Figure 1
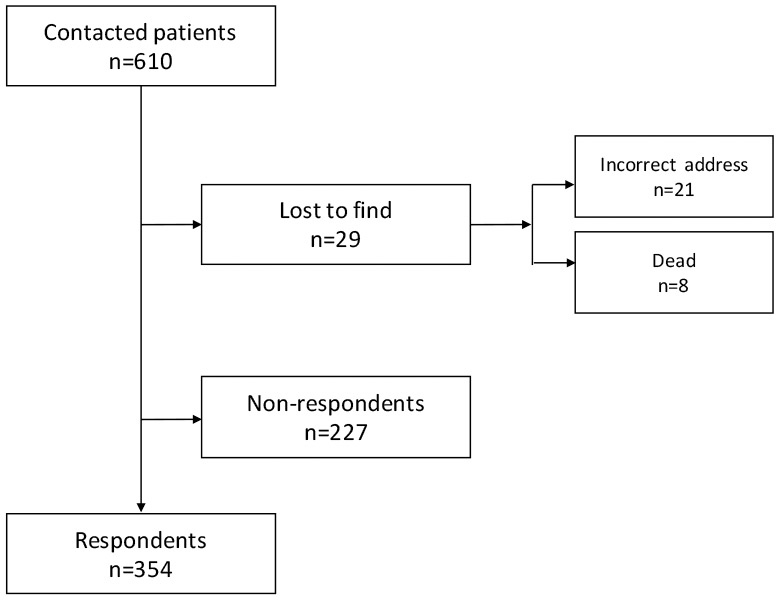
Patients' recruitment.
DOI: https://doi.org/10.4414/smw.2015.14169
Kidney transplantation is considered to be the most successful therapy for end-stage renal disease (ESRD) regarding patient survival [1, 2]. Many data are available on the medical outcome of kidney allograft recipients [3, 4]. Outcome data for all Swiss kidney allograft recipients have been collected and analysed by the Swiss Transplant Cohort Study since 2008 [4]. But the impact of transplantation on the socioeconomic status (SES), especially working ability, is less well investigated. Research on working ability after successful kidney transplantation has been conducted in different countries and the results are controversial [5–16]; for example, employment rates after successful renal transplantation are 30%–40% in the United States [5], 67% in the Netherlands [17], 40% in Finland [12], and 64.8% in Italy [15]. Overall, the rate of full- or part-time employment varies between 18% and 82% in these analyses. Patients with ESRD requiring renal replacement therapy are often considered as disabled and thus receive a partial or full disability pension [16]. At least a part of patients of working age is expected to go back to work after successful renal transplantation. Data from Switzerland regarding the change in working ability are lacking. The current study addresses socioeconomic factors and the change of working ability after successful kidney transplantation in a Swiss single centre population with a high proportion of living kidney donors. The aim of the study was, therefore, to evaluate the socioeconomic status of kidney recipients 1 year before transplantation and to compare the data with their status 1 year after successful kidney transplantation.
This study was approved by the ethics committee of north-western Switzerland. Between 1 January 2000 and 31 December 2011, a total of 745 renal transplants were performed at the University Hospital of Basel. In autumn 2013, all living kidney allograft recipients with a functioning graft for at least 1 year were contacted with a two-page questionnaire, an explanatory letter and an informed consent form. Minimal time between transplantation and the survey was 18 months. The questionnaire consisted of 12 questions and was available in German (basic version, see appendix), French and Italian languages. Translations to French and Italian were made by professional translators. Respondents gave their answers using tick boxes and wrote additional information in the provided spaces. Questions regarding health or activity perception could be answered by setting a mark on a 0 to 10 scale. Five out of the 12 questions were used for the current analysis. Question 1: education and training, applicable answers: no graduation, graduated, completed apprenticeship, higher education or university degree. Question 2: type of profession 1 year before transplantation, e.g. “workman”, “journalist”. Questions 3/4: working status 1 year before / 1 year after kidney transplantation, applicable answers: working (if “yes”: percentage of working ability), retired, disability pension (if “yes”: percentage of disability pension), unemployed, others (e.g. housework, studies). Question 5: time of transplantation, applicable answers: too early, just in time, too late. Patients who had given unclear or illegible answers were contacted by telephone to clarify and confirm the answers.
Baseline characteristics (age, gender, time/type of dialysis, number of transplantations, donor type) were extracted from the patient documentation system of the University Hospital of Basel and were collected for all contacted patients. Working ability was defined as the ability to work, full- or part-time, from the medical point of view. Unemployment was considered as being formally able to work.
