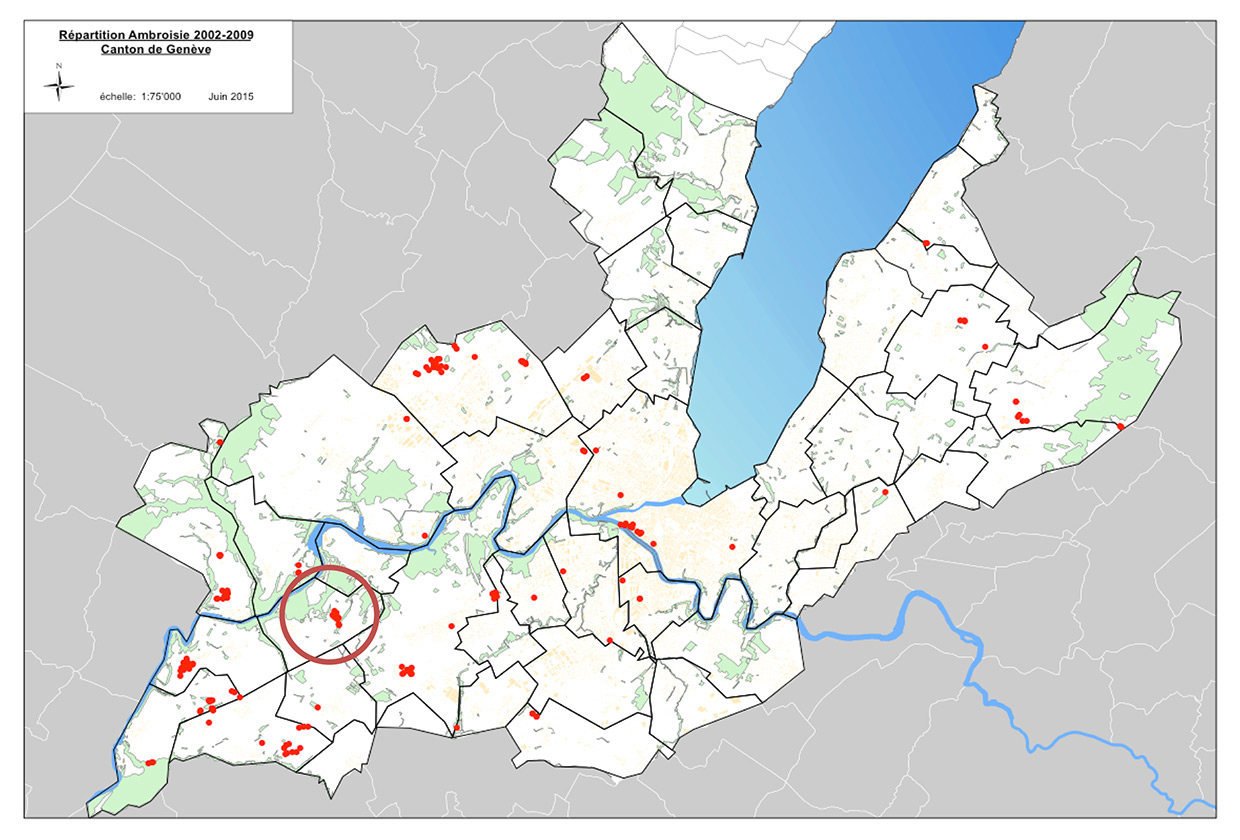
Figure 1
Ragweed invaded areas in Geneva between 2002 to 2009 (red dots). The ragweed invaded location «la Petite Grave» (red circle)
DOI: https://doi.org/10.4414/smw.2015.14198
Ambrosiabelongs to the Asteraceae family, including more than 40 species [1]. Ambrosia artemisiifolia(common ragweed) is the most widespread Ambrosia species. Ambrosia trifida(giant ragweed) is predominant in North America but is much less abundant in Europe. These two species are the main cause of health problems in the sensitive atopic population [2]. They were accidentally introduced into Europe, at the end of the 19th century, by importation of ragweed seeds, hidden in North American cereals [3].
