New treatment for non-Hodgkin B-cell lymphomas with a special focus on the impact of junctional adhesion molecules
DOI: https://doi.org/10.4414/smw.2017.14487
Beat A.
Imhof, Thomas
Matthes
Faculté de Médecine, Université de Genève, Geneva, Switzerland
Summary
Current therapeutic modalities used for B-cell lymphoma include chemotherapy, immunotherapy, and radiation therapy. Chemotherapy together with anti-CD20 monoclonal antibodies forms the cornerstone of therapy and has a curative, as well as a palliative, role in this disease. New treatment modalities targeting specific molecules on the surface of lymphoma cells or intracellular pathways regulating apoptosis, proliferation and cell division are intensively investigated. One such target is JAM-C, a molecule implicated in cell adhesion and in B cell migration and whose inhibition blocks B cells from reaching their supportive microenvironments in lymphoid organs. Hopefully this and other strategies will help to improve survival of B cell lymphoma patients in the future.
Abbreviations
- ASCT
-
autologous stem cell transplantation
- ADCC
-
antibody-dependent cellular cytotoxicity
- CDC
-
complement-dependent cytotoxicity
- CLL
-
chronic lymphocytic leukaemia
- DLBCL
-
diffuse large B cell lymphoma
- HL
-
Hodgkin’s lymphoma
- HCL
-
hairy cell leukaemia
- HSC
-
hematopoietic stem cells
- MCL
-
mantle cell lymphoma
- MM
-
multiple myeloma
- MDS
-
myelodysplastic syndrome
- NSCLC
-
non-small-cell lung carcinoma
- NHL
-
non-Hodgkin lymphoma
- WM
-
Waldenstroem’s macroglobulinaemia
Introduction
B-cell non-Hodgkin lymphomas (NHL) are a group of clearly defined cancer types that originate in the lymphatic system from mature B lymphocytes. NHL are among the six most common cancer types in Switzerland, with a stable incidence rate of about 17 diagnoses in males and 12 in females per 100 000 people per year for the last 20 years [1]. The most common age of diagnosis is between 65 and 75 years. The percentage of people in Switzerland who survive five years is approximately 55–75%, depending on the lymphoma subtype.
Lymphadenopathies are the most common manifestation, and symptoms can include fatigue, fever, night sweats, weight loss and signs of organ infiltration, such as splenomegaly, pancytopenia, or CNS involvement. Progression of the disease can be slow and occur over years, like in indolent CLL or marginal-zone lymphoma, or can be much more aggressive, rapid and fatal, as in diffuse large B-cell lymphoma. Malignant B cells can also produce soluble immunoglobulins, which might lead to hyperviscosity and associated complications, such as in Waldenstroem’s macroglubulinaemia. Rarely, spontaneous remissions have been documented.
Traditional treatment is based, to a large extent, on stratification of patients into groups based on disease subtype and stage, and relies on watch-and-wait surveillance for indolent forms, or on external beam irradiation, immunotherapy with anti-CD20 antibodies, and alkylating agent-based chemotherapy for more aggressive forms.
In this review, we provide a survey of established and actively investigated newer treatment approaches and strategies for NHL. We explain the rationale behind each of these approaches and describe the strategies that are currently available in Switzerland or are expected to be approved in the near future. The approval process is often slower than in other European countries or in the USA, and even when drugs are accepted by regulatory agencies, their costs are still not automatically reimbursed by health insurance providers. Special authorisations from the medical officers of insurance companies have to be obtained by the treating haematologist/oncologist on a case-by-case basis.
Chemotherapy
Since 1993, the most common multidrug combination used for the initial chemotherapy of aggressive NHL is the CHOP combination (cyclophosphamide, doxorubicin, prednisone, vincristine). For patients with B-cell lymphoma, adding rituximab to CHOP results in better outcomes than using CHOP alone (see below) [2, 3]. Other commonly used drugs prescribed as single agents or in combinations include bendamustin, fludarabine, vincristine and cyclophosphamide. The most common side effects of these therapies are fatigue, loss of appetite, weight loss, transitory pancytopenia, increased risk of infection, nausea and vomiting, hair loss, and diarrhoea.
Antibiotics
Gastric MALT lymphoma is an indolent lymphoma type that is linked to infection by the bacterium Helicobacter pylori. Patients can sometimes be treated with antibiotics against this pathogen [4, 5]. MALT lymphomas of the orbit and adnexal structures have been linked to infection with the bacterium Chlamydophila psittaci. One study has shown that doxycycline can improve outcomes and lead to a cure in some patients [6, 7].
Monoclonal antibody therapy for NHL
Monoclonal antibodies were the first successful forms of “targeted therapy” for lymphoma, with rituximab, a monoclonal antibody against the pan-B cell target CD20, approved in 1997 by the FDA and now used as the standard course of care for all B-cell lymphomas. Rituximab acts through complement-mediated cytotoxicity, antibody-dependent cell-mediated cytotoxicity, and induction of apoptosis [2, 8]. It can be used either as monotherapy in low-grade lymphomas, in addition to combination chemotherapy (e.g., R-CHOP for DLBCL, FCR and BR for CLL), or as maintenance treatment, as in follicular or mantle-cell lymphoma. In all these applications, rituximab has shown impressive survival benefits when compared to treatments used in the “pre-rituximab” era, and R-CHOP now constitutes the standard of care for FL and DLBCL in European countries.
There are now several newer antibodies that, like rituximab, target the CD20 antigen. They either bind to different epitopes of CD20 or with higher affinity than rituximab [9]. Although these antibodies constitute additional options for the treatment of lymphomas (in particular in cases of resistance/progression under rituximab treatment), their efficiencies are only moderately better than those obtained with rituximab.
Ofatumumab (Arzerra®)
Ofatumumab binds to a different epitope of CD20 than rituximab [10]. It also binds to CD20 for longer periods of time. It is given intravenously and slowly to begin with, and the infusion rate is increased gradually during each treatment. If the drug is well tolerated, the first full dose is then applied a week later. Currently, ofatumumab is approved in chronic lymphocytic leukaemia (CLL) (fig. 1 and table 1).
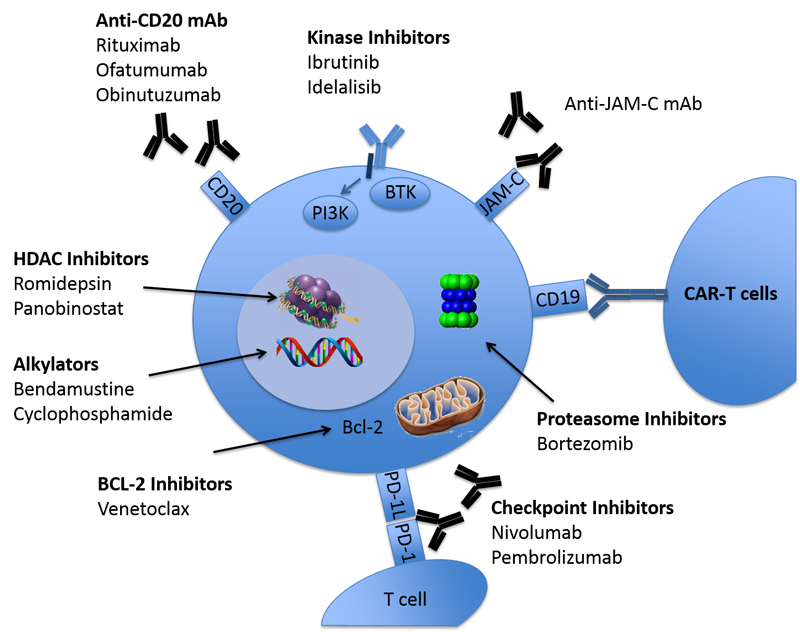
Figure 1
Mechanisms involved in targeting B-cell lymphoma cells. Traditionally, alkylators and anti-CD20 antibodies have been used for B-cell lymphoma treatment. Newly developed drugs target intracellular kinases such as BTK or PI3K, proteasomes, BCL-2 molecules, or HDAC. More recently, modified T-cells (CAR, chimeric antigen receptor), and checkpoint inhibiting monoclonal antibodies have been applied. An alternative approach in the preclinical phase consists of targeting molecules regulating B-cell migration, such as junctional adhesion molecule C (JAM-C).
