Basic concepts of heart-lung interactions during mechanical ventilation
DOI: https://doi.org/10.4414/smw.2017.14491
Martin R.
Grüblera, Olivier
Wiggera, David
Bergerb, Stefan
Bloechlingerab
aDepartment of Cardiology, Inselspital, Bern University Hospital, University of Bern, Switzerland
bDepartment of Intensive Care Medicine, Inselspital, Bern University Hospital, University of Bern, Switzerland
Summary
Critically ill patients with the need for mechanical ventilation show complex interactions between respiratory and cardiovascular physiology. These interactions are important as they may guide the clinician’s therapeutic decisions and, possibly, affect patient outcome. The aim of the present review is to provide the practicing physician with an overview of the concepts of heart-lung interactions during mechanical ventilation. We outline the basic cardiac and respiratory physiology during spontaneous breathing and under mechanical ventilation. The main focus is on the interaction between positive pressure ventilation and its effects on right and left ventricular pre- and afterload and ventricular interdependence. Further we discuss different modalities to assess volume responsiveness, such as pulse pressure variation. We aim to familiarise the reader with cardiovascular side effects of mechanical ventilation when experiencing weaning problems or right heart failure.
Abbreviations
- ARDS
-
acute respiratory distress syndrome
- CPAP
-
continuous positive airway pressure
- CCW
-
compliance of the chest wall
- CL
-
compliance of the lung
- CRS
-
compliance of the respiratory system
- COPD
-
chronic obstructive pulmonary disease
- DAP
-
diastolic arterial pressure
- EDP
-
end-diastolic pressure
- EDV
-
end-diastolic volume
- FRC
-
functional residual capacity
- ICU
-
intensive care unit
- LAPm
-
mean left atrial pressure
- mPAP
-
mean pulmonary artery pressure
- ITP
-
intrathoracic pressure
- MSFP
-
mean systemic filling pressure
- PAL
-
alveolar pressure
- PAOP
-
pulmonary artery occlusion pressure
- PAP
-
pulmonary artery pressure
- PEEP
-
positive end expiratory pressure
- PPV
-
pulse pressure variation
- PPER
-
pericardial pressure
- PPL
-
pleural pressure
- PSUR
-
surrounding pressure
- PTM
-
transmural pressure
- PTP
-
transpulmonary pressure
- PVR
-
pulmonary vascular resistance
- RAP
-
right atrial pressure
- RAPTM
-
right atrial transmural pressure
- RVR
-
resistance to venous return
- ΔVao
-
respiratory variation in aortic flow velocity
- SAP
-
systolic arterial pressure
- SPV
-
systolic pressure variation
- SVV
-
stroke volume variation
Introduction
The cardiorespiratory system provides oxygen for the whole organism. Therefore, by a complex interplay, heart and lungs work as a functional unit. Three centuries ago, the English physiologist Stephen Hales observed that the level of the blood column in a glass tube inserted into the carotid artery of a horse varied cyclically with respiration [1]. This was a first recognition of the mechanical interplay between the respiratory and cardiovascular systems, nowadays referred to as heart-lung or cardiorespiratory interactions, which comprise the effects of respiration on circulation. In the second half of the 19th century, the relevance of pleural pressure was recognised and henceforward phenomena of cardiorespiratory interaction such as pulsus paradoxus elicited intense debates [2]. The need for oxygen-enriched positive pressure breathing at high altitude for fighter pilots in the Second World War and the invention of right-heart catheterisation facilitated research programmes intended to gain a more profound understanding of heart-lung interactions [3, 4]. Subsequent studies described a drop in cardiac output during forced spontaneous inspiration and depression of right ventricular function under positive pressure ventilation [5–8]. Besides the direct mechanical interdependence between lung, heart and circulation, neurally mediated phenomena, such as respiratory sinus arrhythmia, or effects of altered gas exchange (e.g., hypoxic and hypercapnic pulmonary vasoconstriction) in the context of lung disease or high altitude exposure can critically derange cardiorespiratory interplay [9–11].
In this review we focus on the mechanical interaction between the lung and the heart, mainly with respect to pre- and afterload. An understanding of this interaction is crucial in the care of ventilated patients, as mechanical ventilation can compromise cardiac function and haemodynamic stability. The understanding of mechanical heart-lung interactions allows, within the concept of functional hemodynamic monitoring and with certain limits, to predict a patient’s response to a supportive treatment like positive pressure ventilation, volume expansion or administration of vasoactive drugs [12]. We outline the physiological principles of heart-lung interactions and highlight specific clinical applications and pitfalls.
Basics of respiratory and cardio-circulatory physiology
In a simplified view, the human circulatory system consists of two main components: the circuit and the pump. The circuit represents the systemic vessel tree, including arterial resistance and venous capacitance vessels. The right and left ventricles are the main constituents of the pump. They work in parallel, since both are enclosed by the pericardium, but pump in series, connected by the pulmonary circulation. Heart-lung interactions occur because the heart is encompassed by the lungs in the juxtacardiac fossa and all are encased within the rigid chest wall. The heart acts, therefore, as a pressure chamber within another pressure chamber [13]. The compliance of the lung (CL) and chest wall (CCW), as well as the compliance and filling of intrathoracic blood vessels and heart chambers, modify the effects of lung volume, alveolar (PAL), pleural (PPL) and pericardial pressure (PPER) on cardio-circulatory function and vice versa.
Intracavitary and transmural pressures
Pressure measurements with fluid-filled catheters in the clinical setting are not absolute, but depend on the chosen zero level. The zero level is, by convention, the right atrium, and atmospheric pressure serves as zero reference pressure [14]. This practice carries consequences for heart-lung interactions, as it correctly measures pressures outside the thorax, but introduces an error when intrathoracic pressures are assessed. In the thorax, the surrounding pressure is not atmospheric, but the PPL. Changes in PPL relative to atmospheric pressure over the respiratory cycle cyclically affect the gradient for venous return and preload, as well as afterload [15, 16].
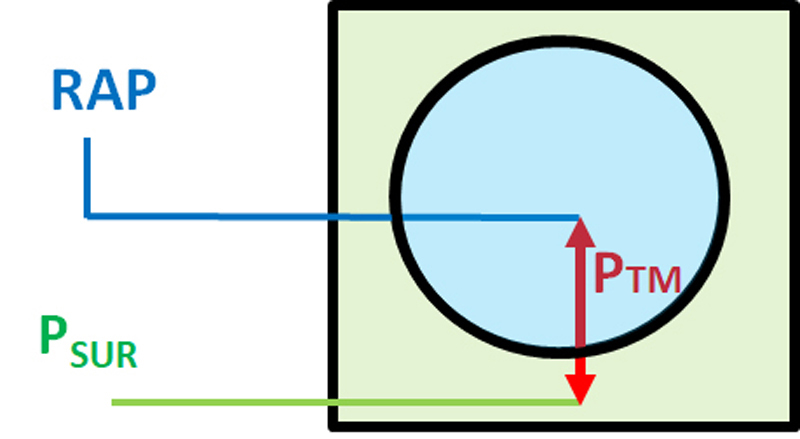
The intracavitary pressure, for example, of the right atrium, is the pressure measured against the atmosphere (right atrial pressure, RAP), that is, against the zero reference. The transmural pressure (PTM) refers to the pressure difference between the inside of a cavity (relative to atmosphere) and the surrounding outside (PSUR, relative to atmosphere). For the right atrium, the transmural pressure (RAPTM) would therefore be: RAPTM = RAP ˗ PPL (fig. 1) [17]. The PTM is the actual working pressure that, together with chamber compliance, defines the filling and dimension of the heart chambers and blood vessels (fig. 1). Within the thorax, PSUR for the heart chambers is considered to be the PPER, PSUR for intrathoracic venous vessels is considered the PPL [18, 19]. For convenience, we assume that PPL and PPER equal intrathoracic pressure (ITP), even though ITP is not homogeneously transmitted throughout the thorax [20]. Diseases can severely affect local PSUR that can be decoupled from ITP (e.g. pericardial effusion, constrictive pericarditis, pleural effusion) [21]. In clinical practice PPL can be approximated by measuring the oesophageal pressure with an air-filled balloon in the oesophagus [22]. As a convention, in order to eliminate cyclic respiratory swings of pressures, pressure measurements are taken at end-expiration, even though this is debatable [15, 23].
Chest wall, lungs and intrathoracic pressures
The lungs, surrounded by the pleura, are enclosed by the chest wall and the diaphragm. The two pleural layers ensure mechanical coupling of the lung to the chest wall. PPL is negative in spontaneous breathing and acts as surrounding pressure of the lung and cardiac structures (see previous subsection). The transpulmonary pressure (PTP = PAL ˗ PPL) defines the lung volume, depending on the compliance of the lung within the chest. Lung (CL) and chest wall compliance (CCW) define the total compliance of the respiratory system (1/CRS = 1/CL + 1/CCW) [24]. During spontaneous inspiration, PPL becomes more negative through the contraction of the diaphragm and accessory respiratory muscles and end-inspiratory lung volume is defined by PPL and CRS, since PAL equals atmospheric pressure, assuming the vocal cords are open. Exhalation is mediated passively by elastic recoil forces of the lung.
Blood flow through the lungs
To allow adequate oxygen and carbon dioxide exchange, blood flow through the lungs must match ventilation. Blood flow through the lungs depends on the driving pressure (mean pulmonary artery pressure [mPAP] – mean left atrial pressure [LAPm]) and pulmonary vascular resistance (PVR) [25]. With use of a pulmonary artery catheter, LAPm can be approximated by measuring pulmonary artery occlusion pressure (PAOP). The resistance is increased by vasoconstriction as, for example, in hypoxic (Euler-Lilijestrand reflex [26]) or hypercapnic pulmonary vasoconstriction [11]. As pulmonary vessels have a much higher compliance than systemic vessels, they are compressible and act as Starling resistors. A vessel working as Starling resistor changes its diameter and the related resistance to flow according to its surrounding pressure, comparable to a collapsible rubber tube. Therefore, blood flow through the pulmonary vasculature depends on PSUR [27, 28]. Increased extravascular pressure (increased PAL or PPL) diminishes transmural pulmonary vascular pressure, resulting in an increased PVR [29]. The lowest PVR during the respiratory cycle is found at resting end-expiration, when the lung is at its functional residual capacity (FRC) and where the resistance of alveolar vessels equals the resistance of extra-alveolar vessels [30]. A conceptual description of pulmonary blood flow based on driving pressure and PAL, which divided the lungs into different zones, was introduced by J.B. West [31]. In the upright healthy person, zone 2 (PAP > PAL > LAP) and 3 (PAP > LAP > PAL) conditions can be found. Zone 3 conditions are characterised by continuous blood flow, since PTM along the vascular bed is always positive. In areas with zone 2 conditions, PTM becomes negative at the capillary level and vessel collapse occurs. Blood flow is regulated by the intermittent collapse of the vessel, which depends on respiratory fluctuations of PAL. Zone 1 conditions (PAL > PAP > LAP) with no vascular blood flow can be observed in the lung apex of healthy upright subjects (for review see [32]). West’s seminal animal studies utilised a continuous-flow pump setup. Whether the pulmonary pressure-flow relationship with pulsatile blood flow is correctly depicted by West’s concept remains currently uncertain.
Effects of mechanical ventilation on intrathoracic pressure
During the inspiratory phase of mechanical ventilation the respirator delivers a tidal volume through the artificial airway to the lungs leading to positive PAL and PPL. Recumbency and anaesthesia diminish FRC [33]. The change in PAL and PPL for a given tidal volume will depend on CRS, as described above. The lower the CRS, the lower is the transmission of airway pressure to the pleural space. Stiff respiratory systems, such as in acute respiratory distress syndrome (ARDS), will therefore have less heart-lung interactions than compliant systems as in chronic obstructive pulmonary disease (COPD) [21]. With the application of positive end-expiratory pressure (PEEP) and the absence of spontaneous breathing efforts, PPL is positive throughout the respiratory cycle, whereas in unforced spontaneous breathing, PPL always remains negative. The physiological consequences of these changes in PPL and PTP are manifold: (i) elevated PAL combined with the recumbent position alters pulmonary blood flow by creating lung areas with zone 1 conditions (compression of alveolar vessels) and increasing the proportion of areas with zone 2 conditions, causing increased PVR and dead space ventilation with loss of FRC; (ii) increased ITP reduces PTM of large intrathoracic blood vessels as venae cavae and thoracic aorta, thereby diminishing intrathoracic blood volume; (iii) ITP is transmitted to the pericardium in the cardiac fossa where the heart is trapped and exposed to pressure elevation. Chamber compression with lower PTM values result. As RAP is elevated with positive ITP, venous return goes down (see section “Venous return and ventricular preload” below) [34, 35]. Profound and sometimes abrupt cardio-circulatory effects with positive pressure breathing need to be expected and patients appropriately monitored. High airway pressures may even mimic cardiac tamponade.
