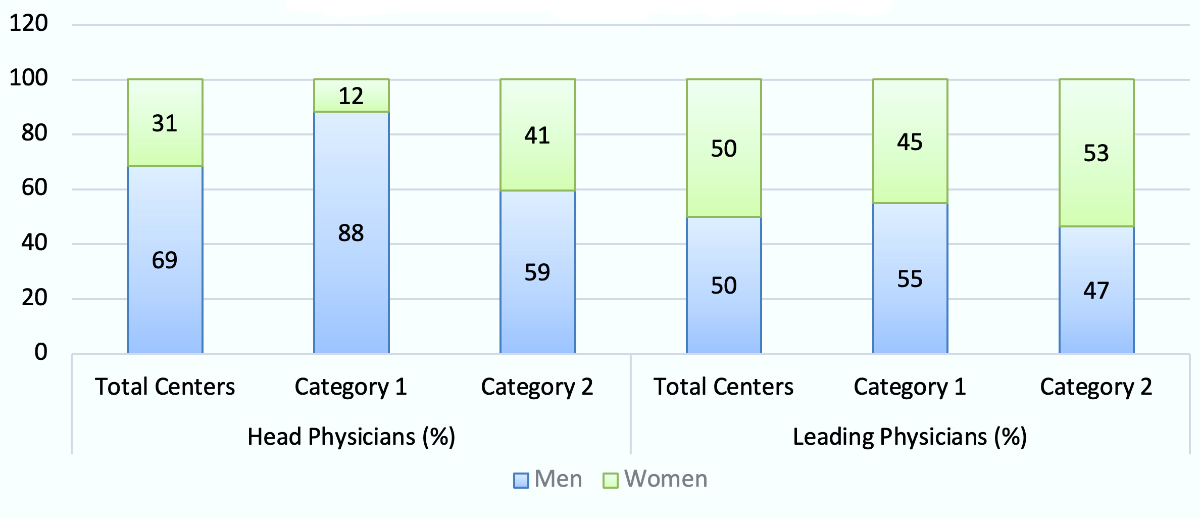
Figure 1 Gender distribution among head and senior physicians of Swiss SSERM-certified emergency departments in 2021. Leading physicians: senior consultants and consultants with extended responsibility.
DOI: https://doi.org/https://doi.org/10.57187/smw.2022.40001
Since specialised emergency medicine units were established for the first time in the 1960s and 70s, emergency medicine has been continuously evolving all over the world and more and more countries have emergency medicine societies and colleges to develop the specialty on a professional and academic level [1, 2]. As already described by Colin Graham in 2015, education and training are the cornerstones of European emergency medicine [2]. However, there are countries, Germany, Austria and Switzerland for example, where emergency medicine is not yet a fully recognised specialty and in-hospital emergency care is often performed by juniors or experts in different medical specialties such as anaesthesiology, surgery, traumatology or internal medicine. Germany is taking actions to foster emergency medicine by creating academic units and establishing a subspecialty. Multiple skills, such as coordination of emergency department flow to minimise overcrowding, correct triage of patients, leadership in large multidisciplinary teams and advanced skills to correctly diagnose and treat critically ill patients are particularly important in emergency physicians [3, 4]. In recognition of the specific skills required, the European Society of Emergency Medicine (EUSEM) has created a European curriculum for emergency physicians including a European board examination [3]. Similar to the standing of clinical emergency training, research in emergency medicine is still young and in many countries, academic expertise such as full professorships are rare compared with other medical specialties. Traditionally, emergency medicine publication rates were lower, but have increased over recent years indicating the important and necessary scientific progress [5].
In terms of gender equality, emergency medicine appears to be lagging behind despite the globally increasing women physician workforce: women physicians were underrepresented among board members of emergency medicine societies associated with the EUSEM as well as in editorial boards of top-ranked academic emergency medicine journals [6, 7]. Reasons for this gender gap are manifold and widely discussed: especially, physical and emotional demands, shift and night work complicating social life and family organisation were declared to be factors contributing to discrimination against women in emergency medicine [8]. Additionally, salary and salary increases were found to stagnate in women compared with men and women were underrepresented in chair positions of emergency medicine residency programmes irrespective of the number of women physicians in practice or training [9, 10].
