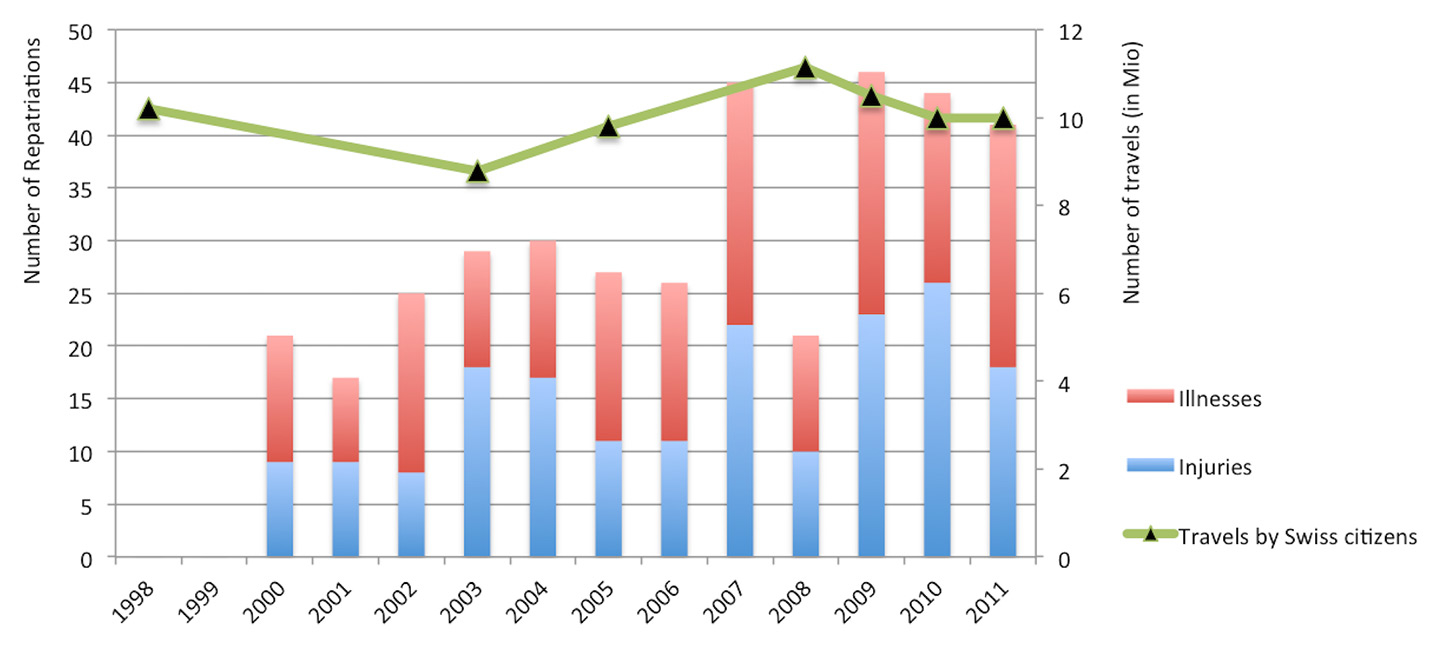
Figure 1
Number of repatriated patients per year over the study period and number of travels by Swiss citizens.
DOI: https://doi.org/10.4414/smw.2015.14208
The number of travellers is growing throughout the world [1, 2]. As life expectancy is increasing, even the elderly, many of whom may have pre-existing conditions, travel to remote locations and countries with underdeveloped health systems [2]. Therefore, the number of injuries and illness from underlying medical conditions has also increased, as has the number of air ambulance repatriations [3]. Almost all travellers are able to finish their trips successfully. Fewer than 0.5% need medical evacuation [4]. However, in the year 2010 there were almost 940 million international, so this low percentage results in thousands of repatriations every year [1, 2].
Depending on the severity of the injury or illness, the patient’s previous health and the available treatment facilities, medical evacuation may be necessary. An aeromedical evacuation is expensive and could be stressful for the patient. For a physician, it is a challenge to decide whether an urgent evacuation is necessary or not [5]. In Switzerland, patients are repatriated, depending on the country of travel and the distance from Switzerland, either by Swiss Air Ambulance jet, by helicopter, by ground ambulance or a by scheduled flight (with or without medical assistance). The majority of repatriations are provided by the foundation Swiss Air-Rescue “Rega” with the Swiss Air Ambulance jets and helicopters or by medical assistance on a scheduled flight. About 2.5 million Swiss citizens are Rega members and can benefit from free repatriation due to their membership if their health or travel insurance company does not cover costs for the transport. A minority of repatriations is provided by helicopter or ground ambulances of other companies. The decision on whether repatriation is necessary lies with the insurance company of the patient or, in the case of Rega members, with the Rega itself [6]. Patients are repatriated to different hospitals in Switzerland, ranging from smaller hospitals or private clinics to university hospitals, depending on the required level of care, hospital capacities, the patient’s place of residence and the patient’s or their relatives’ choice of hospital.