Determinants of cardiac function
The pump work of the heart has one major goal: to keep cardiac output, and therefore oxygen delivery, at a level to meet the body’s oxygen consumption. Cardiac output must be quickly variable in response to altered oxygen demand as in physical activity or illness. It is determined by the heart rate and stroke volume. Stroke volume is the amount of blood that is expelled from the left ventricle to the systemic circulation with each heartbeat. Averaged over several seconds to minutes, left ventricular stroke volume equals right ventricular stroke volume. Stroke volume itself depends on ventricular myocardial contractility, and ventricular preload and afterload.
Venous return and ventricular preload
The law of mass conservation demands that the heart can only pump out what it is fed with [36]. This statement redirects the ever present focus in medicine and cardiology from the left sided heart chambers and the arterial tree to the right sided heart chambers and the venous system. To approach and understand cardio-circulatory physiology and heart-lung interactions it is essential to become familiar with determinants of venous return and the functioning of the right ventricle.
Venous return curves
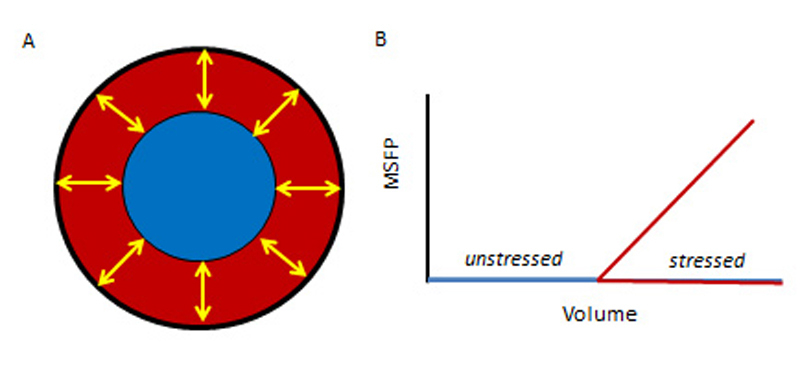
Roughly 70% of the blood volume resides within the veins (also called capacitance vessels) as a reserve pool [37]. Most of this blood volume resides in the vessels at near zero PTM (fig. 2), referred to as unstressed. The blood volume that creates positive PTM in the systemic circuit is named stressed volume and is represented by the mean systemic filling pressure (MSFP) [37–39], the elastic recoil pressure generated by the systemic vessel tree around the stressed volume [38, 41]. MSFP can be measured in circulatory standstill and is therefore independent of myocardial properties [42]. Expansion or reduction of stressed volume by change of total intravascular volume and recruitment or derecruitment of unstressed volume through intensified or alleviated vessel tone will influence MSFP [39, 43, 44].
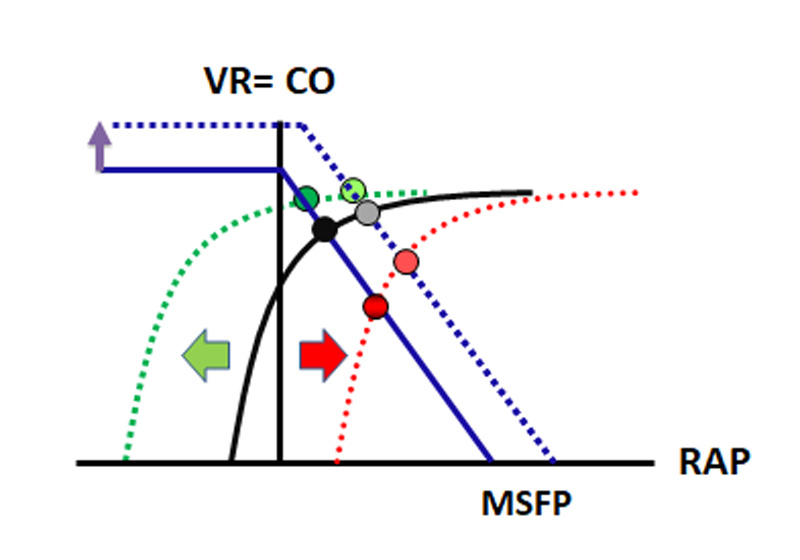
The return of blood to the heart must equal cardiac output. Venous return was first described by Arthur Guyton as VR = (MSFP ˗ RAP) / RVR, where VR is venous return and RVR is resistance to venous return [45, 46] (see fig. 3, blue line). MSFP as upstream and RAP as downstream pressure [48] for venous return create the pressure gradient necessary to overcome the resistance to VR [39, 49]. MSFP is considered to be constant throughout the cardiac cycle due to the large compliance of the vessel system and is assumed to be unaltered during the respiratory cycle [36, 37, 50–52]. This has been challenged, however [39, 53–55].
The backpressure role of RAP is crucial for the understanding of heart-lung interactions [50, 52, 56, 57], but has caused considerable controversy over the usefulness of Guyton’s model [58–60]. We have recently shown that increases in RAP lower venous return and consequently cardiac output [48]. In the classic view, RAP is primarily seen as the surrogate for right ventricular preload, and one would expect higher cardiac output with higher RAP [36, 42, 45, 61, 62]. How this can be explained is outlined below.
Contractility and the Starling curve
Contractility describes the intrinsic ability of the myocardium to generate force and to contract. It is regulated by the Ca2+ concentration in myocytes and the transfer of Ca2+ ions from the sarcoplasmic reticulum to the cytoplasm and vice versa. Availability of Ca2+ ions is tightly regulated by the sympathetic nervous system via β1-adrenoceptors. Contractility can be augmented therapeutically by β1-agonists such as dobutamine and by drugs that either sensitise contractile proteins for Ca2+ ions, e.g., levosimendan, or augment intracellular cyclic adenosine monophosphate (cAMP) levels, e.g., milrinone [63–65]. A raise in heart rate per se can also increase contractility (Bowditch effect) [66, 67]. Contractility is load dependent. Afterload elevation increases contractility (Anrep effect) and raising preload recruits contractile reserves, in accordance with the Starling’s law of the heart [68–70]. Whether there is a direct effect of mechanical ventilation on myocardial contractility is unclear. The application of PEEP may negatively affect coronary perfusion, but PEEP levels up to 15 cm H2O do not seem to worsen myocardial contractility or stroke work [71–75]. From a clinical intensivist’s perspective, the direct effects of mechanical ventilation on contractility appear far less important than the ones on pre- and afterload.
Starling’s law of the heart states that myocardial work varies with the initial length of the cardiomyocytes [76]. Pre-stretching of sarcomeres results in a more vigorous contraction up to a maximum effect whereupon further stretching will no longer increase, but possibly reduce, myocardial work [77]. In healthy subjects, this mechanism provides a beat-by-beat adaption of ventricular output (stroke volume) to ventricular input (filling or preload). This must be kept in mind when interpreting Starling curves, which unintentionally suggest that RAP acts as right ventricular preload. Study of Patterson’s and Starling’s original experiment makes it apparent that it was not RAP that was primarily altered, but venous return. RAP rose as a result of more volume in the right atrium due to increased venous return, and RAP rose more rapidly when ventricular contractile reserve was reached [69]. We therefore point out that in the Starling curve, RAP or central venous pressure do not reflect a pure preload signal, but the node of interaction between cardiac function and VR function (see fig. 3, black dot) [14, 76]. In addition, Starling used an isolated heart model that ignores the surrounding pressures of the heart and circuit within the thorax. This will be discussed below.
Combination of venous return and the Starling curve: a graphical solution
Guyton superimposed the Starling curve on the venous return curve (fig. 3) [78]. This graphical combination, even though simplified and thus challenged [79], holds large potential for helping to understand circulatory changes [61]. It integrates circuit factors, volume state and cardiac factors [39, 41]. A change in any of the aforementioned factors will result in a new equilibrium between venous return and cardiac output. As already mentioned, RAP represents the node of interaction between circuit and pump in this graphical analysis. Since RAP is measured relative to the atmosphere (see section “Intracavitary and transmural pressures” above), but the right atrium is enclosed by the pericardium, RAP is subject to large swings over the respiratory cycle, which continuously shift the cardiac function curve (fig. 3).
During spontaneous breathing, PPL becomes more negative in inspiration. RAP, measured relative to the atmosphere, drops during inspiration and creates a higher pressure gradient for venous return, resulting in higher venous return. Accordingly, in the new state the Starling curve is shifted to the left (fig. 3, green dotted line), since venous return equals cardiac output, creating a new intersection between the two curves at a lower RAP (dark green dot), but higher venous return and cardiac output. Please keep in mind that RAPTM has actually risen if PPL has been transmitted to the right atrium – we describe the function curves from a perspective outside the thorax [62].
The opposite will happen with mechanical ventilation. PPL increases with mechanical inflation of a tidal volume and is partially transmitted to the right atrium whose intracavitary pressure rises (dark red dot; the transmural pressure actually falls). The Starling curve is shifted to the right (red dotted line), cardiac output and venous return decrease. Under mechanical ventilation, right ventricular preload is mainly affected by changes in PPL, whereas left ventricular preload is mainly affected by changes in PTP [80].
The same graphical analysis can be used to assess volume responsiveness. An increase in cardiac output is considered a positive response to a volume challenge. Rapidly infusing a crystalloid solution will elevate MSFP and shift the venous return curve to the right (fig. 3; dotted blue line). A heart with the intersection (RAP) of the venous return curve and the Starling curve in the steep part of Starling curve (red dotted line) will exhibit a profounder positive response to a volume challenge than a heart with the intersection in the flat part (green dotted line). In the latter case, the volume challenge produces a considerable increase in RAP with hardly any increase in venous return or cardiac output. It should be kept in mind that a healthy heart normally works on the steep part of the Starling curve. Volume responsiveness is therefore a normal phenomenon. In the intensive care unit (ICU), only around 50 to 60% of patients are volume responsive [81]. The explanation is often right ventricular failure [82].
Ventricular afterload
Afterload is defined as the force opposing ventricular ejection of blood [83]. Afterload can be approached by assessing ventricular wall tension or vascular resistance and impedance [84]. In order to account for the differences in geometry and muscle mass and different functions of the right and left ventricles, we discuss afterload separately for the two ventricles.
Left ventricular afterload
The left ventricle has to generate high pressures for pulsatile ejection of blood into the arterial system. In the absence of left ventricular outflow tract obstruction or aortic valve stenosis the load on the ventricle is determined by the arterial vasculature. The work the ventricle has to provide depends on the aortic elastance (∆P/∆V), the ability of the aorta to temporarily accommodate and release a proportion of each stroke volume, and the overall resistance of the arterial vessel tree [85]. The stiffer the aorta, as, for example, in older hypertensive subjects, and the higher the arterial resistance, the bigger the work the left ventricle has to deliver to maintain a certain cardiac output.
In a healthy subject, subtle ITP swings during spontaneous respiration cause only minor cyclic changes in left ventricular afterload, but forced spontaneous inspiration or a Müller manoeuvre can considerably affect cardiac output [8]. During mechanical ventilation by inflation of the tidal volume or by application of PEEP, ITP and, concomitantly PPER, rise. PTM of the left ventricle and, to a lesser extent, of the intrathoracic part of the aorta, fall while PTM in the abdominal aorta remains higher, resulting in a net afterload reduction and facilitating blood flow from the intrathoracic to the abdominal compartment. This seems to be mainly mediated by changes in PPL [80]. With left ventricular afterload reduction, application of continuous positive airway pressure (CPAP) in spontaneously breathing patients, or pressure support ventilation with PEEP in sedated patients, can be a valuable supportive measure in the treatment of acutely decompensated left ventricular failure [86].