Obinutuzumab (Gazyvaro®)
Obinutuzumab (previously known as GA101) is an antibody that has been glycoengineered to bind more tightly to CD20 than rituximab and at a slightly different but overlapping epitope [11]. It is given intravenously and increases the ADCC of targeted B cells. A recent phase-III trial, comparing head-to-head the effects of rituximab and ofatumumab in untreated follicular lymphoma patients showed higher PFS rates for Ofatumumab (80% vs. 73.3% for three-year PFS; HR = 0.66), establishing this drug as a new option in untreated follicular lymphoma [12]. Currently, obinutuzumab is approved in CLL and follicular lymphoma (see table 1 and fig. 1).
Several other antigens on malignant B cells are currently studied and in pre-clinical or early clinical phases of development:
- − Epratuzumab, a humanised monoclonal antibody, which targets the CD22 antigen on mature and malignant B-cells, has been studied with some encouraging results in follicular lymphoma and diffuse large B cell lymphoma (DLBCL) [13], but failed in two phase-III studies in Lupus patients [14].
- − CD37, a transmembrane molecule and member of the tetraspanin superfamily, has recently gathered renewed interest as a target for NHL and CLL that are resistant or refractory to Rituximab [15, 16].
- − CD44 is highly expressed in malignant, inflammatory, and auto-immunological diseases. Certain isoforms are found to be associated with aggressiveness in NHL (e.g., CD44v6) and the interaction of CD44 isoforms with hyaluronic acid plays a crucial role in cell invasiveness. RG7356, a recombinant anti-CD44 humanised mAb, inhibits cell adhesion and has been associated with macrophage activation in preclinical models. The promising results of a phase-1 trial in relapsed/refractory AML were reported in 2016 [17]. Clinical studies in NHL are yet to be completed.
- − CD47 is an integrin-associated protein and a ligand for the phagocytosis-inhibitory receptor SIRP. It is therefore also recalled as the molecule responsible for the “don’t- eat-me” signal. Various types of NHL including CLL, MCL (mantle-cell lymphoma), and FL and DLBCL, overexpress CD47, which correlates with poor prognosis [18]. Targeting CD47 with a blocking antibody or with RNAi impairs chemokine-controlled migration, promotes macrophage-mediated phagocytosis, and prevents dissemination of malignant B cells in xenograft mouse models [19]. Of particular interest is a bi-specific antibody targeting CD47 and CD19 and developed by Novimmune, which shows significantly higher activity in xenograft mouse models compared to anti-CD19 Abs alone [20].
Table 1 Drugs used for the treatment of non-Hodgkin B cell lymphomas.
Drug
Mechanism |
Swissmedic approved indications for NHL (January 2017)
|
Other approved indications by Swissmedic
|
FDA approved indications in NHL
|
Rituximab
ADCC, CDC, direct cytotoxicity |
Monotherapy of patients with CD20+ follicular lymphoma (stage III and IV) at relapse or refractory to previous chemotherapy.
Treatment of previously untreated patients with CD20+ follicular lymphoma (stage III and IV) in combination with CVP or CHOP. Monotherapy for two year maintenance.
Treatment of CD20pos DLBCL in combination with CHOP.
Treatment of previously untreated CLL in combination with fludarabine and cyclophosphamide. |
Rheumatoid arthritis
ANCA-pos vasculitis (Wegener’s disease) |
For maintenance therapy of untreated CD20pos FL
For CLL.
For CD20pos FL and CD20-pos DLBCL.
Treatment of relapsed or refractory low-grade or follicular CD20+ B-cell NHL. |
Ofatumumab
ADCC, CDC, direct cytotoxicity |
In combination with alkylating agents for previously untreated patients with CLL with comorbidities, for whom a treatment with fludarabine is not possible.
Treatment of CLL progressing after
fludarabine, alemtuzumab and rituximab or for patients for whom these combinations are not adapted. |
|
In combination with chlorambucil, for previously untreated CLL, when fludarabine-based therapy is considered inappropriate.
Extended treatment of patients who are in complete or partial response after at least two lines of therapy for recurrent or progressive CLL.
For CLL refractory to fludarabine and alemtuzumab. |
Obinutuzumab
ADCC, CDC, direct cytotoxicity |
In combination with chlorambucil for the treatment of previously untreated CLL with comorbidities.
In combination with bendamustine for follicular lymphoma refractory to or relapsing after rituximab or a rituximab containing treatment.
Monotherapy for two-year maintenance. |
|
In combination with bendamustine followed by obinutuzumab monotherapy for the treatment of patients with follicular lymphoma, who relapsed after, or are refractory to, a rituximab-containing regimen.
In combination with chlorambucil for previously untreated CLL. |
Brentuximab vedotin
Direct cell toxicity |
For refractory or relapsing anaplastic large cell lymphoma |
CD30+ HL |
Post-ASCT consolidation treatment of patients with classical HL at high risk of relapse or progression. |
Revlimid
Immuno-
modulation and influence of micro-environment |
For refractory or relapsing MCL, after previous therapy with bortezomib, chemotherapy and rituximab containing regimen |
MM
MDS with del5q |
MCL whose disease has relapsed or progressed after two prior therapies, one of which included bortezomib.
Treatment of MM, in combination with dexamethasone
Transfusion-dependent anaemia due to MDS associated with a del 5q abnormality with or without additional cytogenetic abnormalities. |
Pomalidomid
Immuno-
modulation and influence of micro-environment |
Not approved |
MM |
For MM after at least two prior therapies including lenalidomide and bortezomib with demonstrated disease progression on or within 60 days of completion of the last therapy. |
Bortezomib
Proteasome-inhibition |
In combination with rituximab, cyclophosphamide, doxorubicin and prednisone for previously untreated MCL, if not eligible for ASCT.
Refractory or relapsing MCL (stage III and IV) after at least one prior therapy and with proven presence of t(11,14) or cyclin D1 overexpression. Only patients not eligible for ASCT should be treated. |
MM |
For MCL after at least one prior therapy. |
Ibrutinib
Inhibition of BTK kinase activity |
In CLL: first line for unfit patients, for patients with del17 or p53 mutation, or in second line
For MCL as second line treatment
For WM as second line treatment or for patients not eligible for chemo-immunotherapy |
|
Accelerated approval for MCL after at least one prior therapy.
For WM.
For CLL after at least one prior therapy.
For CLL with 17p deletion. |
Idelalisib
Inhibition of PI3K kinase activity |
Not approved |
|
For relapsed CLL, in combination with rituximab, when rituximab alone would be considered appropriate therapy due to other co-morbidities.
Accelerated approval for relapsed FL or relapsed CLL after at least 2 prior therapies. |
Panobinostat
HDAC inhibition |
Not approved |
MM |
|
Temsirolimus
mTOR inhibition |
Not approved |
Renal cell carcinoma |
Not approved by FDA, but approved by EMA for relapsed MCL |
Venetoclax
Bcl-2 inhibition |
Not approved |
|
For CLL with 17p deletion, as detected by an FDA-approved test, after at least one prior therapy. |
Nivolumab
Checkpoint-inhibition |
Not approved |
NSCLC
Melanoma |
|
|
Pembrolizumab Checkpoint-inhibition |
Not approved |
NSCLC.