Figure 1
Ragweed invaded areas in Geneva between 2002 to 2009 (red dots). The ragweed invaded location «la Petite Grave» (red circle)
Ragweed pollination period extends from beginning of August to mid-October. The pollen of Ambrosia artemisiifolia is produced in enormous amounts compared with other weeds and grasses and is very allergenic. Clinical manifestations are mainly rhino-conjunctivitis (87%) and asthma (42%) [3]. North America remains the main home of ragweed, where up to 50% of all cases of pollinosis are related to ragweed pollen [4]. Ragweed distribution and abundance is increasing overall in Europe in a band ranging from the Rhone valley of France to the Pannonian basin, including Hungary and also Poland, Slovakia, Bulgaria, the Czech Republic and Ukraine [5–8]. Low-grade ragweed colonisation started less than two decades ago in some areas of Switzerland, mainly in such areas as Geneva and Ticino [3]. Swiss authorities have raised concerns that sensitisations and allergies to ragweed may progress in the coming years [9]. Infested areas can change from low to heavy ragweed colonisation within a few years.
Indeed, the prevalence rate of ragweed allergies can peak at up to 12% in heavily ragweed colonised areas such as eastern France and northern Italy, where it has become a significant health threat [3, 10].
The focus of this study was to examine the prevalence rate of sensitisation and allergies to Ambrosia artemisiifolia, in the population living in the first rural Swiss setting, where ragweed was identified, in 1996. La Petite Grave is a hamlet of the commune of Cartigny located in the Geneva countryside, where field interventions have been implemented continuously since 2001 (fig. 1). The local population is therefore the ideal target group in which to evaluate whether elimination and containment strategies against ragweed are efficacious in preventing new sensitisations and allergies in the exposed population. The question is, of course, primarily health-related, but it has also a significant financial and political implications.
We recruited, in June 2009, by an open invitation by mail, 35 adults living more than 5 years in la Petite Grave, a hamlet located in the commune of Cartigny, in the canton of Geneva (fig. 2).
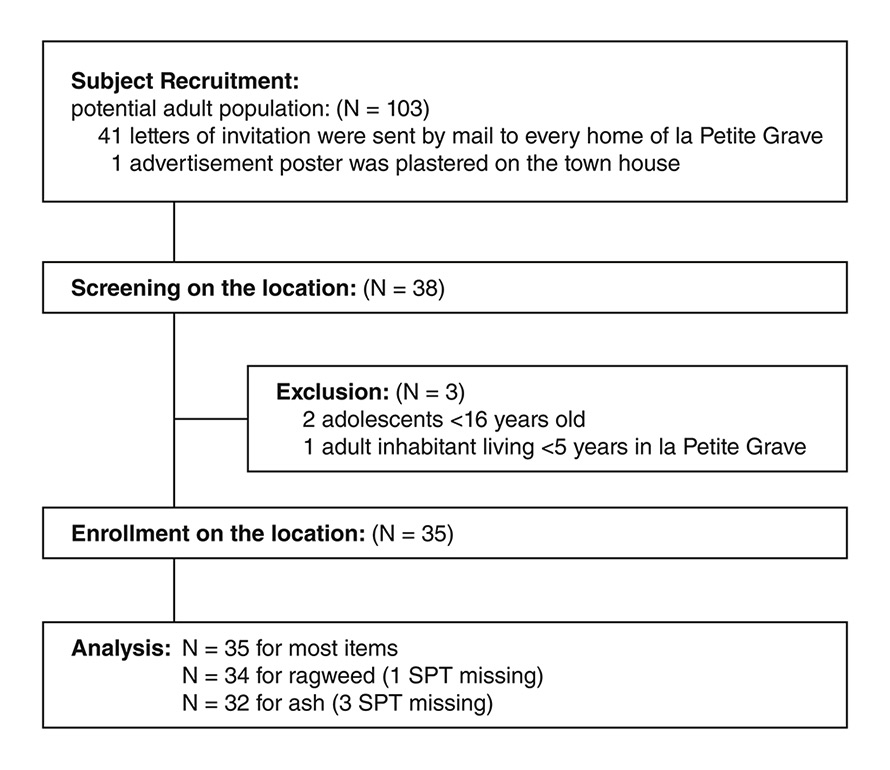
Figure 2
Flow-chart of the recruitment process.