Data were analysed using JMP Pro Version 11 software (SAS Institute Inc., Cary, NC). For categorical data Pearson’s chi-square or Fisher’s exact tests were used and data presented as counts and percentages. For continuous data such as age two sample t-tests were conducted and summarised as mean (±standard deviation [SD]). Univariate and multivariate logistic regression analysis was performed to demonstrate determining factors of employment as a categorical dependent variable. All significant variables in the univariate analyses as indicated in table 3 were selected as explanatory variables for the multivariable models. A two-tailed p-value of <0.05 was considered to indicate statistical significance.
Overall, 354 out of 610 patients (58%) gave their informed consent and completed the questionnaire (see fig. 1). Respondents were significantly older than nonrespondents, with mean (±SD) age at transplantation 51 (±13) vs 48 (±14) years (p = 0.0025), but did otherwise not significantly differ regarding baseline characteristics (data not shown). Baseline data of the respondents are shown in table 1.
Figure 1
Patients' recruitment.
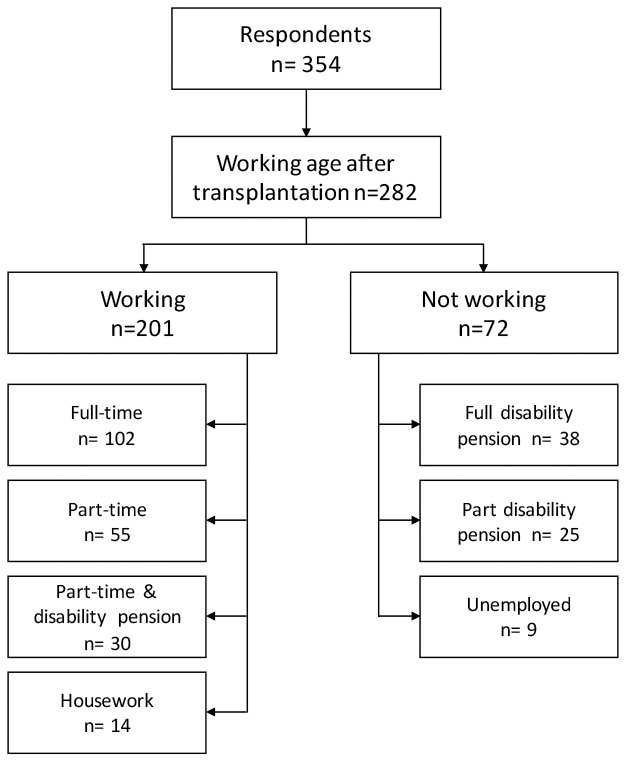
Figure 2
Working status after transplantation.
Of 282 working-age patients, 210 (74.5%) were working or able of work 1 year after transplantation as compared with 216 out of 292 patients (74%) before transplantation (p = 0.92). Table 2 provides detailed data on working status before and after transplantation.
Thirty out of 282 working-age patients (10.6%) improved their working ability after transplantation: 19 of 61 part-time working patients (27.9%) proceeded to a full-time work quota. Four of 28 patients (14.3%) with partial disability pension restarted full-time work, and seven patients (25%) restarted part-time work. No patient with a full disability pension proceeded to a 100% work quota after transplantation. Sixteen patients became dependent on a partial or full disability pension despite successful transplantation. Eight patients became unemployed. Patients who interrupted their work because of transplantation had a median time interval of 3 months (interquartile range [IQR] 2‒5 months) until re-uptake of work.
Overall, 201 out of 282 working age patients (71.3%) were working 1 year after transplantation: 102 full-time, 55 part-time, 30 part-time with an additional disability pension, and 14 had dedicated themselves to housework. Seventy-two patients (25.3%) did not work 1 year after kidney transplantation: 63 patients had a full or partial disability pension, and 9 patients were unemployed. Six patients were in training and the working status of three was unknown. Categorisation of employment after transplantation is shown in figure 2. Table 3 summarises factors with impact on working ability post-transplantation: age ≤50 years, living donor transplantation, pre-emptive transplantation, higher education, a dialysis period ≤1 year, and preserved employment before transplantation were associated with increased working ability after transplantation, whereas age above 50 years and a dialysis period >1 year showed a negative correlation. The multivariate logistic regression confirmed working status before transplantation to be the most important predictive factor (multivariate p <0.0001).
Sixty-six of the 354 patients (19%) could be transplanted pre-emptively. Of these 66, 36 (55%) were working full-time 1 year before transplantation, and 6/66 (9%) had some kind of disability pension at the time of transplantation.