Melanoma |
|
ASCT
Chemotherapy, direct toxicity |
Approved |
Acute leukaemia, HD |
|
Allogeneic BMT
Chemotherapy, GVL effect |
Approved |
Acute leukaemia |
|
Therapeutic vaccines
Stimulation of immune system |
Not approved |
|
BiovaxIDTM: phase III trials completed in follicular lymphoma. |
CAR T cell therapy
T-cell mediated cytotoxicity |
Not approved |
|
Approval for leukaemia/lymphoma expected in 2017 |
Plerixafor
Blocking of CXCL12/CXCR4 axis |
In combination with G-CSF to improve mobilisation of HSC for ASCT |
MM |
In combination with G-CSF to mobilise HSC for collection and subsequent ASCT in patients with NHL and MM |
Anti-JAM-C
Inhibition of cell homing and proliferation |
Not approved |
|
|
Combined treatments that use antibodies to deliver chemotherapy to lymphoma cells
Some newer antibodies are attached to substances that can poison cancer cells, and are known as immunotoxins or antibody-drug conjugates. The antibodies act as homing devices to deliver the toxins directly to the cancer cells. One example of this is brentuximab vedotin (Adcetris®), which is made up of an antibody to CD30 (brentuximab) that is attached to the cell poison monomethyl auristatin E (MMAE). MMAE cannot be given into the bloodstream on its own because of its potential to affect normal blood cells. Brentuximab vedotin, on the other hand, can be given as an intravenous infusion and is approved in classical presentations of Hodgkin lymphoma and in anaplastic large-cell lymphoma [21, 22] (see table 1 and fig. 1).
Another immunotoxin, known as CAT-3888 (BL22), targets the CD22 antigen on certain lymphoma cells, and contains a toxin known as PE38. This drug showed great promise in treating hairy-cell leukaemia (HCL) in early clinical trials [23]. A newer version of this drug, known as CAT-8015 (moxetumomab pasudotox), is now being studied for use against various subtypes of lymphomas [24].
Possible side effects of treatment with the targeted therapies described above include infusion-related reactions such as shivers, fevers, and other flu-like symptoms, neutropenia, increased risk of infection, but also tumour-lysis syndrome and, very rarely, progressive multifocal leukoencephalopathy (PML), a usually fatal neurological complication caused by the JC virus [25].
Immunomodulators
Immunomodulators have been shown to modulate different components of the immune system such as altering cytokine production, regulating T-cell co-stimulation, and augmenting NK cell cytotoxicity. They also exhibit anti-angiogenic and direct anti-tumour activity, and influence the bone-marrow microenvironment [26, 27].
Lenalidomide (Revlimid®) has shown clinical efficacy in different hematologic diseases such as NHL, multiple myeloma, and myelodysplasia. Currently, approved uses of lenalidomide in Switzerland for NHL include treatment of relapsed/refractory MCL [28] (see table 1 and fig. 1). Third-generation immunomodulators such as pomalidomide are still only approved for use in multiple myeloma.
Possible side effects of lenalidomide include loss of appetite and weight loss, infections, low blood counts and, less frequently, venous thromboembolism.
Proteasome inhibitors
Proteasome inhibitors work by stopping proteasomes in cells from breaking down proteins important for keeping cell division under control. They are most often used to treat multiple myeloma, but can be helpful in treating some types of NHL as well (table 1 and fig. 1).
Bortezomib (Velcade®) is a proteasome inhibitor that is used to treat NHL, usually after other treatments have failed [29, 30]. Although a UK/Swiss phase-III trial (REMoDL-B; NCT01324596) comparing R-CHOP with R-CHOP-bortezomib in ABC- and GC- subgroups of DLBCL did not show any benefits, results in other lymphoma subgroups are more encouraging. This is particularly the case with mantle-cell lymphoma, where bortezomib shows high activity as a monotherapy, and various bortezomib-containing strategies are currently being evaluated in newly diagnosed as well as in relapsed/refractory patients [31, 32].
Bortezomib is given as an IV infusion or a subcutaneous injection. Side effects can be similar to those of standard chemotherapeutic drugs, and frequently include nausea, loss of appetite, low blood counts, and peripheral neuropathy.
Histone deacetylase (HDAC) inhibitors
To control gene expression, the coiling and uncoiling of DNA around histones must be finely orchestrated. This is accomplished with the assistance of histone acetyl transferases, which acetylate the lysine residues in core histones leading to a less compact and more transcriptionally active chromatin. Conversely, the actions of histone deacetylases (HDAC), which remove the acetyl groups from the lysine residues, lead to the formation of a condensed and transcriptionally silenced chromatin. HDAC inhibitors interact with histones, which leads to hyperacetylation. This reversible modification of the terminal tails of core histones constitutes the major epigenetic mechanism for remodelling higher-order chromatin structures and controlling gene expression [33].
Currently, romidepsin (Istodax) and belinostat (Beleodaq) have been approved for the treatment of peripheral and cutaneous T-cell lymphomas, but not yet for the treatment of B- cell NHL [34, 35].
Kinase inhibitors
Ibrutinib (Imbruvica®) targets Bruton’s tyrosine kinase (BTK), which is part of an important intracellular signalling pathway that helps B cells and some lymphoma cells to survive and to proliferate [36]. Ibrutinib is already approved in Switzerland for treatment of CLL, MCL and Waldenstroem’s disease [37, 38] (see table 1 and fig. 1). An on-going Swiss trial investigates the combination of ibrutinib with bortezomib in relapsed/refractory MCL (clinical trial: NCT02356458). Ibrutinib is taken as tablets once daily. Treatment usually continues until disease progression or side effects occur. Common side effects include diarrhoea or constipation, nausea and vomiting, fatigue, swelling, loss of appetite, and low blood counts.
Acalabrutinib (ACP-196) is a more selective and irreversible BTK inhibitor and was specifically designed to improve the safety and efficacy of first-generation BTK inhibitors. In one recent study, this drug was tested in patients with relapsed CLL, including those with chromosome 17p13.1 deletion [39, 40].
Idelalisib (Zydelig) is another kinase inhibitor that blocks a different kinase called PI3K. This drug has been shown to be effective in FL and CLL after other treatments have failed, and is approved for these indications in Switzerland [41, 42]. It is taken orally and usually until disease progression or side effects occur. Common side effects include diarrhoea, fever, fatigue, nausea, cough, pneumonia, abdominal pain, chills, rashes and low blood counts. Several clinical trials were stopped because of serious infectious complications [43].
Temsirolimus (Torisel®)
Temsirolimus targets a pathway known as mammalian target of rapamycin (mTOR) that is implicated in lymphoma cell division. Although temsirolimus has been shown to exhibit some effect in relapsed MCL, it is not yet approved by the FDA, nor in Switzerland [44].
Anti-apoptotic treatments
Anti-apoptotic proteins such as BCL-2 have been shown to play an important role in the pathophysiology of NHL, in particular CLL, and blocking BCL-2 can induce apoptosis in lymphoma cells [45]. Venetoclax (Venclyxt®) is a Bcl-2 inhibitor that is already used in the USA for relapsed CLL harbouring the del17. Approval in Switzerland is still pending [46].
Checkpoint inhibitors
A promising avenue of clinical research in lymphoma is the use of immune checkpoint inhibitors. Immune checkpoints are molecules in the immune system that either turn up a signal (co-stimulatory molecules) or turn down a signal. Many cancers protect themselves from the immune system by inhibiting T cell activation via the TCR. By blocking these inhibitory molecules or, alternatively, activating stimulatory molecules, checkpoint inhibitors are designed to unleash or enhance pre-existing anti-cancer immune responses. Several different checkpoint inhibitors are currently being tested in clinical trials for patients with lymphoma (see fig. 1 and table 1): Nivolumab (Opdivo®) is an anti-PD-1 antibody; pembrolizumab (Keytruda®, MK-3475), atezolizumab (Tecentriq™, MPDL3280A), Durvalumab (MEDI473) are all anti-PD-L1 antibodies; and ipilimumab (Yervoy®) and tremelimumab are anti-CTLA-4 antibodies [47, 48]. Particularly promising results have already been obtained in heavily pre-treated refractory/relapsed Hodgkin lymphoma with an ORR of nearly 90% [49]. Currently, checkpoint inhibitor antibodies are not approved for the treatment of NHL in Switzerland.
