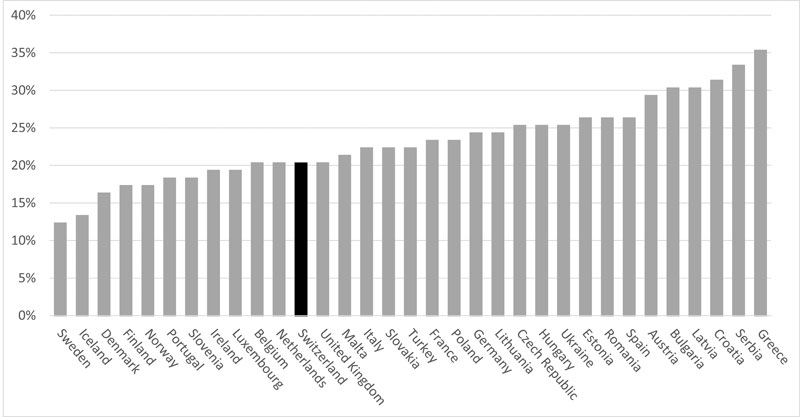
Figure 1 European countries ranked by adult daily smoking prevalence in 2013. Source: WHO Report on the Global Tobacco Epidemic, 2015 [10].
DOI: https://doi.org/10.4414/smw.2017.14437
Every year, more than 9000 persons die in Switzerland because of tobacco-related illnesses, which account for around 15% of all deaths in this country [1]. Furthermore, 300 000 people can be conservatively estimated to suffer from a serious smoking-related disease [2, 3]. (The US Surgeon General in his 2014 report [2] estimated that for one death attributed to smoking, there were 30 people suffering from a serious smoking-related illness; we applied this proportion to the number of deaths caused by tobacco smoking in Switzerland.) This is likely to be an underestimate. Indeed, the Swiss Lung League [3] estimates that 400 000 persons suffer from chronic obstructive pulmonary disease (COPD) alone, a disease which is mostly caused by smoking (80 to 90% of persons with COPD are smokers).) According to official statistics, smoking prevalence in Switzerland is among the lowest in Europe (about 25% [4–7], 28% is the average in Europe [8], 34.1% in France for age group 15–75 years [9]); adult daily smoking prevalence appears to be lower in Switzerland than in most European countries, including all its neighbouring countries [10] (fig. 1). Addiction Monitoring in Switzerland (AMIS), the consortium of organisations mandated by the Swiss Federal Office of Public Health (FOPH) to establish prevalence statistics, states on its website [11] that “Available data on smoking prevalence in the countries neighbouring Switzerland (Germany, France, Italy and Austria) suggest proportions of smokers relatively similar to the Swiss figures or significantly higher, particularly in France.” If smoking prevalence is taken as the indicator of success in tobacco control, Switzerland might appear to be doing as well as or better than its neighbours and better than most European countries. This observation was recently made by the Swiss Senate when rejecting a proposed tobacco product law: the senators considered current smoking prevention measures as effective and thus concluded there was no need to change them [12].
Figure 1 European countries ranked by adult daily smoking prevalence in 2013. Source: WHO Report on the Global Tobacco Epidemic, 2015 [10].
Tobacco is less regulated in Switzerland than in most other European countries. With respect to three key tobacco control measures – taxation, smoke-free policy in public places and advertising bans (corresponding respectively to articles 6, 8 and 13 of the World Health Organization Framework Convention on Tobacco Control) – Switzerland trails behind most of the other countries included in the Tobacco Control Scale Europe 2013 [13]: it is last in terms of advertising bans and next to last in terms of affordability of tobacco products; its smoking ban in public and work places is also among the weakest (figs 2–4 ).
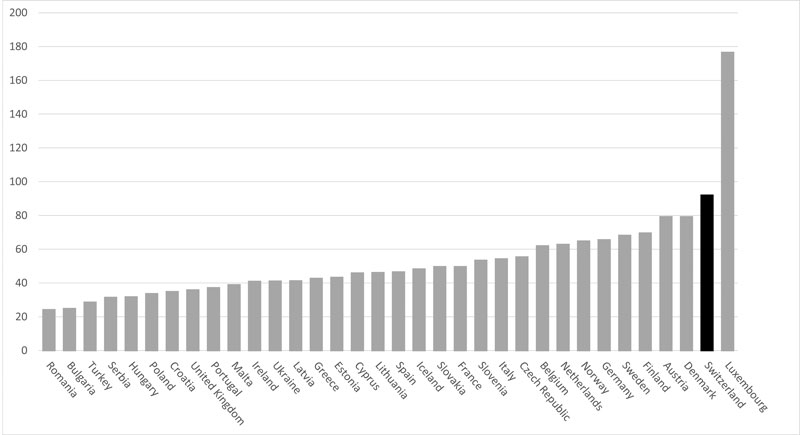
Figure 2 European countries ranked by index of affordability of tobacco products (vertical axis: number of 20-packs that can be purchased with 1% of GDP per capita). Source: WHO Report on the Global Tobacco Epidemic, 2015 [10].
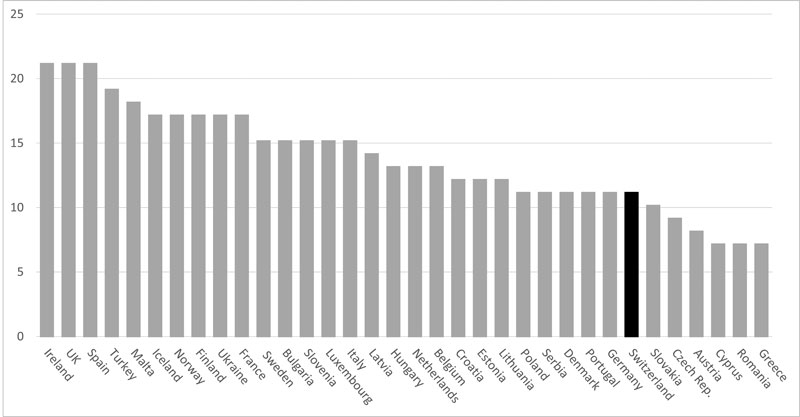
Figure 3 European countries ranked by TCS score for smoke-free policies. Source: Tobacco Control Scale in Europe 2013 [13].