Right ventricular afterload
Whereas the left ventricle pumps blood into a high pressure system with low compliance, the right ventricle ejects the same amount of blood into the highly compliant pulmonary vasculature at low pressures. The right ventricle serves, therefore, more as a flow generator than a pressure generator [87, 88]. Alterations in right ventricular outflow are mainly mediated through changes in ITP [80, 89]. ITP changes can strongly affect transmural pulmonary vascular pressure and PVR, and thereby right ventricular afterload. PVR is commonly assessed in clinical practice by use of the equation PVR = (mPAP ˗ PAOP) / CO, where CO is cardiac output, describing a continuous flow system. Since the right ventricle works as a pulsatile pump and the pulmonary vasculature is highly distensible, the pulmonary vascular elastance or impedance seems a more accurate measure of right ventricular afterload [90, 91]. During spontaneous breathing, inspiration associated with negative PPL distends the pulmonary vasculature and therefore reduces right ventricular afterload. During mechanical ventilation, tidal breathing increases PPL, reduces transmural pulmonary vascular pressure and consequently elevates right ventricular afterload. Pulmonary vascular resistance during mechanical ventilation rises mostly in those areas of the lung where zone 1 and 2 conditions, with negative PTM and intermittent or continuous pulmonary vascular collapse, are created (see section “Blood flow through the lungs” above). Right ventricular afterload is highly sensitive to cyclic tidal inflation with positive pressure, and for this reason mechanical ventilation may elicit right ventricular failure, especially in individuals with pre-existing right ventricular dysfunction or severe hypoxic pulmonary vasoconstriction in the context of ARDS [80, 89, 92–95]. Acute elevations of afterload are poorly tolerated by the right ventricle as compared with the left ventricle, which possesses much higher contractile reserves [96]. The lowest PVR during the respiratory cycle is found at end-expiration at FRC. Below and above FRC, the PVR rises [30].
Interplay between the left and the right ventricles
Anatomical prerequisites
The heart chambers lie within the pericardium, limiting the total blood volume that the heart as a whole can contain [19, 22, 88]. The right and left ventricles differ greatly in their anatomical structure and mode of operation. The left ventricle is spherical, with a helical arrangement of muscle fibres from the apex to the base and obliquely oriented muscle fibre bundles from the inside to the outside, which allows the generation of high pressures with good efficiency [97–99]. The right ventricle is partially wrapped around the left ventricle. Its anatomy, with a thin free wall, is not suitable for efficient work at high pressures, but is adapted to the low resistance pulmonary vasculature [88]. Contraction of the interventricular septum, which mostly consists of muscle fibres attributed to the left ventricle, substantially supports right ventricular ejection [100, 101]. This evident structural dependency of the two ventricles is clinically relevant. Dyssynchronous or absent contraction of the septum, as with left bundle-branch block, with right ventricular pacing or following myocardial infarction, will affect the performance of not only the left but also the right ventricle [102–104].
Ventricular interdependence
The right and left ventricles work as serial pumps connected by the pulmonary and systemic vasculature. Through their electrical and mechanical synchronisation, they work in parallel within the pericardial confinement. Right ventricular stroke volume is ejected into the pulmonary vasculature and provides the left ventricular preload; hence, the left ventricle can only be as good as the right ventricle [87]. However, beyond this sequential dependency, there is also a parallel mechanical coupling of the ventricles referred to as ventricular interdependence [105]. Because of the shared septum and the pericardial constraint, the diastolic pressure of one ventricle directly effects the diastolic filling of the other [106]. When right ventricular volume is increased, left ventricular filling declines. This phenomenon can be observed in situations with right ventricular afterload elevation (e.g., pulmonary embolism, pulmonary hypertension) or as a cyclical respiratory physiological phenomenon that can be aggravated by disease (e.g., pericardial effusion) or mechanical ventilation. Even in healthy individuals, spontaneous respiration affects ventricular filling to a small extent, but forced breathing efforts can make ventricular interdependency overt. Under normal circumstances, end-diastolic ventricular volume (EDV) and pressure (EDP) change in opposite directions in the left and right ventricle during the respiratory cycle. Undulating ventricular filling during respiration results in changing stroke volumes of the left and right ventricles with each heartbeat, again in opposite directions. On average, the sum of stroke volumes of the right ventricle equals left ventricular output, but beat by beat stroke volumes vary with the respiratory cycle. This is possible because the pulmonary vasculature and venous capacitance vessels are very compliant and able to transiently accommodate volume surplus [107]. Important clinical examples of interventricular dependence are pericardial tamponade or status asthmaticus with an exaggerated inspiratory drop in peripheral arterial pressure (pulsus paradoxus) during spontaneous respiration. This drop in arterial pressure is caused by a sudden increase in right ventricular EDV during inspiration that impairs left ventricular filling and stroke volume.
Heart-lung interactions: clinical application and pitfalls
The complex physiology of cardiopulmonary interplay makes heart-lung interactions ever present in the ventilated patient. They are clinically relevant because mechanical ventilation can provoke cardiovascular instability [108] and heart-lung interactions offer possibilities to predict reactions of the cardiovascular system to treatment modalities, especially volume expansion, within the framework of functional haemodynamic monitoring [109].
Ventilator-induced right ventricular dysfunction
The right ventricle is particularly strained by mechanical ventilation, as venous return and its preload are reduced, mediated by elevation of PPL, while afterload is mechanically increased as reduction of the PTM of the pulmonary vasculature increases resistance [89]. In patients with ARDS, these effects are aggravated by hypoxic or hypercapnic pulmonary vasoconstriction, pulmonary microthrombosis, changes in West zones and lung derecruitment [110], all leading to pulmonary hypertension and a worse prognosis [111]. Despite the widespread use of low tidal volume ventilation strategies [112], which may mitigate the mechanical effects on the right ventricle due to lower airway pressures, acute cor pulmonale in patients with ARDS is still highly prevalent (around 25%) and is associated with poor prognosis [93, 108]. The risk for developing acute cor pulmonale becomes higher with worse oxygenation, hypercapnia, high ventilator pressures and pneumonia as the cause of ARDS [113]. Prone positioning can lead to improved right ventricular function via recruitment of dorsal lung areas and vasculature, resulting in reduced right ventricular afterload [114, 115]. Mechanical ventilation is a lifesaving procedure in ARDS. Besides the negative effects discussed, it may improve pulmonary vasoconstriction by improving gas exchange and recruitment. The effects of mechanical ventilation are often unpredictable and highly dynamic. The ventilator strategy should not be set by guidelines or gas exchange alone, but needs to take into account right ventricular function in order to determine the optimal cardiopulmonary functional state. Ventilated patients prone to right ventricular failure need advanced monitoring in order to recognise cardiopulmonary deterioration early. An arterial and central venous line are mandatory. Clinical awareness of right ventricular failure needs to be high. Echocardiography [116] and/or a pulmonary artery catheter [80] – despite criticism a safe device for monitoring right ventricular function and PVR in experienced hands [25, 117] – are suitable tools for evaluating the right ventricle. Measurements of mixed venous oxygenation allow assessment of pulmonary shunting and adequacy of oxygen delivery despite impaired oxygenation through the lung [118]. Optimal lung recruitment can lower right ventricular afterload and improve oxygenation, and can be optimised by measuring oesophageal pressure as a surrogate of PPL [119].
Patients with exacerbations of COPD or status asthmaticus are also prone to develop acute cor pulmonale during mechanical ventilation. The high CL facilitates pressure transmission from the lung to the pulmonary vasculature. The high airway resistance leads to incomplete exhalation with air trapping, dynamic overinflation and auto-PEEP [120, 121], resulting in reduced right ventricular preload and elevated afterload. Auto-PEEP is primarily independent of mechanical ventilation and is caused by the narrowed airway and tachypnoea. It can be minimised by careful ventilator settings. Low tidal volume and low respiratory rates with small inspiration to expiration ratios may prevent auto-PEEP. Often, sedation and tolerance of respiratory acidosis are necessary and monitoring of cardiopulmonary function is needed as described for ARDS. Recognition of right ventricular failure and afterload dependence during mechanical ventilation is of paramount importance, as it can lead to left ventricular preload dependence with pulse pressure variation (PPV, see below) [122, 123]. In such a context, volume therapy may be detrimental owing to ventricular interdependence if the cause PPV is not carefully looked for.
The extent of heart-lung interactions and cardiovascular compromise is comparable between different modes of ventilation, in the case of similar mean airway pressures and tidal volumes [124–126]. We have recently shown beneficial effects on right ventricular function for neurally adjusted ventilatory assist [92] in comparison with pressure support ventilation for patients at the transition from controlled to assisted ventilation.
Functional haemodynamic monitoring
Assessment of preload reserve and volume responsiveness
Heart-lung interactions have been used for preload assessment based on dynamic indices in three different approaches: (i) PPV and its variants, (ii) echocardiographic assessment of the caval veins, (iii) estimation of MSFP with ventilator manoeuvres.
Volume therapy must be guided by clinical signs of inadequate tissue perfusion, such as low urinary output, altered mentation, clammy periphery and mottled skin, elevated lactate levels and the need for vasopressor agents. Positive indicators of fluid responsiveness do not justify fluid therapy by themselves [127]. Even though central venous pressure itself is a bad indicator of volume responsiveness [128], observing its reaction to a volume bolus holds valuable information about the ability of the right heart to handle volume expansion, similar to the hepatojugular reflux test.
Pulse pressure variation and its variants
The cyclic change in PPL during respiration causes RAP to rise during mechanical inspiration and fall with exhalation (fig. 4). Venous return and right ventricular stroke volume therefore drop with mechanical inspiration and rise with exhalation. This varying right ventricular stroke volume causes, with a time delay – the pulmonary transit time – the difference between systolic (SAP) and diastolic arterial pressure (DAP) in the peripheral arterial pressure curve to rise during inspiration and fall in expiration. Such varying arterial pressures are seen as indication that the heart works on the steep part of its Starling curve and could therefore be responsive to volume. Following volume expansion, an increase in cardiac output should be observed.
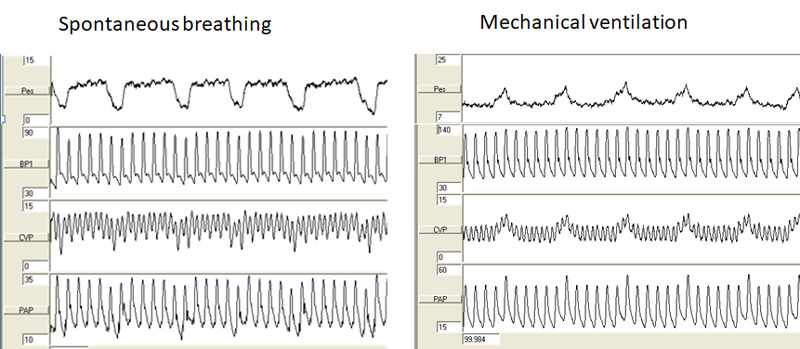
Figure 4
Respiratory pressure variations. With spontaneous breathing, increasingly negative pleural pressure during inspiration (surrogated by oesophageal pressure, left panel) is transmitted to central venous, pulmonary artery and arterial blood pressure (inspiratory drops). With mechanical ventilation, this pattern is reversed. Original pressure tracings from reference [92].
Based on this reasoning, Perel first described systolic pressure variation (SPV) as a surrogate of hypovolaemia in an animal model [129]. After use of SPV transferred to the bedside [130], the assessment was refined to stroke volume variation (SVV) [131, 132] and PPV [133, 134]. PPV, calculated as (maximum pulse pressure – minimum pulse pressure)*100/(maximum pulse pressure + minimum pulse pressure)*0.5, had particularly widespread use after Michard and colleagues showed a good prediction of fluid responsiveness in septic patients with a PPV ≥12% [135]. Its apparent simplicity may distract the clinician from several important pitfalls [136, 137]. PPV of the arterial pressure is caused by preload and stroke volume changes in the right ventricle. The passage of blood through the lung is neglected. Any factor that interferes with the pulmonary vasculature or function may therefore affect PPV [137]. PPV is influenced by any spontaneous respiratory effort [138], tidal volume (needs to be larger than 8 ml/kg, which is not current practice in lung protective ventilation) [139], respiratory rate and pulmonary transit time [140], and the CRS [141]. Absence of sinus rhythm and frequent ectopic beats render PPV unusable. Most critically ill patients do not meet the criteria for valid interpretation of PPV [142]. And in general, more than half of ICU patients are not fluid responsive [143]. Probably the most important limitation of PPV is the failing right ventricle, which also causes the arterial pressure to undulate because of smaller stroke volumes with increased afterload during mechanical inspiration [122, 123]. In order to avoid deleterious volume loading, PPV should not be seen as a marker of volume responsiveness per se [87, 89, 144], but rather as an indicator of left ventricular function depending on right ventricular stroke volume. A failure to increase cardiac output following volume expansion calls for immediate diagnostic evaluation of the right ventricle. Prerequisites for a volume challenge based on PPV are, therefore, signs of insufficient cardiac output, as explained above, continuous measurement of cardiac output during and after the volume expansion to verify fluid responsiveness, and a frequent careful evaluation of whether the patient needs volume in order to establish sufficient tissue perfusion. If cardiac output is not augmented or vasopressors decreased following a volume challenge, no further volume should be applied and if PPV is present, careful evaluation of the right ventricle is needed. Comprehensive information on PPV can be found in two reviews by Magder [136] and Sondergaard [137]. We want to point out that a negative PPV does not necessarily mean that a patient does not need volume, if a patient’s blood volume is centralised owing to adrenergic – endogenous or exogenous – vasoconstriction with concomitant insufficient tissue perfusion. Vasoconstriction shifts volume from the pool of unstressed volume to the pool of stressed volume to maintain venous return. In this case, volume expansion may allow a reduction in the dose of vasopressor agents and restoration of tissue perfusion by normalising unstressed volume and reducing vasoconstriction. Overall, volume administration should be handled restrictively, and only be applied if tissue oxygenation is critical and a positive effect on oxygen delivery can be documented.
