |||||||
| Place of residence | ||||||||
| District 1 | 40 (0.6%) | 19 (0.6%) | 36 (0.6%) | 28 (0.6%) | ||||
| District 2 | 480 (7.5%) | 311 (9.8%) | 467 (7.9%) | 367 (8.1%) | ||||
| District 3 | 862 (13.5%) | 407 (12.8%) | 764 (13.0%) | 578 (12.8%) | ||||
| District 4 | 433 (6.8%) | 202 (6.3%) | 300 (5.1%) | 272 (6.0%) | ||||
| District 5 | 210 (3.3%) | 132 (4.1%) | 148 (2.5%) | 102 (2.3%) | ||||
| District 6 | 428 (6.7%) | 235 (7.4%) | 469 (8.0%) | 312 (6.9%) | ||||
| District 7 | 426 (6.7%) | 240 (7.5%) | 444 (7.5%) | 233 (5.2%) | ||||
| District 8 | 177 (2.8%) | 56 (1.8%) | 157 (2.7%) | 92 (2.0%) | ||||
| District 9 | 833 (13.0%) | 303 (9.5%) | 753 (12.8%) | 610 (13.5%) | ||||
| District 10 | 549 (8.6%) | 270 (8.5%) | 512 (8.7%) | 363 (8.0%) | ||||
| District 11 | 1157 (18.1%) | 646 (20.3%) | 1108 (18.8%) | 930 (20.6%) | ||||
| District 12 | 803 (12.6%) | 365 (11.5%) | 736 (12.5%) | 634 (14.0%) | ||||
| Missing (n) | 747 | 3959 | 1251 | 2624 | ||||
| Boys | Girls | Boys | Girls | Boys | Girls | Boys | Girls | |
| No. | 3,082 (51.3%) | 2,926 (48.7%) | 2,908 (51.3%) | 2,765 (48.7%) | 2,604 (50.5%) | 2,554 (49.5%) | 2,252 (51.3%) | 2,138 (48.7%) |
| Age (years) | 5.9 | 5.9 | 7.2 | 7.1 | 10.1 | 10.1 | 14.2 | 14.2 |
| Height (cm) | 117.2 | 116.1 | 125.0 | 123.8 | 141.6 | 141.0 | 167.3 | 161.5 |
| Weight (kg) | 22.1 | 21.4 | 26.0 | 25.3 | 36.5 | 36.0 | 59.9 | 56.5 |
| BMI percentiles | 53.2 | 49.6 | 58.2 | 54.1 | 63.4 | 55.7 | 66.1 | 63.9 |
The authors thank the School Health Services, the Department of School and Sport and the SSZ, all from the City of Zurich, and the Federal Institute of Technology (ETHZ) for providing anthropometric, sociodemographic and environmental data. In addition, we would like to acknowledge the support of Sabine Rohrmann, Tina Lohse, Isabelle Herter-Aeberli and Hanspeter Stamm.
No financial support and no other potential conflict of interest relevant to this article was reported.
1 Ng M , Fleming T , Robinson M , Thomson B , Graetz N , Margono C , et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9945):766–81. doi:.https://doi.org/10.1016/S0140-6736(14)60460-8
2 de Onis M , Lobstein T . Defining obesity risk status in the general childhood population: which cut-offs should we use? Int J Pediatr Obes. 2010;5(6):458–60. doi:.https://doi.org/10.3109/17477161003615583
3 Ramachandran A , Chamukuttan S , Shetty SA , Arun N , Susairaj P . Obesity in Asia--is it different from rest of the world. Diabetes Metab Res Rev. 2012;28(Suppl 2):47–51. doi:.https://doi.org/10.1002/dmrr.2353
4 Flegal KM , Carroll MD , Ogden CL , Curtin LR . Prevalence and trends in obesity among US adults, 1999-2008. JAMA. 2010;303(3):235–41. doi:.https://doi.org/10.1001/jama.2009.2014
5 Olds T , Maher C , Zumin S , Péneau S , Lioret S , Castetbon K , et al. Evidence that the prevalence of childhood overweight is plateauing: data from nine countries. Int J Pediatr Obes. 2011;6(5-6):342–60. doi:.https://doi.org/10.3109/17477166.2011.605895
6 O’Brien M , Nader PR , Houts RM , Bradley R , Friedman SL , Belsky J , et al. The ecology of childhood overweight: a 12-year longitudinal analysis. Int J Obes. 2007;31(9):1469–78. doi:.https://doi.org/10.1038/sj.ijo.0803611
7 Gortmaker SL , Must A , Sobol AM , Peterson K , Colditz GA , Dietz WH . Television viewing as a cause of increasing obesity among children in the United States, 1986-1990. Arch Pediatr Adolesc Med. 1996;150(4):356–62. doi:.https://doi.org/10.1001/archpedi.1996.02170290022003
8 Fiorito LM , Marini M , Francis LA , Smiciklas-Wright H , Birch LL . Beverage intake of girls at age 5 y predicts adiposity and weight status in childhood and adolescence. Am J Clin Nutr. 2009;90(4):935–42. doi:.https://doi.org/10.3945/ajcn.2009.27623
9 Huang CJ , Hu HT , Fan YC , Liao YM , Tsai PS . Associations of breakfast skipping with obesity and health-related quality of life: evidence from a national survey in Taiwan. Int J Obes. 2010;34(4):720–5. doi:.https://doi.org/10.1038/ijo.2009.285
