Regional sociocultural differences as important correlate of physical activity and sedentary behaviour in Swiss preschool children
DOI: https://doi.org/10.4414/smw.2016.14377
Claudia S.
Leeger-Aschmann, Einat A.
Schmutz, Thomas
Radtke, Tanja H.
Kakebeeke, Annina E.
Zysset, Nadine
Messerli-Bürgy, Kerstin
Stülb, Amar
Arhab, Andrea H.
Meyer, Simone
Munsch, Oskar G.
Jenni, Jardena J.
Puder, Susi
Kriemler
Summary
QUESTION: Regional differences in physical activity in school-aged children and adults even within one country with the same political and health care system have been observed and could not be explained by sociodemographic or individual variables. We analysed whether such differences were already present in preschool children.
METHODS: Swiss children from 84 childcare centres in five cantons (Aargau, Bern, Fribourg, Vaud, Zurich) comprising about 50% of the population of the country participated. Physical activity was quantified with accelerometers (ActiGraph, wGT3X-BT) and potential correlates were assessed with measurements at the childcare centre or questionnaires. Mixed regression models were used to test associations between potential correlates of total physical activity (TPA), moderate-to-vigorous physical activity (MVPA), light physical activity (LPA) or sedentary behaviour with a special focus on regional differences.
RESULTS: 394 of 476 children (83%) provided valid physical activity data (at least 2 weekdays and 1 weekend day with 10 h recording; mean age 3.9 ± 0.7 years, 54% boys) with 26% and 74% living in the French- and German-speaking parts of Switzerland, respectively. Days consisted of (mean ± standard deviation) 1.5 ± 0.5 h MVPA, 5.0 ± 0.6 h LPA, and 6.3 ± 0.8 h sedentary behaviour with an average of 624 ± 150 counts/min TPA. TPA and MVPA (but not sedentary behaviour or LPA) increased with age, were higher in boys and children with better motor skills. Despite controlling for individual characteristics, familial factors and childcare exposure, children from the French-speaking part of Switzerland showed 13% less TPA, 14% less MVPA, 6% less LPA and 8% more sedentary behaviour than German-speaking children.
CONCLUSION: Beside motor skills and non-modifiable individual factors, the regional sociocultural difference was the most important correlate of phyical activity and sedentary behaviour. Therefore, regionally adapted public health strategies may be needed.
Trial registration:ISRCTN41045021
Abbreviations
BMI: body mass index
ISEI: International Socio-Economic Index
LPA: light physical activity
MVPA: moderate-to-vigorous physical activity
TPA: total physical activity
Introduction
Physical activity is fundamental for adequate development of children and important for their general health. Physical activity promotes motor skills, prevents obesity, reduces the risk of cardiovascular diseases, enhances bone density and improves psychosocial health [1–4]. Nevertheless, children spend several hours a day inactive [5] and even most preschool children fulfil only a part of the recommendations in international guidelines of at least 3 h of any physical activity and at most 1 h of media use [6].
Understanding children’s physical activity and sedentary behaviour provides the foundation for evidence-based planning of interventions. Physical activity and sedentary behaviour are highly complex behavioural patterns, which have innumerable influencing factors. Although there may be a variety of reasons such as climate or cohort effects that can explain differences in physical activity between countries, cultural differences may also play a crucial role [7, 8]. A possible explanation may be differences in sport policies and access to sport facilities, which may explain why Swiss school-aged children are more active than children in other European countries [8]. In fact, they are more often engaged in sports and are less likely to be overweight [9]. But even within Switzerland sociocultural differences may have an impact on physical activity. Relatively large differences in physical activity were found between children of native and non-native ethnicity, where immigrant children spent significantly more time sedentary [10] or commuted to school actively less often [9]. According to self-reported information, sport participation is higher in the German- than in the French-speaking populations of Switzerland in children [11] as well as in adults [12]. French-speaking kindergarten children have more adiposity, and are more sedentary and less physically active than those from the German-speaking area [10]. Although the two regions differ with respect to environmental characteristics (such as availability of main or dead-end streets or green playing areas), this could not explain the differences in physical activity behaviour between the language boundaries in early school-age children [13].
We hypothesised that differences in physical activity and sedentary behaviour between language areas within Switzerland may indeed be culturally engrained rather than explained by other predictors such as individual or family characteristics, the school system or the environment in which the children live. Therefore, we aimed to determine if these regional sociocultural differences in physical activity and sedentary behaviour could already be found in a very young population, before they enter the mandatory school system. For this purpose, we used baseline data of a randomly selected cohort attending childcare, the Swiss Preschoolers’ Health Study (SPLASHY).
Methods
Study design and participants
The overall aim of SPLASHY was to investigate how stress and physical activity influence children’s health defined as psychological well-being, adequate cognitive functioning, absence of adiposity and proficient motor skills as described previously [14]. SPLASHY is a registered (ISRCTN41045021) multicentre cohort study including 2- to 6-year-old-children within two sociocultural areas of Switzerland (French- and German-speaking parts).
