Figure 1
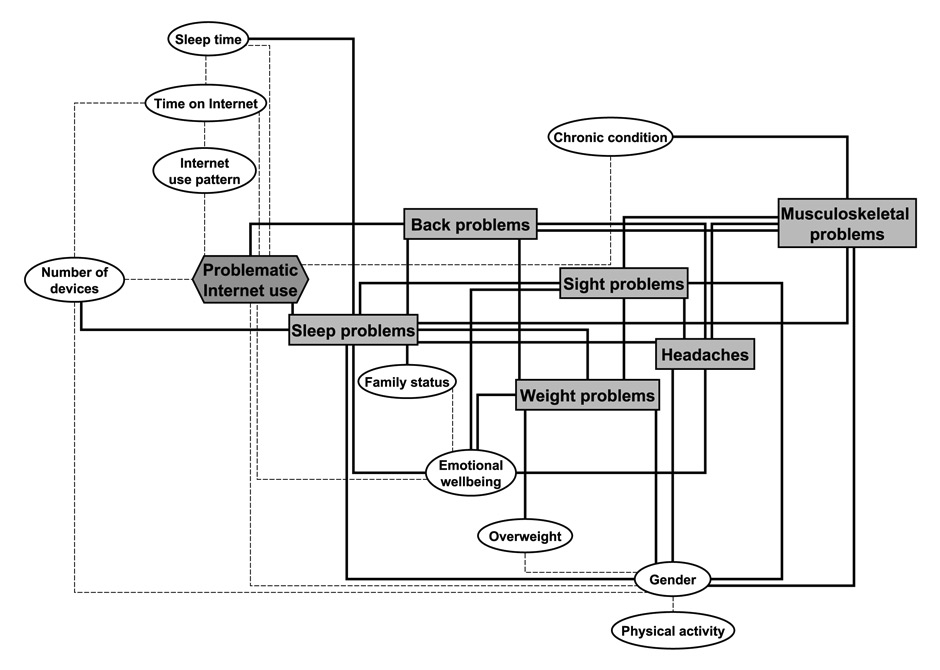
Log-linear model representing the associations between significant variables.
DOI: https://doi.org/10.4414/smw.2014.14061
Internet use has become part of adolescents’ lives, to the point that a young person not using this tool is exceptional. Since the advent of generalised internet use, scholars have been interested in assessing its impact on adolescent health. However, most studies have focused on mental health [1–6] and unhealthy behaviours (such as substance use or sedentary behaviour) [1, 4]. Furthermore, research on the effects of excessive internet use on health mostly relate to overweight/obesity [7–10] and lack of sleep [3, 7, 9, 11].
In fact very few studies on the relationship between youths’ internet use and somatic complaints have been carried out, and the literature seems to indicate that excessive internet use has a negative effect on health. Hakala et al. [12] reported an association between increased internet use and neck-shoulder and low back pain, as well as headaches [13]. In previous research based on a Swiss national survey carried out in 2002, Bélanger et al. [14] described a U-shaped association between the amount of internet use and somatic complaints, with occasional and heavy internet users reporting more complaints than regular users. Finally, in a qualitative study, college students [15] indicated eyesight deterioration, sleep deprivation, fatigue and sore shoulders, back, hands and fingers as negative consequences of internet use.
Moreover, little is known about the association between excessive internet use and health taking into account the type of activity performed on the internet. Nowadays, time online cannot be computed as a whole as youths are increasingly required to use the internet for their schoolwork. For this reason, there is a need to differentiate between time spent on the internet for schoolwork and for leisure. It could thus be hypothesised that those using the internet mainly for leisure (compared to those using it mainly for schoolwork) would potentially have more health complaints.
The objective of this research is to assess whether problematic internet use is associated with somatic complaints and whether this association remains when checking for internet activity among a random sample of adolescents living in the canton of Vaud, Switzerland.
Data were drawn from the ado@internet.ch study, a longitudinal study of a representative sample of 35 schools in the canton of Vaud, in the French-speaking part of Switzerland. In this paper only cross-sectional baseline data are discussed. All 8th graders in each school were invited to participate (n = 3,367). Among them, 230 were absent the day the questionnaire was administered, 60 refused to participate and 10 did not complete the questionnaire correctly and were excluded, for a final sample of 3,067 youths (50.3% females). Data were collected between 23 April and 4 July 2012 (spring quarter in Swiss schools). The questionnaire contained 51 questions and was filled in online in the schools’ computer science rooms. Participating schools were offered the option to have their students fill in the questionnaire under the supervision of a trained research assistant external to the school system, and 21 of the 35 schools (1,939 students) accepted (while the rest of the schools chose supervision by their teachers). There were no significant differences in participants’ age, gender, main socio-demographic variables, problematic internet use or any of the studied health problems when comparing schools requesting a research assistant and those doing it on their own (data not shown).
To assess internet overuse we used the French version of the Internet Addiction Test (IAT) [16], which is widely used, valid and reliable with adolescent populations [17, 18]. The test consists of 20 items (such as “How often do you find that you stay online longer than you intended?” or “How often do you try to hide how long you’ve been online?”) with possible answers ranging from 1 (rarely) to 5 (always). A ‘0’ (does not apply) option is also available. The maximum score is 100, with higher scores indicating a greater level of problematic use. The instrument showed a good internal consistency with a Cronbach alpha coefficient of .89, similar to other studies [17, 19].
As described in the literature [17], we divided our sample into average online users (IAT<50; n = 2,704, 88.2%), frequent problem users (IAT ≥50–79; n = 346, 11.3%) and significant problem users (IAT ≥80; n = 17, 0.6%). Due to the small number of cases in the significant problem users category, we combined it with frequent problem users to create the problematic user category (n = 363; 11.8%), as previously done [20].