SPT = skin-prick test
Data regarding age, gender, allergic and nonallergic rhinitis and asthma symptoms were collected by means of history-taking and on specific questionnaires such as the Allergic Rhinitis Questionnaire [11] and the Asthma Control Questionnaire [12]. We performed skin-prick tests (SPTs) with commercial, standardised extracts (ALK Abello, Wedel, Germany) [13] on every participant in order to detect sensitisation towards ragweed and common inhalant allergens such as: Betula pendula (birch), Corylus avellana (hazel), Alnus glutinosa (alder), Fraxinus excelsior (ash), grass mix, weed mix, Artemisia vulgaris (mugwort), house dust mite mix, cat and dog epithelia and mould mix. One SPT for ragweed was left out, thus changing n from 35 to 34, and three SPTs failed for ash, therefore changing n from 35 to 32 (fig. 2). All other sensitisation rates were calculated with n = 35. SPTs were performed on the flexor forearm with a standardised prick needle. Histamine dihydrochloride (10 mg/ml) was used as a positive control, and the glycerol-containing diluent was used as a negative control. Reactions were recorded after 15 minutes. Wheals with a diameter of at least 3 mm in the presence of a negative control were considered positive. All subjects consented and the study was approved by the Ethics Board for Research of the Department of Internal Medicine and Community Medicine, at the University Hospital of Geneva on 2 June 2009. The 95% confidence intervals of the proportion were assessed with the exact method of Clopper-Pearson. Statistics were calculated with the Microsoft Excel software.
| Table 1:The prevalence of allergy was calculated with the 95% confidence intervals of the proportion which were assessed by the exact method of Clopper-Pearson. | ||||
| Asthma | ||||
| No | Yes | Total | ||
| Rhinitis | No | 18 (51.4%) | 0 (0.0%) | 18 (51.4%) |
| Yes | 11 (31.4%) | 6 (17.1%) | 17 (48.6) | |
| Total | 29 (82.9%) | 6 (17.1%) | 35 (100.0%) | |
During two visits in June 2009, we recruited 35 adults living for more than 5 years in la Petite Grave. Men represented 45.7% (95% CI 30.4–61.8) of the sample (n = 16) with a mean age of 49.5 years and women 54.3% (95% CI 38.1–69.5; n = 19) with a mean age of 51 years.
We investigated rhinitis and asthma using specific questionnaires. We found that 48.6% (95% CI 32.9–64.4) had rhinitis (n = 17/35) and that 17.1% (95% CI 8.1–32.6) had asthma (N = 6/35) (table 1).
We also looked for allergy and found that 48.6% of subject had rhinitis and/or asthma.
Ragweed allergy represented 2.9% (95% CI 0.1–14.9; n = 1/34), as well as mugwort (95% CI 0.1–14.9; n = 1/35) (table 2).
Ragweed sensitisation represented 2.9% (95% CI 0.7–19.7; n = 1/34). Mugwort was measured at 2.9% (95% CI 0.1–14.9; n = 1/35). Alder was calculated at 17.1% (95% CI 6.6–33.6; n = 6/35). Hazel and birch were both evaluated at 20% (95% CI 8.4–36.9; n = 7/35). Ash was quantified at 12.5% (95% CI 3.5–29.0; n = 4/32). Grass sensitisation peaked at 22.9% (95% CI 10.4–40.1; n = 8/35). Atopy, which was defined as at least one positive prick test, was found in 26.4% (95% CI 12.9–44.4) of the sample (n = 9/34) (table 3).