A total of 304 of the 354 (86%) patients declared that transplantation was performed at the right time; 40/354 patients (11%) answered that transplantation was performed too late; 1.5% (5/354) felt that transplantation was carried out too early. Five out of 354 (1.5%) did not respond to this question.
| Table 1:Baseline data of respondents. | |
| Number (n) Percentage women | 354 31.2% |
| Age at transplantation (years) Mean (± standard deviation) | 51 (±13) |
| Dialysis before transplantation (n, %) | |
| Pre-emptive transplantation ≤12 months on dialysis >12 months on dialysis Unknown | 66 (19%) 98 (27%) 188 (53%) 2 (1%) |
| Number of transplants (%) 1 2 ≥3 | 85% 14% 1% |
| Donor type (%) Deceased donor Living donor | 46.5% 53.5% |
| Education and training (%) | |
| No graduation Graduated Apprenticeship completed Higher education or university degree Unknown | 4% 16% 64% 15% 1% |
| Table 2:Working ability before and after transplantation. | ||
| One year before transplantation | One year after transplantation | |
| All patients (n) | 354 | 354 |
| Retired (n) | 62 | 72 |
| Patients of working age, n (%) | 292 (100%) | 282 (100%) |
| Gender: female | 91 (31.2%) | 86 (29.5%) |
| Working full-time | 96 (32.9%) | 102 (36.2%) |
| Working part-time | 61 (20.9%) | 55 (19.5%) |
| Part-time working and part disability pension | 35 (11.9%) | 30 (10.6%) |
| Housework | 18 (6.2%) | 14 (5.0%) |
| Unemployed | 6 (2.1%) | 9 (3.1%) |
| In training | 10 (3.4%) | 6 (2.1%) |
| Full disability pension | 35 (11.9%) | 38 (13.5%) |
| Partial disability pension | 28 (9.6%) | 25 (9.0%) |
| Not known | 3 (1.0%) | 3 (1.0%) |
| Education / training, n (%) | 292 (100%) | 282 (100%) |
| No graduation | 12 (4.1%) | 11 (3.9%) |
| Graduated | 46 (15.8%) | 42 (14.9%) |
| Apprenticeship completed | 186 (63.7%) | 181 (64.2%) |
| Higher education or university degree | 45 (15.4%) | 45 (16%) |
| Unknown | 3 (1.0%) | 3 (1.0%) |
| Age groups, n (%) | 292 (100%) | 282 (100%) |
| <25 years | 16 (5.5%) | 16 (5.7%) |
| 26‒50 years | 135 (46.2%) | 135 (47.9%) |
| 51–65 years | 141 (48.3%) | 131 (46.4%) |
| Table 3: Factors with impact on employment after transplantation. | ||||
| Working after tx (n = 201) * | Not-working after tx (n = 72)† | p-value | Odds ratio (95% confidence interval) | |
| Gender | ||||
| Female, n (%) | 61 (30%) | 21 (29%) | 0.85 | |
| Age group, n (%) | ||||
| <25 years 26‒50 years 51‒65 years | 10 (5%) 109 (54%) 82 (41%) | 6 (8%) 23 (32%) 43 (60%) | 0.006# | 0.46 (0.27–0.80) |
| Donor Type, n (%) | ||||
| Living Deceased | 134 (67%) 67 (33%) | 21 (29%) 51 (71%) | <0.0001 | 4.86 (2.74–8.88) |
| Number of transplants, n (%) | ||||
| 1 >1 | 169 (84%) 32 (16%) | 60 (83.5%) 12 (16.5%) | 0.88 | |
| Dialysis before tx, n (%) | ||||
| No dialysis = pre-emptive ≤12 months on dialysis >12 months on dialysis Unknown | 53 (26%) 68 (34%) 80 (40%) - | 4 (6%) 11 (15%) 56 (78%) 1 (1%) | <0.0001 <0.0001 < 0.0001 | 5.95 (2.31–20.2) 4.33 (2.17–9.31) 0.23 (0.11–0.46) |
| Education and training, n (%) | ||||
| No graduation Graduated Apprenticeship completed Higher education/ university degree Unknown | 4 (2%) 20 (10%) 137 (68%) 39 (19%) 1 (1%) | 8 (11%) 22 (30.5%) 36 (50%) 4 (5.5%) 2 (3%) | 0.003§ | 4.0 (1.53–13.7) |
| Work status before tx, n (%) | ||||
| Working Not working Unknown | 181 (90%) 13 (6.5%) 7 (3.5%) | 20 (28%) 51 (71%) 1 (1%) | <0.0001 | 35.5 (17.0–79.1) |
| tx = transplantation * Working full-time (102) + part-time (55) + part-time and disability pension(30) + housework (14) † Full disability pension (38) + part disability pension (25) + unemployed (9) # Logistic regression analysis of age >50 years vs ≤50 years old patients. ¶ Logistic regression analysis of living vs deceased donors. § Logistic regression analysis of higher education vs others (patients with unknown education status were excluded). | ||||
Kidney transplantation is the medical treatment of choice for ESRD. It improves life expectancy [18] and quality of life [19, 20] as compared with dialysis. The preservation of jobs before transplantation as well as the resumption of work after successful transplantation is crucial from the economic point of view and for the self-esteem of the recipient. Data on employment rates after transplantation differ from country to country [11, 12, 21–23]. National factors such as type of healthcare system, rate of unemployment, social welfare and economic climate complicate and limit the comparison of data.
