Time-trends in assisted and unassisted suicides completed with different methods: Swiss National Cohort
DOI: https://doi.org/10.4414/smw.2015.14153
Nicole
Steck, Marcel
Zwahlen, Matthias
Egger
Summary
OBJECTIVE: The number of suicides assisted by right-to-die associations has increased in recent years in Switzerland. The aim of our study was to compare time trends in rates of assisted and unassisted suicide from 1991–2008.
METHODS: The Swiss National Cohort is a longitudinal study of mortality in the Swiss population; based on linkage of census data with mortality records up to 2008. The Federal Statistical Office coded suspected assisted suicides from 1998 onwards; and from 2003 onwards right-to-die associations reported the suicides they assisted. We used Poisson regression to analyse trends in rates of suicide per 100'000 person-years, by gender and age groups (15–34, 35–64, 65–94 years).
RESULTS: A total of 7'940'297 individuals and 24'842 suicides were included. In women, rates changed little in the younger age groups but increased in 65–94-year-olds, due to an increase in suicide by poisoning (from 5.1 to 17.2 per 100'000; p <0.001). An increase in suicides by poisoning was also observed in older men (from 8.6 to 18.2; p<0.001). Most suicides by poisoning were assisted. In men, suicide rates declined in all age groups, driven by declines in suicide with firearms.
CONCLUSIONS: Research is needed to gain a better understanding of the reasons for the tripling of assisted suicide rates in older women, and the doubling of rates in older men, of attitudes and vulnerabilities of those choosing assisted suicide, and of access to palliative care. Rates of assisted suicide should be monitored; including data on patient characteristics and underlying comorbidities.
Introduction
In Switzerland suicide is an important public health issue: over 1'300 out of about 60'000 deaths each year are by suicide [1, 2]. With an age-standardised rate of 9.2 per 100'000 in 2012, suicide is more common in Switzerland than in other European countries, for example Italy (5.0 per 100'000) or the United Kingdom (6.2 per 100'000) [3]. About two-thirds of suicides are in men who frequently use violent methods such as firearms and hanging, whereas poisoning is more common in women [4].
Euthanasia is prohibited in Switzerland but assistance in suicide is legal if no selfish interests are involved [5]. The number of suicides assisted by right-to-die associations has increased substantially in recent years [6–8]. For example, in 2014 the organization Exit assisted 583 suicides in the German-speaking part of Switzerland, 124 more than in 2013 [9].
There is no legal obligation to report assisted suicides to the Federal Office of Statistics, and previous analyses of trends in suicide mortality in Switzerland could therefore not distinguish between assisted and unassisted suicides [2, 10]. In 1998 the Federal Office of Statistics introduced specific codes for deaths suspected to be assisted suicides [11]. More recently, within the framework of a research project of the Swiss National Cohort [6], the three right-to-die organizations assisting Swiss residents in suicide, reported the suicides they assisted between 2003 to 2008 to the Federal Office: Exit Deutsche Schweiz, Exit Suisse Romande and Dignitas.
We analysed these data to study trends in assisted and unassisted suicides completed by different methods.
Methods
The Swiss National Cohort