Patients suffering an injury or illness while travelling abroad are mostly a distinct group of people. They have already been seen in a hospital, or at least by a physician. Treatment or an operation have already been performed. If repatriation is necessary, the patients have been stabilised in order to survive the transport. The main problems for international repatriations are road traffic accidents, acute coronary syndromes, infectious diseases and complications of pregnancy [7]. In addition, patients may have been exposed to a nosocomial infection, especially in the tropics.
There are only a few studies in the literature on the epidemiology of patients who need medical repatriation. Along with the growing number of travellers and, therefore, presumably higher incidence of repatriated patients, the aim of this study was to analyse epidemiological data of patients repatriated from January 2000 to December 2011 to one major Swiss university hospital.
We conducted a retrospective cross-sectional study.
We analysed all consecutive adult patients (aged ≥16 years) who had been repatriated to our Emergency Department at Bern University Hospital in Switzerland between January 2000 and December 2011, independently of whether they needed a further stay in hospital or could be treated as outpatients. This analysis only refers to patients repatriated form a foreign country and not transferred from another part of Switzerland. Children were excluded from our analysis as they are admitted to a separate children’s hospital nearby.
Descriptive data were presented as means, together with the corresponding standard deviations for parametric data or as medians, with inter-quartile ranges (IQR) for nonparametric data. Categorical data were reported in numbers and percentages. For comparisons, the chi-squared test was used.
The parameters examined were age, gender, 28-day mortality, nationality, occupation, year and type of repatriation, injured body region / diagnostic group of illness and the country from where patients were repatriated. The level of statistical significance was set at an alpha of 5%.
We arbitrarily grouped the occupation or area of work into: (a) pensioners and handicapped pension receivers, (b) social, health and education, (c) technical, (d) agriculture, building trade, and handcrafts, (e) state, justice and services, (f) economy, gastronomy and household, (g) language, journalism and art, (h) apprenticeship, unemployed and unknown. For the type of repatriation, we differentiated between: (a) air ambulance (Rega jet), (b) ground ambulance, (c) helicopter emergency service (HEMS), (d) scheduled flights with medical assistance, (e) repatriation by patients themselves, (f) unknown type of repatriation. Illnesses were arbitrarily grouped as follows: (a–e) nervous system with subgroups (cerebrovascular insult, infections, epilepsy, tumours, other), (f) psychiatry, (g) endocrinology, (h-–j) cardiovascular system with subgroups (myocardial infarction, angina pectoris, other), (k) respiratory system, (l) gastrointestinal system, including liver, (m) haematological system, (n) kidneys and urinary tract, (o) infections, (p) musculoskeletal system, (q) eyes, ears and nose, (r) dermatology, (s) other/unknown. This is also an arbitrary grouping, and if an infection could be clearly assigned to one organ system, the illness was grouped under this, e.g. pneumonia is classified in the respiratory group. For trauma patients injuries were classified using the Abbreviated Injury Scale (AIS) for each anatomical location, based on clinical, surgical or radiological evidence of injury. Scores range from 1 to 6, with higher scores representing more severe injury. The AIS scores of the three body regions with most severe injuries was then used to calculate the Injury Severity Score (ISS), ranging from 1 to 75: the sum of the squares of the three highest AIS scores [8].
For patients with missing data on the type of repatriation, we completed our data with the records from the Swiss Air-Rescue Rega, which was in charge of most repatriations. Where information for one of the outcomes is missing, this is indicated as “unknown” in the tables and figures.
Analyses were performed in Stata Release 11 (Stata Corp, College Station, USA).
Data collection and analysis were performed according to the ethical standards of the hospital. Ethical approval was received from the Bern Cantonal Ethics Committee (registration number: 25-11-13). No funding was received.