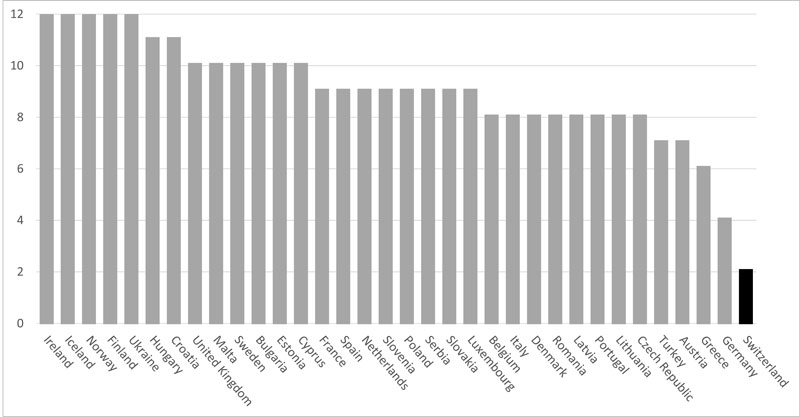
Figure 4 European countries ranked by TCS score for advertising bans. Source: Tobacco Control Scale in Europe 2013 [13].
The present study was motivated by a crude comparison we had made between reported results of FOPH population-based surveys and aggregate measures of national tobacco consumption, which exhibited a substantial discrepancy, suggesting that official statistics might perhaps underestimate the actual prevalence of smoking in Switzerland. Could it be that legislators and other public health professional base their tobacco control policy decisions on smoking prevalence estimates that are more reassuring than may be justified?
It has been observed in other studies [14–16] that in surveys smokers tend to underreport (declare smoking fewer daily cigarettes than they actually do) or misreport (declaring themselves as nonsmokers when they are irregular users or as non-daily users when they are regular smokers) their smoking status. This is seen notably when total consumption estimated through survey data (hereafter called reported consumption, following Kenneth Warner’s terminology [14]) is compared with consumption figures estimated from national aggregate data (hereafter called “actual consumption”, again Warner’s terminology [14]): shortfalls of up to 33% have been observed, which means that reported consumption accounted only for two thirds of actual consumption [14, 15].
Our aim was to perform a detailed comparison between reported consumption and actual consumption in Switzerland in view of assessing the level of underreporting. Based on our finding, we will put forward possible reasons for this phenomenon.
To evaluate cigarette consumption in a population, two methods are generally available: the first method is to obtain data by surveying a representative sample of the population, asking questions about individual smoking behaviour (hereafter “survey data”) – this is the usual way of calculating smoking prevalence officially reported by governments; the second approach uses aggregate data about volumes of sales of cigarettes, usually obtained by governmental administrations in the context of collecting excise taxes (hereafter “aggregate data”) [14–17]. Survey data offer the advantage of identifying group characteristics and factors linked to smoking, and provide more information about the consumer, but tend to suffer from reporting issues. Aggregate data (presented as total and/or per capita cigarette consumption) generally produce objective quantitative information about overall volumes. They are not affected by changing social attitudes towards smoking but lack information about consumers.
To be meaningful from a public health perspective, actual consumption of cigarettes by the resident population needs to be assessed. To estimate this, a starting point is legal domestic sales data (number of duty-paid cigarettes sold in the country). We obtained these data from the Federal Customs Administration [18], which provided them with a disclaimer that “the sales figures do not correspond to the quantities consumed by the resident population. Indeed, the quantities of cigarettes sold strongly depend on the evolution of purchases by cross-border commuters and foreign tourists, on contraband, of imports done in the context of touristic traffic or Internet sales, on transition from manufactured cigarettes to roll-you-own tobacco, and on provisions made by consumers when price increases are announced.” Thus, to obtain quantities consumed by the resident population, two adjustments are needed:
We will elaborate below how we applied these two adjustments to obtain an estimate of the number of cigarettes consumed by the Swiss resident population. All our calculations are yearly and relate to years 2012-2015. We have all the data needed to perform our analysis for years 2013-2015 and have also included year 2012 by extrapolating some data, as will be shown below, to include the year covered by the most recent Swiss Health Survey (SHS) [19].
In the factsheet [20] published to present its proposal for a new tobacco product law, the Federal Office of Public health compared tobacco regulations on advertising, promotion and sponsorship of Switzerland with Germany and France. France is also pointed out as a country in which the proportions of smokers is “significantly higher” than in Switzerland [11].
Motivated by this reference to France, we decided to compare the Swiss results with corresponding French results. Fortunately, France is a neighbouring country for which we could obtain all the data for a recent year (2014) necessary to make a full comparison. We could not get similarly complete data from other neighbouring countries.
In addition to manufactured cigarettes, our aggregate data also include roll-your-own (RYO) cigarettes. National sales data on RYO are usually expressed in units of weight (tonnes). We have converted these measures (for both Switzerland and France) into number of cigarettes, by assuming that one RYO cigarette contains 0.75 g of fine-cut tobacco, which corresponds to the median weight in Europe [21].
Since 2011, the Swiss Federal Office of Public Health (FOPH) has been mandating a consortium of organisations, operating under the label Addiction Monitoring in Switzerland (AMIS), to carry out on its behalf representative monitoring of addiction and use of psychoactive substances, including tobacco and alcohol. Each year, around 10 000 persons are interviewed through a telephone survey using predominantly home phones (with a mobile phone sample limited to 1000 persons). In the analysis below, we use the estimates contained in the AMIS report for the years 2012 to 2015 [4–7] for smoking prevalence and smoking intensity (number of daily cigarettes smoked on average by a smoker) for daily and occasional (non-daily) smokers, as well as for all smokers confounded. Using these estimates, we calculated reported consumption:
Reported consumption (bn) = pop15+ * prevalence * dailycig * ndays / 109, with ndays = 366 for 2012 and 365 for the other years
In addition, we did the same calculation for year 2012 using prevalence data obtained from the Swiss Health Survey 2012 [19] conducted by the Federal Office of Statistics every 5 years.