Described in detail elsewhere [12, 13], the Swiss National Cohort (SNC) is a longitudinal study of mortality in Switzerland based on linkage of census and mortality records. The records of the 1990 and 2000 censuses were linked to a death or emigration record up to 2008 using deterministic and probabilistic linkage procedures, based on gender, date of birth, place of residence and other variables. The SNC was approved by the Cantonal Ethics Committees of Bern and Zurich, with approval covering the present study.
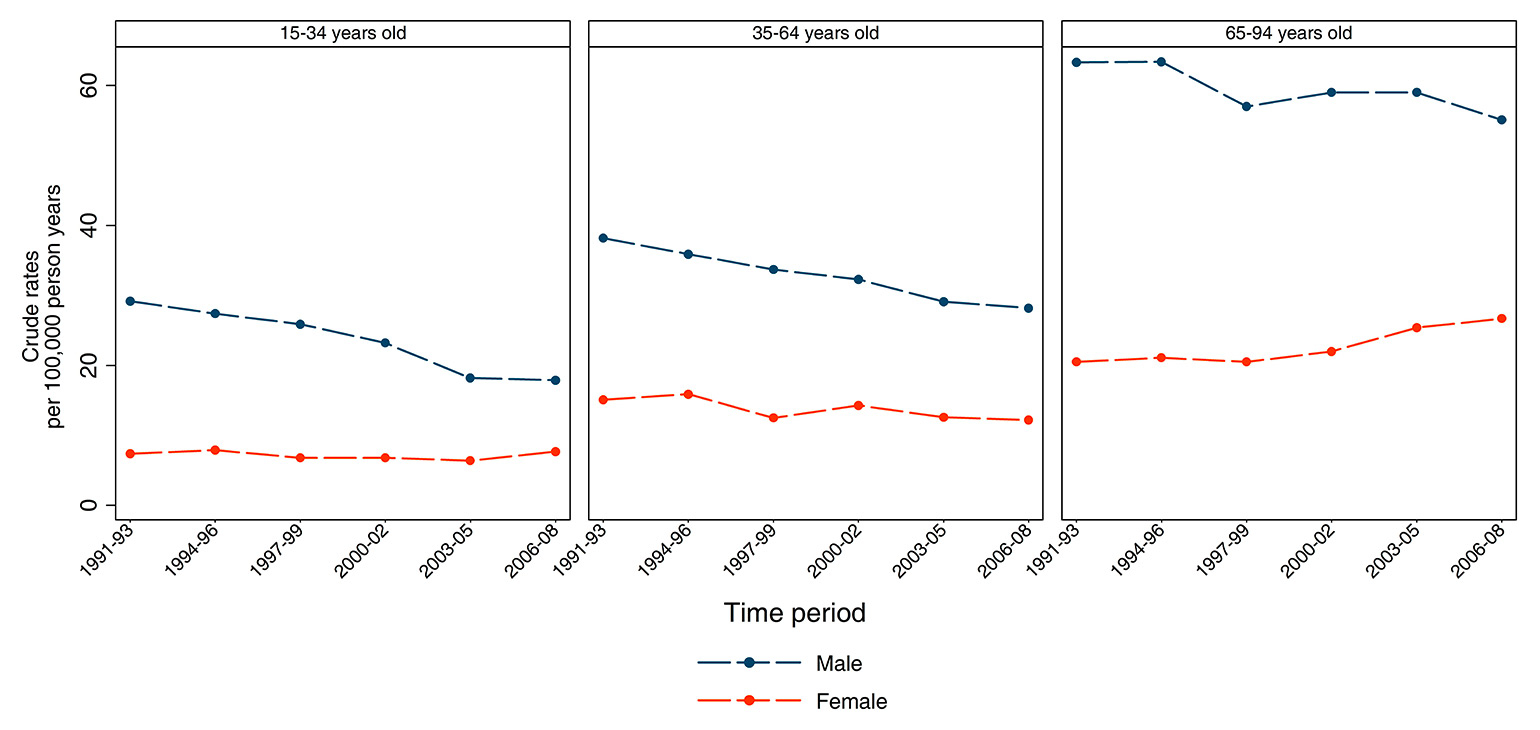
Figure 1
Time-trends of suicide rates in Switzerland by age group and sex, 1991–2008. In men there was a decline in all age groups (all p <0.001); in women there was no change over time in the youngest age group (p = 0.40); a slight decline in the age group 35–64 years and an increase in the oldest age group (both p <0.001).
Ascertainment of assisted and unassisted suicides
Suicides were identified from the causes of death recorded on the death certificate. From 1991 to 1994 deaths were coded according to the International Classification of Diseases, Eighth Revision (ICD-8). We used codes E950 to E958, which denote deaths by intentional self-harm. Since 1995 deaths have been coded on the basis of the Tenth Revision (ICD-10) and we used codes X60.0 to X84.0. We created six categories for the most common methods of suicide: (i) poisoning (ICD-8 E950-952 or ICD-10 X60-X69); (ii) hanging (ICD-8: E953 or ICD-10: X70, including strangulation and suffocation); (iii) firearms (ICD-8 955 or ICD-10 X72-X74, including all suicides by discharge of handguns, shotguns, larger or unspecified firearms); (iv) jumping from a high place (ICD-8 957 or ICD-10 X80); (v) suicide by train (ICD-8 E958.00, ICD-10 X81, including jumping or lying before moving object) and (vi) other means of suicide.
From 1998 onwards the Federal Statistical Office coded deaths from suspected assisted suicide using code 61.8 if assisted suicide or a right-to-die organisation was mentioned on the death certificate. Code 61.9 was used if poisoning with pentobarbital sodium was recorded as the cause of death; this is the drug used by the right-to-die organisations. We analysed suicides coded as 61.8 or 61.9 from 1998 onwards. For the time period 2003 to 2008 the three right-to-die associations Exit Deutsche Schweiz, Exit Suisse Romande and Dignitas reported all their assisted suicides to the Federal Statistical Office, within the framework of a research project funded by the Swiss National Science Foundation [6]. For this period we also analysed the assisted suicides reported by these organisations.
Statistical analysis
We calculated rates of assisted and unassisted suicides, and of unassisted suicides completed by different methods, by dividing the number of suicides by the number of person-years at risk. We stratified analyses by gender and three age groups (15–34 years, 35–64 years and 65–94 years). For each method of suicide we calculated rates per 100'000 person-years by gender, the three age groups and six calendar periods (1991–93, 1994–96, 1997–99, 2000–02, 2003–05, 2006–08). We used Poisson regression with calendar year as the independent variable to calculate rate ratios per year with 95% confidence intervals (CIs) and p-values. Statistical analyses were done in Stata version 12 (Stata Corporation, College Station, TX, USA). Results are given as rates per 100'000 population and rate ratios per year (relative annual change in rate), with 95% CIs.