Echocardiographic assessment of volume state
Respiratory variations of the diameters of the superior [145, 146] and inferior caval veins [147] or variations in the aortic flow velocity (ΔVao) [131] have been reported to predict fluid responsiveness in ventilated patients. In a recently published large cohort study, respiratory ΔVao had the highest sensitivity (79%) for fluid responsiveness and respiratory variations in superior vena cava diameter where most specific (84%) [143]. ΔVao may suffer from limitations similar to those of PPV. The assessment of superior vena cava diameter necessitates transoesophageal echocardiography, but is a robust measure with few validity criteria [143, 145, 146]. As the measured variable lies before the right heart, it is primarily independent of right heart function, possibly explaining its high specificity. Still, superior vena cava diameter changes depend on the amount of airway pressure change and therefore tidal volume, as we have recently shown in an animal model [39]. Overall, the accuracy of these dynamic echocardiographic predictors is modest and the same considerations regarding the need for fluid administration as for PPV apply.
Estimation of mean systemic filling pressure with respiratory manoeuvres
As cardiac output drops with increasing airway pressure, it is possible to extrapolate MSFP, that is, the pressure in the vasculature at zero blood flow, when venous return curves are constructed (analogous to fig. 3) by stepwise increases in RAP and decreasing cardiac output with increasing airway pressure. These physiological concepts were developed in animal models by Versprille [56, 148] and Pinsky [50]. Estimates of MSFP with increasing pressures in inspiratory hold manoeuvres have lately been used at the bedside [149] in cardiac [150–152] and septic ventilated ICU patients [153]. Whereas these methods have shown a good correlation with mathematical estimates of MSFP [152], we have recently shown in an experimental model that such extrapolates overestimate the standstill MSFP, as the manoeuvres themselves influence the target measure directly, possibly via hepatosplanchnic waterfalls [39]. Whether inspiration influences MSFP is an ongoing, unresolved debate [39, 54, 55, 154], which warrants caution in the application of these methods. Further research in this field of heart-lung interactions is needed. The concepts hold great clinical potential, since direct measurement of right atrial pressure and MSFP may help to guide fluid resuscitation. If volume expansion causes MSFP to raise more than RAP, the driving pressure for venous return (MSFP – RAP), and consequently venous return and cardiac output increase.
Weaning from mechanical ventilation
Weaning describes the gradual withdrawal of ventilatory support. This procedure can be seen as a cardiopulmonary stress test [13], as the work for breathing is gradually returned to the patient, while preload and afterload may rise because less airway pressure is applied. Weaning is accompanied by an increase in cardiac output [155]. In patients who fail weaning trials, left ventricular EDP has been shown to increase [156]. Mixed venous oxygenation may drop owing to a rising metabolic demand and the inability of the cardiopulmonary system to adapt [157]. Myocardial ischaemia with resulting diastolic dysfunction and pulmonary oedema may develop [158, 159]. Besides pulmonary artery catheter measurements as the gold standard [156, 157], weaning failure can be predicted by changes in levels of brain natriuretic peptide [160, 161] and increases in extravascular lung water [162]. Diastolic left ventricular dysfunction leading to increased PAOP and pulmonary oedema seems to be a crucial aspect of weaning failure. Left ventricular diastolic dysfunction is classically assessed by use of echocardiography to measure mitral valve tissue Doppler velocities or transmitral flow patterns [163, 164]. It must be kept in mind that echocardiographic assessments of diastolic function with Doppler are preload dependent and therefore influenced by PEEP and mechanical ventilation, with higher PEEP mimicking progressive diastolic dysfunction [165, 166]. Formal validation of echocardiographic diastolic function parameters during mechanical ventilation and during weaning is currently lacking.
Acute cardiogenic lung oedema
In patients with acute cardiogenic lung oedema, most commonly following acute myocardial infarction, left ventricular EDP is elevated, with subsequent elevation in PAOP and fluid extravasation from the pulmonary vasculature to the interstitium and alveoli [167]. Mechanical ventilation associated with elevated airway pressures is often the only tool to secure oxygenation in these patients. Besides its effects on gas exchange, mechanical ventilation has potentially beneficial effects on left ventricular function. It reduces left ventricular afterload (see previous section “Left ventricular afterload”) and preload by reducing venous return to the thorax and thereby lowering left ventricular EDP. Mechanical ventilation and its haemodynamic effects need to be monitored closely, since right ventricular function may also be reduced, for example, in a septal myocardial infarction, and mechanical ventilation may worsen haemodynamics. Acute cardiogenic lung oedema still carries a high mortality of 10 to 20% [168, 169]. Noninvasive ventilatory support, be it CPAP or noninvasive positive-pressure ventilation, has been shown to rapidly improve dyspnoea and acidosis, but with no convincing effect on mortality compared with oxygen therapy only [170]. We emphasise here that the underlying condition leading to acute cardiogenic lung oedema needs to be treated vigorously, by means of, for example, afterload reduction in hypertensive emergencies or percutaneous coronary intervention for acute myocardial infarction. Invasive mechanical ventilation should be introduced in unstable patients and in those who do not rapidly improve during noninvasive ventilator support in order to minimise oxygen consumption and exaggerated spontaneous respiratory efforts with its detrimental effects on haemodynamics. In the acute setting, introduction of mechanical ventilation in cardiogenic shock patients carries risks, and we recommend discussing the option of installing a temporary left ventricular assist device, such as an Impella CP®, in order to stabilise haemodynamics before intubation, especially in patients that will undergo percutaneous coronary intervention.
Obstructive sleep apnoea
In obstructive sleep apnoea, patients exhibit inspiratory muscular efforts against a closed upper airway creating a strongly negative PPL, which is transmitted to the intrathoracic large veins and the right atrium, augmenting venous return. This leads to dilation of the right ventricle accompanied by a shift of the interventricular septum towards the left ventricle and a reduction in left ventricular compliance and stroke volume (pulsus paradoxus) [171]. Patients with an impaired right ventricular function especially cannot sufficiently adapt right ventricular output to frequent and sudden increases in venous return, and are prone to right ventricular failure. Negative PPL also increases left ventricular afterload [8]. Arterial desaturation occurs during these episodes of negative PPL swings, paralleled by hypoxic pulmonary vasoconstriction. Cor pulmonale and left ventricular dysfunction are common in patients with severe obstructive sleep apnoea. Nocturnal continuous positive airway pressure (CPAP) therapy helps to keep the upper airway open, and reduces daytime sleepiness and cognitive dysfunction (for review see [172]). Whether it can improve cardiovascular comorbidities remains debatable [173]. So far no survival benefit in patients with obstructive sleep apnoea treated with CPAP could be demonstrated [174].
Conclusions
Heart-lung interactions describe the effects of changing intrathoracic pressures and lung volumes on the heart and circulation. This interplay has major consequences for the patient under mechanical ventilation, as venous return, and pre- and afterload for the right and left ventricles are dynamically influenced by mechanical ventilation. These effects are modified by the underlying lung mechanics and the circulatory state of the patient. Heart-lung interactions can potentially lead to dramatic clinical deterioration when they are not recognised during mechanical ventilation. On the other hand, they offer possibilities to dynamically assess the volume state and right heart function of a patient.
Author contributions
DB and SB contributed equally.
References
1
Sette
P
,
Dorizzi
RM
,
Azzini
AM
. Vascular access: an historical perspective from Sir William Harvey to the 1956 Nobel prize to André F. Cournand, Werner Forssmann, and Dickinson W. Richards. J Vasc Access. 2012;13(2):137–44. doi:https://doi.org/10.5301/jva.5000018.https://doi.org/10.5301/jva.5000018
2
Barr
J
. The Effects of Respiration on the Circulation; and the Pulsus Paradoxus Vel Pulsus Inspiratione Intermittens. BMJ. 1907;1(2416):913–8. doi:https://doi.org/10.1136/bmj.1.2416.913.https://doi.org/10.1136/bmj.1.2416.913
3
Swan
HJ
,
Ganz
W
. Hemodynamic monitoring: a personal and historical perspective. Can Med Assoc J. 1979;121(7):868–71.
4
Farhi
LE
. World War II and respiratory physiology: the view from Rochester, New York. J Appl Physiol (1985). 1990;69(5):1565–70.
5
Carr
DT
,
Essex
HE
. Certain effects of positive pressure respiration on the circulatory and respiratory systems. Am Heart J. 1946;31(1):53–73. doi:https://doi.org/10.1016/0002-8703(46)90391-2.https://doi.org/10.1016/0002-8703(46)90391-2
6
Otis
AB
,
Rahn
H
,
Brontman
M
,
Mullins
LJ
,
Fenn
WO
. Ballistocardiographic study of changes in cardiac output due to respiration. J Clin Invest. 1946;25(3):413–21. doi:https://doi.org/10.1172/JCI101723.https://doi.org/10.1172/JCI101723
7
Cournand
A
,
Motley
HL
,
Werko
L
. Mechanism underlying cardiac output change during intermittent positive pressure breathing (IPP). Fed Proc. 1947;6(1 Pt 2):92.
8
Buda
AJ
,
Pinsky
MR
,
Ingels
NB, Jr
,
Daughters
GT, 2nd
,
Stinson
EB
,
Alderman
EL
. Effect of intrathoracic pressure on left ventricular performance. N Engl J Med. 1979;301(9):453–9. doi:https://doi.org/10.1056/NEJM197908303010901.https://doi.org/10.1056/NEJM197908303010901
9
Yasuma
F
,
Hayano
J
. Respiratory sinus arrhythmia: why does the heartbeat synchronize with respiratory rhythm?
Chest. 2004;125(2):683–90. doi:https://doi.org/10.1378/chest.125.2.683.https://doi.org/10.1378/chest.125.2.683
10
Marshall
BE
,
Marshall
C
,
Frasch
F
,
Hanson
CW
. Role of hypoxic pulmonary vasoconstriction in pulmonary gas exchange and blood flow distribution. 1. Physiologic concepts. Intensive Care Med. 1994;20(4):291–7. doi:https://doi.org/10.1007/BF01708968.https://doi.org/10.1007/BF01708968
11
Dorrington
KL
,
Talbot
NP
. Human pulmonary vascular responses to hypoxia and hypercapnia. Pflugers Arch. 2004;449(1):1–15. doi:https://doi.org/10.1007/s00424-004-1296-z.https://doi.org/10.1007/s00424-004-1296-z
12
Pinsky
MR
,
Payen
D
. Functional hemodynamic monitoring. Crit Care. 2005;9(6):566–72. doi:https://doi.org/10.1186/cc3927.https://doi.org/10.1186/cc3927
13Tobin MJ. Effect of Mechanical Ventilation on Heart-Lung Interactions Principles and Practice of Mechanical Ventilation, Third Edition. New York: McGraw Hill; 2012 (Chapter 36).
14
Magder
S
. Right Atrial Pressure in the Critically Ill: How to Measure, What Is the Value, What Are the Limitations?
Chest. 2017;151(4):908–16.
15
Magder
S
,
Verscheure
S
. Proper reading of pulmonary artery vascular pressure tracings. Am J Respir Crit Care Med. 2014;190(10):1196–8. doi:https://doi.org/10.1164/rccm.201408-1526LE.https://doi.org/10.1164/rccm.201408-1526LE
16
Marini
JJ
,
Culver
BH
,
Butler
J
. Mechanical effect of lung distention with positive pressure on cardiac function. Am Rev Respir Dis. 1981;124(4):382–6.
17
Tyberg
JV
,
Taichman
GC
,
Smith
ER
,
Douglas
NW
,
Smiseth
OA
,
Keon
WJ
. The relationship between pericardial pressure and right atrial pressure: an intraoperative study. Circulation. 1986;73(3):428–32. doi:https://doi.org/10.1161/01.CIR.73.3.428.https://doi.org/10.1161/01.CIR.73.3.428
18
Holt
JP
,
Rhode
EA
,
Kines
H
. Pericardial and ventricular pressure. Circ Res. 1960;8(6):1171–81. doi:https://doi.org/10.1161/01.RES.8.6.1171.https://doi.org/10.1161/01.RES.8.6.1171
19
Tyberg
JV
,
Smith
ER
. Ventricular diastole and the role of the pericardium. Herz. 1990;15(6):354–61.