10 Wang Y , Beydoun MA . The obesity epidemic in the United States--gender, age, socioeconomic, racial/ethnic, and geographic characteristics: a systematic review and meta-regression analysis. Epidemiol Rev. 2007;29(1):6–28. doi:.https://doi.org/10.1093/epirev/mxm007
11 Dunton GF , Kaplan J , Wolch J , Jerrett M , Reynolds KD . Physical environmental correlates of childhood obesity: a systematic review. Obes Rev. 2009;10(4):393–402. doi:.https://doi.org/10.1111/j.1467-789X.2009.00572.x
12 Singh AS , Mulder C , Twisk JWR , van Mechelen W , Chinapaw MJ . Tracking of childhood overweight into adulthood: a systematic review of the literature. Obes Rev. 2008;9(5):474–88. doi:.https://doi.org/10.1111/j.1467-789X.2008.00475.x
13 Datar A , Shier V , Sturm R . Changes in body mass during elementary and middle school in a national cohort of kindergarteners. Pediatrics. 2011;128(6):e1411–7. doi:.https://doi.org/10.1542/peds.2011-0114
14 Stamm H , Gebert A , Guggenbühl L , Lamprecht M . Excess weight among children and adolescents in Switzerland--prevalence and correlates for the early 2010s. Swiss Med Wkly. 2014;144:w13956.
15 Murer SB , Saarsalu S , Zimmermann MB , Aeberli I . Pediatric adiposity stabilized in Switzerland between 1999 and 2012. Eur J Nutr. 2014;53(3):865–75. doi:.https://doi.org/10.1007/s00394-013-0590-y
16 Cole TJ , Bellizzi MC , Flegal KM , Dietz WH . Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320(7244):1240–3. doi:.https://doi.org/10.1136/bmj.320.7244.1240
17 Cole TJ , Lobstein T . Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes. 2012;7(4):284–94. doi:.https://doi.org/10.1111/j.2047-6310.2012.00064.x
18Petrini L, Camenzind P, Hämmig O, Bopp M, eds. Gesundheit im Kanton Zürich: Band 1: Ergebnisse der Schweizerischen Gesundheitsbefragung 2012. Institut für Epidemiologie, Biostatistik und Prävention der Universität Zürich. 2014
19 Murer SB , Saarsalu S , Zimmermann J , Herter-Aeberli I . Risk factors for overweight and obesity in Swiss primary school children: results from a representative national survey. Eur J Nutr. 2016;55(2):621–9. doi:.https://doi.org/10.1007/s00394-015-0882-5
20 Mustillo S , Worthman C , Erkanli A , Keeler G , Angold A , Costello EJ . Obesity and psychiatric disorder: developmental trajectories. Pediatrics. 2003;111(4 Pt 1):851–9. doi:.https://doi.org/10.1542/peds.111.4.851
21 Hesketh K , Wake M , Waters E , Carlin J , Crawford D . Stability of body mass index in Australian children: a prospective cohort study across the middle childhood years. Public Health Nutr. 2004;7(2):303–9. doi:.https://doi.org/10.1079/PHN2003537
22 Wheaton N , Millar L , Allender S , Nichols M . The stability of weight status through the early to middle childhood years in Australia: a longitudinal study. BMJ Open. 2015;5(4):e006963. doi:.https://doi.org/10.1136/bmjopen-2014-006963
23 Kurth BM , Schaffrath Rosario A . Übergewicht und Adipositas bei Kindern und Jugendlichen in Deutschland [Overweight and obesity in children and adolescents in Germany]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2010;53(7):643–52. Article in German. doi:.https://doi.org/10.1007/s00103-010-1083-2
24 Neovius M , Janson A , Rössner S . Prevalence of obesity in Sweden. Obes Rev. 2006;7(1):1–3. doi:.https://doi.org/10.1111/j.1467-789x.2006.00190.x
25 Furnham A , Badmin N , Sneade I . Body image dissatisfaction: gender differences in eating attitudes, self-esteem, and reasons for exercise. J Psychol. 2002;136(6):581–96. doi:.https://doi.org/10.1080/00223980209604820
26Bundesamt für Statistik BFS. Gesundheitsstatistik 2014. http://www.bfs.admin.ch/bfs/portal/de/index/news/publikationen.Document.193423.pdf (accessed November 2015)