For France, the data for reported prevalence are taken from the Baromètre santé 2014 survey [22]. However, as Baromètre santé 2014 only covers age group 15-75, we have extrapolated data from Baromètre santé 2010 [23] for the age group 76+ years.
We obtained aggregate data on legal domestic sales for 2012 to 2015 from the Federal Customs Administration [18], which provided us with precise figures of the number of cigarettes and the quantity of fine cut tobacco (expressed in tons) sold on the domestic market for each year of the period.
For France, aggregate figures for legal domestic sales come from the data compiled by the Observatoire français des drogues et des toxicomanies (OFDT) [24]. OFDT obtained aggregate data from the French customs administration in charge of tobacco taxation, a source that is very similar to the one from which we obtained corresponding Swiss data.
For adjustment 1, we used the estimates of inflows/outflows (for both Switzerland and France) from the KPMG Project Sun reports [25, 26]. KPMG is one of the Big Four accountancy firms offering audit, assurance, tax, consulting and advisory services. In their Project Sun contracted by the four largest multinational tobacco firms, they studied and reported “on the estimated size and composition of the total cigarette market (including counterfeit and contraband products) […] for each of the 28 EU Member States, Norway and Switzerland.” Their reports present data on total consumption of manufactured cigarettes for each country included in the study. The amount of legal domestic sales was provided by the manufacturers themselves. To reach the total amount of consumed manufactured cigarettes, outflows (cigarette bought in a country but consumed abroad) and inflows (both legal and illegal) were estimated by KPMG using a method they developed called the “empty pack survey”. Their methodology has been the subject of criticism, notably because it “tends to overestimate illicit cigarette levels particularly where cross-border shopping is frequent (Austria, Finland, France)” [27]. However, these overestimates will not significantly affect our results and, if so, only conservatively (towards reducing reporting discrepancy).
It should be noted that KPMG’s estimates of inflows and outflows concern only manufactured cigarettes and do not relate to RYO. We assume that the inflows/outflows balance for RYO, which we have no means of estimating, is in any case negligible in our context and thus it is acceptable to ignore it in the calculations. This decision is conservative for our purpose, since because the inflows/outflows balance is positive for manufactured cigarettes, it is also likely to be positive for RYO, which would result in a larger total consumption in Switzerland.
Finally, KPMG’s data do not cover year 2012. To extend our analysis to the year of the Swiss Health Survey, we have extrapolated KPMG 2013–2015 inflows/outflows results to 2012 by using their average. It is believed that the small inaccuracy thus introduced is unlikely to substantially alter our conclusions.
The tool we have at our disposal for adjustment 2 is the balance of tourism published in Switzerland by the Federal Office of Statistics [28] (and in France by the Institut national de la statistique et des études économiques: INSEE [29]). The balance of tourism is the difference between the money nonresidents spend in the country when visiting it and the money spent by residents when they visit other countries. Our assumption is that, at equal budget, Swiss residents traveling abroad will buy the same number of cigarettes outside the country as nonresidents visiting Switzerland, so that the net resulting consumption will be zero if the balance of tourism is zero. This is in fact conservative for our purpose. Indeed, using data from the 2014 results of the KPMG report [25], yearly per capita consumption of manufactured cigarettes is higher among Swiss people (1279) than the European average (1070), and the price of cigarettes is higher in Switzerland than in most European countries. Thus, Swiss smokers travelling abroad will be more likely to buy cigarettes in the destination country (or in duty-free shops), than tourists visiting Switzerland to buy domestic cigarettes. We thus assumed (conservatively) that only the balance of tourism needs to be considered to apply adjustment 2. We assumed (again conservatively) that a third of tourists smoke and spend on average 5% of their budget on cigarettes.
The results leading to the calculation of actual consumption of cigarettes by Swiss residents during the period 2012 to 2015 are shown in table 1.
Table 1 Total cigarette consumption in Switzerland for the years 2012 to 2015.
| Category | 2012 | 2013 | 2014 | 2015 |
|---|---|---|---|---|
| Legal domestic sales* | 11.43 | 10.81 | 10.25 | 9.91 |
| Outflows† | ˗0.37 | ˗0.35 | ˗0.47 | ˗0.28 |
| Inflows† | 1.20 | 1.32 | 0.92 | 1.36 |
| Net inflows | 0.83 | 0.97 | 0.45 | 1.08 |
| Total manufactured cigarettes | 12.26 | 11.78 | 10.70 | 10.99 |
| Roll-your-own cigarettes* | 0.77 | 0.76 | 0.91 | 0.91 |
| Total cigarettes consumed in Switzerland | 13.03 | 12.53 | 11.60 | 11.91 |
| Tourism balance adjustment‡ | -0.04 | -0.03 | -0.04 | -0.01 |
| Total cigarettes consumed by Swiss residents | 12.99 | 12.50 | 11.56 | 11.90 |
Sources: * Federal Customs Administration [18] † KPMG Sun Report 2014 and 2015 [25, 26] ‡ calculated based on Federal Office of Statistics data [28] – see text
Domestic legal sales data obtained from the Swiss Federal Customs Administration (FCA) indicates that the sales of manufactured cigarettes steadily decreased over the period, ranging from 11.43 billion (bn: 109) in 2012 to 9.91 bn in 2015 [18].