| Table 2:Theprevalence of allergy to ragweed was calculated with the 95% confidence intervals of the proportion which were assessed by the exact method of Clopper-Pearson. The variable symptoms was defined positive if rhinitis = yes OR asthma = yes. | ||||
| Ragweed | ||||
| No | Yes | Total | ||
| Symptoms | No | 18 (51.4%) | 0 (0.0%) | 18 (51.4%) |
| Yes | 16 (45.7%) | 1 (2.9%) | 17 (48.6) | |
| Total | 34 (97.1%) | 1 (2.9%) | 35 (100.0%) | |
| Table 3:The prevalence of sensitisation to ragweed and mugwort was calculated with the 95% confidence intervals of the proportion which were assessed by the exact method of Clopper-Pearson. One missing value for ragweed. | ||||
| Mugwort | ||||
| No | Yes | Total | ||
| Ragweed | No | 32 (94.1%) | 0 (0.0%) | 32 (94.1%) |
| Yes | 1 (2.9%) | 1 (2.9%) | 2 (5.9) | |
| Total | 33 (97.1%) | 1 (2.9%) | 34 (100.0%) | |
The ragweed invasion of continental Europe has been the focus of several publications [14–19]. A common finding of most reports is that areas can change from low to heavy ragweed colonisation in only a few years, such as happened in the Po valley of northern Italy and in the Rhône channel of eastern France.
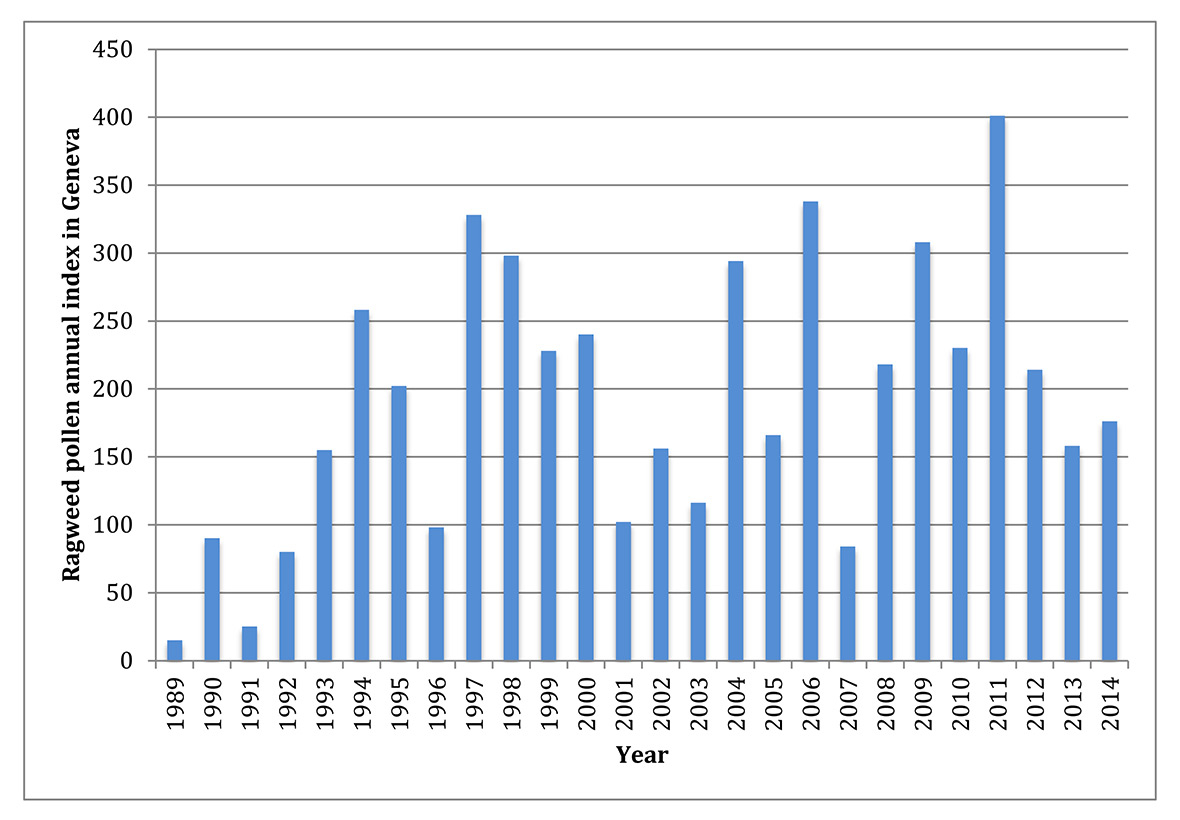
Figure 3
Ragweed annual pollen counts over 20 years in Geneva (source: MétéoSuisse).