20
Lansdorp
B
,
Hofhuizen
C
,
van Lavieren
M
,
van Swieten
H
,
Lemson
J
,
van Putten
MJ
, et al.
Mechanical ventilation-induced intrathoracic pressure distribution and heart-lung interactions. Crit Care Med. 2014;42(9):1983–90. doi:https://doi.org/10.1097/CCM.0000000000000345.https://doi.org/10.1097/CCM.0000000000000345
21
Jardin
F
,
Genevray
B
,
Brun-Ney
D
,
Bourdarias
JP
. Influence of lung and chest wall compliances on transmission of airway pressure to the pleural space in critically ill patients. Chest. 1985;88(5):653–8. doi:https://doi.org/10.1378/chest.88.5.653.https://doi.org/10.1378/chest.88.5.653
22
Kingma
I
,
Smiseth
OA
,
Frais
MA
,
Smith
ER
,
Tyberg
JV
. Left ventricular external constraint: relationship between pericardial, pleural and esophageal pressures during positive end-expiratory pressure and volume loading in dogs. Ann Biomed Eng. 1987;15(3-4):331–46. doi:https://doi.org/10.1007/BF02584288.https://doi.org/10.1007/BF02584288
23
Kovacs
G
,
Avian
A
,
Pienn
M
,
Naeije
R
,
Olschewski
H
. Reading pulmonary vascular pressure tracings. How to handle the problems of zero leveling and respiratory swings. Am J Respir Crit Care Med. 2014;190(3):252–7.
24
Rahn
H
,
Otis
AB
, et al.
The pressure-volume diagram of the thorax and lung. Am J Physiol. 1946;146(2):161–78.
25
Naeije
R
. Pulmonary vascular resistance. A meaningless variable?
Intensive Care Med. 2003;29(4):526–9. doi:https://doi.org/10.1007/s00134-003-1693-3.https://doi.org/10.1007/s00134-003-1693-3
26
Lumb
AB
,
Slinger
P
. Hypoxic pulmonary vasoconstriction: physiology and anesthetic implications. Anesthesiology. 2015;122(4):932–46. doi:https://doi.org/10.1097/ALN.0000000000000569.https://doi.org/10.1097/ALN.0000000000000569
27
Permutt
S
,
Bromberger-Barnea
B
,
Bane
HN
. Alveolar pressure, pulmonary venous pressure, and the vascular waterfall. Med Thorac. 1962;19:239–60.
28
Permutt
S
,
Riley
RL
. Hemodynamics of collapsible vessels with tone: the vascular waterfall. J Appl Physiol. 1963;18:924–32.
29
West
JB
,
Dollery
CT
,
Naimark
A
. Distribution of blood flow in isolated lung; relation to vascular and alveolar pressures. J Appl Physiol. 1964;19:713–24.
30
Whittenberger
JL
,
McGREGOR
M
,
Berglund
E
,
Borst
HG
. Influence of state of inflation of the lung on pulmonary vascular resistance. J Appl Physiol. 1960;15:878–82.
31
West
JB
. Understanding pulmonary gas exchange: ventilation-perfusion relationships. J Appl Physiol (1985). 2004;97(5):1603–4.
32
West
JB
. Blood flow to the lung and gas exchange. Anesthesiology. 1974;41(2):124–38. doi:https://doi.org/10.1097/00000542-197408000-00004.https://doi.org/10.1097/00000542-197408000-00004
33
Froese
AB
,
Bryan
AC
. Effects of anesthesia and paralysis on diaphragmatic mechanics in man. Anesthesiology. 1974;41(3):242–55. doi:https://doi.org/10.1097/00000542-197409000-00006.https://doi.org/10.1097/00000542-197409000-00006
34
Feihl
F
,
Broccard
AF
. Interactions between respiration and systemic hemodynamics. Part I: basic concepts. Intensive Care Med. 2009;35(1):45–54. doi:https://doi.org/10.1007/s00134-008-1297-z.https://doi.org/10.1007/s00134-008-1297-z
35
Feihl
F
,
Broccard
AF
. Interactions between respiration and systemic hemodynamics. Part II: practical implications in critical care. Intensive Care Med. 2009;35(2):198–205. doi:https://doi.org/10.1007/s00134-008-1298-y.https://doi.org/10.1007/s00134-008-1298-y
36
Magder
S
. Point: the classical Guyton view that mean systemic pressure, right atrial pressure, and venous resistance govern venous return is/is not correct. J Appl Physiol (1985). 2006;101(5):1523–5. doi:https://doi.org/10.1152/japplphysiol.00698.2006.https://doi.org/10.1152/japplphysiol.00698.2006
37
Magder
S
. Volume and its relationship to cardiac output and venous return. Crit Care. 2016;20(1):271. Correction in: Critical Care. 2017;21:16. doi:https://doi.org/10.1186/s13054-016-1438-7.https://doi.org/10.1186/s13054-016-1438-7
38
Magder
S
,
De Varennes
B
. Clinical death and the measurement of stressed vascular volume. Crit Care Med. 1998;26(6):1061–4. doi:https://doi.org/10.1097/00003246-199806000-00028.https://doi.org/10.1097/00003246-199806000-00028
39
Berger
D
,
Moller
PW
,
Weber
A
,
Bloch
A
,
Bloechlinger
S
,
Haenggi
M
, et al.
Effect of PEEP, blood volume, and inspiratory hold maneuvers on venous return. Am J Physiol Heart Circ Physiol. 2016;311(3):H794–806. doi:https://doi.org/10.1152/ajpheart.00931.2015.https://doi.org/10.1152/ajpheart.00931.2015
40
Funk
DJ
,
Jacobsohn
E
,
Kumar
A
. The role of venous return in critical illness and shock-part I: physiology. Crit Care Med. 2013;41(1):255–62. doi:https://doi.org/10.1097/CCM.0b013e3182772ab6.https://doi.org/10.1097/CCM.0b013e3182772ab6
41
Berger
D
,
Moller
PW
,
Takala
J
. Reply to “Letter to the editor: Why persist in the fallacy that mean systemic pressure drives venous return?”. Am J Physiol Heart Circ Physiol. 2016;311(5):H1336–7. doi:https://doi.org/10.1152/ajpheart.00622.2016.https://doi.org/10.1152/ajpheart.00622.2016
42
Henderson
WR
,
Griesdale
DE
,
Walley
KR
,
Sheel
AW
. Clinical review: Guyton--the role of mean circulatory filling pressure and right atrial pressure in controlling cardiac output. Crit Care. 2010;14(6):243. doi:https://doi.org/10.1186/cc9247.https://doi.org/10.1186/cc9247
43
Magder
S
,
Vanelli
G
. Circuit factors in the high cardiac output of sepsis. J Crit Care. 1996;11(4):155–66. doi:https://doi.org/10.1016/S0883-9441(96)90026-X.https://doi.org/10.1016/S0883-9441(96)90026-X
44
Bloch
A
,
Berger
D
,
Takala
J
. Understanding circulatory failure in sepsis. Intensive Care Med. 2016;42(12):2077–9. doi:https://doi.org/10.1007/s00134-016-4514-1.https://doi.org/10.1007/s00134-016-4514-1
45
Guyton
AC
,
Lindsey
AW
,
Abernathy
B
,
Richardson
T
. Venous return at various right atrial pressures and the normal venous return curve. Am J Physiol. 1957;189(3):609–15.
46
Guyton
AC
,
Lindsey
AW
,
Kaufmann
BN
. Effect of mean circulatory filling pressure and other peripheral circulatory factors on cardiac output. Am J Physiol. 1955;180(3):463–8.
47Magder S. Venous Return. In: S. Scharf, ed. Respiratory-Circulatory Interactions in Health and Disease. New York: Marcel Dekker; 2001.
48
Moller
PW
,
Winkler
B
,
Hurni
S
,
Heinisch
PP
,
Bloch
AM
,
Sondergaard
S
, et al. Right atrial pressure and venous return during cardiopulmonary bypass. Am J Physiol Heart Circ Physiol. 2017 May 26:ajpheart.00081. [Epub ahead of print]
49
Sondergaard
S
,
Parkin
G
,
Aneman
A
. Central venous pressure: soon an outcome-associated matter. Curr Opin Anaesthesiol. 2016;29(2):179–85. doi:https://doi.org/10.1097/ACO.0000000000000305.https://doi.org/10.1097/ACO.0000000000000305
50
Pinsky
MR
. Instantaneous venous return curves in an intact canine preparation. J Appl Physiol. 1984;56(3):765–71.
51
Fessler
HE
,
Brower
RG
,
Wise
RA
,
Permutt
S
. Effects of positive end-expiratory pressure on the gradient for venous return. Am Rev Respir Dis. 1991;143(1):19–24. doi:https://doi.org/10.1164/ajrccm/143.1.19.https://doi.org/10.1164/ajrccm/143.1.19
52
Fessler
HE
,
Brower
RG
,
Wise
RA
,
Permutt
S
. Effects of positive end-expiratory pressure on the canine venous return curve. Am Rev Respir Dis. 1992;146(1):4–10. doi:https://doi.org/10.1164/ajrccm/146.1.4.https://doi.org/10.1164/ajrccm/146.1.4
53
Chihara
E
,
Hashimoto
S
,
Kinoshita
T
,
Hirose
M
,
Tanaka
Y
,
Morimoto
T
. Elevated mean systemic filling pressure due to intermittent positive-pressure ventilation. Am J Physiol. 1992;262(4 Pt 2):H1116–21.
54
Jellinek
H
,
Krenn
H
,
Oczenski
W
,
Veit
F
,
Schwarz
S
,
Fitzgerald
RD
. Influence of positive airway pressure on the pressure gradient for venous return in humans. J Appl Physiol (1985). 2000;88(3):926–32.
55
Repesse
X
,
Charron
C
,
Geri
G
,
Aubry
A
,
Paternot
A
,
Maizel
J
, et al. Impact of positive pressure ventilation on mean systemic filling pressure in critically ill patients after death. J Appl Physiol. 2017;7(1):73.
56
Versprille
A
,
Jansen
JR
,
Drop
A
,
Hulsmann
AR
. Mean systemic filling pressure as a characteristic pressure for venous return. Pflugers Arch. 1985;405(3):226–33. doi:https://doi.org/10.1007/BF00582565.https://doi.org/10.1007/BF00582565
57
Fessler
HE
,
Brower
RG
,
Shapiro
EP
,
Permutt
S
. Effects of positive end-expiratory pressure and body position on pressure in the thoracic great veins. Am Rev Respir Dis. 1993;148(6 Pt 1):1657–64. doi:https://doi.org/10.1164/ajrccm/148.6_Pt_1.1657.https://doi.org/10.1164/ajrccm/148.6_Pt_1.1657
58
Levy
MN
. The cardiac and vascular factors that determine systemic blood flow. Circ Res. 1979;44(6):739–47. doi:https://doi.org/10.1161/01.RES.44.6.739.https://doi.org/10.1161/01.RES.44.6.739
59
Brengelmann
GL
. A critical analysis of the view that right atrial pressure determines venous return. J Appl Physiol (1985). 2003;94(3):849–59. doi:https://doi.org/10.1152/japplphysiol.00868.2002.https://doi.org/10.1152/japplphysiol.00868.2002
60
Tyberg
JV
. How changes in venous capacitance modulate cardiac output. Pflugers Arch. 2002;445(1):10–7. doi:https://doi.org/10.1007/s00424-002-0922-x.https://doi.org/10.1007/s00424-002-0922-x
61
Beard
DA
,
Feigl
EO
. CrossTalk opposing view: Guyton’s venous return curves should not be taught. J Physiol. 2013;591(23):5795–7. doi:https://doi.org/10.1113/jphysiol.2013.260034.https://doi.org/10.1113/jphysiol.2013.260034
62
Magder
S
. Bench-to-bedside review: An approach to hemodynamic monitoring--Guyton at the bedside. Crit Care. 2012;16(5):236. doi:https://doi.org/10.1186/cc11395.https://doi.org/10.1186/cc11395
63
Tuttle
RR
,
Mills
J
. Dobutamine: development of a new catecholamine to selectively increase cardiac contractility. Circ Res. 1975;36(1):185–96. doi:https://doi.org/10.1161/01.RES.36.1.185.https://doi.org/10.1161/01.RES.36.1.185
64
Pagel
PS
,
Harkin
CP
,
Hettrick
DA
,
Warltier
DC
. Levosimendan (OR-1259), a myofilament calcium sensitizer, enhances myocardial contractility but does not alter isovolumic relaxation in conscious and anesthetized dogs. Anesthesiology. 1994;81(4):974–87. doi:https://doi.org/10.1097/00000542-199410000-00025.https://doi.org/10.1097/00000542-199410000-00025
65
Baim
DS
,
McDowell
AV
,
Cherniles
J
,
Monrad
ES
,
Parker
JA
,
Edelson
J
, et al.