What is the situation in Switzerland? Overall, emergency medicine is evolving rather slowly but steadily. The Swiss Society of Emergency and Rescue Medicine (SSERM) was founded in 1990 and guidelines for standard requirements of emergency departments are regularly published. Even though the Swiss system of public health is widely respected to be of high quality, it lacks a basic description of emergency care, which is still governed regionally rather than centrally. National efforts were made to create specialty training programmes and standards of care to improve emergency care. However, emergency medicine is no officially board-certified specialisation but rather a certificate of competence acquired during or after completing specialist training. The two educational paths, "prehospital emergency medicine" and "in-hospital emergency medicine", mainly differ in terms of setting. The SSERM curriculum for prehospital emergency medicine includes training in anaesthesiology and intensive care and focusses on out-of-hospital emergency care. The programme for in-hospital emergency medicine requires completed specialisation in either general internal medicine, anaesthesiology, surgery, intensive care, cardiology or orthopaedics-traumatology and focusses on in-hospital emergency care [11].
In view of the evidence presented above, it was the aim of this study to investigate the trends and developments in Swiss emergency medicine over time against the background of a known gender gap to analyse the situation in Switzerland to date. Firstly, the development and gender distribution of the emergency physician workforce were analysed and compared to physicians certified in six other specialties in 2011, 2016 and 2021. Additionally, the number and gender distribution of head and leading physicians of SSERM-certified emergency departments in categories 1 and 2 was investigated in 2021. Secondly, an analysis of Swiss academic emergency medicine including academic tracks, SSERM conferences, professors and chairs was performed.
It was the aim of this retrospective observational longitudinal study to analyse the development of emergency medicine in Switzerland in terms of workforce, gender equality and academic posts.
Firstly, the numbers of SSERM members as well as physicians certified in prehospital and in-hospital emergency medicine were analysed in 2011, 2016 and 2021 to identify relevant trends in number and gender distribution of emergency physicians in Switzerland over a period of 10 years. In order to investigate the workforce development in emergency medicine, the number and gender distribution of SSERM-certified physicians were compared with the number of specialists in general internal medicine, surgery, anaesthesiology, intensive care, cardiology and orthopaedics-traumatology in 2011, 2016 and 2021, since all of these specialists can acquire a board certificate in in-hospital emergency medicine. Additionally, all head physicians, senior consultants and consultants with extended responsibility of emergency departments certified in SSERM categories 1 and 2 as published online [11] were analysed in 2021 with special regard to gender distribution. Criteria for SSERM category 2 include more than 8000 annual consultations, a 24-hour gastroenterology service and an in-house monitoring unit of at least intermediate care standard. In addition to this, emergency departments of SSERM category 1 are mostly tertiary care facilities with more than 20,000 annual consultations and the resources to treat the entire spectrum of emergencies, including, for example, intensive care units, 24-hour interventional radiology and cardiology, a stroke and trauma centre. SSERM category 3 emergency departments focus on primary care and were not included in this analysis since only six-months of working experience can be accredited for the curriculum of in-hospital emergency medicine by the trainee physician. Full details on classification criteria are available online [11].
Secondly, this study focused on Swiss academic emergency medicine. Therefore, the number and gender distribution of professors of emergency medicine in Switzerland were analysed in 2021. Moreover, the number and gender distribution of organising committees, chairs and speakers at annual SSERM conferences were analysed in 2016, 2017, 2018 and 2019. In 2020, no SSERM conference took place due to the COVID-19 pandemic and data for 2021 were not available.
The term “gender” refers to an individual’s social identity, not their biological “sex” at birth. Naturally, both terms include more than two entities. Since “gender” is a well-established term when comparing women and men, this expression was used throughout the manuscript for reasons of simplicity.