| Table 1:Nationality of repatriated patients. | ||||||
| All | Injuries | Illnesses | ||||
| Nationality | n = 372 | (100%) | n = 182 | (100%) | n = 190 | (100%) |
| Switzerland | 320 | (86.0%) | 156 | (85.7%) | 164 | (86.3%) |
| Italy | 18 | (4.8%) | 7 | (3.9%) | 11 | (5.8%) |
| Germany | 4 | (1.1%) | 3 | (1.7%) | 1 | (0.5%) |
| Macedonia | 2 | (0.5%) | 0 | (0.0%) | 2 | (1.1%) |
| Austria | 2 | (0.5%) | 1 | (0.5%) | 1 | (0.5%) |
| France | 1 | (0.3%) | 1 | (0.5%) | 0 | (0.0%) |
| Egypt | 1 | (0.3%) | 1 | (0.5%) | 0 | (0.0%) |
| Portugal | 1 | (0.3%) | 1 | (0.5%) | 0 | (0.0%) |
| Bosnia-Herzegovina | 2 | (0.5%) | 1 | (0.5%) | 1 | (0.5%) |
| Algeria | 1 | (0.3%) | 1 | (0.5%) | 0 | (0.0%) |
| Croatia | 4 | (1.1%) | 2 | (1.1%) | 2 | (1.1%) |
| Greece | 1 | (0.3%) | 0 | (0.0%) | 1 | (0.5%) |
| Denmark | 1 | (0.3%) | 1 | (0.5%) | 0 | (0.0%) |
| Spain | 3 | (0.8%) | 1 | (0.5%) | 2 | (1.1%) |
| Turkey | 4 | (1.1%) | 1 | (0.5%) | 3 | (1.6%) |
| Serbia and Montenegro | 3 | (0.8%) | 2 | (1.1%) | 1 | (0.5%) |
| Yugoslavia | 1 | (0.2%) | 1 | (0.5%) | 0 | (0.0%) |
| Unknown | 3 | (0.8%) | 2 | (1.1%) | 1 | (0.5%) |
| Table 2: Occupation groups of repatriated patients. | ||||||
| All | Injuries | Illnesses | ||||
| Occupation groups | n = 372 | (100%) | n = 182 | (100%) | n = 190 | (100%) |
| Pensioners, handicapped | 147 | (39.5%) | 47 | (25.8%) | 100 | (52.6%) |
| Social, health, education | 26 | (7.0%) | 15 | (8.2%) | 11 | (5.8%) |
| Technical | 12 | (3.2%) | 7 | (3.8%) | 5 | (2.6%) |
| Agriculture, building trade, handcraft | 43 | (11.6%) | 26 | (14.3%) | 17 | (8.9%) |
| State, justice, service | 18 | (4.8%) | 10 | (5.5%) | 8 | (4.2%) |
| Economy, gastronomy, household | 79 | (21.2%) | 44 | (24.2%) | 35 | (18.4%) |
| Language, journalism, art | 8 | (2.2%) | 4 | (2.2%) | 4 | (2.1%) |
| Apprenticeship, unemployed, unknown | 39 | (10.5%) | 29 | (15.9%) | 10 | (5.3%) |
Between January 2000 and December 2011, 372 patients (100%) were repatriated to our university hospital. Two thirds (n = 249, 67%) were male (p <0.001). Half (n = 182, 49%) had sustained an injury, whereas 140 patients (38%) suffered from medical conditions and 50 patients (13%) from surgical pathologies.
Figure 1
Number of repatriated patients per year over the study period and number of travels by Swiss citizens.
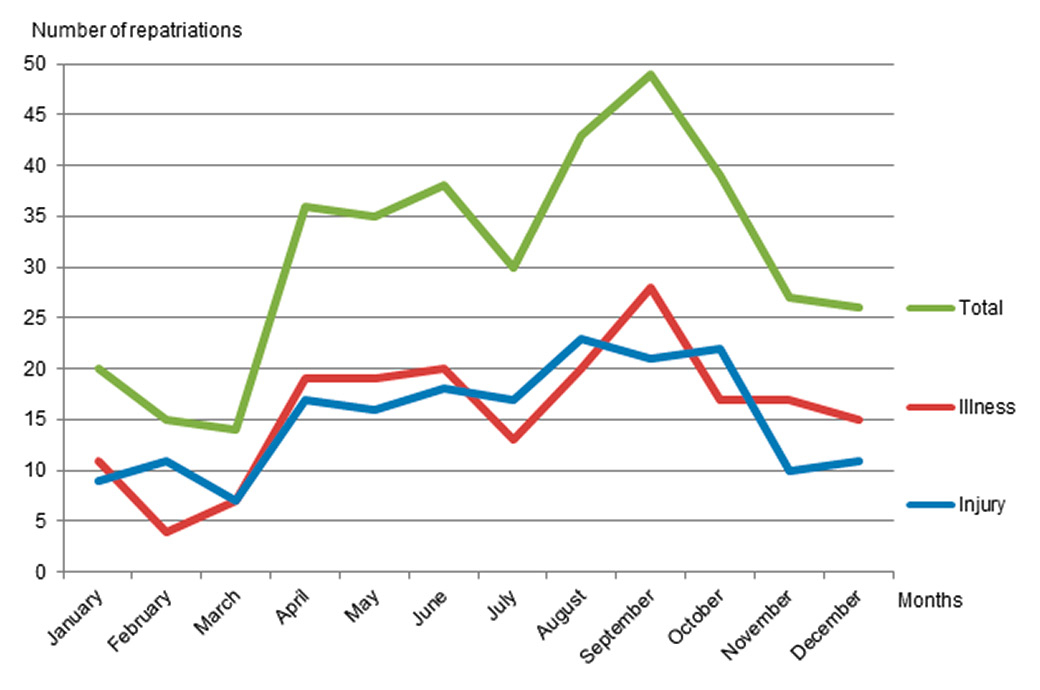
Figure 2
Repatriations per month.