The KPMG reports [25, 26] provide data for the years 2013 to 2015 indicating that the number of manufactured cigarettes that were brought into the country, either legally or illegally via contraband or as counterfeit cigarettes (inflows) ranged from 0.92 bn (in 2014) to 1.36 bn (in 2015), while the number of manufactured cigarettes sold in Switzerland which were consumed outside the country (outflows) ranged from 0.28 bn (in 2015) to 0.47 bn (2014). As explained above, inflows/outflows data for 2012 were obtained by extrapolation. The inflows/outflows balance was positive throughout the period 2013 to 2015, adding from 0.45 bn units (in 2014) to 1.08 bn units (in 2015) to legal domestic sales, while remaining below 10% of the total number of manufactured cigarettes consumed in Switzerland, which ranged from 12.26 units in 2012 to 10.70 units in 2014. It should be noted that the decrease in legal domestic sales of cigarettes observed in 2015 was partly compensated by an increase of legal nondomestic consumption (from 0.68 bn in 2014 to 1.07 bn in 2015 – not shown in table 1) [26]. KPMG observes that duty-free inflows account for a quarter of the cigarettes legally entering the country, a proportion higher than other EU countries, notably since 2011, when travellers entering Switzerland were entitled to a duty-free allowance. This phenomenon was accentuated in 2015 with the strong appreciation of the Swiss franc at the beginning of the year, which also reduced outflows [26].
Conversion of the amounts of fine-cut tobacco sold in the period 2012 to 2015 [18] adds between 0.76 bn cigarettes (in 2013) to 0.91 bn cigarettes (in 2014 and 2015). Consequently, the total number of cigarettes (manufactured and RYO) consumed in Switzerland was 13.03 bn units in 2012, decreased to reach 11.60 bn units in 2014, and slightly increased again in 2015 to 11.91 bn units.
Switzerland’s balance of tourism was positive throughout all four years (maximum CHF 854 million in 2014, minimum CHF 323 million in 2015). The related excess of cigarettes bought on the domestic market by visitors led to a small adjustment ranging between 0.01 bn units (2015) and 0.04 bn units (2014), which were subtracted as these cigarettes were not consumed by Swiss residents.
The final estimate of the number of cigarettes smoked by the Swiss resident population was above 11.5 bn units across all four years, ranging from 11.56 bn units in 2014 to 12.99 bn units in 2012 (see table 1).
The AMIS results for the period 2012 to 2015 (table 2) show overall prevalence figures that have remained relatively stable over the period, ranging from of 24.9% (2014) to 25.9% (2012). The average number of daily cigarettes per smoker has slightly decreased, from 10.3 in 2012 and 10.5 in 2013, down to 9.9 in 2014 and 2015.
Table 2 Swiss Health Survey (SHS) and Addiction Monitoring in Switzerland (AMIS) reported cigarette consumption compared with estimated actual consumption for the years 2012 to 2014.
| SHS | AMIS | ||||
|---|---|---|---|---|---|
| 2012 | 2012 | 2013 | 2014 | 2015 | |
| Reported prevalence* | 28.2% | 25.9% | 25.0% | 24.9% | 25.0% |
| Average daily cigarettes per smoker† | 10.1 | 10.3 | 10.5 | 9.9 | 9.9 |
| Population aged 15+ years‡ | 6 838 457 | 6 838 457 | 6 927 354 | 7 012 685 | 7 090 334 |
| Reported consumption (bn cigarettes)§ | 7.14 | 6.65 | 6.61 | 6.31 | 6.41 |
| Estimated actual consumption (bn cigarettes)¶ | 12.99 | 12.99 | 12.50 | 11.56 | 11.90 |
| Discrepancy between reported consumption and actual consumption (bn cigarettes)§ | 5.85 | 6.34 | 5.90 | 5.26 | 5.48 |
| Relative discrepancy of reported consumption§ | 45.0% | 48.8% | 47.2% | 45.5% | 46.1% |
| Actual number of cigarettes per year per capita§ | 1900 | 1900 | 1805 | 1649 | 1678 |
bn = billion (109) Sources: * SHS 2012 [19] and AMIS 2012, 2013, 2014 and 2015 [4–7] † Calculated from SHS and AMIS data (same source as *) ‡ Federal Office of Statistics [30] § Calculated – see text ¶ See table 1
When applied to the resident population aged 15+ years [30], these figures translate into reported consumption which, again, is rather stable over the period, ranging from a minimum of 6.31 bn units (in 2014) to a maximum of 6.65 bn units (in 2012). For all years, the shortfall between reported consumption and estimated actual consumption is consistently high, exceeding 5 bn cigarettes. Over the entire period, reported consumption only accounts for between 50 and 55% of estimated actual consumption.
For the year 2012, we also extrapolated total consumption using the prevalence estimate taken from the Swiss Health Survey 2012 [19], which was slightly higher than its AMIS counterpart (28.2 vs 25.9%), whereas the average of daily cigarettes per smoker was slightly lower (10.1 vs 10.3). Although a bit smaller, the discrepancy between SHS reported consumption and estimated actual consumption remains large (5.85 bn cigarettes): SHS reported consumption accounts for only 55.0% of estimated actual consumption.
To compare Swiss results with corresponding French results (Table 3), we took data from Baromètre santé 2014 [22], adjusted with data from Baromètre santé 2010 [23] for ages classes 76+ years to make them comparable with AMIS results. In 2014, the French reported smoking prevalence was 31.0%. This prevalence, together with an average of 11.3 cigarettes consumed daily, applied to the French metropolitan population on 1 January 2015 [31], result in a reported consumption of 66.38 bn cigarettes for year 2014. Legal domestic sales came from OFDT [24] and inflows/outflows were obtained from KPMG’s publication for the year 2014 [25], totalling 60.45 bn units for manufactured cigarettes. The number of RYO cigarettes (11.26 bn) was calculated from the amount of fine-cut tobacco sold in 2014 [24], again assuming 0.75 g per cigarette, resulting in a total of 71.72 bn cigarettes consumed in metropolitan France in 2014, excluding Corsica. Applying a correction factor proportional to the population for the omission of Corsica in OFDT and KPMG data, the total becomes 72.08 bn cigarettes. As a last step, we applied adjustment 2 based on the balance of tourism. The French balance of tourism was approximately a positive EUR 10 bn in 2014 [29]. The excess of cigarettes consumed by tourists, which was not compensated by cigarettes consumed by French residents when visiting other countries, was thus estimated to be 0.49 bn units. Subtracting this last number left 71.59 bn cigarettes consumed by the French resident population in 2014 (see table 1).