27 Cattaneo A , Monasta L , Stamatakis E , Lioret S , Castetbon K , Frenken F , et al. Overweight and obesity in infants and pre-school children in the European Union: a review of existing data. Obes Rev. 2010;11(5):389–98. doi:.https://doi.org/10.1111/j.1467-789X.2009.00639.x
28 Jeannot E , Mahler P , Elia N , Cerruti B , Chastonnay P . Sociodemographic and Economic Determinants of Overweight and Obesity for Public-school Children in Geneva State, Switzerland: A Cross-sectional Study. Int J Prev Med. 2015;6(1):39. doi:.https://doi.org/10.4103/2008-7802.156836
29 Nagel G , Wabitsch M , Galm C , Berg S , Brandstetter S , Fritz M , et al. Determinants of obesity in the Ulm Research on Metabolism, Exercise and Lifestyle in Children (URMEL-ICE). Eur J Pediatr. 2009;168(10):1259–67. doi:.https://doi.org/10.1007/s00431-009-1016-y
30 Lobstein T , Baur L , Uauy R ; IASO International Obesity TaskForce. Obesity in children and young people: a crisis in public health. Obes Rev. 2004;5(s1, Suppl 1):4–85. doi:.https://doi.org/10.1111/j.1467-789X.2004.00133.x
31 Faeh D , Braun J , Bopp M . Prevalence of obesity in Switzerland 1992-2007: the impact of education, income and occupational class. Obes Rev. 2011;12(3):151–66. doi:.https://doi.org/10.1111/j.1467-789X.2010.00793.x
32 Guessous I , Joost S , Jeannot E , Theler JM , Mahler P , Gaspoz JM , et al.; GIRAPH Group. A comparison of the spatial dependence of body mass index among adults and children in a Swiss general population. Nutr Diabetes. 2014;4(3):e111. doi:.https://doi.org/10.1038/nutd.2014.8
33 Joost S , Duruz S , Marques-Vidal P , Bochud M , Stringhini S , Paccaud F , et al. Persistent spatial clusters of high body mass index in a Swiss urban population as revealed by the 5-year GeoCoLaus longitudinal study. BMJ Open. 2016;6(1):e010145. doi:.https://doi.org/10.1136/bmjopen-2015-010145
34 Moser A , Panczak R , Zwahlen M , Clough-Gorr KM , Spoerri A , Stuck AE , et al.; Swiss National Cohort. What does your neighbourhood say about you? A study of life expectancy in 1.3 million Swiss neighbourhoods. J Epidemiol Community Health. 2014;68(12):1125–32. doi:.https://doi.org/10.1136/jech-2014-204352
35 Whitaker RC , Dietz WH . Role of the prenatal environment in the development of obesity. J Pediatr. 1998;132(5):768–76. doi:.https://doi.org/10.1016/S0022-3476(98)70302-6
36 Gale CR , Martyn CN , Kellingray S , Eastell R , Cooper C . Intrauterine programming of adult body composition. J Clin Endocrinol Metab. 2001;86(1):267–72.
37 Gillman MW , Rifas-Shiman SL , Camargo CA, Jr , Berkey CS , Frazier AL , Rockett HR , et al. Risk of overweight among adolescents who were breastfed as infants. JAMA. 2001;285(19):2461–7. doi:.https://doi.org/10.1001/jama.285.19.2461
38 Lindsay AC , Sussner KM , Kim J , Gortmaker S . The role of parents in preventing childhood obesity. Future Child. 2006;16(1):169–86. doi:.https://doi.org/10.1353/foc.2006.0006
39 Muckelbauer R , Libuda L , Clausen K , Toschke AM , Reinehr T , Kersting M . Immigrational background affects the effectiveness of a school-based overweight prevention program promoting water consumption. Obesity (Silver Spring). 2010;18(3):528–34. doi:.https://doi.org/10.1038/oby.2009.270
40 Staub K , Rühli FJ , Woitek U , Pfister C . BMI distribution/social stratification in Swiss conscripts from 1875 to present. Eur J Clin Nutr. 2010;64(4):335–40. doi:.https://doi.org/10.1038/ejcn.2010.7
DF conceived the study and assisted in data analysis, design of figures and tables and writing. AP mainly performed statistical analyses, designed tables and figures and wrote the manuscript. JB assisted in data modelling and analysis and writing of the Methods section. MB and KS added important background knowledge and improved the manuscript by repeated readings and rephrasing as well as critical discussions of the intellectual content. All authors contributed to the final version of the manuscript.
No financial support and no other potential conflict of interest relevant to this article was reported.