|
Table 1:Study population; person-years at risk and number of suicides by different methods by age and gender; Switzerland 1991–2008. |
|
|
Age at baseline (years)
|
|
14‒34
|
35‒64
|
65‒94
|
|
Study population
|
|
|
|
| Men |
2'080'828 |
1'431'308 |
403'405 |
| Women |
1'985'773 |
1'423'513 |
615'470 |
|
Person-years at risk
|
|
|
|
| Men |
17'031'381 |
26'266'425 |
8'101'880 |
| Women |
16'221'880 |
26'054'470 |
11'725'183 |
|
Number of suicides
|
|
|
|
| Men |
|
|
|
| Poisoning* |
451 |
1'283 |
1'069 |
| Firearms |
1'600 |
2'875 |
1'458 |
| Hanging |
967 |
2'521 |
1'161 |
| Jumping |
437 |
629 |
461 |
| Train |
383 |
543 |
183 |
| Other method |
236 |
742 |
427 |
| Any method |
4'074 |
8'593 |
4'759 |
| Women |
|
|
|
| Poisoning†
|
283 |
1'144 |
1'257 |
| Firearms |
82 |
186 |
32 |
| Hanging |
268 |
708 |
355 |
| Jumping |
210 |
518 |
419 |
| Train |
203 |
400 |
100 |
| Other method |
117 |
619 |
515 |
| Any method |
1'163 |
3'575 |
2'678 |
| * Including 552 suicides reported by right-to-die organisations (2003–2008) and additional 446 suspected assisted suicides (codes, 1998–2008)
† Including 723 suicides reported by right-to-die organisations (2003–2008) and additional 575 suspected assisted suicides (codes, 1998–2008) |
Results
Study population
The SNC included 8'527'786 individuals (4'215'516 men and 4'312'270 women) who contributed follow-up time in the period 1991 to 2008. A total of 3'915'541 men and 4'024'756 women were 15 to 94 years old and included in the present analysis. Table 1 shows the number of men and women and person-years at risk in the different age groups, and the number of suicides completed by different methods. Analyses were based on a total of 24'842 suicides and over 100 million person-years of follow-up. Overall, 17'426 (71.3%) suicides were by men. In men, firearms suicide was the most important method in all age groups, followed by hanging in age groups 15–34 years and 35-64 years, and poisoning in age group 65–94 years. In women hanging and jumping were the most important methods in age group 15–34 years, whereas poisoning followed by hanging or jumping dominated the two older groups.
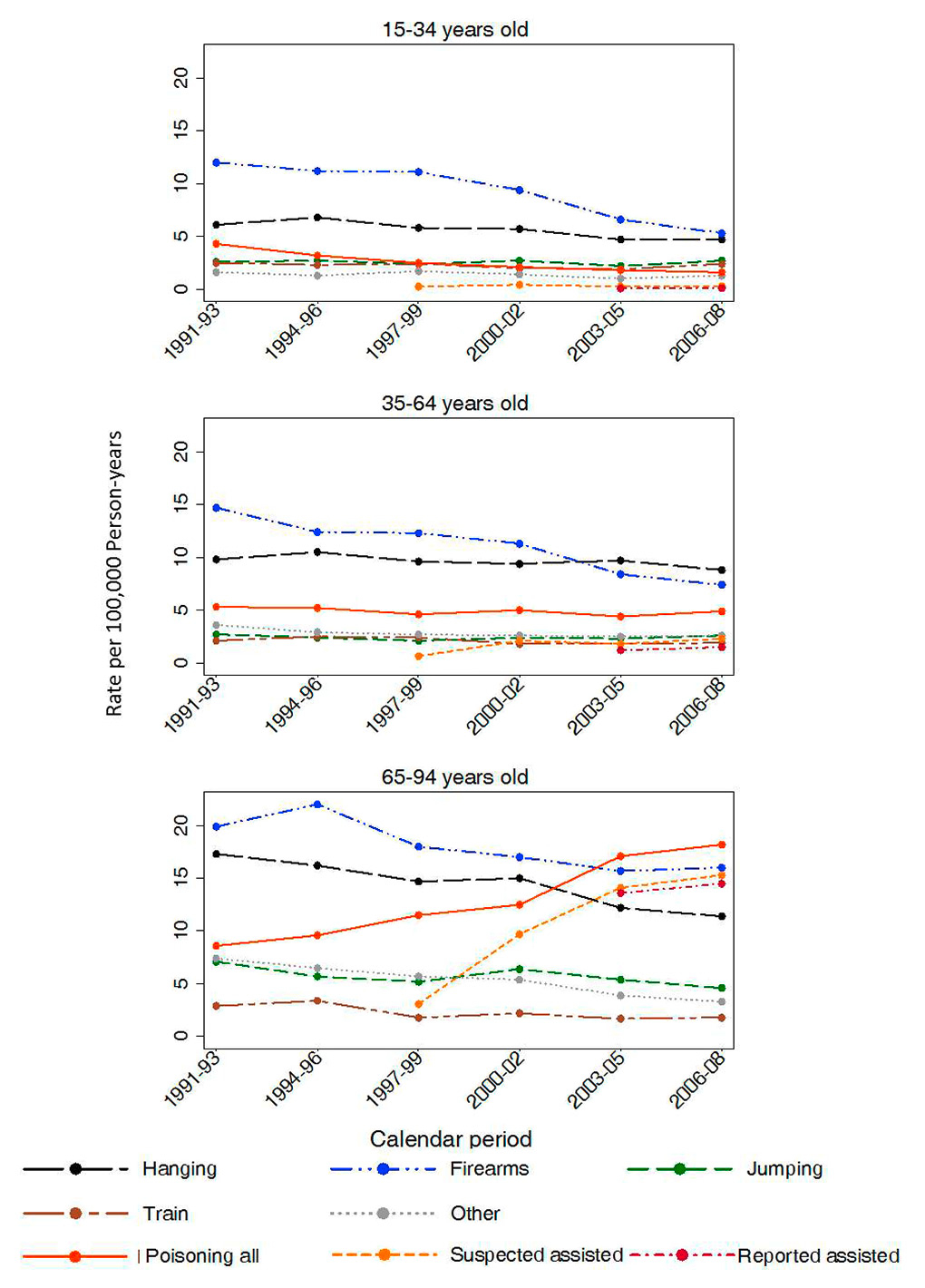
Figure 2
Time-trends of suicide rates by method in men; Switzerland 1991–2008.