Table 3 Comparison of Switzerland and France with respect to relevant cigarette smoking variables for the year 2014.
| Switzerland | France | |
|---|---|---|
| Reported prevalence* | 24.9% | 31.0% |
| Average daily cigarettes per smoker* | 9.9 | 11.3 |
| Population aged 15+ years† | 7 012 685 | 52 197 423 |
| Reported consumption (bn cigarettes)‡ | 6.31 | 66.38 |
| Estimated actual consumption (bn cigarettes)§ | 11.57 | 71.59 |
| Relative discrepancy of reported consumption compared to actual consumption‡ | 45.5% | 7.3% |
| Actual number of cigarettes / year per capita‡ | 1649 | 1371 |
bn = billion (109) Sources: For Switzerland, see table 2. For France: * Calculated – see text - from Baromètre santé 2014 [22] and Baromètre santé 2010 [23] † Institut national de la statistique et des études économiques (INSEE) [31] ‡ Calculated – see text § Calculated based on data from Observatoire français des drogues et des toxicomanies (OFDT) [24], KPMG Sun Project report 2014 [25] and INSEE [29] – see text
In 2014, reported smoking prevalence was substantially lower in Switzerland than in France (24.9% vs 31.0%) and Swiss smokers reported an average consumption of fewer daily cigarettes than their French counterparts (9.9 vs 11.3). However, per capita consumption of cigarettes was 20% higher in Switzerland than in France (1649 vs 1371). (Per capita consumption = average of consumed cigarettes per year per resident aged 15+, regardless of smoking status.) One element of an answer to this apparent contradiction may be provided by looking at the discrepancy between reported consumption and actual consumption, which was much higher for Switzerland than for France (45.5% vs 7.3%).
The discrepancy between reported consumption and our estimate of actual consumption appears to be a phenomenon that has remained large and relatively constant over the period under study, ranging between 45 and 50% in the years 2012 to 2015. Although this paper has concentrated on the AMIS survey, the SHS survey does not appear to be immune from the phenomenon, although it is slightly less pronounced (SHS reporting discrepancy: 45.1%; AMIS reporting discrepancy in 2012: 48.8%).
The reporting discrepancy might be the result of one or several of the following anomalies:
The way we derived total consumption from the AMIS estimates of prevalence and smoking intensity was rather straightforward and can be easily verified. As a matter of verification, the amount we described for 2014 (6.31 bn cigarettes) for reported consumption is just slightly larger, that is, on the conservative side, than the reported consumption calculated by the Federal Office of Public Health of 6.137 bn cigarettes [32].
The reported consumption refers only to age group 15+ years and does not take into account consumption by children below the age of 15. Although smoking in children aged less than 15 years is a highly preoccupying problem from a public health point of view, this part of total cigarette consumption in the general population is very small. Assuming plausibly that 5% of the children aged 12–14 smoke on average 5 cigarettes per day, their total consumption would amount to 0.02 bn cigarettes. (Taking 2012 as reference year (year with maximum 12–14 population of the study period), (249 945 persons aged 12–14)*0.05*5*366/109 = 0.023 bn cigarettes / year.) If this number is added to the reported consumption estimated by FOPH, the total is still under the 6.31 bn cigarettes shown in table 2 for 2014. It should be noted also that this issue does not affect the comparison with France, since French data also relate to age group 15+.
Two other issues also arise in the calculation of reported consumption. People who declared themselves as smokers may have subsequently quit smoking during the same year, therefore consuming cigarettes for fewer than 365 days, whereas our calculation assumes that all smokers keep smoking the average number of daily cigarettes for the whole year, thus overestimating actual consumption. On the other hand, especially among young respondents, some nonsmokers at the time of the interview may have started smoking later in the year, thus consuming cigarettes that are not taken into account in our measure of reported consumption. However, consistently with previous findings by Hatziandreu et al. [15], we can assume that these two effects are small and, as the population of smokers has remained relatively stable in 2014 compared with previous years, that they cancel each other out.
We therefore reject explanation 1.
The possibility that actual consumption was lower than our estimates cannot be excluded. Data that could be questioned are the inflows and outflows taken from the KPMG reports [25, 26], which indicate a positive balance. However, this balance is relatively small (always less than 10% of the domestic consumption of manufactured cigarettes) and, even assuming the unlikely possibility that it is zero, this would not remove the discrepancy between reported consumption and actual consumption: there would still remain a discrepancy of at least 4 bn cigarettes for each year of the period.
Cigarettes bought in Switzerland and on which excise taxes were fully levied were very unlikely to have been massively exported to other countries, as they were similarly or more expensive than cigarettes in neighbouring countries at the time, as is shown in table 4.
Table 4 Weighted average price for a pack of 20 cigarettes in Switzerland and neighbouring countries at end of 2014 and 2015.
| Average price of a pack of 20 cigarettes (euros) | |||||
|---|---|---|---|---|---|
| Switzerland | France | Germany | Austria | Italy | |
| End of 2014 | 6.64 | 6.74 | 5.13 | 4.33 | 4.52 |
| End of 2015 | 7.12 | 6.75 | 5.34 | 4.48 | 4.66 |
| Source: KPMG Sun Project reports [25, 26]. | |||||
The KPMG reports [25, 26] found that inflows of legally imported cigarettes originate mostly from Germany and Italy, whereas the legal flow from France (between 0.04 bn and 0.12 bn cigarettes) is reflected by the high volumes of tourists and commuters consuming French-origin packs when in Switzerland. This is something we have taken into account with our balance of tourism adjustment.