A growing concern also arose in Switzerland at the time of discovery of the first areas of ragweed colonisation, mainly in Geneva and Ticino [20].
In a previous review published in 2005, we alerted about the risk of ragweed progression in Geneva and Switzerland, despite the fact that the ragweed invasion was still at an early stage of spread. We emphasised, that early intervention may prevent further colonisation, at a lower cost, and that this window of opportunity should not be missed [3].
Indeed, the growing concern of the environmental and health threats of common ragweed has generated, in our country, a concerted action against this species [21]. Geneva allergists monitored new clinical cases and others have measured trends of increase in locally produced Ambrosia artemisiifolia pollen loads over the years [22] (fig. 3). A research programme about various strategies for fighting ragweed was started by the Federal Station of Agronomical Research of Changin in several fields in Geneva. It concerned mainly the use of herbicides and successive cutting [23–24]. Local authorities, such as those of the commune of Cartigny, where the hamlet la Petite Grave is located, have implemented early field intervention since 2001, by systematically pulling out all plants, where possible (eradication), and by early successive cutting (containment).
Our field study, although based on a small population, surprisingly found very low incidences of ragweed sensitisation and allergy at 2.9% and 2.9%, respectively, 13 years after the discovery of the first ragweed infested area in Geneva and Switzerland.
On the basis of these results, the feared rise in ragweed sensitisation and allergy seem not, or not yet, to have occurred, as has been the case in France, Italy and Hungary over the past 20 years.
Our results are consistent with those of the large population-based SAPALDIA study, which compared 4 774 patients who provided blood samples for specific IgE to ragweed measurements in 1991 and in 2002 [25]. Singularly, in contrast to the situation in all neighbouring countries, the sensitisation rate to ragweed did not change over 11 years. Investigators also pooled and compared serum from 1 091 subjects from Geneva and Ticino, which are the two areas with the highest pollen load in Switzerland. Again, the sensitisation rates were low in 1991 and had even diminished in 2002, from 1.9% to 1.3%, respectively [25].
The results from our small clinical study are of importance for ragweed management and allergy prevention, despite the small number of subjects involved. We have detected only one subject allergic to ragweed in the setting first colonised by ragweed of Switzerland, 13 years after the discovery of this new infestation in Geneva, at la Petite Grave.
We provide indirect new evidence that early and coordinated intervention on this invasive weed, by eradication and containment, is an effective means to protect the population against new sensitisations and allergies to ragweed. This is the first acknowledgement, in 70 years, that a concerted and repeated fight against ragweed can be successful. Indeed, the previous successful ragweed eradication campaign took place in Gaspesia, a province of Quebec in 1938 [26]. The similarity between these two successful campaigns, namely the still ongoing Geneva campaign and the historical Gaspesia campaign is the use of effective manpower, which allowed systematic uprooting of ragweed plants. Indeed, the uprooting of this weed, year after year, is the most effective eradication measure.
Later it became more difficult to recruit large numbers of workers such as school children, scouts or even professional ragweed workers, because of the feared potential risk of developing a work-related ragweed allergy. This ethical issue, which is related to the intrinsic high allergenicity of ragweed pollen and the high pollen release rate, has limited extensive pull out campaigns all over the world. This ethical issue has recently been evaluated in a pilot study with 20 ragweed workers, who were followed up after 13.8 months of intensive contact with this invasive plant. All workers were protected with gloves and facial masks. Surprisingly, none developed sensitisation or allergy to ragweed [27].
This recent finding solves part of the ethical issue of implementing professional and voluntary workers and opens the route to further eradication campaigns, aiming at extensive and complete pull out of ragweed, in Switzerland.