Regarding technical terms, the following definitions were used throughout the manuscript in order to be as clear as possible against the background of a heterogeneous and multilingual nomenclature:
Most data were fully publicly available from the official website of the Swiss Medical Association FMH [12]. The managing director of the SSERM provided data on the number and gender distribution of SSERM members as well as annual SSERM conferences. First and last names of head physicians, senior consultants and consultants with extended responsibility were obtained online as published on the hospital websites of SSERM-certified emergency departments in categories 1 and 2. If online data were missing, information was gathered by written inquiry from the departments directly. The gender of each physician was assessed by examination of the first name. In ambiguous cases where gender could not be determined by first name or officially provided picture, an internet search was performed to identify the corresponding individual. Individuals whose gender could not be determined with the above-mentioned methods were classified as “unknown”. Information on Swiss academic tracks in medicine and professorships in emergency medicine was directly obtained from the deaneries by written inquiry.
After completion of data collection, data were exported to a statistical software package (MS Excel, Microsoft Office Professional Plus 2016 for Windows). Data are presented in absolute numbers as well as percentages. Continuous data are presented as median and interquartile ranges or as mean and standard deviation (± SD).
There was no need for ethics committee approval since all data involved in this study were either available online by public access or part of regular statistical analyses. No patient-related data were analysed. The study is not registered and there is no study protocol publicly available.
In 2021, the SSERM had 1191 members overall of whom 415 were women (35%). Compared with 784 members in 2011, there was a growth in members of 52% over a period of 10 years. The proportion of women in 2011 was 26%. The absolute number of woman SSERM members more than doubled during the observation period from 202 in 2011 to 415 in 2021. All numbers as well as numerators and denominators of percentages are given in table 1.
Table 1Physicians by board certification and gender in 2011, 2016 and 2021 in Switzerland.
| Year | Total | Change from 2011 to 2021 | Women | Women | Change proportion of women from 2011 to 2021 | Men | Men | |
| SSERM members | 2021 | 1191 | +52% | 415 | 35% | +9% | 776 | 65% |
| 2016 | 921 | 265 | 29% | 656 | 71% | |||
| 2011 | 784 | 202 | 26% | 582 | 74% | |||
| Board certificate In-Hospital Emergency Medicine | 2021 | 583 | +66% | 228 | 39% | +13% | 355 | 61% |
| 2016 | 449 | 132 | 29% | 317 | 71% | |||
| 2011 | 351 | 90 | 26% | 261 | 74% | |||
| Board certificate Prehospital Emergency Medicine | 2021 | 1322 | +79% | 489 | 37% | +8% | 833 | 63% |
| 2016 | 942 | 308 | 33% | 634 | 67% | |||
| 2011 | 737 | 212 | 29% | 525 | 71% | |||
| Board certificate General Internal Medicine | 2021 | 8423 | +3% | 3828 | 45% | +16% | 4595 | 55% |
| 2016 | 8306 | 3209 | 39% | 5097 | 61% | |||
| 2011 | 8172 | 2360 | 29% | 5812 | 71% | |||
| Board certificate Surgery | 2021 | 1203 | +17% | 309 | 26% | +13% | 894 | 74% |
| 2016 | 1152 | 241 | 21% | 911 | 79% | |||
| 2011 | 1032 | 135 | 13% | 897 | 87% | |||
| Board certificate Anaesthesiology | 2021 | 1591 | +26% | 730 | 46% | +6% | 861 | 54% |
| 2016 | 1499 | 649 | 43% | 850 | 57% | |||
| 2011 | 1259 | 509 | 40% | 750 | 60% | |||
| Board certificate Intensive Care Medicine | 2021 | 744 | +65% | 275 | 37% | +8% | 469 | 63% |
| 2016 | 576 | 181 | 31% | 395 | 69% | |||
| 2011 | 452 | 129 | 29% | 323 | 71% | |||
| Board certificate Cardiology | 2021 | 894 | +114% | 202 | 23% | +7% | 692 | 77% |
| 2016 | 723 | 131 | 18% | 592 | 82% | |||
| 2011 | 417 | 65 | 16% | 352 | 84% | |||
| Board certificate Orthopaedics-Traumatology | 2021 | 1243 | +48% | 142 | 11% | +5% | 1101 | 89% |
| 2016 | 1089 | 97 | 9% | 992 | 91% | |||
| 2011 | 839 | 52 | 6% | 787 | 94% |
In terms of board certificates in in-hospital emergency medicine, 583 carried the certificate in 2021 compared with 351 in 2011 of whom 228 were women (39%) in 2021 and 90 (26%) in 2011. There was an increase in the number of certified in-hospital emergency physicians of 66% over the observed 10-year period. There was an increase of 153% in the number of women physicians certified for In-Hospital Emergency Medicine over the 10 years.