Illegal inflows (mostly contraband) are estimated by the KPMG reports [25, 26] to be 3.7%, 2.2% and 2.6% of the total consumption of manufactured cigarettes in 2013, 2014 and 2015, respectively, whereas the Federal Customs Administration estimates that it is “well below 5%” [33]. Both agree that this proportion is small. Even allowing for possible inaccuracies, the contribution of inflows and outflows, and their balance, would remain within a few percent of total consumption and therefore cannot explain the discrepancy.
Finally, one possibility could consist in smokers not consuming all the cigarettes they buy and throwing away some of them. Although we do not have scientific data on this subject, we find it unlikely that smokers would throw away cigarettes in any significant way, given their price. If the phenomenon exists, it must be very rare: KPMG has called its methodology “empty pack survey” [25, 26] probably because the cigarette packs they collect in the streets are indeed empty. We therefore assume such a phenomenon is not of sufficient scale to alter our results in any significant way.
We therefore reject explanation 2.
The AMIS survey results for 2014 indicate that smoking intensity was lower in Switzerland than in France (see table 3): on average, Swiss smokers declared consuming 9.9 cigarettes per day, and their French counterparts reported 11.3 cigarettes daily. The proportion of nondaily consumers among smokers was much larger in Switzerland (31%) than in France (17%).
It is known that smokers tend to underreport the quantity of cigarettes they smoke, for instance by 32% as described in a study from the USA [11]. While this phenomenon could be involved here, it is still intriguing why it would particularly affect Swiss survey respondents, while the French Baromètre santé 2014 survey seems to be almost immune to such underreporting. Assuming that French smokers only underreported the daily number of cigarettes they smoke, this would be at most by 7.3%: the true number of cigarettes they smoked on average per day in 2014 would not exceed 12.1 cigarettes. As Europeans, Swiss and French smokers can be presumed to be culturally closer to each other than they are to smokers in the USA, one could thus assume that underreporting of smoking intensity by Swiss residents would be closer to that of French residents than in the USA. Thus, the Swiss underreporting of daily cigarettes is plausibly between 7.3% (like France) and the upper limit of 32% (like the USA).
To assess the sensitivity to smoking intensity, we performed the calculations comparing AMIS prevalence and smoking intensity values with two scenarios (shown in table 5), with 2014 results as reference, to make it possible to compare with corresponding French results:
Table 5 Two scenarios of smoking intensity in Switzerland.
Scenario 1: Daily cigarettes same as maximum for France after correction for underreporting; Scenario 2: Prevalence of smoking same as France. The fixed variable for each scenario is shown in bold type.
| AMIS | Scenario 1 | Scenario 2 | |
|---|---|---|---|
| Reported prevalence (AMIS 2014) | 24.9% | 24.9% | 24.9% |
| Daily cigarettes | 9.9 | 12.1 | 14.6 |
| (Implied actual underreporting in scenario) | – | 18.4% | 32.2% |
| Reported consumption (bn cigarettes) |
6.31 | 7.74 | 9.31 |
| Actual consumption in 2014 (bn cigarettes) |
11.57 | 11.57 | 11.57 |
| Reporting discrepancy: gap between reported and actual consumption as a percentage of actual consumption | 45.5% | 33.1% | 19.6% |
| Implied prevalence | 45.7% | 37.2% | 31.0% |
| Prevalence discrepancy: gap between reported and implied prevalence | 20.8% | 12.3% | 6.1% |
AMIS = Addiction Monitoring in Switzerland; bn = billion (109)
The two scenarios assume that Swiss smokers consume as many or more cigarettes daily than their French counterparts, an assumption that is not highly plausible and would need to be verified. For instance, in 2014, the level of unemployment was three times higher in France than in Switzerland [34, 35]. People with a low socioeconomic status or who are unemployed tend to smoke more than the rest of the population, both in terms of prevalence and number of daily cigarettes [36–38]. With more than 10% of its active population without a job [39], France had in 2014 a large pool of heavy smokers with no similar counterpart in Switzerland [40].
We further observe that in these two scenarios, the prevalence required to consume 11.56 bn cigarettes is above 31%, which is at least 6% higher than AMIS reported prevalence.
Finally, we have calculated that if the discrepancy came only from underreporting, this would imply that daily smokers in Switzerland smoke on average 25 cigarettes per day, 10 more than their French counterparts under the same assumption. We see no valid explanation for such a huge difference.
We therefore conclude that explanation 3 can be accepted, but is not sufficient to fully explain the discrepancy even when adjusted for underreporting of smoking intensity.
Having been unable to fully elicit the discrepancy with the previous explanations, we are left with the explanation that actual prevalence in Switzerland is higher than what is being reported. What could be the cause of such differences? We see two possibilities:
We therefore conclude that explanations 3 and 4 together provide the plausible answer. The large discrepancy between reported consumption and actual consumption is most likely the combined effect of underreporting the intensity of smoking (number of daily cigarettes), misreporting the smoking status and sampling bias.
Our analysis therefore suggests that Swiss reported statistics underestimate true prevalence. Comparisons with France further suggests that the level of underestimation could be at least by 6 percentage points, i.e., true prevalence might be 31% or more.
Misreporting prevalence and underreporting smoking intensity in surveys have been documented in the literature, but the level of discrepancy is generally smaller than the discrepancy observed in the Swiss surveys on smoking, where reported consumption from AMIS and SHS survey results explain only about 55% of actual consumption of cigarettes.
Swiss data on tobacco smoking offer an illustration of Kenneth Warner’s observation that “analyses of the surveys not only understate the level of smoking at any point in time, they also present the public with an erroneous view of behavioural change, mixing under that label true changes in smoking behaviour with increases in underreporting” [14]. For instance, a decrease of self-reported smoking prevalence would not necessarily mean a corresponding decrease in actual smoking prevalence, but could reflect a behavioural change of respondents who become more reluctant to declare themselves as smokers and who are more prone to claim that they smoke fewer cigarettes than they actually do [15]. Thus, prevalence results may not be comparable across years and their public health pertinence may thus be reduced.