Children were recruited from randomly selected childcare centres in five cantons of Switzerland (Aargau, Bern, Fribourg, Vaud, Zurich) comprising about 50% of the Swiss population, stratified for area (urban vs rural) and socioeconomic region of the childcare centres (high vs low). Eighty-four of 639 contacted childcare centres participated; the only exclusion criterion for preschool children was the inability to perform the tests (e.g., motor or cognitive disability).
Measurements
Physical activity was monitored with an accelerometer (wGT3X-BT, ActiGraph, Pensacola, Florida, USA) that was continuously worn at the hip for at least 1 week. The device is a small and lightweight tri-axial accelerometer (4.6 cm × 3.3 cm × 1.5 cm, 19 g) that measures accelerations of the body in a three dimensional system. The sampling rate of the accelerometer was set at 30 Hertz. Initialisation, downloading and converting was done with the ActiLife software (version 6). Raw data were downloaded, at a sampling epoch of 3 sec, able to capture very brief episodes of physical activity, typical for preschool children. For further data control by the statistical software R, the raw files were converted (from gt3x into csv). Only the activity behaviour during the day (between 7 a.m. and 9 p.m.) was analysed. Periods of 20 min or more of continuous zeros were removed and considered as non-wear time [15]. Data were valid if the children accumulated at least two weekdays and one weekend day with a minimum of 10 h of wearing time. The epoch length of the valid days was finally integrated from 3 to 15 sec and data were expressed as total physical activity (TPA; counts/min) and as time spent in sedentary behaviour, or light or moderate-to-vigorous physical activity (LPA and MVPA; min/day) according to validated cut-points [16] and most recent recommendations [17]. The cut-points were 25 and 420 counts/15 sec for LPA and MVPA, respectively.
Gross motor skills were assessed by trained investigators using a valid and reliable test (Zurich Neuromotor Assessment) [18, 19]. A shortened version was used, which included the assessments of pure and adaptive motor tasks, and static and dynamic balance. All tests were video recorded and analysed offline by trained evaluators. A total age and gender adapted z-score was calculated for the quantification of gross motor skill performance for all children with a full set of individual test items [18].
Questionnaires were completed by parents either on paper or electronically according to their preference. They comprised information on age, sex, living area (French vs German and urban vs rural), the migrant status of the child (defined as yes if at least one parent was born outside Switzerland), the presence of older siblings (yes-no), and the workload of the parents (both/one single parent(s) working vs only one of two parents working vs one single/both parent(s) doesn’t/don’t work). The socioeconomic status was calculated by coding the profession of both parents with further transformation into the International Socio-Economic Index (ISEI) value [20]. The higher of the two parental ISEI values was taken for analyses. Furthermore, parents provided information about their physical activity behaviour together with the child (categorised into no physical activity vs at least once a week physical activity with either mother/father or one organised physical activity lesson vs at least 2–3 times a week physical activity with either mother/father or several organised physical activity lessons), home environment safety based on the subjective perception of the road, neighbourhood, child and yard safety [21] and the childcare attendance (number of days per week).
Ethical considerations
The cantonal ethics committee of each study site (Vaud, Berne, Fribourg and Zurich) approved the study protocol. The study was conducted in accordance with the Declaration of Helsinki. Children consented orally and parents gave their written informed consent for study participation and families received CHF 200 for the collaboration.
Statistical analyses
The software R was used to conduct analyses (R version 3.2.1) and the significance level set at 0.05. Descriptive analyses were performed for the whole sample and stratified by invalid vs valid physical activity data and language area. Differences between children with and without physical activity data and between children of French- and German-speaking areas were compared with multilevel regression models.
Based on the socioecological approach, multilevel models were used to define potential correlates that might explain variability and differences in physical activity and sedentary behaviour in preschool children with a special focus on the language area [22]. Models for TPA were selected on the basis of the Bayesian information criterion for well-known potential correlates of physical activity in this age group, after literature research and checking for collinearity. In a first step we fixed the core correlates that were a priori included in all models 1–4 (set 1: language area [French vs German], age, sex, socioeconomic status, living area [urban vs rural], and season of physical activity measurement [spring: March–May, summer: June–August or autumn: September–November]). In each further model (2–4) an additional set of potential correlates was added (fig. 1). The potential correlates were grouped along the socioecological model in a set of modifiable individual factors (set 2: body mass index, motor skills), familial factors (set 3: migrant status, parents workload, older siblings, parent-child physical activity, safety), and a childcare factor (set 4: childcare attendance). Childcare centres were used as a random effect to account for variability among these. Multiple imputation with a chained equations technique was done to obtain 40 complete datasets [23] on the basis of the final model 4 for TPA, which included all sets of potential correlates. For the other outcomes (MVPA, LPA and sedentary behaviour) the same models as for TPA were used. To cope with multiple testing due to the use of four models, a Bonferroni correction was applied and the significance level was set at 0.0125. All models were visually checked for normally distributed residuals using q-q-plots.