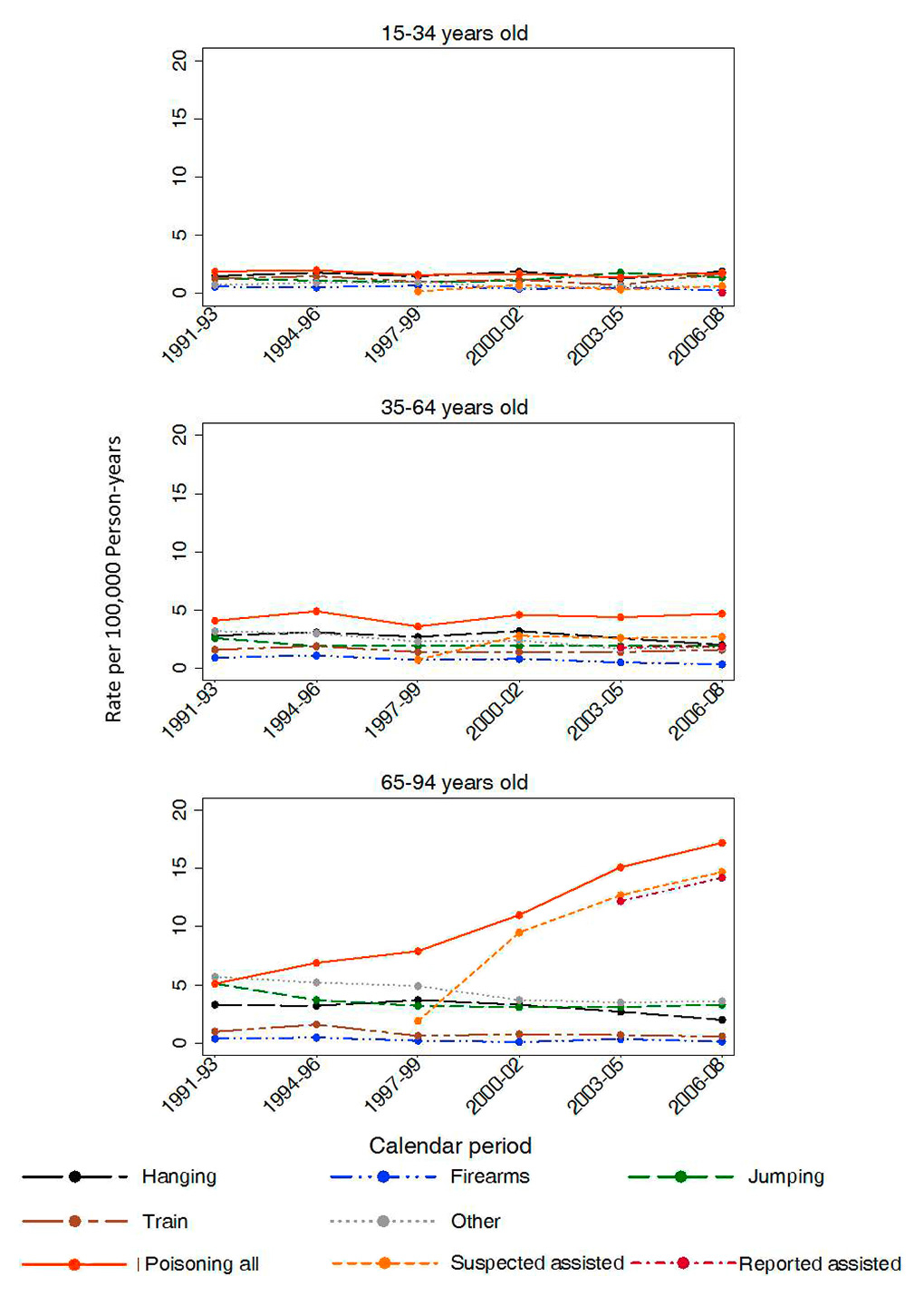
Figure 3
Time-trends of suicide rates by method in women; Switzerland 1991–2008.
During 1998 to 2008 a total of 2'211 suicides were classified as suspected assisted suicides (based on codes 61.8 or 61.9 on the death certificate). Furthermore, 1'275 assisted suicides were reported by the right-to-die organisations from 2003–2008. Of the 1'275 suicides assisted by the right-to-die organisations, 1'190 (93.3%) had been coded as suspected suicides (937 with code 61.8, 253 with 61.9). There were an additional 47 deaths with assisted suicide or a right-to-die organisation mentioned on the death certificate (code 61.8) and an additional 255 deaths with pentobarbital sodium as the cause of death (code 61.9).