Bone marrow and peripheral blood stem cell transplants
Researchers continue to improve bone marrow and peripheral blood stem-cell transplant methods, including new ways to collect these cells before the transplant [50].
Autologous transplants run the risk of reintroducing lymphoma cells back into the patient after treatment. New and improved ways are studied to remove residual lymphoma cells from the stem cells before they are transfused back to the patient. Some of the new monoclonal antibodies described above are used in this context [51].
Intense research efforts are also focusing on eliminating graft-versus-host disease in allogeneic transplants, by altering the transplanted T-cells so that they do not react with the recipient’s normal cells but still eliminate the lymphoma cells [52].
The effectiveness of non-myeloablative (reduced-intensity) stem-cell transplants in patients with lymphoma is also being investigated in several studies [53].
Therapeutic vaccines
Unlike vaccines against infections, tumour vaccines are developed to treat, not to prevent, lymphomas. They are designed to elicit an immune response against tumour-specific or tumour-associated antigens in situations where patients are at a very early stage of their disease or where the disease is in remission. Some of these vaccines are administered intravenously while others are injected directly into a single lymphoma site (“in-situ vaccination”) with the aim of inducing an immune response that subsequently spreads throughout the body to attack lymphoma cells residing elsewhere [54, 55].
Biovax is a vaccine based on the unique immunoglobulin idiotype expressed on the surface of a patient’s lymphoma B cells [56]. The vaccine uses the idiotype isolated from the lymphoma cells, which are obtained during a biopsy. This tumour idiotype is combined with an adjuvant, a carrier protein that boosts the body’s immune response when the combination is injected into the patient. Clinical trials in FL and MCL are on-going.
Immunotransplantation, a treatment strategy in which a vaccine is given in combination with autologous stem-cell transplantation, is under investigation at Stanford University. In patients with MCL, the lymphoma cells are first activated with CpG, a toll-like receptor agonist, and then used as a vaccine when patients are in remission after chemotherapy. This stimulates the immune system to produce lymphoma-specific T cells, which are then taken from the patient and given back along with the stem cells after high dose chemotherapy [57].
Adoptive T-cell therapy
In adoptive T-cell therapy, T cells are removed from a patient, genetically modified or treated with chemicals to enhance their activity, and then re-introduced into the patient, often in vastly increased numbers. The T cells then seek out and destroy the cancer.
One specific form of this approach, “chimeric antigen receptor (CAR) T-cell therapy”, has been shown in early clinical trials to be particularly effective at treating B-ALL and lymphoma. In this strategy, T cells from a patient are removed and then genetically modified to express a receptor that recognises, independently from the MHC, a particular antigen found on the tumour cells. This receptor is called “chimeric” because it consists of a fusion protein with an extracellular target binding domain derived from the single-variable fragment of an antibody (scFv), a spacer domain, a transmembrane domain, and an intracellular signalling domain containing CD3zeta linked with zero, one or two co-stimulatory domains, such as CD28 or CD137 [58, 59]. Although highly promising and already granted breakthrough therapy designation by the FDA for relapsed B-ALL and DLBCL, several challenges to the broad application of CAR-T cell therapy in the future remain: (1) tumour editing leading to antigen escape, thus rendering CAR-T cells ineffective. This has mainly been observed in anti-CD19 CAR-T cells in B-ALL. (2) On-target but off-tumour toxicity since the majority of CAR targets are tumour-associated antigens that are overexpressed on tumour cells, but also shared by normal bystander cells. Severe and life-threatening toxicities have been observed, especially in solid tumours. (3) Difficulty of industrialised production, because of personalised autologous T-cell manufacture. How to surmount these hurdles and increase therapeutic safety currently presents the principal direction of CAR-T cell-therapy development [60].
Inhibiting B-cell migration and B-cell homing
B cells need the microenvironment of bone marrow, spleen, lymph nodes or similar niches to survive and to proliferate [61, 62]. Inhibiting the homing of B cells circulating within the blood stream to these niches could constitute an alternative strategy for the treatment of NHL.
JAMs (junctional adhesion molecules) are cell-surface glycoproteins belonging to the Ig superfamily. JAMs are generally expressed in subsets of leukocytes (e.g., activated T cells and NK cells) and epithelial and endothelial cells, where JAM-C is localised at tight junctions of blood and lymphatic vessels [63]. It binds JAM-B, another member of the JAM family, and can also establish interactions with VLA-4 and CD11b/CD18 (Mac-1) integrins on leukocytes [64–66]. It is well established that JAMs are involved in the control of vascular permeability, leukocyte transendothelial migration, angiogenesis, and tumour progression [67–69].
In our own laboratories, we have conducted a series of studies on the expression and function of JAM-C in normal and malignant B cells. We have shown that a population of normal B cells expresses JAM-C and that the expression pattern of JAM-C allows distinction of CD27+ memory B cells homing to the germinal centres, and from B cells located outside of the germinal centres, the former being JAM-Cneg and the latter JAM-Cpos. Furthermore, two categories of NHL were identified based on JAM-C expression i.e., JAM-Cneg lymphomas, including CLL, FL, and DLBCL, and JAM-Cpos lymphomas, including marginal zone B-cell lymphomas, MCL, and hairy cell leukaemia [70]. As JAM-C plays a role in neutrophil and monocyte migration, we have investigated whether JAM-C is also involved in B-cell migration. With the use of an in-vivo assay, we were able to show that anti-JAM-C antibodies decrease the homing of B cells to lymphatic organs (bone marrow, spleen, and lymph nodes). This effect was complementary to that of an anti-VLA-4 antibody, which decreased B-cell homing to bone marrow and lymph nodes but not to the spleen. When JAM-C+ lymphoma B cells were tested in the same assay, the results obtained were similar to those achieved with normal B cells, but the inhibition of lymph-node homing was of a higher degree [71].
Subsequently, we have completed in-depth investigation into the effects of JAM-C on the in-vivo growth and dissemination of MCL cells, and have developed a novel, preclinical therapeutic strategy using anti-JAM-C monoclonal antibodies [72]. MCL cells were generated in immunodeficient NOD/SCID mice by intravenous injection of a human MCL cell line. Treatment of the mice with an anti-JAM-C mAb virtually abolished MCL cell homing to the spleen, liver, bone marrow, and lymph nodes. This effect on the homing of MCL cells was accompanied by an effect on tumour size when mice were treated with the mAb for several weeks. Therefore, the anti-JAM-C mAb affects not only homing of MCL cells but also their proliferation.
Inhibition of MCL cell homing to lymphoid tissue by blocking the JAM-C molecule with monoclonal antibodies is a novel and promising strategy to interfere with B-cell lymphoma development.
A second approach aiming at influencing B-cell migration centres on the chemokine/receptor CXCL12/CXCR4 axis. The chemokine CXCL12 signals through its receptor CXCR4, which are expressed by normal and malignant cells of hematopoietic lineages. Data from knockout mice indicate that the CXCR4 plays an important role in haematopoiesis, in particular in the homing and retention of haematopoietic progenitor cells in the microenvironment of the bone marrow [73]. Overexpression of CXCR4 has been found in 75% of cancers, including leukaemias and lymphomas. This receptor plays a critical role in B-cell migration into the bone marrow where CXCL12 is expressed and where B-cell growth and survival is supported. Furthermore, blockade of the CXCL12/CXCR4 axis was shown to attenuate tumour growth in multiple myeloma tumour models. It was also associated with treatment resistance, notably in AML, where the resistance of residual, post-chemotherapy blasts to additional chemotherapeutic agents constitutes a major problem [74].
Plerixafor (Mozobil) is a small molecule antagonist of CXCR4 that mobilises hematopoietic stem cells into the bloodstream. It was approved by the FDA in 2008 for administration in combination with granulocyte colony-stimulating factor to enhance the mobilisation of stem cells to the peripheral blood supply for collection and subsequent autologous transplantation in patients with lymphoma and multiple myeloma. Over the past few years, clinical trials have been initiated using several CXCR4 antagonists (plerixafor as well as mAbs) in patients with haematological malignancies in combination with anticancer drugs [75]. In particular, plerixafor and the IgG4 mAb BMS-936564 are now undergoing phase I and phase II clinical trials for several indications, including NHL and CLL, multiple myeloma, and AML [76–78].