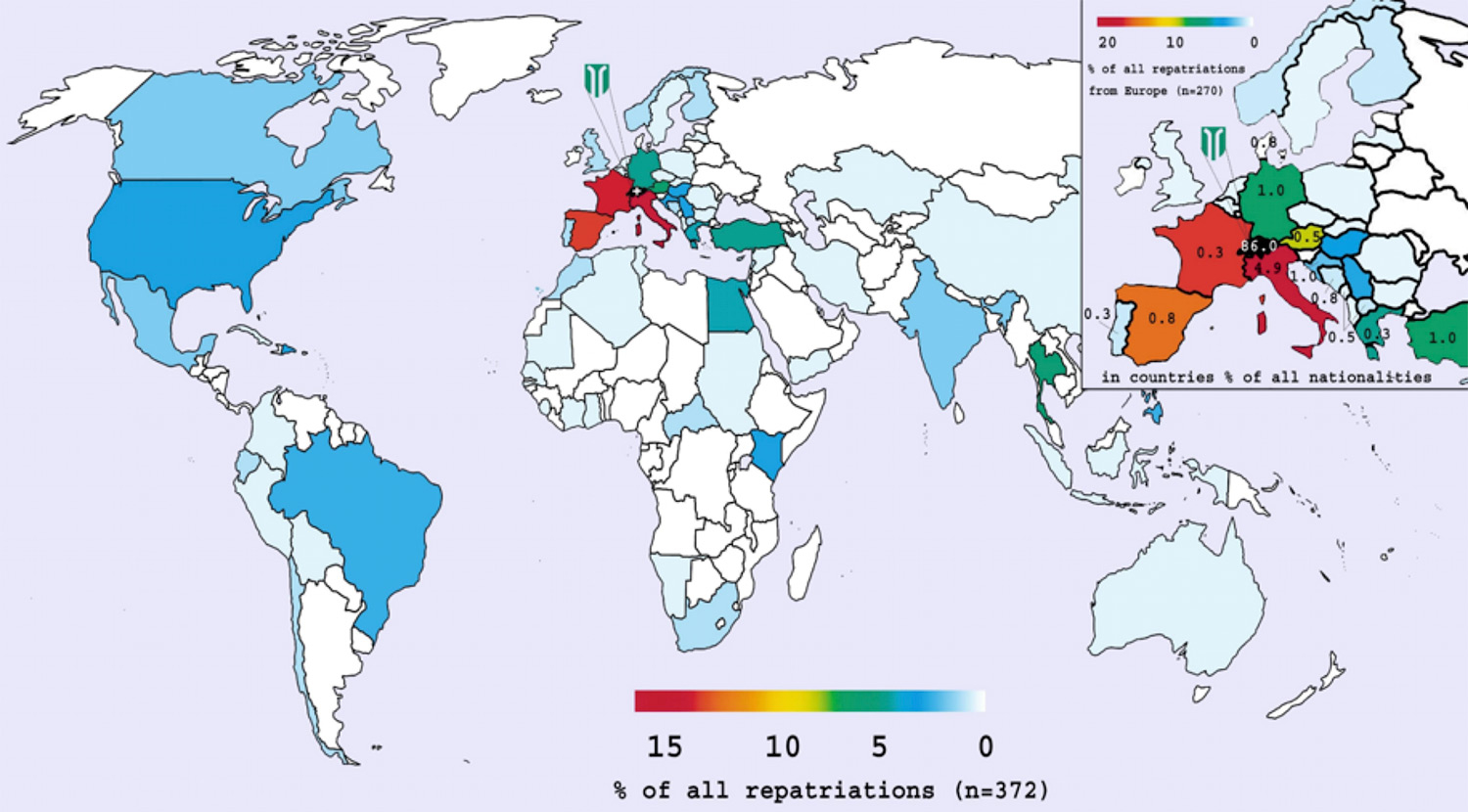
Figure 3
The percentages per country indicate the proportion of repatriated patients to the Inselspital Bern, who were nationals of this country (e.g. 4.9% of repatriated patients were Italians). The colour of the countries indicates the percentage of all repatriations from that country to Inselspital Bern.