Trends in suicide rates over time
Figure 1 shows trends in suicide rates over calendar periods in men and women for all methods combined. In men rates declined in all age groups: from 29.2 in 1991–1993 to 17.9 during 2006–2008 (p <0.001) in age group 15–34 years, from 38.2 to 28.2 in age group 35‒64 years (p <0.001), and from 63.3 to 55.1 in age group 65‒94 years (p = 0.001). In women no decline was observed in age group 15–34 years, with a rate per 100'000 of 7.4 during 1991–1993 and 7.7 in 2006–2008 (p = 0.40). A slight decline was noted in age group 35‒64 years (from 15.1 in 1991–1993 to 12.2 during 2006–2008, p <0.001) whereas an increase was noted in the oldest age group (from 20.5 in 1991–1993 to 26.7 during 2006–2008, p <0.001). For all age groups combined, rates declined in men from 38.3 in 1991–1993 to 29.9 during 2006–2008 (p <0.001), but increased in women from 13.6 in 1991–1993 to 14.3 2006–2008 (p <0.001).
Trends in suicide rates by method
Trends in suicide rates 1991–2008 are shown in figure 2 for men and in figure 3 for women. Table 2 shows rates of suicide for the periods 1991–1993 and 2006–2008, the relative annual change and the p-value for time trend from Poisson regression.
The most important changes in incidence were observed for suicide by poisoning in the oldest age group: in men rates more than doubled (from 8.6 in 1991–1993 to 18.2 per 100'000 in 2006–2008) and in women they more than tripled (from 5.1 to 17.2 per 100'000). The rate of suspected assisted suicides increased from 2.37 per 100'000 in 1998–1999 to 14.98 per 100'000 in 2006–2008. In men 611 suicides were suspected assisted suicides, corresponding to 76.4% of all 800 suicides by poisoning recorded in men 1998 to 2008. In women the corresponding figures were 792 of 979 suicides by poisoning (80.9%). Similarly, in men 418 suicides were reported from 2003 to 2008 by the right-to-die associations, corresponding to 79.3% of all 527 suicides by poisoning recorded in these years. In women the corresponding figures were 547 of 669 suicides by poisoning (81.8%). There were no substantial changes in rates of suicide by poisoning in the other age groups except for a decline in men aged 14–34 years (from 4.3 to 1.6 per 100'000).
Other notable trends over time related to suicide by firearms, with reductions in both genders and all age groups. There were also reductions in suicides by hanging, jumping, train and other means. In both men and women the reductions in the incidence of these suicides was more pronounced in the oldest age group, both in relative and absolute terms (table 2).
|
Table 2: Rates of suicide per 100'000 person-years by different methods in the first time period (1991–1993), in the last time period (2006–2008); the relative annual change and the p-value for time trend (from Poisson regression) by age group and sex. |
|
|
Age group 15–34 years
|
Age group 35–64 years
|
Age group 65–94 years
|
| Rate |
Relative annual change (95% CI) |
p-value |
Rate |
Relative annual change (95% CI) |
p-value |
Rate |
Relative annual change (95% CI) |
p-value |
| 1991–93 |
2006–08 |
1991–93 |
2006–08 |
1991–93 |
2006–08 |
|
Men
|
|
|
|
|
|
|
|
|
|
|
|
|
| Poisoning* |
4.30 |
1.62 |
0.93 (0.92–0.95) |
<0.001 |
5.30 |
4.92 |
0.99 (0.98–1.00) |
0.197 |
8.56 |
18.22 |
1.06 (1.04–1.07) |
<0.001 |
| Firearms |
12.0 |
5.28 |
0.95 (0.94–0.96) |
<0.001 |
14.74 |
7.38 |
0.96 (0.95–0.96) |
<0.001 |
20.04 |
15.81 |
0.98 (0.97–0.99) |
<0.001 |
| Hanging |
6.13 |
4.66 |
0.98 (0.97–0.99) |
<0.001 |
9.82 |
8.81 |
0.99 (0.98–1.00) |
0.046 |
17.28 |
11.35 |
0.97 (0.96–0.98) |
<0.001 |
| Jumping |
2.64 |
2.66 |
1.00 (0.98–1.01) |
0.691 |
2.65 |
2.60 |
1.00 (0.98–1.01) |
0.841 |
7.13 |
4.61 |
0.98 (0.96–0.99) |
0.021 |
| Train |
2.54 |
2.43 |
0.99 (0.97–1.01) |
0.301 |
2.10 |
1.89 |
0.98 (0.97–0.99) |
0.034 |
2.94 |
1.75 |
0.96 (0.93–0.99) |
0.003 |
| Other |
1.57 |
1.27 |
0.98 (0.96–1.01) |
0.191 |
3.61 |
2.64 |
0.98 (0.97–0.99) |
0.004 |
7.38 |
3.31 |
0.94 (0.93–0.97) |
<0.001 |
| Any |
29.18 |
17.91 |
0.97 (0.96–0.97) |
<0.001 |
38.22 |
28.24 |
0.98 (0.98–0.98) |
<0.001 |
63.25 |
55.08 |
0.99 (0.98–0.99) |
0.001 |
|
Women
|
|
|
|
|
|
|
|
|
|
|
|
|
| Poisoning* |
1.92 |
1.84 |
0.99 (0.96–1.01) |
0.259 |
4.11 |
4.68 |
1.01 (0.99–1.02) |
0.314 |
5.06 |
17.16 |
1.09 (1.07–1.10) |
<0.001 |
| Firearms |
0.61 |
0.28 |
0.96 (0.92–1.01) |
0.085 |
0.91 |
0.34 |
0.94 (0.91–0.97) |
<0.001 |
0.39 |
0.14 |
0.94 (0.88–1.01) |
0.083 |
| Hanging |
1.48 |
1.88 |
1.00 (0.98–1.03) |
0.704 |
2.77 |
1.96 |
0.98 (0.97–1.00) |
0.012 |
3.33 |
2.04 |