Results
Descriptive characteristics of the study participants according to availability of valid physical activity data and language area are shown in table 1. In total, 394 (83%) of 476 consented preschool children had valid accelerometer data, 427 (90%) parents completed questionnaires, 463 (93%) children had anthropometry data, and 348 (73%) had valid motor tests. Children with missing or invalid accelerometer data did not differ from those with valid physical activity data, except for BMI (more overweight children had valid physical activity data) and parent-child physical activity (more children with high parent-child physical activity had valid physical activity data). Children from the French language area showed 13% less TPA, 14% less MVPA, 6% less LPA and 8% more sedentary behaviour (all p ≤0.001) compared with those from the German language area. Age, sex, socioeconomic status, living area, prevalence of overweight, motor skill performance, migrant status, workload of the parents and presence of older siblings did not differ by language area. Children from the French-speaking area differed according to season of the physical activity measurement compared with children from the German-speaking region (p <0.001). Furthermore, parents from the French language area performed physical activity with their child less often, had the subjective impression of living in a less safe home environment and their children attended childcare more often (all p <0.001).
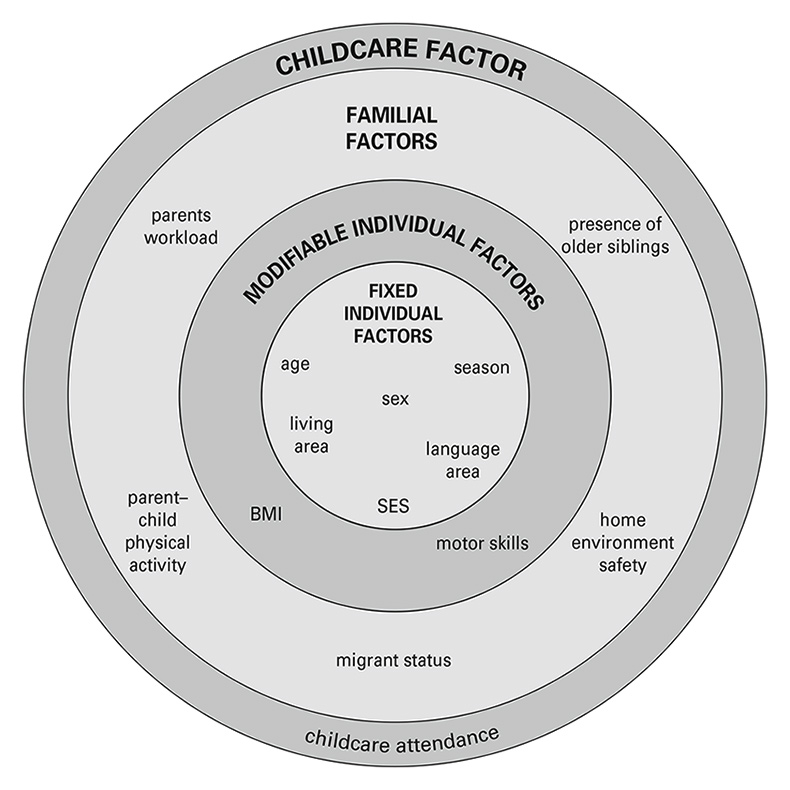
Figure 1
Based on the socioecological model potential correlates of physical activity and sedentary behaviour were grouped in different sets and added stepwise in the analysis.
Model 1 included the core correlates with fixed individual factors, Model 2 = Model 1 + modifiable individual factors, Model 3 = Model 2 + familial factors, Model 4 = Model 3 + childcare factor.
BMI = body mass index; SES = socioeconomic status
Table 2 presents results from multilevel models testing the association between potential correlates and physical activity or sedentary behaviour starting with model 1 as the core model including language area and well-known fixed individual factors. In models 2–4 successively additional sets of potential correlates that may explain differences in physical activity and sedentary behaviour were added. Among all tested correlates shown in figure 1, only correlates significantly associated with physical activity or sedentary behaviour in at least one of the models 1–4 are shown, but the non-significant variables were kept in all models. The language area was the most consistent correlate of physical activity and sedentary behaviour that persisted throughout the stepwise integration of all additional sets of potential correlates. Despite controlling for individual characteristics, familial factors and childcare exposure, children from the French-speaking part of Switzerland showed less Pphysical activityA and more sedentary behaviour than German-speaking children. The additional correlates with an association with physical activity or sedentary behaviour included age (increasing TPA and MVPA with age), sex (boys showed more TPA and MVPA than girls), season (more LPA and less sedentary behaviour in autumn compared with spring), and motor skills (positively related to TPA and MVPA).