Our finding suggests that current official data about smoking prevalence in Switzerland may underestimate actual prevalence by at least 6 percentage points. Identifying the specific causes for the reporting discrepancy described in the present paper could help in finding ways to improve official data quality through adaptation of survey methodology. Swiss public health and political decision makers need reliable indicators of smoking prevalence, notably if Switzerland wants to monitor its progress towards achieving the voluntary global target of a 30% relative reduction in prevalence of current tobacco use in persons aged 15 or older by year 2025, a key target of the WHO Global Action Plan for the Prevention and Control of Non-Communicable Diseases 2013-2020 [43], of which Switzerland is a signatory.
No financial support and no other potential conflict of interest relevant to this article was reported.
1Bundesamt für Statistik (BFS). Tabakbedingte Todesfälle in der Schweiz, 1995 bis 2012. Neuchâtel, 2015. Available from: https://www.bfs.admin.ch/bfsstatic/dam/assets/350100/master
2U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014.
3Schweiz L. COPD Früh erkennen - wirksam behandeln. Lungenliga Schweiz, 2016. Available from: http://www.lungenliga.ch/uploads/tx_pubshop/COPD_Broschuere.pdf
4Schweiz S. Konsum von Alkohol, Tabak und illegaler Drogen in der Schweiz im Jahr 2012. Bundesamt für Gesundheit, Bern. Available from: http://www.suchtmonitoring.ch/de/page/9-7.html
5Schweiz S. Konsum von Alkohol, Tabak und illegaler Drogen in der Schweiz im Jahr 2013. Bundesamt für Gesundheit, Bern. Available from: http://www.suchtmonitoring.ch/de/page/9-7.html
6Schweiz S. Konsum von Alkohol, Tabak und illegaler Drogen in der Schweiz im Jahr 2014. Bundesamt für Gesundheit, Bern. Available from: http://www.suchtmonitoring.ch/de/page/9-7.html
7Schweiz S. Konsum von Alkohol, Tabak und illegaler Drogen in der Schweiz im Jahr 2015. Bundesamt für Gesundheit, Bern. Available from: http://www.suchtmonitoring.ch/de/page/9-7.html
8World Health Organization, Regional Office for Europe (WHO/EURO). Tobacco – Data and Statistics. Available from: http://www.euro.who.int/en/health-topics/disease-prevention/tobacco/data-and-statistics
9Guignard R, Beck F, Richard JB, Lermenier A, Wilquin JL, Nguyen-Thanh V. La consommation de tabac en France en 2014: caractéristiques et évolutions récentes. Institut national de prévention et d’éducation pour la santé (INPES). Évolutions 31. Janvier 2015. Available from: http://inpes.santepubliquefrance.fr/CFESBases/catalogue/detaildoc.asp?numfiche=1623
10WHO report on the global tobacco epidemic, 2015: raising taxes on tobacco. World health Organization. Geneva 2015. Available from: http://www.who.int/tobacco/global_report/2015/report/en/
11Schweiz S. Tabak. Überblick. Available from: http://www.suchtmonitoring.ch/de/1.html
12Mariani D. Reduziert ein Werbeverbot die Zahl der Raucher. Swissinfo.ch. 4 July 2016. Available from: http://www.swissinfo.ch/ger/faktencheck_reduziert-ein-werbeverbot-diezahl-der-raucher-/42260898
13Joossens L, Raw M. The Tobacco Control Scale 2013 in Europe. A report of the Association of European Cancer Leagues. Brussels, 2014. Available from: http://www.europeancancerleagues.org/images/TobaccoControl/TCS_2013_in_Europe_13-03-14_final_1.pdf
14 Warner KE . Possible Increases in the Underreporting of Cigarette Consumption. J Am Stat Assoc. 1978;73(362):314–8. Available at: https://www.industrydocumentslibrary.ucsf.edu/tobacco/docs/#id=qgmk0088. https://doi.org/10.1080/01621459.1978.10481575
15 Hatziandreu EJ , Pierce JP , Fiore MC , Grise V , Novotny TE , Davis RM . The reliability of self-reported cigarette consumption in the United States. Am J Public Health. 1989;79(8):1020–3. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1349899/. https://doi.org/10.2105/AJPH.79.8.1020
16 Farrelly MC , Nonnemaker JM , Watson KA . The consequences of high cigarette excise taxes for low-income smokers. PLoS One. 2012;7(9):e43838. Available at: http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0043838#pone.0043838-Warner2. https://doi.org/10.1371/journal.pone.0043838
17International Agency for Research on Cancer. IARC Handbook of Cancer Prevention Volume 12. WHO/IARC. 2008. Available from: http://www.iarc.fr/en/publications/pdfs-online/prev/handbook12/
18Zollverwaltung E. Personal communication, emails of 16 August 2016 and 18 November 2016
19Bundesamt für Statistik (BFS). Bundesamt für Sport (BASPO). Schweizerische Gesundheitsbefragung 2012: "Bewegung und Gesundheit", Neuchâtel, October 2014. Available from https://www.bfs.admin.ch/bfsstatic/dam/assets/350839/master
20Bundesamt für Gesundheit (BAG). Was sich mit dem neuen Tabakproduktegesetz ändert. Faktenblatt. 11 November 2015. Available from: https://www.bag.admin.ch/dam/bag/de/dokumente/npp/tabak/tabpg/fb-tabpg-alle.pdf.download.pdf/faktenblatt-tabpg-alle.pdf
21 Gallus S , Lugo A , Ghislandi S , La Vecchia C , Gilmore AB . Roll-your-own cigarettes in Europe: use, weight and implications for fiscal policies. Eur J Cancer Prev. 2014;23(3):186–92. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4127802/. https://doi.org/10.1097/CEJ.0000000000000010