0.97 (0.95–0.99) |
0.008 |
| Jumping |
1.31 |
1.44 |
1.02 (0.99–1.05) |
0.125 |
2.56 |
1.85 |
0.98 (0.97–0.99) |
0.038 |
5.06 |
3.27 |
0.97 (0.95–0.99) |
0.004 |
| Train |
1.38 |
1.72 |
1.00 (0.97–1.02) |
0.778 |
1.55 |
1.55 |
0.99 (0.97–1.01) |
0.492 |
0.94 |
0.57 |
0.95 (0.92–0.99) |
0.013 |
| Other |
0.73 |
0.56 |
0.97 (0.94–1.01) |
0.092 |
3.22 |
1.85 |
0.96 (0.94–0.97) |
<0.001 |
5.67 |
3.55 |
0.96 (0.95–0.98) |
<0.001 |
| Any |
7.43 |
7.72 |
1.00 (0.98–1.01) |
0.404 |
15.13 |
12.22 |
0.98(0.98–0.99) |
<0.001 |
20.46 |
26.73 |
1.02 (1.01–1.03) |
<0.001 |
| CI = confidence interval
* Including suicides suspected (codes, 1998–2008) or reported (2003–2008) as assisted suicides |
Discussion
We analysed trends in suicides completed using different methods in Switzerland during the 18-year period from 1991 to 2008. Thanks to dedicated codes used at the Federal Statistical Office for suspected assisted suicides and data provided by three right-to-die organisations, we were able to distinguish between assisted and unassisted suicides by poisoning. We found that in men suicide rates declined in all age groups, but declines were more pronounced in younger men. The trends in men were driven by declining rates of suicide by firearms, and in the oldest age group by an increase in suicide by poisoning. In women rates changed little over time in the younger age groups but increased substantially in older women, owing to an increase in suicides by poisoning. Overall, the rate of suicide increased in women whereas it declined in men. Of note, in the oldest age group about 80% of suicides by poisoning were assisted suicides, both in men and women.
In Switzerland euthanasia is prohibited, but article 115 of the penal code rules that assistance in suicide is allowed if no selfish interests are involved [5]. Proposed in 1918, the article did not intend to regulate assisted suicide at the end of life, but was concerned with suicides motivated by honour and romance [8]. Today volunteers working for right-to-die associations assist suicides in members requesting such assistance based on this law. The physicians’ role is restricted to assessing the decisional capacity of the person requesting assistance, and to prescribing the lethal drug. According to internal regulations of the right-to-die organisations, but not according to the law, assistance is provided only to members suffering from an incurable illness, intolerable suffering or a severe disability.
To the best of our knowledge, the Swiss National Cohort is the only population-based cohort study of assisted suicide worldwide [6]. Previous analyses of the cohort showed that sociodemographic factors associated with assisted and unassisted suicide differed. For example, whereas individuals with tertiary education had a lower risk of unassisted suicide compared with people with primary education, they were more likely to die by assisted suicide [6, 14]. Divorced people, those living alone and those without religious affiliation had a higher rate of unassisted and assisted suicide than the married, those living with others and Protestants or Catholics [6, 14, 15]. Mental and behavioural disorders were the most common underlying causes recorded on the death certificate of unassisted suicides, and cancer was the most common condition among those who died by assisted suicide [6, 14].
Comorbidities such as cancer and other debilitating chronic diseases are risk factors both for assisted and unassisted suicide [16] and one of the reasons for the increasing rate of suicide with age [17–19]. Other risk factors for suicide in later life are stressful life events and social isolation, but also access to means [14, 18]. In countries where assisted dying is legal the rates of assisted suicide also increase with age [20]. In Switzerland about 85% of death certificates of assisted suicides mentioned at least one underlying cause, mainly cancer and nervous system causes [6]. In the present study the substantial increase in assisted suicide in older women, with a net increase in the rate of suicide overall in women, must be of concern. We have argued previously that further research is needed to clarify the reasons for the tripling of rates in assisted suicides in women, and the doubling of rates in men, and to what extent this difference might reflect greater vulnerability of women compared with men [6]. A better understanding of the attitudes and values of those choosing assisted suicide, the attitudes and values of their families, and of access to palliative care is required [6].