|
Table 1: Descriptive characteristics of the participants. |
|
Children without valid physical activity data
n = 82
|
Children
with valid physical activity data
n = 394
|
French-
speaking
children
n =104
|
German-
speaking
children
n = 290
|
|
Fixed individual factors
|
| French-speaking children†, n (%) |
19 (23) |
104 (26) |
104 (100) |
0 (0) |
| Age (years) |
3.8 ± 0.6 |
3.9 ± 0.7 |
3.8 ± 0.6 |
4.0 ± 0.7 |
| Male, n (%) |
38 (46) |
213 (54) |
57 (55) |
156 (54) |
| Socioeconomic status‡
|
63.8 ± 16.1 |
61.5 ± 15.9 |
58.5 ± 17.7 |
62.6 ± 15.0 |
| Living area, n (%) |
|
|
|
|
| Urban |
29 (35) |
136 (35) |
52 (50) |
84 (29) |
| Rural |
45 (55) |
245 (62) |
52 (50) |
193 (67) |
| Season†, n (%) |
|
|
|
|
| Spring |
32 (39) |
226 (57) |
70 (67) |
156 (54) |
| Summer |
33 (40) |
98 (25) |
18 (17) |
80 (28) |
| Autumn |
17 (21) |
70 (18) |
16 (15) |
54 (19) |
|
Modifiable individual factors
|
| Body mass index*, n (%) |
|
|
|
|
| Normal weight |
65 (79) |
292 (74) |
80 (77) |
212 (73) |
| Overweight |
9 (11) |
97 (25) |
22 (21) |
75 (26) |
| Motor skills (z-scores) |
–0.04 ± 1.04 |
0.00 ± 1.00 |
0.04 ± 0.93 |
–0.01 ± 1.02 |
|
Familial factors
|
| Migrant status, n (%) |
|
|
|
|
| Both parents Swiss |
23 (28) |
164 (42) |
38 (37) |
126 (43) |
| 1 or 2 parent(s) from abroad |
49 (60) |
211 (54) |
65 (63) |
146 (50) |
| Workload, n (%) |
|
|
|
|
| No work |
3 (4) |
7 (2) |
3 (3) |
4 (1) |
| 1 parent works |
7 (9) |
41 (10) |
14 (13) |
27 (9) |
| Single/both parent(s) work(s) |
61 (74) |
323 (82) |
82 (79) |
241 (83) |
| Older siblings, n (%) |
|
|
|
|
| Yes |
29 (35) |
164 (42) |
49 (47) |
115 (40) |
| No |
44 (54) |
217 (55) |
55 (53) |
162 (56) |
| Parent-child physical activity*†, n (%) |
|
|
|
|
| Never |
14 (17) |
36 (9) |
22 (21) |
14 (5) |
| Once a week |
23 (28) |
142 (36) |
40 (38) |
102 (35) |
| 2 or more times/week |
34 (41) |
178 (45) |
34 (33) |
144 (50) |
| Home environment safety†
|
12.4 ± 6.8 |
12.5 ± 7.0 |
15.8 ± 7.2 |
11.3 ± 6.4 |
|
Childcare factors
|
| Childcare attendance† (days/week) |
3.0 ± 1.3 |
2.8 ± 1.2 |
3.4 ± 1.2 |
2.6 ± 1.1 |
|
Physical activity and sedentary behaviour
|
| Mean wear time (min/day) |
|
769 ± 35 |
768 ± 30 |
769 ± 36 |
| Total physical activity† (counts/min) |
|
624 ± 150 |
562 ± 118 |
646 ± 155 |
| Moderate-to-vigorous physical activity† (min/day) |
93 ± 30 |
83 ± 24 |
96 ± 30 |
| Light physical activity† (min/day) |
|
301 ± 33 |
288 ± 31 |
306 ± 33 |
| Sedentary behaviour† (min/day) |
|
374 ± 48 |
397 ± 41 |
367 ± 48 |
| If not otherwise specified, values are mean ± standard deviation
* Significant difference between children with invalid vs valid physical activity data
† Significant difference between French- vs German-speaking part of Switzerland
‡ Based on the International Socio-Economic Index (ISEI) |
|
Table 2: Data show imputed beta coefficients with 95% confidence limits for significant tested correlates of physical activity according to four models based on the socioecological theory. |
|
Model
|
Language area
|
Age
|
Sex
|
Season
|
Motor skills
|
|
TPA
(counts/min)
|
1 |
75.1 (42.6, 107.5) |
58.6 (38.6, 78.6) |
–41.5 (–69.3, –13.7) |
n.s. |
– |
| 2 |
76.7 (44.6, 108.8) |
59.2 (39.6, 79.1) |
–42.0 (–69.4, –14.4) |
n.s. |
25.5 (10.5, 40.4) |
| 3 |
65.5 (31.5, 99.6) |
57.2 (37.1, 77.3) |
–39.0 (–66.6, –11.2) |
n.s. |
25.3 (10.1, 40.5) |
| 4 |
62.7 (28.0, 97.5) |
56.8 (36.7, 76.9) |
–39.6 (–67.4, –11.6) |
n.s. |
25.4 (10.2, 40.5) |
|
MVPA
(min/day)
|
1 |
11.7 (5.5, 17.8) |
13.8 (10.1, 17.6) |
–13.3 (–18.5, –8.0) |
n.s. |
– |
| 2 |
11.9 (5.9, 18.0) |
14.0 (10.3, 17.8) |
–13.4 (–18.6, –8.2) |