Evaluation of a new bipyridine inotropic agent--milrinone--in patients with severe congestive heart failure. N Engl J Med. 1983;309(13):748–56. doi:https://doi.org/10.1056/NEJM198309293091302.https://doi.org/10.1056/NEJM198309293091302
66
Koch-Weser
J
,
Blinks
JR
. The Influence of the Interval between Beats on Myocardial Contractility. Pharmacol Rev. 1963;15:601–52.
67
Lakatta
EG
. Beyond Bowditch: the convergence of cardiac chronotropy and inotropy. Cell Calcium. 2004;35(6):629–42. doi:https://doi.org/10.1016/j.ceca.2004.01.017.https://doi.org/10.1016/j.ceca.2004.01.017
68
Cingolani
HE
,
Pérez
NG
,
Cingolani
OH
,
Ennis
IL
. The Anrep effect: 100 years later. Am J Physiol Heart Circ Physiol. 2013;304(2):H175–82. doi:https://doi.org/10.1152/ajpheart.00508.2012.https://doi.org/10.1152/ajpheart.00508.2012
69
Patterson
SW
,
Starling
EH
. On the mechanical factors which determine the output of the ventricles. J Physiol. 1914;48(5):357–79. doi:https://doi.org/10.1113/jphysiol.1914.sp001669.https://doi.org/10.1113/jphysiol.1914.sp001669
70
Ross
J, Jr
,
Braunwald
E
. Studies on Starling’s Law of the Heart. Ix. The Effects of Impeding Venous Return on Performance of the Normal and Failing Human Left Ventricle. Circulation. 1964;30(5):719–27. doi:https://doi.org/10.1161/01.CIR.30.5.719.https://doi.org/10.1161/01.CIR.30.5.719
71
Tucker
HJ
,
Murray
JF
. Effects of end-expiratory pressure on organ blood flow in normal and diseased dogs. J Appl Physiol. 1973;34(5):573–7.
72
Fessler
HE
,
Brower
RG
,
Wise
R
,
Permutt
S
. Positive pleural pressure decreases coronary perfusion. Am J Physiol. 1990;258(3 Pt 2):H814–20.
73
Hevrøy
O
,
Grundnes
O
,
Bjertnaes
L
,
Mjøs
OD
. Myocardial blood flow and oxygen consumption during positive end-expiratory pressure ventilation at different levels of cardiac inotropy and frequency. Crit Care Med. 1989;17(1):48–52. doi:https://doi.org/10.1097/00003246-198901000-00010.https://doi.org/10.1097/00003246-198901000-00010
74
Calvin
JE
,
Driedger
AA
,
Sibbald
WJ
. Positive end-expiratory pressure (PEEP) does not depress left ventricular function in patients with pulmonary edema. Am Rev Respir Dis. 1981;124(2):121–8.
75
Johnston
WE
,
Vinten-Johansen
J
,
Santamore
WP
,
Case
LD
,
Little
WC
. Mechanism of reduced cardiac output during positive end-expiratory pressure in the dog. Am Rev Respir Dis. 1989;140(5):1257–64. doi:https://doi.org/10.1164/ajrccm/140.5.1257.https://doi.org/10.1164/ajrccm/140.5.1257
76
Berlin
DA
,
Bakker
J
. Starling curves and central venous pressure. Crit Care. 2015;19(1):55. doi:https://doi.org/10.1186/s13054-015-0776-1.https://doi.org/10.1186/s13054-015-0776-1
77
Hanft
LM
,
Korte
FS
,
McDonald
KS
. Cardiac function and modulation of sarcomeric function by length. Cardiovasc Res. 2008;77(4):627–36. doi:https://doi.org/10.1093/cvr/cvm099.https://doi.org/10.1093/cvr/cvm099
78
Guyton
AC
. Determination of cardiac output by equating venous return curves with cardiac response curves. Physiol Rev. 1955;35(1):123–9.
79
Beard
DA
,
Feigl
EO
. Understanding Guyton’s venous return curves. Am J Physiol Heart Circ Physiol. 2011;301(3):H629–33. doi:https://doi.org/10.1152/ajpheart.00228.2011.https://doi.org/10.1152/ajpheart.00228.2011
80
Vieillard-Baron
A
,
Matthay
M
,
Teboul
JL
,
Bein
T
,
Schultz
M
,
Magder
S
, et al.
Experts’ opinion on management of hemodynamics in ARDS patients: focus on the effects of mechanical ventilation. Intensive Care Med. 2016;42(5):739–49. doi:https://doi.org/10.1007/s00134-016-4326-3.https://doi.org/10.1007/s00134-016-4326-3
81
Marik
PE
,
Cavallazzi
R
,
Vasu
T
,
Hirani
A
. Dynamic changes in arterial waveform derived variables and fluid responsiveness in mechanically ventilated patients: a systematic review of the literature. Crit Care Med. 2009;37(9):2642–7. doi:https://doi.org/10.1097/CCM.0b013e3181a590da.https://doi.org/10.1097/CCM.0b013e3181a590da
82
Mahjoub
Y
,
Pila
C
,
Friggeri
A
,
Zogheib
E
,
Lobjoie
E
,
Tinturier
F
, et al.
Assessing fluid responsiveness in critically ill patients: False-positive pulse pressure variation is detected by Doppler echocardiographic evaluation of the right ventricle. Crit Care Med. 2009;37(9):2570–5. doi:https://doi.org/10.1097/CCM.0b013e3181a380a3.https://doi.org/10.1097/CCM.0b013e3181a380a3
83
Reichek
N
,
Wilson
J
,
St John Sutton
M
,
Plappert
TA
,
Goldberg
S
,
Hirshfeld
JW
. Noninvasive determination of left ventricular end-systolic stress: validation of the method and initial application. Circulation. 1982;65(1):99–108. doi:https://doi.org/10.1161/01.CIR.65.1.99.https://doi.org/10.1161/01.CIR.65.1.99
84
Borlaug
BA
,
Kass
DA
. Invasive hemodynamic assessment in heart failure. Heart Fail Clin. 2009;5(2):217–28. doi:https://doi.org/10.1016/j.hfc.2008.11.008.https://doi.org/10.1016/j.hfc.2008.11.008
85
Walley
KR
. Left ventricular function: time-varying elastance and left ventricular aortic coupling. Crit Care. 2016;20(1):270. doi:https://doi.org/10.1186/s13054-016-1439-6.https://doi.org/10.1186/s13054-016-1439-6
86
Pinsky
MR
. Cardiovascular issues in respiratory care. Chest. 2005;128(5, Suppl 2):592S–7S. doi:https://doi.org/10.1378/chest.128.5_suppl_2.592S.https://doi.org/10.1378/chest.128.5_suppl_2.592S
87
Magder
S
. The left heart can only be as good as the right heart: determinants of function and dysfunction of the right ventricle. Crit Care Resusc. 2007;9(4):344–51.
88
Pinsky
MR
,
Desmet
JM
,
Vincent
JL
. Effect of positive end-expiratory pressure on right ventricular function in humans. Am Rev Respir Dis. 1992;146(3):681–7. doi:https://doi.org/10.1164/ajrccm/146.3.681.https://doi.org/10.1164/ajrccm/146.3.681
89
Vieillard-Baron
A
,
Loubieres
Y
,
Schmitt
JM
,
Page
B
,
Dubourg
O
,
Jardin
F
. Cyclic changes in right ventricular output impedance during mechanical ventilation. J Appl Physiol (1985). 1999;87(5):1644–50.
90
Morimont
P
,
Lambermont
B
,
Ghuysen
A
,
Gerard
P
,
Kolh
P
,
Lancellotti
P
, et al.
Effective arterial elastance as an index of pulmonary vascular load. Am J Physiol Heart Circ Physiol. 2008;294(6):H2736–42. doi:https://doi.org/10.1152/ajpheart.00796.2007.https://doi.org/10.1152/ajpheart.00796.2007
91
Maggiorini
M
,
Brimioulle
S
,
De Canniere
D
,
Delcroix
M
,
Naeije
R
. Effects of pulmonary embolism on pulmonary vascular impedance in dogs and minipigs. J Appl Physiol (1985). 1998;84(3):815–21.
92
Berger
D
,
Bloechlinger
S
,
Takala
J
,
Sinderby
C
,
Brander
L
. Heart-lung interactions during neurally adjusted ventilatory assist. Crit Care. 2014;18(5):499. doi:https://doi.org/10.1186/s13054-014-0499-8.https://doi.org/10.1186/s13054-014-0499-8
93
Mekontso Dessap
A
,
Boissier
F
,
Charron
C
,
Bégot
E
,
Repessé
X
,
Legras
A
, et al.
Acute cor pulmonale during protective ventilation for acute respiratory distress syndrome: prevalence, predictors, and clinical impact. Intensive Care Med. 2016;42(5):862–70. doi:https://doi.org/10.1007/s00134-015-4141-2.https://doi.org/10.1007/s00134-015-4141-2
94
Jardin
F
,
Brun-Ney
D
,
Cazaux
P
,
Dubourg
O
,
Hardy
A
,
Bourdarias
JP
. Relation between transpulmonary pressure and right ventricular isovolumetric pressure change during respiratory support. Cathet Cardiovasc Diagn. 1989;16(4):215–20. doi:https://doi.org/10.1002/ccd.1810160402.https://doi.org/10.1002/ccd.1810160402
95
Pinsky
MR
. Determinants of pulmonary arterial flow variation during respiration. J Appl Physiol. 1984;56(5):1237–45.
96
Matthews
JC
,
McLaughlin
V
. Acute right ventricular failure in the setting of acute pulmonary embolism or chronic pulmonary hypertension: a detailed review of the pathophysiology, diagnosis, and management. Curr Cardiol Rev. 2008;4(1):49–59. doi:https://doi.org/10.2174/157340308783565384.https://doi.org/10.2174/157340308783565384
97
Voorhees
AP
,
Han
HC
. Biomechanics of Cardiac Function. Compr Physiol. 2015;5(4):1623–44. doi:https://doi.org/10.1002/cphy.c140070.https://doi.org/10.1002/cphy.c140070
98
Bloechlinger
S
,
Grander
W
,
Bryner
J
,
Dünser
MW
. Left ventricular rotation: a neglected aspect of the cardiac cycle. Intensive Care Med. 2011;37(1):156–63. doi:https://doi.org/10.1007/s00134-010-2053-8.https://doi.org/10.1007/s00134-010-2053-8
99
Bishop
VS
,
Stone
HL
,
Guyton
AC
. Cardiac function curves in conscious dogs. Am J Physiol. 1964;207:677–82.
100
Haddad
F
,
Doyle
R
,
Murphy
DJ
,
Hunt
SA
. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation. 2008;117(13):1717–31. doi:https://doi.org/10.1161/CIRCULATIONAHA.107.653584.https://doi.org/10.1161/CIRCULATIONAHA.107.653584
101
Haddad
F
,
Hunt
SA
,
Rosenthal
DN
,
Murphy
DJ
. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008;117(11):1436–48. doi:https://doi.org/10.1161/CIRCULATIONAHA.107.653576.https://doi.org/10.1161/CIRCULATIONAHA.107.653576
102
Kaul
S
,
Hopkins
JM
,
Shah
PM
. Chronic effects of myocardial infarction on right ventricular function: a noninvasive assessment. J Am Coll Cardiol. 1983;2(4):607–15. doi:https://doi.org/10.1016/S0735-1097(83)80299-X.https://doi.org/10.1016/S0735-1097(83)80299-X
103
Danchin
N
,
Juilliere
Y
,
Schrijen
F
,
Cherrier
F
. Differential effects on right ventricular function of transient right, left anterior descending and left circumflex coronary occlusions during percutaneous transluminal coronary angioplasty. J Am Coll Cardiol. 1991;18(2):437–42. doi:https://doi.org/10.1016/0735-1097(91)90597-3.https://doi.org/10.1016/0735-1097(91)90597-3
104
Buckberg
G
,
Hoffman
JI
. Right ventricular architecture responsible for mechanical performance: unifying role of ventricular septum. J Thorac Cardiovasc Surg. 2014;148(6):3166–71.e1, 4. doi:https://doi.org/10.1016/j.jtcvs.2014.05.044.https://doi.org/10.1016/j.jtcvs.2014.05.044
105
Jardin
F
,
Dubourg
O
,
Guéret
P
,
Delorme
G
,
Bourdarias
JP
. Quantitative two-dimensional echocardiography in massive pulmonary embolism: emphasis on ventricular interdependence and leftward septal displacement. J Am Coll Cardiol. 1987;10(6):1201–6. doi:https://doi.org/10.1016/S0735-1097(87)80119-5.https://doi.org/10.1016/S0735-1097(87)80119-5
106
Taylor
RR
,
Covell
JW
,
Sonnenblick
EH
,
Ross
J, Jr
. Dependence of ventricular distensibility on filling of the opposite ventricle. Am J Physiol. 1967;213(3):711–8.