Overall, the median age was 56 years (IQR 40–67). Patients with injuries were significantly younger (median age 47.5 years, IQR 34.0–61.0) than patients suffering from illnesses (median 63.0, IQR 49.2–70.0). Based on a Wilcoxson's rank sum test a p-value <0.001 was detected. The vast majority of patients were Swiss nationals (n = 320, 86%), followed by Italians (n = 18, 5%). Other nationalities were rare (<2% each) (table 1).
The majority of patients were pensioners and handicapped pension receivers (n = 147, 40%). The other occupations of all repatriated patients are displayed in table 2.
Over the study period, there was a significant increase in repatriated patients, from 21 patients in the 2000 to 41 in 2011 (Spearman’s rho = 0.68, p = 0.015). An exception was the year 2008, with only 21 patients (fig. 1). On average, most repatriations occurred at the end of summer and beginning of autumn (fig. 2). Figure 1 displays the number of trips by Swiss citizens and the number of repatriations over the years. Whereas the number of travels varied between, 9 million and 11 million per year, the number of repatriations steadily increased.
Figure 3 displays the percentages per country and nationalities repatriated to Inselspital Bern.
Three quarters (n = 270, 73%) of all repatriations were from European countries – mainly from Italy, France and Spain – followed by the continents of Asia (n = 34, 9%), Africa (n = 32, 9%) and North or South America (n = 30, 8%). Repatriations from Oceania were rare (<1%) (table 3 and fig. 3).
Elderly people (>65 years) were most often repatriated from Spain (43% of repatriations from Spain), Italy (40% of repatriations from Italy) and France (26% of repatriations from France), whereas only 25% of individuals >65 years were repatriated from other countries.
Most patients from France and Italy had sustained an injury (n = 32, 60% and n = 34, 57%, respectively), whereas most patients from Spain suffered from illnesses or surgical pathologies (n = 34, 67%).
The Swiss Air Ambulance “Rega-Jet” transported 169 (45%) patients and 97 (26%) patients were repatriated by ground ambulance. Almost one tenth (n = 34, 9%) were brought back to Switzerland by a scheduled flight with medical assistance. Another 32 (9%) patients were repatriated independently on scheduled flights. Two patients (0.5%) who were injured near the Swiss boarder were repatriated by HEMS. For 31 patients (8%), the type of repatriation was unknown (table 4).
For repatriations from Africa trauma was slightly more frequent (55%, n = 18) than illnesses, whereas for America illnesses were distinctly more frequent (n = 21, 70%) with only medical repatriations (n = 5) from the USA. For other countries illnesses and trauma were equally distributed.
Trauma mechanisms were road traffic accidents (n = 63, 35%), falls (n = 59, 32%), sport accidents (n = 50, 27%), the Indian Ocean tsunami 2004 (n = 5, 3%), violence (n = 1, 0.5%) and others (n = 3, 2%). For one patient there was no data on trauma mechanism. Injured patients had a median ISS of 8 (IQR 4–12, range 1–38). As illustrated in table 5, the largest group were patients suffering from illnesses affecting the nervous system (n = 73, 38%), including cerebrovascular insult (transient ischaemic attack and stroke, n = 32, 17%), others (n = 20, 11%), tumours (n = 13, 7%), epilepsy and infections (n = 4, 2% each). The other patients suffered from conditions involving the cardiovascular system (n = 29, 15%), including 22 (12%) with an acute coronary syndrome, and conditions of the gastrointestinal system (n = 24, 13%) or respiratory system (n = 21, 11%).
Of all repatriated patients, 15 (4%) died within the first 4 weeks after they arrived at the university hospital. The majority of them were male (n = 11, 73%). Five patients (1%) died on the day of arrival. Of those patients who died, 12 (80%) suffered from medical illnesses (four with tumours, three with infections, two with acute coronary syndrome, two with cerebrovascular insult and one with illness of the respiratory system). Two patients had suffered trauma and one patient died after laparotomy of a metastatic tumour.
Regarding age and occupation, the largest group were pensioners (n = 10, 67%). Nine of the ten of them were older than 65 years (90%). Ten of the 15 patients (67%), who died within 28 days, were repatriated from Europe (five France, two Italy, one Germany, one Spain, and one Albania). The other five travelled from Africa (n = 2), Asia (n = 2) and the USA (n = 1).