In 2021, 1322 physicians were board certified in prehospital emergency medicine, of whom 489 were women (37%), whereas in 2011, 737 were board certified, of whom 212 (29%) were women. There was an overall increase of 79% in board certified prehospital emergency physicians and an increase in the number of women of 131% over a 10-year period.
The development in number and gender distribution of SSERM board-certified emergency physicians compared with the Swiss board-certified physicians in six other specialties (general internal medicine, surgery, anaesthesiology, intensive care, cardiology, orthopaedics-traumatology) in 2011, 2016 and 2021 is given in table 1.
In 2021, 49 emergency departments were accredited teaching sites for category 1 or 2 by the SSERM of which 16 were ranked category 1 and 33 category 2. For 15 emergency departments no data were available online. Seven centres provided information after written inquiry, whereas no information was available from eight emergency departments for the final analysis (16%). Overall, of all 54 head physicians 37 were men (69%). Five emergency departments were led by two head physicians concomitantly, one emergency department of SSERM category 1 and four emergency departments of category 2. In all 17 head physicians category 1, 15 were men (88%), whereas in category 2, of all 37 head physicians 22 were men (60%) in 2021.
Overall, there were 148 consultants with extended responsibility and senior consultants of whom 74 were men (50%). There were 62 senior consultants and consultants with extended responsibility in SSERM emergency departments category 1 of whom 34 were men (55%), and 86 in category 2 of whom 40 were men (47%). The proportions of women and men among emergency department leading physicians are given in figure 1.
Figure 1 Gender distribution among head and senior physicians of Swiss SSERM-certified emergency departments in 2021. Leading physicians: senior consultants and consultants with extended responsibility.
In total, 11 Swiss universities offered at least partial studies of medicine in 2021. At six Swiss universities, students could graduate with a full medical degree: the Universities of Basel, Bern, Zurich, Fribourg, Lausanne and Geneva. Two universities, namely the Universities of Lucerne and St Gallen, offered a shared track together with the University of Zurich where Bachelor and Master of Medicine take place in both locations. The University of the Italian Speaking Part of Switzerland offered the Master Degree only while students completed their Bachelor Degree at either the University of Basel or Zurich. At the University of Neuchâtel, medical students could complete the first year of their studies and needed afterwards to change to another university. At the ETH Zurich, the federal institute of technology, medical students could earn a Bachelor of Science in Medicine degree.
Emergency medicine was a mandatory subject in the student curriculum of all universities apart from the University of Neuchâtel where only the first year of medical studies could be completed. In 2021, there were six full professors in emergency medicine of whom one was a woman holding the professorship for cardiology rather than emergency medicine (17%) and three associated professors of whom all were men.
The analysis of the organisational committees of annual Swiss emergency medicine conferences organised by the SSERM revealed that men by far outnumbered women from 2016 to 2019. In terms of chairs and speakers, men outnumbered women at every conference. Details of gender distribution at the annual SSERM conference are given in figure 2.