n.s. |
5.3 (2.5, 8.0) |
| 3 |
10.8 (4.4, 17.3) |
13.6 (9.8, 17.5) |
–12.9 (–18.2, –7.7) |
n.s. |
5.3 (2.5, 8.1) |
| 4 |
10.6 (4.0, 17.2) |
13.6 (9.8, 17.4) |
–13.0 (–18.2, –7.7) |
n.s. |
5.3 (2.5, 8.1) |
|
LPA
(min/day)
|
1 |
17.8 (10.3, 25.3) |
n.s. |
n.s. |
14.4 (5.6, 23.3) |
– |
| 2 |
17.8 (10.3, 25.3) |
n.s. |
n.s. |
14.4 (5.4, 23.4) |
n.s. |
| 3 |
16.2 (8.0, 24.5) |
n.s. |
n.s. |
14.3 (4.9, 23.7) |
n.s. |
| 4 |
14.7 (6.5, 23.0) |
n.s. |
n.s. |
13.7 (4.4, 22.9) |
n.s. |
|
sedentary behaviour
(min/day)
|
1 |
–29.8 (–40.6, –19.0) |
n.s. |
n.s. |
–17.4 (–30.2, –4.5) |
– |
| 2 |
–29.9 (–40.7, –19.1) |
n.s. |
n.s. |
n.s. |
n.s. |
| 3 |
–25.1 (–36.5, –13.6) |
n.s. |
n.s. |
n.s. |
n.s. |
| 4 |
–23.6 (–35.4, –12.0) |
n.s. |
n.s. |
n.s. |
n.s. |
| LPA = light physical activity; MVPA = moderate-to-vigorous physical activity; n.s. = not significant; TPA = total physical activity
Model 1 = fixed individual factors (language area, age, sex, SES, living area, season)
Model 2 = Model 1 + modifiable individual factors (BMI and motor skills)
Model 3 = Model 2 + familial factors (migrant status, parents workload, older siblings, parent-child physical activity, safety)
Model 4 = Model 3 + childcare factor (childcare attendance)
The reference category for language area is French (vs German), for sex boys (vs girls), and for season spring (vs autumn). Only the variables that were significant in at least one of the models are listed
p-values ≥0.0125 are stated as not significant (n.s.). |
Discussion
This study showed that discrepancies in physical activity and sedentary behaviour along the French-German language boundaries indeed already exist in Swiss preschool children. These findings are in accordance with studies in Swiss school-aged children [10, 12, 13] and adults [12, 24], which indicated that the German-speaking part of Switzerland shows a healthier activity pattern than the French-speaking area. These differences remained despite our extensive attempt to explain them by a stepwise integration of known correlates of physical activity and sedentary behaviour in our age group, such as individual, familial or environmental factors.
The difference in physical activity and sedentary behaviour remained stable across the language boundaries, even if the models were controlled for known individual, familial and environmental correlates of physical activity and sedentary behaviour in the preschool period (see fig. 1). Age, gender and motor skills were highly related to physical activity and sedentary behaviour, but could not explain differences across language boundaries. The variability of physical activity and sedentary behaviour among the French- and German-speaking areas ranged from 6–14%, corresponding to 13 min MVPA, 18 min LPA and 30 min of sedentary behaviour per day. The difference in physical activity between the two language regions remained significant even when weekdays or weekend days were considered separately. These differences were shown to have a significant, clinically relevant influence on cardiovascular risk reduction in school-aged children [3, 25, 26], but their relevance at preschool age is less clear [2]. As our children meet guideline recommendations for physical activity of at least 180 min of any type of physical activity per day or 60 min of MVPA even in the French part of Switzerland, very early prevention to maintain sufficient levels of physical activity and prevent a rise in sedentary behaviour may start during the first years of life and if so, needs to be adapted to the regional sociocultural environment.