| Table 3:Continents and countries from which patients were repatriated. | ||||||
| All | Injuries | Illnesses | ||||
| Country of repatriation | n = 372 | (100%) | n = 182 | (100%) | n = 190 | (100%) |
| Europe | 270 | (72.6%) | 134 | (73.6%) | 136 | (71.6%) |
| Italy | 60 | (16.1%) | 34 | (18.7%) | 26 | (13.7%) |
| France | 53 | (14.2%) | 32 | (17.6%) | 21 | (11.1%) |
| Spain | 51 | (13.7%) | 17 | (9.3%) | 34 | (17.9%) |
| Asia | 33 | (8.9%) | 17 | (9.3%) | 16 | (8.4%) |
| Thailand | 15 | (4.0%) | 9 | (5.0%) | 6 | (3.2%) |
| Philippines | 4 | (1.1%) | 0 | (0.0%) | 4 | (2.1%) |
| India | 3 | (0.8%) | 1 | (0.5%) | 2 | (1.1%) |
| America | 30 | (8.1%) | 9 | (4.9%) | 21 | (11.1%) |
| Dominican Republic | 6 | (1.6%) | 3 | (1.6%) | 3 | (1.6%) |
| USA | 5 | (1.3%) | 0 | (0.0%) | 5 | (2.6%) |
| Brasilia | 4 | (1.1%) | 2 | (1.1%) | 2 | (1.1%) |
| Africa | 33 | (8.9%) | 18 | (9.9%) | 15 | (7.9%) |
| Egypt | 10 | (2.7%) | 4 | (2.2%) | 6 | (3.2%) |
| Kenya | 5 | (1.3%) | 4 | (2.2%) | 1 | (0.5%) |
| South Africa | 2 | (0.5%) | 1 | (0.5%) | 1 | (0.5%) |
| Oceania | 2 | (0.5%) | 1 | (0.5%) | 1 | (0.5%) |
| Australia | 1 | (0.3%) | 1 | (0.5%) | 0 | (0.0%) |
| French Polynesia | 1 | (0.3%) | 0 | (0.0%) | 1 | (0.5%) |
| Unknown | 4 | (1.1%) | 3 | (1.6%) | 1 | (0.5%) |
| Table 4:Means of transport of repatriated patients. | ||||||
| All | Injuries | Illnesses | ||||
| Means of repatriation | n = 372 | (100%) | n = 182 | (100%) | n = 190 | (100%) |
| Rega Jet* | 169 | (45.4%) | 77 | (42.3%) | 92 | (48.4%) |
| Rega Helicopter¶ | 1 | (0.3%) | 1 | (0.5%) | 0 | (0.0%) |
| Scheduled flight | 34 | (9.1%) | 12 | (6.6%) | 22 | (11.6%) |
| Ground ambulance | 97 | (26.1%) | 53 | (29.1%) | 44 | (23.2%) |
| On their own | 32 | (8.6%) | 21 | (11.5%) | 11 | (5.78%) |
| Other | 7 | (1.9%) | 5 | (2.7%) | 2 | (1.1%) |
| Air Zermatt Helicopter¶ | 1 | (0.3%) | 1 | (0.5%) | 0 | (0.0%) |
| Unknown | 31 | (8.3%) | 12 | (6.6%) | 19 | (10.0%) |
| * Swiss Air Ambulance ¶ Swiss Helicopter Emergency Services (HEMS) | ||||||
| Table 5: Diagnostic groups of patients with illnesses. | ||
| Diagnostic groups | n = 190 | (100%) |
| Nervous system: cerebrovascular insult | 32 | (16.8%) |
| Nervous system: infections | 4 | (2.1%) |
| Nervous system: epilepsy | 4 | (2.1%) |
| Nervous system: tumors | 13 | (6.8%) |
| Nervous system: other | 20 | (10.5%) |
| Psychiatry | 1 | (0.5%) |
| Endocrinology | 2 | (1.1%) |
| Cardiovascular system: myocardial infarction | 18 | (9.5%) |
| Cardiovascular system: angina pectoris | 4 | (2.1%) |
| Cardiovascular system: other | 7 | (3.7%) |
| Respiratory system | 21 | (11.1%) |
| Gastrointestinal system (including liver) | 24 | (12.6%) |
| Haematological system | 2 | (1.1%) |
| Kidneys and urinary tract | 9 | (4.7%) |
| Infections | 7 | (3.7%) |
| Musculosceletal system | 5 | (2.6%) |
| Eyes, ears and nose | 3 | (1.6%) |
| Dermatology | 4 | (2.1%) |
| Other and unknown | 10 | (5.3%) |
Of 372 repatriated patients, 249 (67%) were male and 182 (49%) had suffered an injury. Whereas the average age was 56 years, the group with injuries was younger (48 years). Most patients were Swiss nationals (n = 320, 86%), pensioners and handicapped pension recipients (n = 147, 40%) and were repatriated from European countries (n = 270, 73%) – especially from Italy (n = 60, 16%), France (n = 53, 14%) and Spain (n = 51, 14%). Over the study period, the number of repatriated patients increased. In comparison, the number of trips of Swiss citizens abroad remained almost constant between 10.2 million in 1998 to 9.8 million in 2005 and 10 million in the year 2011 [10]. A Swiss Air Ambulance jet repatriated almost half of all patients (n = 169, 45%). A quarter (n = 97, 26%) were transported by ground ambulance. The median ISS of injured patients was 8, with a range from 1 to 38. For repatriations from Africa, trauma was slightly more frequent than illnesses. The main reasons for repatriations from America were illnesses, whereas for other countries illnesses and trauma were almost equally distributed. The overall 28-day mortality was 4% (n = 15).