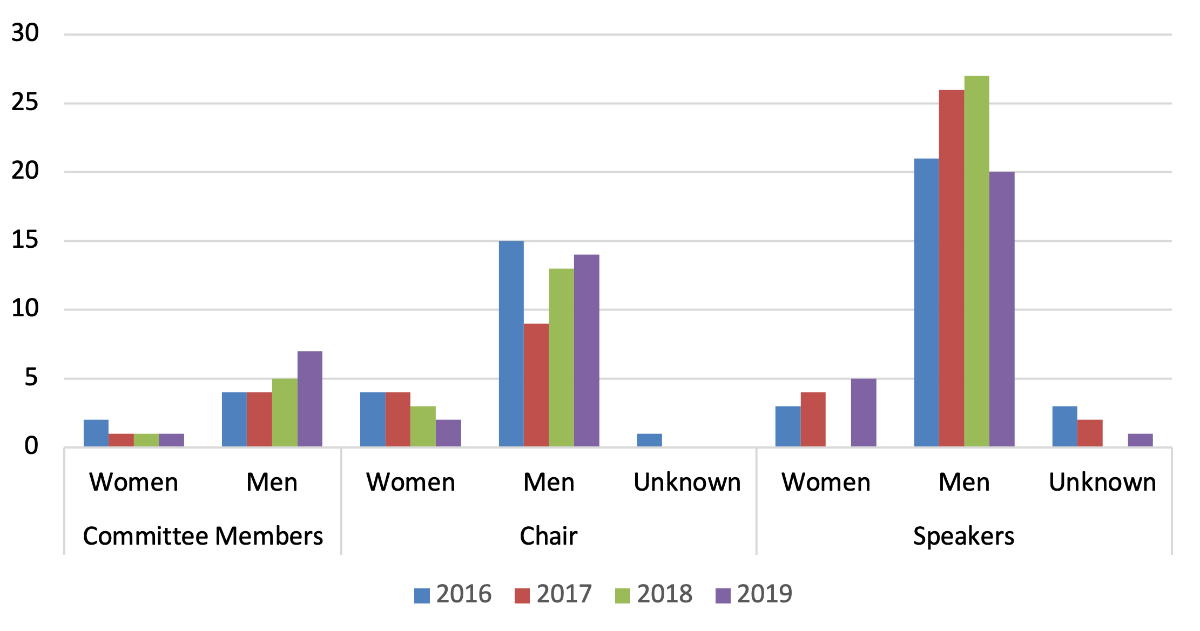
Figure 2 Gender distribution among committee members, chairs and speakers at the annual SSERM conferences in 2016, 2017, 2018 and 2019.
The present study of the development of emergency medicine in Switzerland not only showed an increase of SSERM members overall, but clearly a growing number of women members over a 10-year period. Similar trends were found for SSERM board certificates, with a rise of 66% in physicians certified in in-hospital emergency medicine and a rise of 79% in prehospital emergency medicine. The number and proportion of women remarkably increased for both certificates. In comparison with other specialties such as general internal medicine and surgery, the increase of board-certified physicians in emergency medicine was markedly larger (table 1). In view of this trend, it is essential to ensure and even promote adequate training for the growing workforce of emergency physicians with focus on specific skills. In a first description and national analysis of Swiss emergency departments in 2006, crowding of emergency departments, limited experience of emergency physicians and the regional heterogeneity of emergency care capabilities were identified as threats to a high-quality emergency care in Switzerland [13]. Therefore, advancement in emergency training and recognition of emergency medicine as a distinct speciality has repeatedly been argued and merits reconsideration in view of the continuously increasing number of emergency physicians [4, 14]. In terms of gender equality, 69% of all analysed head physicians in SSERM-certified emergency departments of category 1 or 2 were men in 2021. Fortunately, gender equality seems to be established in leading physician teams with a gender distribution of exactly 50% in consultants with extended responsibility and senior consultants. Electing head physicians is a time-consuming process which might explain a delay in women becoming head physicians even though they are growing in number among emergency physicians overall and leading physicians.