Other examples of anti-tumour activity operated by inhibitors of cell migration include:
- − CD44, a multifunctional cell surface glycoprotein that binds to Hyaluronan, a non-sulphated glycosaminoglycan distributed throughout the extracellular matrix. Studies have shown that binding of Hyaluronan to CD44 in cancer cells activates survival pathways resulting in cancer-cell survival [79]. This effect can be blocked by anti-CD44 monoclonal antibodies. A6, a peptide derived from the human serine protease urokinase plasminogen activator (uPa), binds to CD44. This results in the inhibition of migration, invasion, and metastasis of tumour cells [80]. Recently, A6 has also been shown to be directly cytotoxic for CLL B-lymphocytes expressing the kinase ZAP-70 [81]. In an established CLL xenograft model, A6 treatment resulted in 80- 90% reduction in CLL burden [82]. Clinical trials in CLL are expected to start in the near future.
- − Bruton’s tyrosine kinase (BTK), a key component of the BCR pathway, which mediates B lymphocyte adhesion and survival [83]. BTK also plays a role in chemokine (such as CXCL12) -controlled B-cell chemotaxis and homing [84]. Ibrutinib suppresses these activities, as well as migration of lymphocytes beneath stromal cells (pseudo-emperipoiesis). In-vitro studies with MCL have shown that Ibrutinib treatment leads to loss of adhesion and migratory ability on stromal cell layers [85]. These observations could explain why lymphocyte numbers increase in peripheral circulation after Ibrutinib administration.
- − CCR7, a chemokine receptor that is expressed on naïve and memory lymphocytes and mature dendritic cells. It allows B lymphocytes to respond to the CCR7 ligands CCL21 and CCL19 produced in secondary lymphoid organs, and to enter survival niches through the endothelium of high-endothelial venules [86]. Consistent with their lymphoid origin, many leukaemias and lymphomas express CCR7 [87], and it was shown that CCR7 plays a major role in the migration and nodular dissemination of certain NHL, including CLL and MCL [88]. In a NOD/SCID xenograft mouse model, anti-CCR7 mAb’s drastically increased survival of the mice by nearly abrogating dissemination and infiltration of tumour cells in lymphoid and non-lymphoid organs, including the lungs and central nervous system [89].
In conclusion, a multitude of novel molecular targets have been discovered recently and new treatment strategies have been developed. This is urgently needed because lymphomas still remain mostly incurable diseases that decrease the life expectancy of patients. The main challenge in the coming years will be to bring these preclinical discoveries to the bedside and to incorporate them into traditional treatment approaches.
References
1
Felicitas Hitz
VA
, Matthias Lorez, and the NICER Working Group. Survival Trends for non- Hodgkin lymphoma patients in Switzerland. Schweizer Krebsbulletin. 2015;1:61–6.
2
Plosker
GL
,
Figgitt
DP
. Rituximab: a review of its use in non-Hodgkin’s lymphoma and chronic lymphocytic leukaemia. Drugs. 2003;63(8):803–43 .https://doi.org/10.2165/00003495-200363080-00005
3
Coiffier
B
,
Lepage
E
,
Briere
J
,
Herbrecht
R
,
Tilly
H
,
Bouabdallah
R
, et al.
CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 2002;346(4):235–42 .https://doi.org/10.1056/NEJMoa011795
4
Raderer
M
,
Kiesewetter
B
,
Ferreri
AJ
. Clinicopathologic characteristics and treatment of marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma). CA Cancer J Clin. 2016;66(2):153–71 .https://doi.org/10.3322/caac.21330
5
Foster
LH
,
Portell
CA
. The role of infectious agents, antibiotics, and antiviral therapy in the treatment of extranodal marginal zone lymphoma and other low-grade lymphomas. Curr Treat Options Oncol. 2015;16(6):28 .https://doi.org/10.1007/s11864-015-0344-6
6
Annibali
O
,
Sabatino
F
,
Mantelli
F
,
Olimpieri
OM
,
Bonini
S
,
Avvisati
G
. Review article: Mucosa-associated lymphoid tissue (MALT)-type lymphoma of ocular adnexa. Biology and treatment. Crit Rev Oncol Hematol. 2016;100:37–45 .https://doi.org/10.1016/j.critrevonc.2016.01.009
7
Ferreri
AJ
,
Govi
S
,
Pasini
E
,
Mappa
S
,
Bertoni
F
,
Zaja
F
, et al.
Chlamydophila psittaci eradication with doxycycline as first-line targeted therapy for ocular adnexae lymphoma: final results of an international phase II trial. J Clin Oncol. 2012;30(24):2988–94 .https://doi.org/10.1200/JCO.2011.41.4466
8
Pescovitz
MD
. Rituximab, an anti-cd20 monoclonal antibody: history and mechanism of action. Am J Transplant. 2006;6(5 Pt 1):859–66 .https://doi.org/10.1111/j.1600-6143.2006.01288.x
9
Herter
S
,
Herting
F
,
Mundigl
O
,
Waldhauer
I
,
Weinzierl
T
,
Fauti
T
, et al.
Preclinical activity of the type II CD20 antibody GA101 (obinutuzumab) compared with rituximab and ofatumumab in vitro and in xenograft models. Mol Cancer Ther. 2013;12(10):2031–42 .https://doi.org/10.1158/1535-7163.MCT-12-1182
10
Grosicki
S
. Ofatumumab for the treatment of chronic lymphocytic leukemia. Expert Rev Hematol. 2015;8(3):265–72 .https://doi.org/10.1586/17474086.2015.1037736
11
Al-Sawaf
O
,
Fischer
K
,
Engelke
A
,
Pflug
N
,
Hallek
M
,
Goede
V
. Obinutuzumab in chronic lymphocytic leukemia: design, development and place in therapy. Drug Des Devel Ther. 2017;11:295–304 .https://doi.org/10.2147/DDDT.S104869
12
Marcus
RE
,
Davies
DA
,
Ando
K
,
Klapper
W
,
Opat
S
,
Owen
CJ
, et al.
Obinutuzumab-Based Induction and Maintenance Prolongs Progression-Free Survival (PFS) in Patients with Previously Untreated Follicular Lymphoma: Primary Results of the Randomized Phase 3 GALLIUM Study. Blood. 2017;128:6.
13
Micallef
IN
,
Maurer
MJ
,
Wiseman
GA
,
Nikcevich
DA
,
Kurtin
PJ
,
Cannon
MW
, et al.
Epratuzumab with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone chemotherapy in patients with previously untreated diffuse large B-cell lymphoma. Blood. 2011;118(15):4053–61 .https://doi.org/10.1182/blood-2011-02-336990
14
Onuora
S
. Systemic lupus erythematosus: Epratuzumab not effective in phase III trials. Nat Rev Rheumatol. 2016;12(11):622. doi:.https://doi.org/10.1038/nrrheum.2016.165
15
Repetto-Llamazares
AH
,
Larsen
RH
,
Patzke
S
,
Fleten
KG
,
Didierlaurent
D
,
Pichard
A
, et al.
Targeted Cancer Therapy with a Novel Anti-CD37 Beta-Particle Emitting Radioimmunoconjugate for Treatment of Non-Hodgkin Lymphoma. PLoS One. 2015;10(6):e0128816 .https://doi.org/10.1371/journal.pone.0128816
16
Pereira
DS
,
Guevara
CI
,
Jin
L
,
Mbong
N
,
Verlinsky
A
,
Hsu
SJ
, et al.
AGS67E, an Anti-CD37 Monomethyl Auristatin E Antibody-Drug Conjugate as a Potential Therapeutic for B/T-Cell Malignancies and AML: A New Role for CD37 in AML. Mol Cancer Ther. 2015;14(7):1650–60 .https://doi.org/10.1158/1535-7163.MCT-15-0067
17
Vey
N
,
Delaunay
J
,
Martinelli
G
,
Fiedler
W
,
Raffoux
E
,
Prebet
T
, et al.