Our study covers repatriations to one of the largest university hospitals in Switzerland. However, this is a limitation on a global or national view. As a result of a lack of travel data per country over the study years, the results are not adjusted to the numbers of the travelling population in general. It might well be that the number of repatriations calculated per trip abroad is in fact decreasing (i.e. because ofbetter pretravel advice), whereas the total number of repatriations is increasing. Due to the retrospective nature of the study, some data were inevitably missing. To address missing data, we completed our data with the records from the Swiss Air Rescue Rega, which was in charge of the majority of repatriations. A major strength of our study is that it relies on the definitive discharge diagnosis of patients from the university hospital and not on initial assumptions and/or incomplete diagnostic testing. The system of a 24-hour air ambulance repatriation service is unique to Switzerland. Therefore, our study might provide important information for other countries, which are in the process of establishing a repatriation system.
In our study, we found that 40% of patients (n = 147) were pensioners or handicapped pension recipients, mainly from European countries (73%). At present, only sparse literature exists on repatriations and their characteristics. Wilde et al showed that an increasing number of elderly patients with pre-existing diseases travel to remote locations and countries [2]. There are no data on whether the number of repatriations in this group (>65 years) is increasing, especially from outside Europe. Similarly to Kramer et al, we found that the number of air ambulance repatriations increased over the years, from 21 in 2000 to 41 in 2011 [3]. Teichman et al. list medical conditions that may require medical evacuation as an appendix to the Air Medical Physician Handbook. They state that the main medical problems are acute coronary syndromes, infectious diseases and complications of pregnancy [7]. In our study, we also found that acute coronary syndrome was one of the main medical reasons. This corresponds to the findings that acute coronary syndrome is – at 3% – one of the most frequently diagnosed diseases in Swiss emergency departments, especially for patients aged between 50 and 64 years [9]. Most of our main diagnoses were in the group of acute cardiac, neurological, vascular or surgical emergencies requiring time-sensitive intervention.
Whereas the number of trips abroad by Swiss citizens seemed to vary over the years, repatriations have increased, although we present crude estimates only, not adjusted by the total population. Reasons for the increase might be an increasing gap between the healthcare status abroad compared with Switzerland, an increased demand for high standard healthcare or the fear of inadequate treatment or hospital-acquired infections abroad. Another explanation might be that, especially elderly people, tend to spend much of their time in close European countries (may also be their country of origin before becoming a Swiss citizen) but, in the event of an accident or illness, prefer to be repatriated to Switzerland for medical treatment. However, we have to keep in mind that the number of trips refers to the whole country and not only the catchment area of the hospital [9].
As in other countries, in Switzerland the number of travellers is increasing (20.3 million travellers in 2012) [10]. Travelling primarily takes place within the home country (36%) and Europe (56%), especially to neighbouring countries, such as Germany, Italy and France.
In contrast to the frequency of these destinations, only 3% of all repatriations are from Germany. We can hypothesise that the healthcare level in Germany is high enough that most travellers agree to be treated there instead of being repatriated back to Switzerland. Another explanation could be that the prevention of accidents and the hygiene level meet higher standards in Germany than in other countries, leading to fewer accidents and diseases.
A further interesting finding is that only 8% of all journeys from Switzerland are to outside Europe, although these account for one quarter of the repatriations. One explanation for this could be that patients face a lower quality of health systems in these countries and therefore need repatriation more urgently for adequate diagnostic testing and therapy. Furthermore, the time spent overseas is often longer than in a neighbouring country and the risk of injury or illness increases over time.
In our study we found a relatively high overall 28-day mortality rate of 4%. This is comparable to the mortality rate of major trauma patients admitted to a Swiss level 1 trauma centre [12]. In the current study, the majority of deaths in our repatriated patients were due to medical illnesses. A reason for the high mortality rate might be that repatriated patients represent a selected group of more severely ill or injured patients for whom standard care abroad is no longer sufficient or who do not reach a health status to allow them to travel back home by themselves after a period of treatment abroad. Moreover, these patients might suffer from additional burdens, such as nosocomial infections, complications due to less established healthcare or multidrug resistant (MDR) bacteria, aggravating the original cause [12–14]. Furthermore, the majority are elderly patients who have an increased mortality rate due to their age and comorbidities [15].