When looking at academics in Swiss emergency medicine, the heterogeneous nomenclature unfortunately complicates a proper comparison. Overall, the number of medical schools increased and emergency medicine was a mandatory subject in the curricula of all but one university in 2021. It also appears reasonable not to include emergency medicine in the mandatory curriculum of first year students at the University of Neuchâtel. Six full professors in emergency medicine were reported for 2021 by the deaneries. In view of the clearly increasing numbers of emergency physicians in Switzerland and the fact that emergency medicine is part of the mandatory curriculum of all medical students, the number of professors for this specialty is surprisingly low. Strikingly, academic terminology and information provided differed between Swiss universities and it appeared as if the definition of chair / full professor was not used homogeneously at all. This finding alone already indicates a certain lack of a clearly structured and straightforward academic track in emergency medicine. The development of specific research curricula and mentorship in emergency medicine are crucial to foster academic careers and increase the scientific credibility of this medical discipline.
The fact that only one of all reported emergency medicine professors in Switzerland was a woman in 2021, including the three additional men associate professors, is once more representative for the academic gender gap in emergency medicine. Concerning the annual SSERM conference, results were even more distinct: the proportion of women even decreased in the scientific committee and, with the exception of one year, also in chairs. Among speakers, women were similarly underrepresented, but at least an upward trend was noted with an increase from 11% in 2016 to 21% in 2019. Whether similar results would be found for publication rates, first and senior authorships for emergency physicians in Switzerland needs to be investigated. This proof of the academic gender gap in emergency medicine stands in line with the findings of numerous previous studies [6, 7]. What are the reasons for the constant underrepresentation of women in emergency research even though the proportion of women in the physician workforce is clearly increasing? The explanation of a time delay between finishing clinical training and success in science can be rebutted by our finding that the proportion of women in scientific committees decreased rather than increased over the years. Even though women are still underrepresented as speakers at the SSERM conferences, there is a favourable upward trend. However, Wiler et al. found that women worked more clinical hours and were paid less when holding leadership roles in academic emergency medicine compared with men [15]. Proposed strategies to increase diversity in healthcare and academic leadership in emergency medicine include early career planning with senior faculty members, establishing and continuously expanding a mentorship network as well as overcoming misalignments of one's own experiences and goals and the priorities of the working institution [16]. One more crucial goal is to create leadership and development opportunities by diverse, inclusive and trained search committees [16].
Since the analyses of the present study especially regarding SSERM-certified emergency departments are based on data published online, outdated information cannot be ruled out and might affect the analysis and interpretation. Furthermore, data on leading physicians was missing from 16% of all emergency departments in SSERM categories 1 or 2. In terms of gender classification, we are well aware that gender is no binary term but for reasons of statistical analysis the classification “woman”, “man” and “unknown” were determined. To correctly identify gender, secondary determinants such as internet research and photos or faculty profiles on institutional websites were consulted. For academic emergency medicine and professorships, the heterogeneous and multilingual terminology among Swiss universities might have led to misclassifications.
However, this study is the first analysis and description of the status quo in Swiss emergency medicine including a national investigation of working physicians and academics with observational longitudinal data. It would be interesting to conduct larger national studies with more profound demographic data, for example including age or language to identify influencing factors. Furthermore, measures should be taken to foster academic careers in emergency medicine to increase the influence and scientific credibility of the specialty.
Despite the fact that emergency medicine is not yet a fully independent medical specialty in Switzerland, this study showed that the number of SSERM members and board-certified emergency physicians remarkably increased during the observed 10 years. The increase of women physicians in emergency medicine was even more distinct, with 50% of leading physicians in SSERM certified emergency departments of category 1 and 2 being women. However, academic emergency medicine in Switzerland appears underdeveloped with only a few leading academic positions at medical faculties, potentially complicating the progress in Swiss emergency medicine on a scientific and professional level.
Mostly public access. G. Kaufmann, managing director of SSERM, provided data on SSERM members, board certified physicians and participants of SSERM conferences. Missing data on leading physicians of SSERM-certified emergency departments was partially provided by the departments on direct request. Deaneries and university secretaries of medical departments supported missing data on academics.
We would like to express our special thanks to Gabriela Kaufmann, the managing director of SSERM, for provision of all relevant data regarding SSERM members and physicians with SSERM board certification in emergency medicine. Additionally, we would also like to express our gratitude to all participating SSERM-certified emergency departments and to all deaneries and university secretaries supporting us with missing data.