Most existing anti-ragweed campaigns in neighbouring countries have been less effective, mainly because they had started too late after the initial ragweed invasion, at a time where seeds had already colonised the soil. The difference is striking when you compare Ticino in Switzerland and Lombardia in Italy. For example, in the town of Legnano, close to Milano, the sensitisation rates to ragweed have constantly increased over a period of more than 15 years, and moreover the incidence of allergy was delayed during the first years. The relatively low sensitisation rates in Lugano, compared with Legnano, can be explained by the much lower amount of ragweed pollen and also by the lower number of days with a high pollen load (more than 11 or more pollen/m3). The authors speculate that the difference may be related to the efforts implemented by the authorities in the canton of Ticino to contain the spread of ragweed. This Italian study emphasises the importance of consistent measures and strategies to prevent a further spreading of Ambrosia artemisiifolia [28].
In Geneva, concerted action started relatively quickly after the beginning of the invasion. A multidisciplinary group was launched in 2004 to organise the response to ragweed invasion. This network is now called Observatoire Genevois des Plantes Envahissantes (OGPE) [29]. The Geneva government has charged this network to elaborate the fight against invasive species, including ragweed. Its goal is to inform the State Council of Geneva and to provide the basis for political decisions, for an efficient application of the existing federal legislation: “ordonnance fédérale sur l’utilisation d’organismes dans l’environnement” (ODE).
This field study shows that currently, ragweed pollen does not appear to be an important cause of inhalant allergies in Geneva and in Switzerland. There is evidence that early field strategies against ragweed are an effective sanitary measure. Therefore, every effort should be made by the Geneva political authorities to pursue these successful campaigns repeatedly over time, in particular by allocating adequate financial support.
The strengths of this small pilot study are to provide original data estimating the prevalence of ragweed sensitisation and allergy. This study also highlights the relevance of early ragweed management in allergy prevention. Its limitation is the small sample size, in terms of statistical power. Further studies are needed to determine if repeated actions can limit the spread of ragweed and protect the population, in invaded areas.
1 Dessaint F, Chauvel B, Bretagnolle F. L’ambroisie. Chronique de l’extension d’un «polluant biologique» en France. Medecine/Sciences. 2005;21:207–9.
2 Wopfner N, Gardermaier G, Egger M, Asero R, Ebner C, Jahn-Schmied B, Ferreira F, et al. The spectrum of allergens in Ragweed and Mugwort pollen. Int Arch Allergy Immunol. 2005;138:337–46.
3 Taramarcaz P, Lambelet C, Clot B, Keimer C, Hauser C. Ragweed (Ambrosia) progression and its health risks: will Switzerland resist the invasion? Swiss Med Wkly. 2005;135:538–48.
4 Frenz DA. Volumetric ragweed pollen data for eight cities in the continental United States. Ann Allergy Asthma Immunol. 1999;82:41–6.
5 Kasprzyk I, Myszkowska D, Grewling L, Stach A, Skjøth CA, Smith M. The occurrence of Ambrosia pollen in Rzeszów, Kraków and Poznań, Poland: investigation of trends and possible transport of Ambrosia pollen from Ukraine. Int J Biometeorol. 2011;55(4):633–44.
6 Smith M, Cecchi L, Skjøth CA, Karrer G, Šikoparija B. Common ragweed: A threat to environmental health in Europe. Environ Int. 2013;61:115–26.
7 Burbach GC, Heinzerling LM, Röhnelt C, Bergmann K-C, Behrendt H, Zuberbier T. Ragweed sensitization in Europe – GA(2)LEN study suggests increasing prevalence. Allergy. 2009;64:664–5.
8 Peternel R, Musić Milanović S, Srnec L. Airborne ragweed (Ambrosia artemisiifolia L.) pollen content in the city of Zagreb and implications on pollen allergy. Ann Agric Environ Med. 2008;15:125–30.
9 Bundesamt für Gesundheit: Ambrosia: eine Pflanze die die Gesundheit Millionen Kostet. BAG Journal. 2005;30:528–9. German.
10 Asero R. Ragweed allergy in northern Italy: are patterns of sensitization changing? Eur Ann Allergy Clin Immunol. 2012;44:157–9.