107
Magder
S
,
Guerard
B
. Heart-lung interactions and pulmonary buffering: lessons from a computational modeling study. Respir Physiol Neurobiol. 2012;182(2-3):60–70. doi:https://doi.org/10.1016/j.resp.2012.05.011.https://doi.org/10.1016/j.resp.2012.05.011
108
Vieillard-Baron
A
,
Schmitt
JM
,
Augarde
R
,
Fellahi
JL
,
Prin
S
,
Page
B
, et al.
Acute cor pulmonale in acute respiratory distress syndrome submitted to protective ventilation: incidence, clinical implications, and prognosis. Crit Care Med. 2001;29(8):1551–5. doi:https://doi.org/10.1097/00003246-200108000-00009.https://doi.org/10.1097/00003246-200108000-00009
109
Pinsky
MR
. Functional haemodynamic monitoring. Curr Opin Crit Care. 2014;20(3):288–93. doi:https://doi.org/10.1097/MCC.0000000000000090.https://doi.org/10.1097/MCC.0000000000000090
110
Duggan
M
,
McCaul
CL
,
McNamara
PJ
,
Engelberts
D
,
Ackerley
C
,
Kavanagh
BP
. Atelectasis causes vascular leak and lethal right ventricular failure in uninjured rat lungs. Am J Respir Crit Care Med. 2003;167(12):1633–40. doi:https://doi.org/10.1164/rccm.200210-1215OC.https://doi.org/10.1164/rccm.200210-1215OC
111
Bull
TM
,
Clark
B
,
McFann
K
,
Moss
M
; National Institutes of Health/National Heart, Lung, and Blood Institute ARDS Network. Pulmonary vascular dysfunction is associated with poor outcomes in patients with acute lung injury. Am J Respir Crit Care Med. 2010;182(9):1123–8. doi:https://doi.org/10.1164/rccm.201002-0250OC.https://doi.org/10.1164/rccm.201002-0250OC
112
Brower
RG
,
Matthay
MA
,
Morris
A
,
Schoenfeld
D
,
Thompson
BT
,
Wheeler
A
; Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–8. doi:https://doi.org/10.1056/NEJM200005043421801.https://doi.org/10.1056/NEJM200005043421801
113
Mayo
P
,
Mekontso Dessap
A
,
Vieillard-Baron
A
. Myths about critical care echocardiography: the ten false beliefs that intensivists should understand. Intensive Care Med. 2015;41(6):1103–6. doi:https://doi.org/10.1007/s00134-014-3622-z.https://doi.org/10.1007/s00134-014-3622-z
114
Vieillard-Baron
A
,
Charron
C
,
Caille
V
,
Belliard
G
,
Page
B
,
Jardin
F
. Prone positioning unloads the right ventricle in severe ARDS. Chest. 2007;132(5):1440–6. doi:https://doi.org/10.1378/chest.07-1013.https://doi.org/10.1378/chest.07-1013
115
Jozwiak
M
,
Teboul
JL
,
Anguel
N
,
Persichini
R
,
Silva
S
,
Chemla
D
, et al.
Beneficial hemodynamic effects of prone positioning in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2013;188(12):1428–33. doi:https://doi.org/10.1164/rccm.201303-0593OC.https://doi.org/10.1164/rccm.201303-0593OC
116
Vignon
P
,
Merz
TM
,
Vieillard-Baron
A
. Ten reasons for performing hemodynamic monitoring using transesophageal echocardiography. Intensive Care Med. 2017;43(7):1048–51. doi:https://doi.org/10.1007/s00134-017-4716-1.https://doi.org/10.1007/s00134-017-4716-1
117
Shaw
AM
,
Shook
D
,
Hayashida
D
,
Zhang
X
,
Munson
H
. Pulmonary artery catheter (PAC) use is associated with improved clinical outcomes after adult cardiac surgery. Crit Care. 2017;21(Suppl 1).
118
Takala
J
. Hypoxemia due to increased venous admixture: influence of cardiac output on oxygenation. Intensive Care Med. 2007;33(5):908–11. doi:https://doi.org/10.1007/s00134-007-0546-x.https://doi.org/10.1007/s00134-007-0546-x
119
Talmor
D
,
Sarge
T
,
Malhotra
A
,
O’Donnell
CR
,
Ritz
R
,
Lisbon
A
, et al.
Mechanical ventilation guided by esophageal pressure in acute lung injury. N Engl J Med. 2008;359(20):2095–104. doi:https://doi.org/10.1056/NEJMoa0708638.https://doi.org/10.1056/NEJMoa0708638
120
Pepe
PE
,
Marini
JJ
. Occult positive end-expiratory pressure in mechanically ventilated patients with airflow obstruction: the auto-PEEP effect. Am Rev Respir Dis. 1982;126(1):166–70.
121
Marini
JJ
. Dynamic hyperinflation and auto-positive end-expiratory pressure: lessons learned over 30 years. Am J Respir Crit Care Med. 2011;184(7):756–62. doi:https://doi.org/10.1164/rccm.201102-0226PP.https://doi.org/10.1164/rccm.201102-0226PP
122
Daudel
F
,
Tüller
D
,
Krähenbühl
S
,
Jakob
SM
,
Takala
J
. Pulse pressure variation and volume responsiveness during acutely increased pulmonary artery pressure: an experimental study. Crit Care. 2010;14(3):R122. doi:https://doi.org/10.1186/cc9080.https://doi.org/10.1186/cc9080
123
Wyler von Ballmoos
M
,
Takala
J
,
Roeck
M
,
Porta
F
,
Tueller
D
,
Ganter
CC
, et al.
Pulse-pressure variation and hemodynamic response in patients with elevated pulmonary artery pressure: a clinical study. Crit Care. 2010;14(3):R111. doi:https://doi.org/10.1186/cc9060.https://doi.org/10.1186/cc9060
124
Sternberg
R
,
Sahebjami
H
. Hemodynamic and oxygen transport characteristics of common ventilatory modes. Chest. 1994;105(6):1798–803. doi:https://doi.org/10.1378/chest.105.6.1798.https://doi.org/10.1378/chest.105.6.1798
125
Lessard
MR
,
Guérot
E
,
Lorino
H
,
Lemaire
F
,
Brochard
L
. Effects of pressure-controlled with different I:E ratios versus volume-controlled ventilation on respiratory mechanics, gas exchange, and hemodynamics in patients with adult respiratory distress syndrome. Anesthesiology. 1994;80(5):983–91. doi:https://doi.org/10.1097/00000542-199405000-00006.https://doi.org/10.1097/00000542-199405000-00006
126
Abraham
E
,
Yoshihara
G
. Cardiorespiratory effects of pressure controlled ventilation in severe respiratory failure. Chest. 1990;98(6):1445–9. doi:https://doi.org/10.1378/chest.98.6.1445.https://doi.org/10.1378/chest.98.6.1445
127
Takala
J
. Volume responsive, but does the patient need volume?
Intensive Care Med. 2016;42(9):1461–3. doi:https://doi.org/10.1007/s00134-015-4172-8.https://doi.org/10.1007/s00134-015-4172-8
128
Eskesen
TG
,
Wetterslev
M
,
Perner
A
. Systematic review including re-analyses of 1148 individual data sets of central venous pressure as a predictor of fluid responsiveness. Intensive Care Med. 2016;42(3):324–32. doi:https://doi.org/10.1007/s00134-015-4168-4.https://doi.org/10.1007/s00134-015-4168-4
129
Perel
A
,
Pizov
R
,
Cotev
S
. Systolic blood pressure variation is a sensitive indicator of hypovolemia in ventilated dogs subjected to graded hemorrhage. Anesthesiology. 1987;67(4):498–502. doi:https://doi.org/10.1097/00000542-198710000-00009.https://doi.org/10.1097/00000542-198710000-00009
130
Coriat
P
,
Vrillon
M
,
Perel
A
,
Baron
JF
,
Le Bret
F
,
Saada
M
, et al.
A comparison of systolic blood pressure variations and echocardiographic estimates of end-diastolic left ventricular size in patients after aortic surgery. Anesth Analg. 1994;78(1):46–53. doi:https://doi.org/10.1213/00000539-199401000-00009.https://doi.org/10.1213/00000539-199401000-00009
131
Feissel
M
,
Mangin
I
,
Ruyer
O
,
Faller
J-P
,
Michard
F
,
Teboul
J-L
. Respiratory changes in aortic blood velocity as an indicator of fluid responsiveness in ventilated patients with septic shock. Chest. 2001;119(3):867–73. doi:https://doi.org/10.1378/chest.119.3.867.https://doi.org/10.1378/chest.119.3.867
132
Reuter
DA
,
Felbinger
TW
,
Kilger
E
,
Schmidt
C
,
Lamm
P
,
Goetz
AE
. Optimizing fluid therapy in mechanically ventilated patients after cardiac surgery by on-line monitoring of left ventricular stroke volume variations. Comparison with aortic systolic pressure variations. Br J Anaesth. 2002;88(1):124–6. doi:https://doi.org/10.1093/bja/88.1.124.https://doi.org/10.1093/bja/88.1.124
133
Michard
F
,
Boussat
S
,
Chemla
D
,
Anguel
N
,
Mercat
A
,
Lecarpentier
Y
, et al.
Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am J Respir Crit Care Med. 2000;162(1):134–8. doi:https://doi.org/10.1164/ajrccm.162.1.9903035.https://doi.org/10.1164/ajrccm.162.1.9903035
134
Michard
F
,
Chemla
D
,
Richard
C
,
Wysocki
M
,
Pinsky
MR
,
Lecarpentier
Y
, et al.
Clinical use of respiratory changes in arterial pulse pressure to monitor the hemodynamic effects of PEEP. Am J Respir Crit Care Med. 1999;159(3):935–9. doi:https://doi.org/10.1164/ajrccm.159.3.9805077.https://doi.org/10.1164/ajrccm.159.3.9805077
135
Michard
F
,
Boussat
S
,
Chemla
D
,
Anguel
N
,
Mercat
A
,
Lecarpentier
Y
, et al.
Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am J Respir Crit Care Med. 2000;162(1):134–8. doi:https://doi.org/10.1164/ajrccm.162.1.9903035.https://doi.org/10.1164/ajrccm.162.1.9903035
136
Magder
S
. Clinical usefulness of respiratory variations in arterial pressure. Am J Respir Crit Care Med. 2004;169(2):151–5. doi:https://doi.org/10.1164/rccm.200211-1360CC.https://doi.org/10.1164/rccm.200211-1360CC
137
Sondergaard
S
. Pavane for a pulse pressure variation defunct. Crit Care. 2013;17(6):327. doi:https://doi.org/10.1186/cc13109.https://doi.org/10.1186/cc13109
138
Magder
S
. Clinical usefulness of respiratory variations in arterial pressure. Am J Respir Crit Care Med. 2004;169(2):151–5. doi:https://doi.org/10.1164/rccm.200211-1360CC.https://doi.org/10.1164/rccm.200211-1360CC
139
De Backer
D
,
Heenen
S
,
Piagnerelli
M
,
Koch
M
,
Vincent
JL
. Pulse pressure variations to predict fluid responsiveness: influence of tidal volume. Intensive Care Med. 2005;31(4):517–23. doi:https://doi.org/10.1007/s00134-005-2586-4.https://doi.org/10.1007/s00134-005-2586-4
140
De Backer
D
,
Taccone
FS
,
Holsten
R
,
Ibrahimi
F
,
Vincent
JL
. Influence of respiratory rate on stroke volume variation in mechanically ventilated patients. Anesthesiology. 2009;110(5):1092–7. doi:https://doi.org/10.1097/ALN.0b013e31819db2a1.https://doi.org/10.1097/ALN.0b013e31819db2a1
141
Mesquida
J
,
Kim
HK
,
Pinsky
MR
. Effect of tidal volume, intrathoracic pressure, and cardiac contractility on variations in pulse pressure, stroke volume, and intrathoracic blood volume. Intensive Care Med. 2011;37(10):1672–9. doi:https://doi.org/10.1007/s00134-011-2304-3.https://doi.org/10.1007/s00134-011-2304-3
142
Mahjoub
Y
,
Lejeune
V
,
Muller
L
,
Perbet
S
,
Zieleskiewicz
L
,
Bart
F
, et al.