Age and sex have consistently been shown to be associated with physical activity and sedentary behaviour in children and adolescents. Physical activity increases continuously to a peak in childhood with a culmination point that is not well defined, but it drops thereafter towards adult levels by about 4% per year [7]. Nevertheless, literature reports are conflicting for the preschool age, ranging from a positive [6, 7] to no association [27]. Different findings may have been caused by heterogeneous assessment methods (types of accelerometers, chosen epoch length and/or cut-points [28]) or a lack of variation in age range. Although males show higher physical activity values than females throughout life [6–8, 29], it is important to realise that in our study this sex difference already existed at a very young age, starting at 2 years. These gender differences may also be rooted in a weaker influence of familial and environmental factors on physical activity in girls than boys [30] or may simply be inherited gender-related differences in temperament [31].
Motor skill performance was the only potentially modifiable correlate of physical activity and sedentary behaviour that remained in the models 1–4 and on which we could base intervention strategies. Children with more poorly developed motor skills were less active than those with better performance, which is consistent with the literature for both French- and German-speaking regions [32]. In fact, it was shown that motor skill interventions improve physical activity [33] and vice versa [1, 32]. The direction of the relationship (i.e., whether children with better motor skills are more active or more active children have better motor skills) is still controversial [34]. However, the best strategy may simply be to intervene on both sides of the equation. Therefore attempts should be made to increase physical activity and reduce sedentary behaviour on the one hand, and to implement programmes aiming to improve motor skills on the other hand. Intervening at a very young age, preferably in the preschool setting, seems to be a convenient and effective way [35] not only to improve physical activity and motor skills, but also to enhance psychosocial health [2] and prevent obesity [36].
Strengths of the SPLASHY study are the randomly selected, relatively large population within a small country, with the ratio of French- to German-speaking participants representing the proportional distribution in Switzerland. Furthermore, objective assessments were applied whenever possible. Limitations of our study include the fact that that we only assessed physical activity of the two main lingual regions, while the much smaller Italian and Rhaeto-Romance areas of Switzerland were not included for logistical reasons. Furthermore, the study participation was voluntary and focused only on children attending childcare, which may have led to a potential participation bias. The assessments of rolling activities such as riding bogie wheels, tricycles or bicycles are measured imprecisely by accelerometers because there is not much change in acceleration. Even though we removed the night sleep between 9 p.m. and 7 a.m., most of the preschool children still tended to nap during the day. This day sleep could have led to an underestimation of physical activity. Nevertheless, we assume that most of this nap sleep was excluded from the analysis as a result of our definition of non-wear time (20 min of consecutive zeros of recorded activity). The analysis approach included a number of data selection decisions (number of days, length of day, epoch length, cut-points and definition of non-wear time). Any of these data selection decisions could have influenced the results of the study, but it is unlikely that this would have affected the German- and French-speaking population differently. Another disadvantage was the fact that physical activity was not recorded during water activities, which could have led to an underestimation of overall physical activity. However, our findings perfectly reflect previous Swiss studies looking at differences in physical activity or lifestyle behaviour in older age groups [10, 12, 13, 24]. This may reinforce the assumption that there was no major selection bias and the abovementioned limitations occurred at random in both language areas.
Conclusion
Beside motor skills and non-modifiable individual factors, the regional sociocultural difference in activity behaviour beyond socioeconomic state was the most important correlate of physical activity and sedentary behaviour and, thus, may exist within one country and already at a very young age. Key differences may occur according to language boundaries (as in our example), religious differences or an immigrant background. These differences may be clinically relevant and should be assessed in multicultural countries to better understand variation of physical activity and sedentary behaviour within and between countries. Finally, such findings will help to define public health recommendations and interventions that may need to be culturally adapted.
Acknowledgement: We would like to thank all children, families and childcare centres that contributed data to SPLASHY. We also thank all students and the research team for their valuable contribution.