Phase I clinical study of RG7356, an anti-CD44 humanized antibody, in patients with acute myeloid leukemia. Oncotarget. 2016;7(22):32532–42 .https://doi.org/10.18632/oncotarget.8687
18
Chao
MP
,
Alizadeh
AA
,
Tang
C
,
Myklebust
JH
,
Varghese
B
,
Gill
S
, et al.
Anti-CD47 antibody synergizes with rituximab to promote phagocytosis and eradicate non-Hodgkin lymphoma. Cell. 2010;142(5):699–713 .https://doi.org/10.1016/j.cell.2010.07.044
19
Piccione
EC
,
Juarez
S
,
Liu
J
,
Tseng
S
,
Ryan
CE
,
Narayanan
C
, et al.
A bispecific antibody targeting CD47 and CD20 selectively binds and eliminates dual antigen expressing lymphoma cells. MAbs. 2015;7(5):946–56 .https://doi.org/10.1080/19420862.2015.1062192
20
Ferlin
WG
,
Chauchet
X
,
Buatois
V
,
Salgado-Pires
S
,
Shang
L
,
Dheilly
E
, et al.
A CD47xCD19 bispecific antibody that remodels the tumor microenvironment for improved killing and provokes a memory immune response to cancer B cells. Blood. 2016;128:44.
21
Pro
B
,
Advani
R
,
Brice
P
,
Bartlett
NL
,
Rosenblatt
JD
,
Illidge
T
, et al.
Brentuximab vedotin (SGN-35) in patients with relapsed or refractory systemic anaplastic large-cell lymphoma: results of a phase II study. J Clin Oncol. 2012;30(18):2190–6 .https://doi.org/10.1200/JCO.2011.38.0402
22
Scott
LJ
. Brentuximab Vedotin: A Review in CD30-Positive Hodgkin Lymphoma. Drugs. 2017;77(4):435–45 .https://doi.org/10.1007/s40265-017-0705-5
23
Kreitman
RJ
,
Stetler-Stevenson
M
,
Margulies
I
,
Noel
P
,
Fitzgerald
DJ
,
Wilson
WH
, et al.
Phase II trial of recombinant immunotoxin RFB4(dsFv)-PE38 (BL22) in patients with hairy cell leukemia. J Clin Oncol. 2009;27(18):2983–90 .https://doi.org/10.1200/JCO.2008.20.2630
24
Jain
P
,
Polliack
A
,
Ravandi
F
. Novel therapeutic options for relapsed hairy cell leukemia. Leuk Lymphoma. 2015;56(8):2264–72 .https://doi.org/10.3109/10428194.2014.1001988
25
Wick
W
,
Hertenstein
A
,
Platten
M
. Neurological sequelae of cancer immunotherapies and targeted therapies. Lancet Oncol. 2016;17(12):e529–41 .https://doi.org/10.1016/S1470-2045(16)30571-X
26
Riches
JC
,
Gribben
JG
. Mechanistic and Clinical Aspects of Lenalidomide Treatment for Chronic Lymphocytic Leukemia. Curr Cancer Drug Targets. 2016;16(8):689–700 .https://doi.org/10.2174/1568009616666160408145741
27
Maffei
R
,
Fiorcari
S
,
Bulgarelli
J
,
Rizzotto
L
,
Martinelli
S
,
Rigolin
GM
, et al.
Endothelium-mediated survival of leukemic cells and angiogenesis-related factors are affected by lenalidomide treatment in chronic lymphocytic leukemia. Exp Hematol. 2014;42(2):126–36.e1 .https://doi.org/10.1016/j.exphem.2013.10.007
28
Arora
M
,
Gowda
S
,
Tuscano
J
. A comprehensive review of lenalidomide in B-cell non-Hodgkin lymphoma. Ther Adv Hematol. 2016;7(4):209–21 .https://doi.org/10.1177/2040620716652861
29
Arkwright
R
,
Pham
TM
,
Zonder
JA
,
Dou
QP
. The preclinical discovery and development of bortezomib for the treatment of mantle cell lymphoma. Expert Opin Drug Discov. 2017;12(2):225–35 .https://doi.org/10.1080/17460441.2017.1268596
30
Gu
JJ
,
Kaufman
GP
,
Mavis
C
,
Czuczman
MS
,
Hernandez-Ilizaliturri
FJ
. Mitotic catastrophe and cell cycle arrest are alternative cell death pathways executed by bortezomib in rituximab resistant B-cell lymphoma cells. Oncotarget. 2017;8(8):12741–53. doi:.https://doi.org/10.18632/oncotarget.14405
31
Vallumsetla
N
,
Paludo
J
,
Kapoor
P
. Bortezomib in mantle cell lymphoma: comparative therapeutic outcomes. Ther Clin Risk Manag. 2015;11:1663–74. doi:.https://doi.org/10.2147/TCRM.S72943
32
Robak
T
,
Huang
H
,
Jin
J
,
Zhu
J
,
Liu
T
,
Samoilova
O
, et al.; LYM-3002 Investigators. Bortezomib-based therapy for newly diagnosed mantle-cell lymphoma. N Engl J Med. 2015;372(10):944–53 .https://doi.org/10.1056/NEJMoa1412096
33
Olzscha
H
,
Sheikh
S
,
La Thangue
NB
. Deacetylation of chromatin and gene expression regulation: a new target for epigenetic therapy. Crit Rev Oncog. 2015;20(1-2):1–17 .https://doi.org/10.1615/CritRevOncog.2014012463
34
Broccoli
A
,
Zinzani
PL
. Peripheral T-cell lymphoma, not otherwise specified. Blood. 2017;129(9):1103–12 .https://doi.org/10.1182/blood-2016-08-692566
35
Holkova
B
,
Yazbeck
V
,
Kmieciak
M
,
Bose
P
,
Ma
S
,
Kimball
A
, et al.
A phase 1 study of bortezomib and romidepsin in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma, indolent B-cell lymphoma, peripheral T-cell lymphoma, or cutaneous T-cell lymphoma. Leuk Lymphoma. 2017;58(6):1349–57 .https://doi.org/10.1080/10428194.2016.1276287
36
Roskoski
R, Jr
. Ibrutinib inhibition of Bruton protein-tyrosine kinase (BTK) in the treatment of B cell neoplasms. Pharmacol Res. 2016;113(Pt A):395–408 .https://doi.org/10.1016/j.phrs.2016.09.011
37
Deeks
ED
. Ibrutinib: A Review in Chronic Lymphocytic Leukaemia. Drugs. 2017;77(2):225–36 .https://doi.org/10.1007/s40265-017-0695-3
38
Gertz
MA
. Waldenström macroglobulinemia: 2017 update on diagnosis, risk stratification, and management. Am J Hematol. 2017;92(2):209–17 .https://doi.org/10.1002/ajh.24557
39
Patel
V
,
Balakrishnan
K
,
Bibikova
E
,
Ayres
M
,
Keating
MJ
,
Wierda
WG
, et al.
Comparison of Acalabrutinib, A Selective Bruton Tyrosine Kinase Inhibitor, with Ibrutinib in Chronic Lymphocytic Leukemia Cells. Clin Cancer Res. 2017;23(14):3734–43 .https://doi.org/10.1158/1078-0432.CCR-16-1446
40
Byrd
JC
,
Harrington
B
,
O’Brien
S
,
Jones
JA
,
Schuh
A
,
Devereux
S
, et al.