The observed decline in numbers of unassisted suicides is in accordance with studies from other European countries and the United States [2, 10]. One explanation for this decrease is an improvement in treatment of psychiatric conditions [21], the most important risk factor for suicides. Restriction of access to suicide means may have had an impact [10, 22], for example, the introduction of catalytic converters in cars [23]. In Switzerland the accelerated decline in firearms suicide after the “ARMY XXI” reform could explain the more pronounced decline of suicides in younger men [24]. The soldiers of the Swiss military army keep their firearms at home and, after completing their service, many buy their ordnance weapons for a small fee. Army-issued firearms are therefore widely available: about half of Swiss households keep or own a firearm [24]. From March 2003 through February 2004, the number of Swiss soldiers was halved as a result of the reform, leading to a decrease in the availability of guns. A recent analysis of the trends in firearms suicides in men aged 18–43 years 1995–2008 concluded that this reduction was accompanied by a drop in firearms suicide during the period from 2002 to 2005 [25]. Interestingly, there was some evidence of methods substitution, with about one fifth of the reduction in firearms suicide substituted by other methods [26]. An association between suicide rates and unemployment and other economic indicators has also been reported [22, 27, 28]. In Switzerland suicide rates declined even in the early 1990s, despite increasing rates of unemployment [29].
We relied on routine mortality statistics which are known to underestimate the number of suicides: some suicides might be coded as other causes. A recent systematic review of studies of the reliability of suicide statistics concluded that only few studies had been done, with under-reporting varying widely from less than 10% to over 30% of suicides [30]. Misclassification of suicides may be less likely in Switzerland because families and local authorities do not receive a copy of the death certificate. Furthermore, death registration is anonymous in Switzerland. A weakness of our study is the lack of data on psychiatric morbidity and the use of alcohol and other drugs. A systematic review of psychological autopsy studies of suicide found that mental disorders were present in about 90% of suicides [31], but this literature has been criticised because psychological autopsy may be unreliable [32, 33].
The World Health Organization (WHO) recommends a multi-sectorial approach to suicide prevention, which includes measures to restrict access to means for suicide, including pesticides, firearms and medications, early diagnosis and treatment of depression and other psychiatric conditions, and social support of vulnerable individuals and the fight against stigma [3]. High-quality, patient-centred palliative care services have been advocated to prevent assisted suicides [34]. Of note, WHO stresses the importance of surveillance to monitor the effect of prevention efforts [3]. Today, the three main right-to-die organisations report the suicides they assisted on a voluntary basis to the Federal Statistical Office, but small organisations and physicians who assist suicides without an organisation do not. We believe that in Switzerland and other countries where assisted suicide is legal, rates of assisted suicide should be carefully monitored, and that reporting of assisted suicides should be compulsory, including data on patient characteristics and underlying comorbidities [6].
Acknowledgments:We thank the Federal Statistical Office (FSO) for providing mortality and census data and for the support that made the Swiss National Cohort and this study possible. We would like especially to thank Christoph Junker and Chantal Violand from the FSO for their help with this study. The members of the Swiss National Cohort Study Group are Matthias Egger (Chairman of the Executive Board), Adrian Spoerri and Marcel Zwahlen (Bern, Switzerland), Milo Puhan (Chairman of the Scientific Board), Matthias Bopp (Zurich, Switzerland), Nino Künzli (Basel, Switzerland), Fred Paccaud (Lausanne, Switzerland), and Michel Oris (Geneva, Switzerland).
References
1 Federal Statistical Office. Todesfälle: Anzahl, Entwicklung und Ursachen. Secondary Todesfälle: Anzahl; Entwicklung und Ursachen 2014. Available at: http://www.bfs.admin.ch/bfs/portal/de/index/themen/14/02/04/key/01.html.
2 Levi F, La Vecchia C, Lucchini F, Negri E, Saxena S, Maulik PK, et al. Trends in mortality from suicide; 1965–99. Acta Psychiatr Scand. 2003;108(5):341–9.
3 WHO. Preventing suicide: A global imperative. Secondary Preventing suicide: A global imperative 2014. Available at: http://www.who.int/mental_health/suicide-prevention/world_report_2014/en/ (accessed 28.01.2015).
4 Bundesamt für Gesundheit. Suizid und Suizidprävention in der Schweiz; 2005:41.
5 Burkhardt S, La HR. Debates About Assisted Suicide in Switzerland. Am J Forensic Med Pathol. 2012.
6 Steck N, Junker C, Maessen M, Reisch T, Zwahlen M, Egger M. Suicide assisted by right-to-die associations: a population based cohort study. Int J Epidemiol. 2014;43(2):614–22 doi: 10.1093/ije/dyu010 [published Online First: Epub Date]|.
7 Bosshard G, Ulrich E, Bar W. 748 cases of suicide assisted by a Swiss right-to-die organisation. Swiss Med Wkly. 2003;133(21-22):310–7.
8 Hurst SA, Mauron A. Assisted suicide and euthanasia in Switzerland: allowing a role for non-physicians. BMJ. 2003;326(7383):271–3.
9 exit. Erneut mehr Leidenden geholfen. 2015. Available at: http://www.exit.ch/news/news/details/erneut-mehr-leidenden-geholfen/.
10 Hepp U, Ring M, Frei A, Rössler W, Schnyder U, Ajdacic-Gross V.. Suicide trends diverge by method: Swiss suicide rates 1969–2005. Eur Psychiatry. Epub 2009 Aug 19. PMID: 19695842.