Authors' contributions: SR, MH and GL were involved in data collection, statistical analysis and performed the manuscript draft. All authors critically revised the manuscript draft.
None
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflict of interest was disclosed.
1. Totten V, Bellou A. Development of emergency medicine in Europe. Acad Emerg Med. 2013 May;20(5):514–21. https://doi.org/10.1111/acem.12126
2. Graham CA. Emergency medicine in Europe: looking forward to 2015. Eur J Emerg Med. 2015 Feb;22(1):1. https://doi.org/10.1097/MEJ.0000000000000238
3. Stroobants J, Arafat R, Leach R, Halpern P, Golea A, Heyworth J, et al. Cooperation in emergency medicine in Europe: the bright side of the medal. Eur J Emerg Med. 2018 Feb;25(1):1–2. https://doi.org/10.1097/MEJ.0000000000000521
4. Hautz WE, Sauter TC, Lehmann B, Exadaktylos AK. Professionalisation rather than monopolisation is the future of emergency medicine in Europe. Eur J Anaesthesiol. 2018 Mar;35(3):234–5. https://doi.org/10.1097/EJA.0000000000000744
5. Miró OS, Burillo-Putze G. Research in emergency medicine in Europe. Eur J Emerg Med. 2012 Apr;19(2):63–8. https://doi.org/10.1097/MEJ.0b013e32834749a0
6. Lindner G, Rupp A, Exadaktylos AK, Ravioli S. Gender distribution in board memberships of emergency medicine societies. Am J Emerg Med. 2021 Sep;47:176–9. https://doi.org/10.1016/j.ajem.2021.04.042
7. Ravioli S, Rupp A, Exadaktylos AK, Lindner G. Gender distribution in emergency medicine journals: editorial board memberships in top-ranked academic journals. Eur J Emerg Med. 2021 Oct;28(5):380–5. https://doi.org/10.1097/MEJ.0000000000000842
8. Ortega M. Feminization of Emergency Medicine in Europe in the 21st century. Eur J Emerg Med. 2020 Jun;27(3):167–8. https://doi.org/10.1097/MEJ.0000000000000709
9. Wiler J, Roubds K. McGowan and Baird J. Continuation of Gender Disparities in Pay Among Academic Emergency Medicine Physicians. Acad Emerg Med. 2019 Mar;26(3):286–92. https://doi.org/10.1111/acem.13694
10. Parsons M, Krzyzaniak S, Mannix A, Rocca N, Chan TM, Gottlieb M. Peek at the glass ceiling: gender distribution of leadership among emergency medicine residency programs. Emerg Med J. 2021 May;38(5):381–6. https://doi.org/10.1136/emermed-2019-208951
11. https://www.sgnor.ch/weiter-und-fortbildung/, accessed 25.03.2022
12. https://www.fmh.ch/themen/aerztestatistik/fmh-aerztestatistik.cfm, accessed 28.03.2022
13. Sanchez B, Hirzel AH, Bingisser R, Ciurea A, Exadaktylos A, Lehmann B, et al. State of Emergency Medicine in Switzerland: a national profile of emergency departments in 2006. Int J Emerg Med. 2013 Jul;6(1):23. https://doi.org/10.1186/1865-1380-6-23
14. Zimmermann H, Bachmann D, Berger P, Diem K, Durrer B, Ummenhofer W. Die klinische Notfallmedizin im Wandel. Schweiz Arzteztg. 2015;96(1-2):6–7.
15. Wiler JL, Wendel SK, Rounds K, McGowan B, Baird J. Salary disparities based on gender in academic emergency medicine leadership. Acad Emerg Med. 2022 Mar;29(3):286–93. https://doi.org/10.1111/acem.14404
16. Oh L, Linden JA, Zeidan A, Salhi B, Lema PC, Pierce AE, et al. Overcoming barriers to promotion for women and underrepresented in medicine faculty in academic emergency medicine. J Am Coll Emerg Physicians Open. 2021 Dec;2(6):e12552. https://doi.org/10.1002/emp2.12552