The current study provided for the first time data on the employment rate before and after successful kidney transplantation in Switzerland. Pretransplant employment (part- or full-time) of working-age patients in the current analysis was 65.7%; 21.6% of patients awaiting kidney transplantation had a full or partial disability pension. These numbers on pretransplant employment differ significantly from those in other European countries such as Finland (about 30%; [12] or Denmark (22%, [22]), and even more from the US (18.9%) [21]. We assume that the avoidance of a dialysis period by pre-emptive transplantation (about 20%) or by transplantation after a short dialysis duration (about 25%) is mainly responsible for the preservation of employment before transplantation in the analysed population. Our data and data from others [10, 23] show that a preserved pretransplant employment status is crucial for the post-transplant working status. The avoidance or shortening of dialysis duration is mainly achieved by the high number of living donors (>50%) in this analysis and not by a sufficient rate of deceased donors in Switzerland [24]. Therefore, early planning of living donor transplantation is crucial to avoid time on dialysis, and to preserve employment. This interpretation is in line with the patient’s statement in nearly 90% (question 5) that the transplantation was performed at the right time. A high educational and training status of the analysed population might have also favoured the positive outcome [25, 26].
Seventy-one percent of working age patients in this analysis were fully or part-time working 1 year after transplantation. This number is higher than most reported rates in the literature [12, 23, 27]. Ten percent of patients could improve their employment status after a successful kidney transplant, not a big increase at first glance. But it has to be taken into account that the rate of employment before transplantation in the current analysis (65.7%) was already as high as many reported post-transplant rates in other countries [12, 23, 27]. Nevertheless, a careful evaluation of disability pensions after successful kidney transplantation might further improve the number of patients able to work. But it remains doubtful whether overall the rate of employment can further be increased as the employability of chronically ill patients is difficult [5, 7–10].
This study has several limitations. First, it is a retrospective analysis. Second, the respondents’ rate was 58%, and nonrespondents were slightly, but significantly younger than respondents, leading to the assumption that younger, working patients were reluctant to participate. Third, results relied upon the respondents’ accuracy and honesty in their answers. Furthermore, the study format poses the question about recall bias ‒ some patients were >11 years post-transplant at the time of the survey ‒ but usually patients remember well their working ability and their disability pension. In addition, unmeasured factors may have had an additional impact on the results and the questionnaire has not been validated.
In conclusion, the employment rate in this Swiss cohort before and after successful kidney transplantation is high as compared with the literature. A high number of living donors, of pre-emptive transplantations, and short dialysis duration may contribute to this observation.
> Download PDF file http://www.smw.ch/fileadmin/smw/pdf/SMW-14169-Appendix.pdf
Acknowledgements:The authors express their special thanks to Glena Iten, MA in Psychology, for the reviewing and standardising of the questionnaire, to Catherine Hänlin and Cathrine Wohlhüter for the French translation, and to Serenella Eppenberger, PhD, for the Italian translation. Also the authors express their thanks to Margrit Bucher and Heike Markus for the assistance in collecting the questionnaires.
1 Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341(23):1725–30.
2 Schnuelle P, Lorenz D, Trede M, Van Der Woude FJ. Impact of renal cadaveric transplantation on survival in end-stage renal failure: evidence for reduced mortality risk compared with hemodialysis during long-term follow-up. J Am Soc Nephrol. 1998;9(11):2135–41.
3 Collaborative Transplant Study (CTS) 2015 Feb 1. http://www.ctstransplant.org
4 Swiss Transplant Cohort Study (STCS) 2015 Apr 9. http://www.stcs.ch
5 McGee J, Jackson NR, Slakey DP. Disability and kidney transplantation in the United States. Clin Transplant. 2012;26(3):377–81.
6 Petersen E, Baird BC, Barenbaum LL, Leviatov A, Koford JK, Shihab F, et al. The impact of employment status on recipient and renal allograft survival. Clin Transplant. 2008;22(4):428–38.