References
1 Roth K, Kriemler S, Lehmacher W, Ruf KC, Graf C, Hebestreit H. Effects of a Physical Activity Intervention in Preschool Children. Med Sci Sports Exerc. 2015;47(12):2542–51. doi:http://dx.doi.org/10.1249/MSS.0000000000000703. PubMed
2 Timmons BW, Leblanc AG, Carson V, Connor Gorber S, Dillman C, Janssen I, et al. Systematic review of physical activity and health in the early years (aged 0-4 years). Appl Physiol Nutr Metab. 2012;37(4):773–92. doi:http://dx.doi.org/10.1139/h2012-070. PubMed
3 Andersen LB, Riddoch C, Kriemler S, Hills AP. Physical activity and cardiovascular risk factors in children. Br J Sports Med. 2011;45(11):871–6. doi:http://dx.doi.org/10.1136/bjsports-2011-090333. PubMed
4 Meyer U, Ernst D, Zahner L, Schindler C, Puder JJ, Kraenzlin M, et al. 3-Year follow-up results of bone mineral content and density after a school-based physical activity randomized intervention trial. Bone. 2013;55(1):16–22. doi:http://dx.doi.org/10.1016/j.bone.2013.03.005. PubMed
5 Pate RR, Mitchell JA, Byun W, Dowda M. Sedentary behaviour in youth. Br J Sports Med. 2011;45(11):906–13. doi:http://dx.doi.org/10.1136/bjsports-2011-090192. PubMed
6 Hinkley T, Salmon J, Okely AD, Crawford D, Hesketh K. Preschoolers’ physical activity, screen time, and compliance with recommendations. Med Sci Sports Exerc. 2012;44(3):458–65. doi:http://dx.doi.org/10.1249/MSS.0b013e318233763b. PubMed
7 Cooper AR, Goodman A, Page AS, Sherar LB, Esliger DW, van Sluijs EM, et al. Objectively measured physical activity and sedentary time in youth: the International children’s accelerometry database (ICAD). Int J Behav Nutr Phys Act. 2015;12(1):113. doi:http://dx.doi.org/10.1186/s12966-015-0274-5. PubMed
8 Verloigne M, Van Lippevelde W, Maes L, Yıldırım M, Chinapaw M, Manios Y, et al. Levels of physical activity and sedentary time among 10- to 12-year-old boys and girls across 5 European countries using accelerometers: an observational study within the ENERGY-project. Int J Behav Nutr Phys Act. 2012;9(1):34. doi:http://dx.doi.org/10.1186/1479-5868-9-34. PubMed
9 Herzig M, Dössegger A, Mäder U, Kriemler S, Wunderlin T, Grize L, et al. Differences in weight status and energy-balance related behaviors among schoolchildren in German-speaking Switzerland compared to seven countries in Europe. Int J Behav Nutr Phys Act. 2012;9(1):139. doi:http://dx.doi.org/10.1186/1479-5868-9-139. PubMed
10 Bürgi F, Meyer U, Niederer I, Ebenegger V, Marques-Vidal P, Granacher U, et al. Socio-cultural determinants of adiposity and physical activity in preschool children: a cross-sectional study. BMC Public Health. 2010;10(1):733. doi:http://dx.doi.org/10.1186/1471-2458-10-733. PubMed
11 Lamprecht M, Fischer A, Wiegand D, Stamm HP. Sport Schweiz 2014: Kinder- und Jugendbericht. Magglingen: Bundesamt für Sport BASPO; 2014
12 Lamprecht M, Fischer, A, Wiegand, D, Stamm, HP. Sport Schweiz 2014: Sportaktivität und Sportinteresse der Schweizer Bevölkerung. Magglingen: Bundesamt für Sport BASPO; 2014.
13 Bringolf-Isler B, Mäder U, Dössegger A, Hofmann H, Puder JJ, Braun-Fahrländer C, et al. Regional differences of physical activity and sedentary behaviour in Swiss children are not explained by socio-demographics or the built environment. Int J Public Health. 2015;60(3):291–300. doi:http://dx.doi.org/10.1007/s00038-014-0645-8. PubMed
14 Messerli-Bürgy N, Kakebeeke TH, Arhab A, Stülb K, Zysset AE, Leeger-Aschmann CS, et al. The Swiss Preschoolers’ health study (SPLASHY): objectives and design of a prospective multi-site cohort study assessing psychological and physiological health in young children. BMC Pediatr. 2016;16(1):85. doi:http://dx.doi.org/10.1186/s12887-016-0617-7. PubMed
15 Cliff DP, Reilly JJ, Okely AD. Methodological considerations in using accelerometers to assess habitual physical activity in children aged 0-5 years. J Sci Med Sport. 2009;12(5):557–67. doi:http://dx.doi.org/10.1016/j.jsams.2008.10.008. PubMed
16 Pate RR, Almeida MJ, McIver KL, Pfeiffer KA, Dowda M. Validation and calibration of an accelerometer in preschool children. Obesity (Silver Spring). 2006;14(11):2000–6. doi:http://dx.doi.org/10.1038/oby.2006.234. PubMed
17 Janssen X, Cliff DP, Reilly JJ, Hinkley T, Jones RA, Batterham M, et al. Predictive validity and classification accuracy of ActiGraph energy expenditure equations and cut-points in young children. PLoS One. 2013;8(11):e79124. doi:http://dx.doi.org/10.1371/journal.pone.0079124. PubMed
18 Kakebeeke TH, Locatelli I, Rousson V, Caflisch J, Jenni OG. Improvement in gross motor performance between 3 and 5 years of age. Percept Mot Skills. 2012;114(3):795–806. doi:http://dx.doi.org/10.2466/10.13.25.PMS.114.3.795-806. PubMed
19 Kakebeeke TH, Caflisch J, Chaouch A, Rousson V, Largo RH, Jenni OG. Neuromotor development in children. Part 3: motor performance in 3- to 5-year-olds. Dev Med Child Neurol. 2013;55(3):248–56. doi:http://dx.doi.org/10.1111/dmcn.12034. PubMed
20 Ganzeboom HBG: A new international socio-economic index (ISEI) of occupational status for the international standard classification of occupation 2008 (ISCO-08) constructed with data fro the ISSP 2002-2007; with an analysis of quality of occupational measurement in ISSP. Paper presented at Annual Conference of International Social Survey Programm, Lisbon, May 1 2010.