22Guignard R, Beck F, Richard JB, Lermenier A, Wilquin J-L, Nguyen-Thanh V. La consommation de tabac en France en 2014: caractéristiques et évolutions récentes. Institut national de prévention et d’éducation pour la santé (INPES). Évolutions 31. Janvier 2015. Available from: http://inpes.santepubliquefrance.fr/CFESBases/catalogue/detaildoc.asp?numfiche=1623
23Guignard R, Beck F, Richard JB, Peretti-Watel P. Le tabagisme en France: analyse de l’enquête Baromètre santé 2010. Institut national de prévention et d’éducation pour la santé (INPES), coll. Baromètres santé, 2013. Available from: http://inpes.santepubliquefrance.fr/CFESBases/catalogue/detaildoc.asp?numfiche=1513
24Observatoire français des drogues et des toxicomanies (OFDT). Tableau de bord tabac, séries longues. Available from http://www.ofdt.fr/statistiques-et-infographie/tableau-de-bord-tabac/
25KPMG. Project Sun. A study of the illicit cigarette market in the European Union, Norway and Switzerland, 2014 Results. Available from: https://home.kpmg.com/uk/en/home/insights/2015/05/project-sun-a-study-of-the-illicit-cigarette-market.html
26KPMG. Project Sun. A study of the illicit cigarette market in the European Union, Norway and Switzerland, 2015 Results. Available from: https://home.kpmg.com/uk/en/home/insights/2016/05/project-sun.html
27Gilmore AB, Rowell A, Gallus S, Lugo A, Joossens L, Sims M. Towards a greater understanding of the illicit tobacco trade in Europe: a review of the PMI funded ‘Project Star’ report. Tob Control. 2014;23(e1):e51–61 Published Online: 11 December 2013 doi:https://doi.org/10.1136/tobaccocontrol-2013-051240. Available from: http://tobaccocontrol.bmj.com/content/early/2013/12/11/tobaccocontrol-2013-051240
28Bundesamt für Statistik (BFS). Monetäre Aspekte – Daten, Indikatoren. Fremdenverkehrsbilanz. Available from: https://www.bfs.admin.ch/bfs/de/home/statistiken/tourismus/monetaere-aspekte/fremdenverkehrsbilanz.assetdetail.253019.html
29Institut national de la statistique et des études économiques (INSEE). Balance commerciale. Available from: http://www.insee.fr/fr/themes/document.asp?reg_id=0&ref_id=T15F142
30Bundesamt für Statistik (BFS). Ständige Wohnbevölkerung nach Alter, Kanton, Bezirk und Gemeinde 2010-2015. Available from: https://www.bfs.admin.ch/bfs/de/home/statistiken/bevoelkerung/stand-entwicklung/raeumliche-verteilung.assetdetail.290789.html
31Institut national de la statistique et des études économiques (INSEE). Pyramide des âges au 1er janvier 2015. France métropolitaine. Available from http://www.insee.fr/fr/ppp/bases-de-donnees/donnees-detaillees/bilan-demo/fichiers-xls/pyramide-des-ages-2015.xls
32Bundesamt für Gesundheit. Personal communication, email of 20 November 2015
33Die Bundesversammlung — Das Schweizer Parlament. Bekämpfung von Schmuggel und Fälschungen. Tabakproduktegesetz als Basis. Interpellation 14.3062 by Verena Diener Lenz. Stellungnahme des Bundesrates vom 21.05.2014. Available from: https://www.parlament.ch/de/ratsbetrieb/suche-curia-vista/geschaeft?AffairId=20143062
34Staatssekretariat für Wirtschaft SECO. Arbeitsmarkt und Arbeitslosenversicherung. Arbeitslosenquote nach Kantonen. Available from https://www.amstat.ch/v2/index.jsp?lang=de
35Institut national de la statistique et des études économiques (INSEE). Taux de chômage France (y compris Dom) depuis 1996. Available from http://www.insee.fr/fr/indicateurs/ind14/20150305/sl_chomage_metrodom.xls
36 Arcaya M , Glymour MM , Christakis NA , Kawachi I , Subramanian SV . Individual and spousal unemployment as predictors of smoking and drinking behavior. Soc Sci Med. 2014;110:89–95. https://doi.org/10.1016/j.socscimed.2014.03.034
37Office for National Statistics (ONS). Opinions and Lifestyle Survey, Smoking Habits Amongst Adults, 2012. Available from http://www.ons.gov.uk/ons/dcp171776_328041.pdf
38Action on Smoking and health (ASH). Smoking Statitistics: Who Smokes and How Much. ASH Fact Sheet, June 9 2016. Available from http://ash.org.uk/download/smoking-statistics-who-smokes-and-how-much-2/
39Institut national de la statistique et des études économiques (INSEE). Taux de chômage France (y compris Dom) depuis 1996. Available from http://www.insee.fr/fr/indicateurs/ind14/20150305/sl_chomage_metrodom.xls
40Staatssekretariat für Wirtschaft SECO. Arbeitsmarkt und Arbeitslosenversicherung. Arbeitslosenquote nach Kantonen. Available from https://www.amstat.ch/v2/index.jsp?lang=de
41 Bélanger RE , Marclay F , Berchtold A , Saugy M , Cornuz J , Suris JC . To what extent does adding tobacco to cannabis expose young users to nicotine? Nicotine Tob Res. 2013;15(11):1832–8. https://doi.org/10.1093/ntr/ntt063
42 Marmet S , Rehm J , Gmel G , Frick H , Gmel G . Alcohol-attributable mortality in Switzerland in 2011--age-specific causes of death and impact of heavy versus non-heavy drinking. Swiss Med Wkly. 2014;144:w13947. Available at: https://smw.ch/article/doi/smw.2014.13947.
43World health Organization. Global Action Plan for the Prevention and Control of Non-Communicable Diseases 2013-2020. WHO 2013. Available from http://www.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf?ua=1
No financial support and no other potential conflict of interest relevant to this article was reported.