7 Raiz L, Monroe J. Employment post-transplant: a biopsychosocial analysis. Soc Work Health Care. 2007;45(3):19–37.
8 Sangalli V, Dukes J, Doppalapudi SB, Costa G, Neri L. Work Ability and Labor Supply after Kidney Transplantation. Am J Nephrol. 2014;40(4):353–61.
9 Slakey DP, Rosner M. Disability following kidney transplantation: the link to medication coverage. Clin Transplant. 2007;21(2):224–8.
10 Tzvetanov I, D’Amico G, Walczak D, Jeon H, Garcia-Roca R, Oberholzer J, Benedetti E. High rate of unemployment after kidney transplantation: analysis of the United network for organ sharing database. Transplant Proc. 2014;46(5):1290–4.
11 van der Mei SF, Kuiper D, Groothoff JW, van den Heuvel WJ, van Son WJ, Brouwer S. Long-term health and work outcomes of renal transplantation and patterns of work status during the end-stage renal disease trajectory. J Occup Rehabil. 2011;21(3):325–34.
12 Helantera I, Haapio M, Koskinen P, Gronhagen-Riska C, Finne P. Employment of patients receiving maintenance dialysis and after kidney transplant: a cross-sectional study from Finland. Am J Kidney Dis. 2012;59(5):700–6.
13 Aitken E, Dempster N, Ceresa C, Daly C, Kingsmore D. The impact of socioeconomic deprivation on outcomes following renal transplantation in the West of Scotland. Transplant Proc. 2013;45(6):2176–83.
14 Axelrod DA, Dzebisashvili N, Schnitzler MA, Salvalaggio PR, Segev DL, Gentry SE, et al. The interplay of socioeconomic status, distance to center, and interdonor service area travel on kidney transplant access and outcomes. Clin J Am Soc Nephrol. 2010;5(12):2276–88.
15 Mistretta A, Veroux M, Grosso G, Contarino F, Biondi M, Giuffrida G, et al. Role of socioeconomic conditions on outcome in kidney transplant recipients. Transplant Proc. 2009;41(4):1162–7.
16 IV – Leistungsarten – IV-Renten [Internet]. [cited 2014 Mar 25]. Available from: http://www.svash.ch/site/index.cfm?id_art=11470&actMenuItemID=6616&vsprache/DE/V___Leistungsarten___IV_Rent.cfm.[electronic mail system]. 2014 May.
17 van der Mei SF, Kuiper D, Groothoff JW, van den Heuvel WJ, van Son WJ, Brouwer S. Long-term health and work outcomes of renal transplantation and patterns of work status during the end-stage renal disease trajectory. J Occup Rehabil. 2011;21(3):325–34.
18 Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341(23):1725–30.
19 Jofre R, Lopez-Gomez JM, Moreno F, Sanz-Guajardo D, Valderrabano F. Changes in quality of life after renal transplantation. Am J Kidney Dis. 1998;32(1):93–100.
20 Czyzewski L, Sanko-Resmer J, Wyzgal J, Kurowski A. Assessment of health-related quality of life of patients after kidney transplantation in comparison with hemodialysis and peritoneal dialysis. Ann Transplant. 2014;19:576–85.
21 Kutner N, Bowles T, Zhang R, Huang Y, Pastan S. Dialysis facility characteristics and variation in employment rates: a national study. Clin J Am Soc Nephrol. 2008;3(1):111–6.
22 Molsted S, Aadahl M, Schou L, Eidemak I. Self-rated health and employment status in chronic haemodialysis patients. Scand J Urol Nephrol. 2004;38(2):174–8.
23 van der Mei SF, Krol B, van Son WJ, de Jong PE, Groothoff JW, van den Heuvel WJ. Social participation and employment status after kidney transplantation: a systematic review. Qual Life Res. 2006;15(6):979–94.
24 Organ Donation and Transplantation activity in Switzerland Preliminary statistics 2013 Swisstransplant. 2015 Jan 7.
25 Feinstein JS. The relationship between socioeconomic status and health: a review of the literature. Milbank Q. 1993;71(2):279–322.
26 Marmot M, Feeney A. General explanations for social inequalities in health. IARC Sci Publ. 1997;(138):207–28.
27 Messias AA, Reichelt AJ, dos Santos EF, Albuquerque GC, Kramer JSP, Hirakata VN, Garcia VD. Return to Work After Renal Transplantation: A Study of the Brazilian Public Social Security System. Transplantation. 2014;98(11).
Disclosures: The study was supported by a grant from Novartis AG. The authors of this manuscript have no potential competing interests to disclose as described by the Journal of Swiss Medical Weekly.