21 Ding D, Sallis JF, Kerr J, Lee S, Rosenberg DE. Neighborhood environment and physical activity among youth a review. Am J Prev Med. 2011;41(4):442–55. doi:http://dx.doi.org/10.1016/j.amepre.2011.06.036. PubMed
22 Davison KK, Birch LL. Childhood overweight: a contextual model and recommendations for future research. Obes Rev. 2001;2(3):159–71. doi:http://dx.doi.org/10.1046/j.1467-789x.2001.00036.x. PubMed
23 van Buuren S, Groothuis-Oudshoorn K. mice: Multivariate Imputation by Chained Equations in R. J Stat Softw. 2011;45(3):1–67.
24 Faeh D, Minder C, Gutzwiller F, Bopp M; Swiss National Cohort Study Group. Culture, risk factors and mortality: can Switzerland add missing pieces to the European puzzle? J Epidemiol Community Health. 2009;63(8):639–45. doi:http://dx.doi.org/10.1136/jech.2008.081042. PubMed
25 Kriemler S, Zahner L, Schindler C, Meyer U, Hartmann T, Hebestreit H, et al. Effect of school based physical activity programme (KISS) on fitness and adiposity in primary schoolchildren: cluster randomised controlled trial. BMJ. 2010;340(feb23 1):c785. doi:http://dx.doi.org/10.1136/bmj.c785. PubMed
26 Ekelund U, Luan J, Sherar LB, Esliger DW, Griew P, Cooper A; International Children’s Accelerometry Database (ICAD) Collaborators. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA. 2012;307(7):704–12. doi:http://dx.doi.org/10.1001/jama.2012.156. PubMed
27 Finn K, Johannsen N, Specker B. Factors associated with physical activity in preschool children. J Pediatr. 2002;140(1):81–5. doi:http://dx.doi.org/10.1067/mpd.2002.120693. PubMed
28 Bornstein DB, Beets MW, Byun W, McIver K. Accelerometer-derived physical activity levels of preschoolers: a meta-analysis. J Sci Med Sport. 2011;14(6):504–11. doi:http://dx.doi.org/10.1016/j.jsams.2011.05.007. PubMed
29 Bonvin A, Barral J, Kakebeeke TH, Kriemler S, Longchamp A, Marques-Vidal P, et al. Weight status and gender-related differences in motor skills and in child care – based physical activity in young children. BMC Pediatr. 2012;12(1):23. doi:http://dx.doi.org/10.1186/1471-2431-12-23. PubMed
30 Telford RM, Telford RD, Olive LS, Cochrane T, Davey R. Why Are Girls Less Physically Active than Boys? Findings from the LOOK Longitudinal Study. PLoS One. 2016;11(3):e0150041. doi:http://dx.doi.org/10.1371/journal.pone.0150041. PubMed
31 Maia JAR, Thomis M, Beunen G. Genetic factors in physical activity levels: a twin study. Am J Prev Med. 2002;23(2, Suppl):87–91. doi:http://dx.doi.org/10.1016/S0749-3797(02)00478-6. PubMed
32 Bürgi F, Meyer U, Granacher U, Schindler C, Marques-Vidal P, Kriemler S, et al. Relationship of physical activity with motor skills, aerobic fitness and body fat in preschool children: a cross-sectional and longitudinal study (Ballabeina). Int J Obes. 2011;35(7):937–44. doi:http://dx.doi.org/10.1038/ijo.2011.54. PubMed
33 Barnett LM, van Beurden E, Morgan PJ, Brooks LO, Beard JR. Childhood motor skill proficiency as a predictor of adolescent physical activity. J Adolesc Health. 2009;44(3):252–9. doi:http://dx.doi.org/10.1016/j.jadohealth.2008.07.004. PubMed
34 Stodden DF, Goodway JD, Langendorfer SJ, Roberton MA, Rudisill ME, Garcia C, et al. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest. 2008;60(2):290–306. doi:http://dx.doi.org/10.1080/00336297.2008.10483582.
35 Goldfield GS, Harvey A, Grattan K, Adamo KB. Physical activity promotion in the preschool years: a critical period to intervene. Int J Environ Res Public Health. 2012;9(4):1326–42. doi:http://dx.doi.org/10.3390/ijerph9041326. PubMed
36 Nader PR, O’Brien M, Houts R, Bradley R, Belsky J, Crosnoe R, et al.; National Institute of Child Health and Human Development Early Child Care Research Network. Identifying risk for obesity in early childhood. Pediatrics. 2006;118(3):e594–601. doi:http://dx.doi.org/10.1542/peds.2005-2801. PubMed