11 Federal Statistical Office. Sterbehilfe in der Schweiz 1998–2009: Knapp 300 assistierte Suizide 2009; 2012.
12 Bopp M, Spoerri A, Zwahlen M, Gutzwiller F, Paccaud F, Braun-Fahrländer C, et al. Cohort Profile: the Swiss National Cohort – a longitudinal study of 6.8 million people. Int J Epidemiol. 2009;38(2):379–84.
13 Spoerri A, Zwahlen M, Egger M, Bopp M. The Swiss National Cohort: a unique database for national and international researchers. Int J Public Health. 2010;55(4):239–42.
14 Steck N, Egger M, Zwahlen M, et al. Assisted and unassisted suicide in men and women: longitudinal study of the Swiss population. Br J Psychiatry. 2015; in press.
15 Spoerri A, Zwahlen M, Bopp M, Gutzwiller F, Egger M. Religion and assisted and non-assisted suicide in Switzerland: National Cohort Study. Int J Epidemiol. 2010;39(6):1486–94.
16 Robson A, Scrutton F, Wilkinson L, MacLeod F. The risk of suicide in cancer patients: a review of the literature. Psycho-oncology 2010;19(12):1250–8 doi: 10.1002/pon.1717 [published Online First: Epub Date].
17 Voaklander DC, Rowe BH, Dryden DM, Pahal J, Saar P, Kelly KD.. Medical illness; medication use and suicide in seniors: a population-based case-control study. J Epidemiol Community Health. 2008;62(2):138–46 doi: 10.1136/jech.2006.055533 [published Online First: Epub Date]|.
18 Conwell Y, Duberstein PR, Caine ED. Risk factors for suicide in later life. Biol Psychiatry. 2002;52(3):193–204.
19 Conwell Y, Thompson C. Suicidal behavior in elders. Psychiatr Clin North Am. 2008;31(2):333–56.
20 Steck N, Egger M, Maessen M, Reisch T, Zwahlen M.. Euthanasia and Assisted Suicide in Selected European Countries and US States: Systematic Literature Review. Med Care. 2013;51(10):938–44 doi: 10.1097/MLR.0b013e3182a0f427 [published Online First: Epub Date]|.
21 Rihmer Z. Can better recognition and treatment of depression reduce suicide rates? A brief review. EurPsychiatry. 2001;16(7):406–9.
22 Hawton K; van Heeringen K. Suicide. Lancet. 2009;373:1372–81.
23 Kreitman N. The coal gas story. United Kingdom suicide rates; 1960–71. Br J Prev Soc Med. 1976;30(2):86–93.
24 Reisch T, Steffen T, Habenstein A, Tschacher W.. Change in Suicide Rates in Switzerland Before and After Firearm Restriction Resulting From the 2003 “Army XXI” Reform. Am J Psychiatry. 2013 doi: 10.1176/appi.ajp.2013.12091256 [published Online First: Epub Date].
25 Rhodes AE, Boyle MH, Bridge JA, Sinyor M, Links PS, Tonmyr L, et al. Antecedents and sex/gender differences in youth suicidal behavior. World J Psychiatry. 2014;4(4):120–32 doi: 10.5498/wjp.v4.i4.120 [published Online First: Epub Date]|.
26 Gauthier S, Mausbach J, Reisch T, Bartsch C. Suicide tourism: a pilot study on the Swiss phenomenon. J Med Ethics. 2014 doi: 10.1136/medethics-2014-102091 [published Online First: Epub Date].
27 Blakely TA, Collings SC, Atkinson J. Unemployment and suicide. Evidence for a causal association? J Epidemiol Community Health. 2003;57(8):594–600.
28 Fountoulakis KN, Kawohl W, Theodorakis PN, Kerkhof AJ, Navickas A, Höschl C, et al. Relationship of suicide rates to economic variables in Europe: 2000–2011. Bt J Psychiatry. 2014;205(6):486–96 doi: 10.1192/bjp.bp.114.147454 [published Online First: Epub Date]|.
29 Sheldon G. Der Schweizer Arbeitsmarkt seit 1920: langfristige Tendenzen. Die Volkswirtschaft 2010;1:5.
30 Tollefsen IM, Hem E, Ekeberg O. The reliability of suicide statistics: a systematic review. BMC psychiatry 2012;12:9 doi: 10.1186/1471-244x-12-9 [published Online First: Epub Date]|.
31 Cavanagh JT, Carson AJ, Sharpe M, Lawrie SM. Psychological autopsy studies of suicide: a systematic review. Psychol Med. 2003;33(3):395–405.
32 Hjelmeland H, Dieserud G, Dyregrov K, Knizek BL, Leenaars AA. Psychological autopsy studies as diagnostic tools: are they methodologically flawed? Death Stud. 2012;36(7):605–26.
33 Frei A, Bucher T, Walter M, Ajdacic-Gross V. Suicides in the Canton of Lucerne over 5 years: subjects with and without psychiatric history and diagnosis. Swiss Med Wkly. 2013;143:w13779.
34 Vögeli D. Gian Domenico Borasio im Gespräch: Autonomie geht weit über Suizidhilfe hinaus. Neuer Zürcher Zeitung 2014.