Acalabrutinib (ACP-196) in Relapsed Chronic Lymphocytic Leukemia. N Engl J Med. 2016;374(4):323–32 .https://doi.org/10.1056/NEJMoa1509981
41
Barrientos
JC
. Idelalisib for the treatment of chronic lymphocytic leukemia/small lymphocytic lymphoma. Future Oncol. 2016;12(18):2077–94 .https://doi.org/10.2217/fon-2016-0003
42
Barrientos
JC
. Sequencing of chronic lymphocytic leukemia therapies. Hematology (Am Soc Hematol Educ Program). 2016;2016(1):128–36 .https://doi.org/10.1182/asheducation-2016.1.128
43
Nair
KS
,
Cheson
B
. The role of idelalisib in the treatment of relapsed and refractory chronic lymphocytic leukemia. Ther Adv Hematol. 2016;7(2):69–84 .https://doi.org/10.1177/2040620715625966
44
Calimeri
T
,
Ferreri
AJM
. m-TOR inhibitors and their potential role in haematological malignancies. Br J Haematol. 2017;177(5):684–702 .https://doi.org/10.1111/bjh.14529
45
Lampson
BL
,
Davids
MS
. The Development and Current Use of BCL-2 Inhibitors for the Treatment of Chronic Lymphocytic Leukemia. Curr Hematol Malig Rep. 2017;12(1):11–9 .https://doi.org/10.1007/s11899-017-0359-0
46
Roberts
AW
,
Stilgenbauer
S
,
Seymour
JF
,
Huang
DCS
. Venetoclax in patients with previously treated chronic lymphocytic leukemia. Clin Cancer Res. 2017;23(16):4527–33 .https://doi.org/10.1158/1078-0432.CCR-16-0955
47
Galanina
N
,
Kline
J
,
Bishop
MR
. Emerging role of checkpoint blockade therapy in lymphoma. Ther Adv Hematol. 2017;8(2):81–90 .https://doi.org/10.1177/2040620716673787
48
Hude
I
,
Sasse
S
,
Engert
A
,
Bröckelmann
PJ
. The emerging role of immune checkpoint inhibition in malignant lymphoma. Haematologica. 2017;102(1):30–42 .https://doi.org/10.3324/haematol.2016.150656
49
Ansell
SM
,
Lesokhin
AM
,
Borrello
I
,
Halwani
A
,
Scott
EC
,
Gutierrez
M
, et al.
PD-1 blockade with nivolumab in relapsed or refractory Hodgkin’s lymphoma. N Engl J Med. 2015;372(4):311–9 .https://doi.org/10.1056/NEJMoa1411087
50
Kuruvilla
J
. The role of autologous and allogeneic stem cell transplantation in the management of indolent B-cell lymphoma. Blood. 2016;127(17):2093–100 .https://doi.org/10.1182/blood-2015-11-624320
51
Stiff
P
. What is the role of autologous transplant for lymphoma in the current era?
Hematology (Am Soc Hematol Educ Program). 2015;2015(1):74–81 .https://doi.org/10.1182/asheducation-2015.1.74
52
Merryman
RW
,
Kim
HT
,
Zinzani
PL
,
Carlo-Stella
C
,
Ansell
SM
,
Perales
MA
, et al.
Safety and efficacy of allogeneic hematopoietic stem cell transplant after PD-1 blockade in relapsed/refractory lymphoma. Blood. 2017;129(10):1380–8 .https://doi.org/10.1182/blood-2016-09-738385
53
Hong
S
,
Le-Rademacher
J
,
Artz
A
,
McCarthy
PL
,
Logan
BR
,
Pasquini
MC
. Comparison of non-myeloablative conditioning regimens for lymphoproliferative disorders. Bone Marrow Transplant. 2015;50(3):367–74 .https://doi.org/10.1038/bmt.2014.269
54
Allegra
A
,
Russo
S
,
Gerace
D
,
Calabrò
L
,
Maisano
V
,
Innao
V
, et al.
Vaccination strategies in lymphoproliferative disorders: Failures and successes. Leuk Res. 2015;39(10):1006–19 .https://doi.org/10.1016/j.leukres.2015.08.001
55
Iribarren
K
,
Bloy
N
,
Buqué
A
,
Cremer
I
,
Eggermont
A
,
Fridman
WH
, et al.
Trial Watch: Immunostimulation with Toll-like receptor agonists in cancer therapy. OncoImmunology. 2015;5(3):e1088631 .https://doi.org/10.1080/2162402X.2015.1088631
56
Lee
ST
,
Jiang
YF
,
Park
KU
,
Woo
AF
,
Neelapu
SS
. BiovaxID: a personalized therapeutic cancer vaccine for non-Hodgkin’s lymphoma. Expert Opin Biol Ther. 2007;7(1):113–22 .https://doi.org/10.1517/14712598.7.1.113
57
Brody
J
,
Levy
R
. Lymphoma immunotherapy: vaccines, adoptive cell transfer and immunotransplant. Immunotherapy. 2009;1(5):809–24 .https://doi.org/10.2217/imt.09.50
58
Kochenderfer
JN
,
Dudley
ME
,
Kassim
SH
,
Somerville
RP
,
Carpenter
RO
,
Stetler-Stevenson
M
, et al.
Chemotherapy-refractory diffuse large B-cell lymphoma and indolent B-cell malignancies can be effectively treated with autologous T cells expressing an anti-CD19 chimeric antigen receptor. J Clin Oncol. 2015;33(6):540–9 .https://doi.org/10.1200/JCO.2014.56.2025
59
Locke
FL
,
Neelapu
SS
,
Bartlett
NL
,
Siddiqi
T
,
Chavez
JC
,
Hosing
CM
, et al.
Phase 1 Results of ZUMA-1: A Multicenter Study of KTE-C19 Anti-CD19 CAR T Cell Therapy in Refractory Aggressive Lymphoma. Mol Ther. 2017;25(1):285–95 .https://doi.org/10.1016/j.ymthe.2016.10.020
60
Wang
Z
,
Wu
Z
,
Liu
Y
,
Han
W
. New development in CAR-T cell therapy. J Hematol Oncol. 2017;10(1):53 .https://doi.org/10.1186/s13045-017-0423-1
61
Crassini
K
,
Shen
Y
,
Mulligan
S
,
Giles Best
O
. Modeling the chronic lymphocytic leukemia microenvironment in vitro. Leuk Lymphoma. 2017;58(2):266–79 .https://doi.org/10.1080/10428194.2016.1204654
62
Fowler
NH
,
Cheah
CY
,
Gascoyne
RD
,
Gribben
J
,
Neelapu
SS
,
Ghia
P
, et al.
Role of the tumor microenvironment in mature B-cell lymphoid malignancies. Haematologica. 2016;101(5):531–40 .https://doi.org/10.3324/haematol.2015.139493
63
Luissint
AC
,
Nusrat
A
,
Parkos
CA
. JAM-related proteins in mucosal homeostasis and inflammation. Semin Immunopathol. 2014;36(2):211–26 .https://doi.org/10.1007/s00281-014-0421-0
64
Arrate
MP
,
Rodriguez
JM
,
Tran
TM
,
Brock
TA
,
Cunningham
SA
. Cloning of human junctional adhesion molecule 3 (JAM3) and its identification as the JAM2 counter-receptor. J Biol Chem. 2001;276(49):45826–32 .https://doi.org/10.1074/jbc.M105972200
65
Cunningham
SA
,
Rodriguez
JM
,
Arrate
MP
,
Tran
TM
,
Brock
TA
. JAM2 interacts with alpha4beta1. Facilitation by JAM3. J Biol Chem. 2002;277(31):27589–92 .https://doi.org/10.1074/jbc.C200331200
66
Liang
TW
,
Chiu
HH
,
Gurney
A
,
Sidle
A
,
Tumas
DB
,
Schow
P
, et al.
Vascular endothelial-junctional adhesion molecule (VE-JAM)/JAM 2 interacts with T, NK, and dendritic cells through JAM 3. J Immunol. 2002;168(4):1618–26 .https://doi.org/10.4049/jimmunol.168.4.1618
67
Woodfin
A
,
Voisin
MB
,
Beyrau
M
,
Colom
B
,
Caille
D
,
Diapouli
FM
, et al.