11 International Primary Care Airways Group (IPAG) Handbook available at http://www.globalfamilydoctor.com .
12 Juniper EF, O’Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. Eur Respir J. 1999;14:902.
13 Heinzerling LM, Burbach GJ, Edenharter G, Bachert C, Bindslev-Jensen C, Bonini S, Bousquet J, et al. GA(2)LEN skin test study I: GA(2)LEN harmonization of skin prick testing: novel sensitization patterns for inhalant allergens in Europe. Allergy. 2009;64:1498–506.
14 Laaidi M, Laiidi K, Besancenot JP, Thibaudon M. Ragweed in France: an invasive plant and its allergenic pollen. Ann Allergy Asthma Immunol. 2003;91:195–201.
15 Asero R. Analysis of new respiratory allergies in patients monosensitized to airborne allergens in the area north of Milan. J Investig Allergol Clin Immunol. 2004;14:208–13.
16 Asero R. Birch and ragweed pollinosis north of Milan: a model to investigate the effects of exposure to ‘new’ airborne allergens. Allergy. 2002;57:1063–6.
17 D’Amato G, Liccardi G, D’Amato M, Cazzola M. Outdoor air pollution, climatic changes and allergic bronchial asthma. Eur Respir J. 2002;20:763–76.
18 Jäger S. Are there current trends of pollen change in Europe? EAACI Newsletter. 2006;9:15.
19 Ziska LH, Gebhard DE, Frenz DA, Faulkner S, Singer BD, Straka JG. Cities as harbingers of climate change: common ragweed, urbanization, and public health. J Allergy Clin Immunol. 2003;111:290–5.
20 Delabays N, Lambelet C, Jeanmonod D, Keimer C, Clot B. L’ambroisie à feuille d’Armoise (Ambrosia Artemesifolia), une espèce à surveiller en Suisse Revue Suisse d’Agriculture. 2002;34:1.
21 Bohren C, Mermillod G, Delabays N. Common ragweed (Ambrosia artemisiifolia L.) in Switzerland: developpement of a nationwide concerted action. Journal of Plant Diseases and Protection. 2006;XX:457–503.
22 Davet A, Clot B, Guibert S, Van Eck F, Gaudart M, Gumowski PI. Occurrence of ragweed pollen allergy and sensitization in the Geneva area from 1999 to 2004: the perspective from an allergy outpatient clinic. Swiss Med Wkly. 2007;137(Suppl 157):42.
23 Delabays N, Bohren C, Mermillod G, Keimer C, Kündig C. 2005 l’ambroisie à feuille d’Armoise (Ambrosia Artemesifolia), en Suisse: aspect malherbologiques. Revue Suisse d’Agriculture. 2005;37:17–24.
24 Delabays N, Bohren C, Mermillod G, Baker A, Vertenten J. Briser le cyle de l’ambroisie pour épuiser son stock semancier dans les sites infectés. Efficacité et optimisation des régimes de coupe. Revue suisse d’agriculture. 2008;40(3):143–9.
25 Ackermann-Liebrich U, Schindler C, Frei P, Probst-Hensch NM, Imboden M, Gemperli A, Rochat T, et al. Sensitisation to Ambrosia in Switzerland: a public health threat in waiting. Swiss Med Wkly. 2009;139:70–5.
26 Campagna E. Le problème de l’herbe à poux en Gaspésie [s.l.]
27 Brandt A, Zuberbier T, Bergmann KC. Risk of sensitization and allergy in ragweed workers – a pilot study. Allergy Asthma Clin Immunol. 2014;10:42.
28 Tosi A, Wüthrich B, Bonini M, Pietragalla-Köhler B. Time lag between Ambrosia sensitisation and Ambrosia allergy: a 20-year study (1989-2008) in Legnano, northern Italy. Swiss Med Wkly. 2011;141w13253.
29 OGPE: Lutte contre les plantes exotiques envahissantes (neophytes) et suivi de leur évolution. Stratégie et plan d’action 2012–2023. http://etat.geneve.ch
Disclosure statement:The financial support came from the Service of Allergology and Immunology at the University Hospitals of Geneva. The research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.