The present study is the first reporting epidemiological data of repatriated patients to a Swiss university hospital. The relatively high mortality rate of 4% underlines the importance of thoughtful clinical evaluation of these patients – in the country of origin and on admission to the home hospital. Owing to the heterogeneity of patients and health care systems involved establishing a standard seems to be a difficult task for this group of patients.
Our results could serve as a template for countries that want to establish a repatriation data system to help to estimate numbers and types of patients that need repatriation.
Last but not least, patients, especially the elderly, should be made aware of the fact that illnesses and injuries can happen abroad and that early contact to a repatriation service might be helpful as mortality is highest in this group.
The majority of patients were repatriated from Italy, a country with a very high prevalence of MDR bacteria, especially Gram-negatives with carbapenemases. France and Spain are also countries with a much higher prevalence of MDR bacteria (other than those with extended spectrum beta-lactamases) than Switzerland. Thus, repatriation of patients from these countries is a risk factor for importing MDR bacteria to hospitals if these patients are hospitalised in Switzerland [12, 14]. Furthermore, patients might be exposed to nosocomial infections, mainly in middle to low income countries, not necessarily in the tropics [12].
In conclusion we can say that repatriations to our university hospital increased from 2000 to 2011. About half were due to illnesses and half due to injuries. The largest group of patients were elderly Swiss nationals repatriated from France, Italy and Spain. Repatriation of patients from these countries is a risk factor for importing MDR bacteria to hospitals if these patients are hospitalised in Switzerland.
Mortality was relatively high, at 4%, and therefore special consideration for this group of patients is needed.
1 WHO.int [homepage on the Internet] World Health Organization: International travel and health. World Health Organization, 2012. [updated 2015; cited 2015 Aug 15]. Available from: http://www.who.int/ith/en/
2 Wilde H, Roselieb M, Hanvesakul R, Phaosavasdi S, Pruksapong C. Expatriate clinics and medical evacuation companies are a growth industry worldwide. J Travel Med. 2003;10(6):315–7.
3 Kramer W, Domres B, Dürner P, Stockert K. Evaluation of repatriation parameters: an analysis of patient data of the German Air Rescue. Aviat Space Environ Med. 1996;67(9):885–9.
4 Patel D, Easmon CJ, Dow C, Snashall DC, Seed PT. Medical repatriation of British diplomats resident overseas. J Travel Med. 2000;7(2):64–9.
5 Duchateu FX, Verner L, Cha O, Corder B. Decision criteria of immediate aeromedical evacuation. J Travel Med. 2009;16(6):391–4.
6 Rega.ch [homepage on the Internet] Zuerich/Switzerland: Rega, Operations abroad [cited 2015 Aug 15]. Available from: http://www.rega.ch/de/einsatz/einsatz-ausland/einsatzarten.aspx
7 Teichman PG, Donchin Y, Kot RJ. International aeromedical evacuation. N Engl J Med. 2007;18;356(3):262–70.
8 Committee on Injury Scaling. Association for the advancement of automotive medicine (AAAM). The abbreviated injury scale 2008 revision. Des Plaines, Chicago: AAAM; 2008.
9 Schweizerische Herzstiftung, 3th ed. Bern; Oct 2008. German.
10 bfs.admin.ch [homepage on the Internet] Bern/Switzerland, Swiss Confederation, Reisen der Schweizer Wohnbevoelkerung [cited 2015 Aug 15]. Available from: http://www.bfs.admin.ch/bfs/portal/de/index/themen/10/04.html
11 Hasler RM, Srivastava D, Aghayev E, Keel MJ, Exadaktylos AK, Schnüriger B. First results from a Swiss level I trauma centre participating in the UK Trauma Audit and Research Network (TARN): prospective cohort study. Swiss Med Wkly. 2014;144:w13910
12 Ecdc.europa.eu [homepage on the Internet]. Solna/Sweden: European Centre for Disease Prevention and Control (ECDC) [updated 2015 Aug 15; cited 2015 Aug 15]. Available from: ecdc.europa.eu/en/healthtopics/antimicrobial_resistance/database/Pages/map_reports.aspx
13 WHO.int [homepage on the Internet] World Health Organization: Guidelines on public health pesticide management policy for the WHO African Region. World Health Organization, 2011. [updated 2011; cited 2015 Aug 15]. Available from: whqlibdoc.who.int/publications/2011/9789241501507_eng.pdf
14 Josseaume J1, Verner L, Brady WJ, Duchateau FX. Multidrug-resistant bacteria among patients treated in foreign hospitals: management considerations during medical repatriation. J Travel Med. 2013;20(1):22–8.
15 Duchateau FX1, Verner L, Gauss T, Brady WJ. Air medical repatriation: compassionate and palliative care consideration during transport. Air Med J. 2012;31(5):238–41.
Funding / potential competing interests: No financial support and no other potential conflict of interest relevant to this article was reported.