The junctional adhesion molecule JAM-C regulates polarized transendothelial migration of neutrophils in vivo. Nat Immunol. 2011;12(8):761–9 .https://doi.org/10.1038/ni.2062
68
Bradfield
PF
,
Scheiermann
C
,
Nourshargh
S
,
Ody
C
,
Luscinskas
FW
,
Rainger
GE
, et al.
JAM-C regulates unidirectional monocyte transendothelial migration in inflammation. Blood. 2007;110(7):2545–55 .https://doi.org/10.1182/blood-2007-03-078733
69
Lamagna
C
,
Hodivala-Dilke
KM
,
Imhof
BA
,
Aurrand-Lions
M
. Antibody against junctional adhesion molecule-C inhibits angiogenesis and tumor growth. Cancer Res. 2005;65(13):5703–10 .https://doi.org/10.1158/0008-5472.CAN-04-4012
70
Ody
C
,
Jungblut-Ruault
S
,
Cossali
D
,
Barnet
M
,
Aurrand-Lions
M
,
Imhof
BA
, et al.
Junctional adhesion molecule C (JAM-C) distinguishes CD27+ germinal center B lymphocytes from non-germinal center cells and constitutes a new diagnostic tool for B-cell malignancies. Leukemia. 2007;21(6):1285–93 .https://doi.org/10.1038/sj.leu.2404689
71
Doñate
C
,
Ody
C
,
McKee
T
,
Ruault-Jungblut
S
,
Fischer
N
,
Ropraz
P
, et al.
Homing of human B cells to lymphoid organs and B-cell lymphoma engraftment are controlled by cell adhesion molecule JAM-C. Cancer Res. 2013;73(2):640–51 .https://doi.org/10.1158/0008-5472.CAN-12-1756
72
Doñate
C
,
Vijaya Kumar
A
,
Imhof
BA
,
Matthes
T
. Anti-JAM-C therapy eliminates tumor engraftment in a xenograft model of mantle cell lymphoma. J Leukoc Biol. 2016;100(5):843–53 .https://doi.org/10.1189/jlb.1HI1114-549RR
73
Karpova
D
,
Bonig
H
. Concise Review: CXCR4/CXCL12 Signaling in Immature Hematopoiesis--Lessons From Pharmacological and Genetic Models. Stem Cells. 2015;33(8):2391–9 .https://doi.org/10.1002/stem.2054
74
Rashidi
A
,
Uy
GL
. Targeting the microenvironment in acute myeloid leukemia. Curr Hematol Malig Rep. 2015;10(2):126–31 .https://doi.org/10.1007/s11899-015-0255-4
75
Barbieri
F
,
Bajetto
A
,
Thellung
S
,
Würth
R
,
Florio
T
. Drug design strategies focusing on the CXCR4/CXCR7/CXCL12 pathway in leukemia and lymphoma. Expert Opin Drug Discov. 2016;11(11):1093–109 .https://doi.org/10.1080/17460441.2016.1233176
76
Shaughnessy
P
,
Uberti
J
,
Devine
S
,
Maziarz
RT
,
Vose
J
,
Micallef
I
, et al.
Plerixafor and G-CSF for autologous stem cell mobilization in patients with NHL, Hodgkin’s lymphoma and multiple myeloma: results from the expanded access program. Bone Marrow Transplant. 2013;48(6):777–81 .https://doi.org/10.1038/bmt.2012.219
77
Uy
GL
,
Rettig
MP
,
Motabi
IH
,
McFarland
K
,
Trinkaus
KM
,
Hladnik
LM
, et al.
A phase 1/2 study of chemosensitization with the CXCR4 antagonist plerixafor in relapsed or refractory acute myeloid leukemia. Blood. 2012;119(17):3917–24 .https://doi.org/10.1182/blood-2011-10-383406
78
Kashyap
MK
,
Kumar
D
,
Jones
H
,
Amaya-Chanaga
CI
,
Choi
MY
,
Melo-Cardenas
J
, et al.
Ulocuplumab (BMS-936564 / MDX1338): a fully human anti-CXCR4 antibody induces cell death in chronic lymphocytic leukemia mediated through a reactive oxygen species-dependent pathway. Oncotarget. 2016;7(3):2809–22 .https://doi.org/10.18632/oncotarget.6465
79
Herishanu
Y
,
Gibellini
F
,
Njuguna
N
,
Hazan-Halevy
I
,
Farooqui
M
,
Bern
S
, et al.
Activation of CD44, a receptor for extracellular matrix components, protects chronic lymphocytic leukemia cells from spontaneous and drug induced apoptosis through MCL-1. Leuk Lymphoma. 2011;52(9):1758–69 .https://doi.org/10.3109/10428194.2011.569962
80
Finlayson
M
. Modulation of CD44 Activity by A6-Peptide. Front Immunol. 2015;6:135 .https://doi.org/10.3389/fimmu.2015.00135
81Lai H. S. Z., Christina Wu, Liguang Chen, Grace Liu, RongRong Wu, Fitzgerlad Lao, Jian Yu, Laura Rassenti, Michael Choi, Stephen Howell, Malcolm Finlayson, Thomas Kipps. in Proceedings of the 105th Annual Meeting of the American Association for Cancer Research Vol. 2014 Apr 5-9; San Diego, CA. Philadelphia (PA): AACR; (2014).
82
Zhang
S
,
Lai
H
,
Liu
G
,
Rassenti
L
,
Choi
MY
,
Howell
SB
, et al.
A6 peptide is selectively cytotoxic for chronic lymphocytic leukemia cells. Blood. 2013;122(21):5303.
83
Gayko
U
,
Fung
M
,
Clow
F
,
Sun
S
,
Faust
E
,
Price
S
, et al.
Development of the Bruton’s tyrosine kinase inhibitor ibrutinib for B cell malignancies. Ann N Y Acad Sci. 2015;1358(1):82–94 .https://doi.org/10.1111/nyas.12878
84
de Gorter
DJ
,
Beuling
EA
,
Kersseboom
R
,
Middendorp
S
,
van Gils
JM
,
Hendriks
RW
, et al.
Bruton’s tyrosine kinase and phospholipase Cgamma2 mediate chemokine-controlled B cell migration and homing. Immunity. 2007;26(1):93–104 .https://doi.org/10.1016/j.immuni.2006.11.012
85
Chang
BY
,
Francesco
M
,
De Rooij
MF
,
Magadala
P
,
Steggerda
SM
,
Huang
MM
, et al.
Egress of CD19(+)CD5(+) cells into peripheral blood following treatment with the Bruton tyrosine kinase inhibitor ibrutinib in mantle cell lymphoma patients. Blood. 2013;122(14):2412–24 .https://doi.org/10.1182/blood-2013-02-482125
86
Okada
T
,
Ngo
VN
,
Ekland
EH
,
Förster
R
,
Lipp
M
,
Littman
DR
, et al.
Chemokine requirements for B cell entry to lymph nodes and Peyer’s patches. J Exp Med. 2002;196(1):65–75 .https://doi.org/10.1084/jem.20020201
87
Wong
S
,
Fulcher
D
. Chemokine receptor expression in B-cell lymphoproliferative disorders. Leuk Lymphoma. 2004;45(12):2491–6 .https://doi.org/10.1080/10428190410001723449
88
Rehm
A
,
Mensen
A
,
Schradi
K
,
Gerlach
K
,
Wittstock
S
,
Winter
S
, et al.
Cooperative function of CCR7 and lymphotoxin in the formation of a lymphoma-permissive niche within murine secondary lymphoid organs. Blood. 2011;118(4):1020–33 .https://doi.org/10.1182/blood-2010-11-321265
89
Somovilla-Crespo
B
,
Alfonso-Pérez
M
,
Cuesta-Mateos
C
,
Carballo-de Dios
C
,
Beltrán
AE
,
Terrón
F
, et al.
Anti-CCR7 therapy exerts a potent anti-tumor activity in a xenograft model of human mantle cell lymphoma. J Hematol Oncol. 2013;6(1):89 .https://doi.org/10.1186/1756-8722-6-89