Evaluation of pulse pressure variation validity criteria in critically ill patients: a prospective observational multicentre point-prevalence study. Br J Anaesth. 2014;112(4):681–5. doi:https://doi.org/10.1093/bja/aet442.https://doi.org/10.1093/bja/aet442
143
Vignon
P
,
Repesse
X
,
Begot
E
,
Leger
J
,
Jacob
C
,
Bouferrache
K
, et al.
Comparison of Echocardiographic Indices Used to Predict Fluid Responsiveness in Ventilated Patients. Am J Respir Crit Care Med. 2017;195(8):1022–32.
144
Vieillard-Baron
A
,
Chergui
K
,
Augarde
R
,
Prin
S
,
Page
B
,
Beauchet
A
, et al.
Cyclic changes in arterial pulse during respiratory support revisited by Doppler echocardiography. Am J Respir Crit Care Med. 2003;168(6):671–6. doi:https://doi.org/10.1164/rccm.200301-135OC.https://doi.org/10.1164/rccm.200301-135OC
145
Vieillard-Baron
A
,
Augarde
R
,
Prin
S
,
Page
B
,
Beauchet
A
,
Jardin
F
. Influence of superior vena caval zone condition on cyclic changes in right ventricular outflow during respiratory support. Anesthesiology. 2001;95(5):1083–8. doi:https://doi.org/10.1097/00000542-200111000-00010.https://doi.org/10.1097/00000542-200111000-00010
146
Vieillard-Baron
A
,
Chergui
K
,
Rabiller
A
,
Peyrouset
O
,
Page
B
,
Beauchet
A
, et al.
Superior vena caval collapsibility as a gauge of volume status in ventilated septic patients. Intensive Care Med. 2004;30(9):1734–9. doi:https://doi.org/10.1007/s00134-004-2361-y.https://doi.org/10.1007/s00134-004-2361-y
147
Barbier
C
,
Loubières
Y
,
Schmit
C
,
Hayon
J
,
Ricôme
JL
,
Jardin
F
, et al.
Respiratory changes in inferior vena cava diameter are helpful in predicting fluid responsiveness in ventilated septic patients. Intensive Care Med. 2004;30(9):1740–6. doi:https://doi.org/10.1007/s00134-004-2259-8.https://doi.org/10.1007/s00134-004-2259-8
148
Hartog
EA
,
Jansen
JR
,
Moens
GH
,
Versprille
A
. Systemic filling pressure in the intact circulation determined with a slow inflation procedure. Pflugers Arch. 1996;431(6):863–7. doi:https://doi.org/10.1007/s004240050078.https://doi.org/10.1007/s004240050078
149
Jansen
JR
,
Maas
JJ
,
Pinsky
MR
. Bedside assessment of mean systemic filling pressure. Curr Opin Crit Care. 2010;16(3):231–6. doi:https://doi.org/10.1097/MCC.0b013e3283378185.https://doi.org/10.1097/MCC.0b013e3283378185
150
Maas
JJ
,
Geerts
BF
,
van den Berg
PC
,
Pinsky
MR
,
Jansen
JR
. Assessment of venous return curve and mean systemic filling pressure in postoperative cardiac surgery patients. Crit Care Med. 2009;37(3):912–8. doi:https://doi.org/10.1097/CCM.0b013e3181961481.https://doi.org/10.1097/CCM.0b013e3181961481
151
Maas
JJ
,
Pinsky
MR
,
de Wilde
RB
,
de Jonge
E
,
Jansen
JR
. Cardiac output response to norepinephrine in postoperative cardiac surgery patients: interpretation with venous return and cardiac function curves. Crit Care Med. 2013;41(1):143–50. doi:https://doi.org/10.1097/CCM.0b013e318265ea64.https://doi.org/10.1097/CCM.0b013e318265ea64
152
Maas
JJ
,
Pinsky
MR
,
Geerts
BF
,
de Wilde
RB
,
Jansen
JR
. Estimation of mean systemic filling pressure in postoperative cardiac surgery patients with three methods. Intensive Care Med. 2012;38(9):1452–60. Correction in: Intensive Care Med. 2013;39:163. doi:https://doi.org/10.1007/s00134-012-2586-0.https://doi.org/10.1007/s00134-012-2586-0
153
Persichini
R
,
Silva
S
,
Teboul
JL
,
Jozwiak
M
,
Chemla
D
,
Richard
C
, et al.
Effects of norepinephrine on mean systemic pressure and venous return in human septic shock. Crit Care Med. 2012;40(12):3146–53. doi:https://doi.org/10.1097/CCM.0b013e318260c6c3.https://doi.org/10.1097/CCM.0b013e318260c6c3
154
Chihara
E
,
Hashimoto
S
,
Kinoshita
T
,
Hirose
M
,
Tanaka
Y
,
Morimoto
T
. Elevated mean systemic filling pressure due to intermittent positive-pressure ventilation. Am J Physiol. 1992;262(4 Pt 2):H1116–21.
155
Lemaire
F
,
Teboul
JL
,
Cinotti
L
,
Giotto
G
,
Abrouk
F
,
Steg
G
, et al.
Acute left ventricular dysfunction during unsuccessful weaning from mechanical ventilation. Anesthesiology. 1988;69(2):171–9. doi:https://doi.org/10.1097/00000542-198808000-00004.https://doi.org/10.1097/00000542-198808000-00004
156
Lemaire
F
,
Teboul
JL
,
Cinotti
L
,
Giotto
G
,
Abrouk
F
,
Steg
G
, et al.
Acute left ventricular dysfunction during unsuccessful weaning from mechanical ventilation. Anesthesiology. 1988;69(2):171–9. doi:https://doi.org/10.1097/00000542-198808000-00004.https://doi.org/10.1097/00000542-198808000-00004
157
Jubran
A
,
Mathru
M
,
Dries
D
,
Tobin
MJ
. Continuous recordings of mixed venous oxygen saturation during weaning from mechanical ventilation and the ramifications thereof. Am J Respir Crit Care Med. 1998;158:306–10.
158
Abalos
A
,
Leibowitz
AB
,
Distefano
D
,
Halpern
N
,
Iberti
TJ
. Myocardial ischemia during the weaning period. Am J Crit Care. 1992;1:32–6.
159
Chatila
W
,
Ani
S
,
Guaglianone
D
,
Jacob
B
,
Amoateng-Adjepong
Y
,
Manthous
CA
. Cardiac ischemia during weaning from mechanical ventilation. Chest. 1996;109(6):1577–83. doi:https://doi.org/10.1378/chest.109.6.1577.https://doi.org/10.1378/chest.109.6.1577
160
Mekontso Dessap
A
,
Roche-Campo
F
,
Kouatchet
A
,
Tomicic
V
,
Beduneau
G
,
Sonneville
R
, et al.
Natriuretic peptide-driven fluid management during ventilator weaning: a randomized controlled trial. Am J Respir Crit Care Med. 2012;186(12):1256–63. doi:https://doi.org/10.1164/rccm.201205-0939OC.https://doi.org/10.1164/rccm.201205-0939OC
161
Mekontso-Dessap
A
,
de Prost
N
,
Girou
E
,
Braconnier
F
,
Lemaire
F
,
Brun-Buisson
C
, et al.
B-type natriuretic peptide and weaning from mechanical ventilation. Intensive Care Med. 2006;32(10):1529–36. doi:https://doi.org/10.1007/s00134-006-0339-7.https://doi.org/10.1007/s00134-006-0339-7
162
Dres
M
,
Teboul
JL
,
Anguel
N
,
Guerin
L
,
Richard
C
,
Monnet
X
. Extravascular lung water, B-type natriuretic peptide, and blood volume contraction enable diagnosis of weaning-induced pulmonary edema. Crit Care Med. 2014;42(8):1882–9. doi:https://doi.org/10.1097/CCM.0000000000000295.https://doi.org/10.1097/CCM.0000000000000295
163
Moschietto
S
,
Doyen
D
,
Grech
L
,
Dellamonica
J
,
Hyvernat
H
,
Bernardin
G
. Transthoracic Echocardiography with Doppler Tissue Imaging predicts weaning failure from mechanical ventilation: evolution of the left ventricle relaxation rate during a spontaneous breathing trial is the key factor in weaning outcome. Crit Care. 2012;16(3):R81. doi:https://doi.org/10.1186/cc11339.https://doi.org/10.1186/cc11339
164
Konomi
I
,
Tasoulis
A
,
Kaltsi
I
,
Karatzanos
E
,
Vasileiadis
I
,
Temperikidis
P
, et al.
Left ventricular diastolic dysfunction--an independent risk factor for weaning failure from mechanical ventilation. Anaesth Intensive Care. 2016;44(4):466–73.
165
Juhl-Olsen
P
,
Hermansen
JF
,
Frederiksen
CA
,
Rasmussen
LA
,
Jakobsen
CJ
,
Sloth
E
. Positive end-expiratory pressure influences echocardiographic measures of diastolic function: a randomized, crossover study in cardiac surgery patients. Anesthesiology. 2013;119(5):1078–86. doi:https://doi.org/10.1097/ALN.0b013e3182a10b40.https://doi.org/10.1097/ALN.0b013e3182a10b40
166
Juhl-Olsen
P
,
Frederiksen
CA
,
Hermansen
JF
,
Jakobsen
CJ
,
Sloth
E
. Echocardiographic Measures of Diastolic Function Are Preload Dependent during Triggered Positive Pressure Ventilation: A Controlled Crossover Study in Healthy Subjects. Crit Care Res Pract. 2012;2012:703196. doi:https://doi.org/10.1155/2012/703196.https://doi.org/10.1155/2012/703196
167
Forrester
JS
,
Diamond
G
,
McHugh
TJ
,
Swan
HJ
. Filling pressures in the right and left sides of the heart in acute myocardial infarction. A reappraisal of central-venous-pressure monitoring. N Engl J Med. 1971;285(4):190–3. doi:https://doi.org/10.1056/NEJM197107222850402.https://doi.org/10.1056/NEJM197107222850402
168
Nieminen
MS
,
Brutsaert
D
,
Dickstein
K
,
Drexler
H
,
Follath
F
,
Harjola
VP
, et al.; EuroHeart Survey Investigators; Heart Failure Association, European Society of Cardiology. EuroHeart Failure Survey II (EHFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J. 2006;27(22):2725–36. doi:https://doi.org/10.1093/eurheartj/ehl193.https://doi.org/10.1093/eurheartj/ehl193
169
Jessup
M
,
Brozena
S
. Heart failure. N Engl J Med. 2003;348(20):2007–18. doi:https://doi.org/10.1056/NEJMra021498.https://doi.org/10.1056/NEJMra021498
170
Gray
A
,
Goodacre
S
,
Newby
DE
,
Masson
M
,
Sampson
F
,
Nicholl
J
; 3CPO Trialists. Noninvasive ventilation in acute cardiogenic pulmonary edema. N Engl J Med. 2008;359(2):142–51. doi:https://doi.org/10.1056/NEJMoa0707992.https://doi.org/10.1056/NEJMoa0707992
171
Pinsky
MR
. Sleeping with the enemy: the heart in obstructive sleep apnea. Chest. 2002;121(4):1022–4. doi:https://doi.org/10.1378/chest.121.4.1022.https://doi.org/10.1378/chest.121.4.1022
172
Chai-Coetzer
CL
,
Antic
NA
,
Hamilton
GS
,
McArdle
N
,
Wong
K
,
Yee
BJ
, et al.
Physician Decision Making and Clinical Outcomes With Laboratory Polysomnography or Limited-Channel Sleep Studies for Obstructive Sleep Apnea: A Randomized Trial. Ann Intern Med. 2017;166(5):332–40. doi:https://doi.org/10.7326/M16-1301.https://doi.org/10.7326/M16-1301
173
Peker
Y
,
Glantz
H
,
Eulenburg
C
,
Wegscheider
K
,
Herlitz
J
,
Thunström
E
. Effect of Positive Airway Pressure on Cardiovascular Outcomes in Coronary Artery Disease Patients with Nonsleepy Obstructive Sleep Apnea. The RICCADSA Randomized Controlled Trial. Am J Respir Crit Care Med. 2016;194(5):613–20. doi:https://doi.org/10.1164/rccm.201601-0088OC.https://doi.org/10.1164/rccm.201601-0088OC
174
McEvoy
RD
,
Antic
NA
,
Heeley
E
,
Luo
Y
,
Ou
Q
,
Zhang
X
, et al.; SAVE Investigators and Coordinators. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea. N Engl J Med. 2016;375(10):919–31. doi:https://doi.org/10.1056/NEJMoa1606599.https://doi.org/10.1056/NEJMoa1606599