We analysed six somatic health problems: back pain, weight problems, headaches, musculoskeletal pain, sleep problems, and sight problems. Each health problem had five possible answers dichotomised as at least weekly (at least once a week, most days) and other (never, less than monthly, about once a month).
We checked for several potential confounding factors described in the literature as being related to excessive internet use and/or health problems, such as age [21], gender [22], residence (rural/urban) [1, 23], migrant status (Swiss-born/other) [24], family structure (parents together/other) [1, 22], socioeconomic status (SES) [1, 25], physical activity [1, 26], being overweight [4, 10, 14, 27], sleep deprivation [3, 4, 14], suffering from a chronic condition [28], emotional wellbeing [29], and amount of time online [22].
For SES, we used the question of the European School Project on Alcohol and Other Drugs (ESPAD) survey ( http://www.espad.org ) that reads “Compared to other families in Switzerland, you think that the financial situation of your family is…” with seven possible answers grouped as follows: very well/well above average, above average, average and below average (including below, well below and much below average). Physical activity was determined as the number of days per week performing a physical activity lasting at least 60 minutes. Body mass index (BMI) was calculated from self-reported height and weight and we used the standards published by Cole et al. [30] to define overweight and obesity. The variable was subsequently dichotomised into overweight/obesity and other. Sleep deprivation was measured as self-reported mean hours of sleep on schooldays. Participants were asked if they were suffering from a chronic condition, defined as “A condition lasting more than one year and requiring regular care, such as asthma, diabetes, scoliosis, etc.” To measure emotional wellbeing, we used the World Health Organization Five Well-Being Index (WHO-5), with a score below 13 indicating poor well-being [31]. Amount of time online when connected was divided into four categories: less than 2 hours, 2–<3 hours, 3–<4 hours, and 4 hours or more.
Finally, we also checked for activity performed on the internet. Participants were asked how much of their Internet time was used for schoolwork and for leisure on schooldays with five possible answers to each of the two questions: most of the time, more than half of the time, about the same time, less than half of the time, and almost no time. Based on the responses, the main activity on the internet variable was created with three categories: for schoolwork mainly, similarly for both, for leisure mainly. As adolescents are known to be media multitaskers [32], we also controlled the number of devices used to connect to the Internet, with six possible answers: console, computer, smartphone, tablet, television, and other. Responses were dichotomised into one or two devices and more than two devices, as done by others [33].
We first performed a bivariate analysis comparing the two groups derived from the IAT for each variable. We used student’s t-test for continuous variables and chi-square test for categorical variables. Subsequently all statistically significant variables (plus age) at the bivariate level were included in independent logistic regressions (one for each health problem) with average users being the reference category. Additionally, a logistic regression including all health problems was also performed. Finally, we ran a log-linear model to determine the overall structure of association between all of our variables of interest. On the basis of preliminary computations, we chose to start with a model including all bivariate relations. Unnecessary relations were then removed one by one using the Bayesian Information Criterion. The final model therefore represents the minimal set of associations required to accurately describe the complex relationships among the whole set of variables. All calculations were done with STATA 13.0 (StataCorp, College Station, Texas) except for the log-linear model which was computed using the R environment. The study was approved by the ethics committee of the canton of Vaud.
| Table 1: Bivariate analysis comparing average and problematic internet users. | |||
| Average users (n = 2708) | Problematic users (n = 359) | p-value | |
| Mean age (±SE) | 14.23 ± 0.01 | 14.29 ± 0.04 | NS |
| Gender (female) | 49.3% | 57.6% | <0.01 |
| Nationality (Swiss) | 85.8% | 82.5% | NS |
| Residence (urban) | 46.9% | 50.6% | NS |
| Family status (parents together) | 68.7% | 62.2% | <0.05 |
| Socioeconomic status | NS | ||
| Well/very above average | 11.0% | 10.9% | |
| Above average | 26.2% | 26.2% | |
| Average | 56.7% | 53.8% | |
| Below average | 6.1% | 9.1% | |
| Physical activity (mean days/week) | 3.29 ± 0.04 | 2.76 ± 0.10 | <0.001 |
| Devices to connect to Internet (>2) | 40.3% | 58.9% | <0.001 |
| Hours per day on Internet | <0.001 | ||
| <2 hours | 71.9% | 33.8% | |
| 2‒<3 hours | 16.2% | 20.9% | |
| 3‒<4 hours | 6.8% | 15.2% | |
| 4 hours or more | 5.1% | 30.1% | |
| Main internet use pattern | <0.001 | ||
| For school/work mainly | 18.3% | 6.5% | |
| Similarly for both | 16.9% | 13.5% | |
| For leisure mainly | 64.8% | 80.0% | |
| Average sleeping hours (schooldays) | 8.13 ± 0.02 | 7.37 ± 0.07 | <0.001 |
| Overweight (yes) | 10.5% | 15.9% | <0.01 |
| Emotional wellbeing (poor) | 13.6% | 30.0% | <0.001 |
| Having a chronic condition (yes) | 12.2% | 19.2% | <.01 |
| Back problems | 12.9% | 23.7% | <0.001 |
| Weight problems | 4.7% | 11.8% | <0.001 |
| Headaches | 15.3% | 27.2% | <.001 |
| Musculoskeletal problems | 20.3% | 31.7% | <.001 |
| Sleep problems | 25.9% | 55.2% | <.001 |
| Sight problems | 12.2% | 22.0% | <.001 |
At the bivariate level there were no age differences between groups, but females were significantly more represented among problematic users. Problematic users were also less likely to live with both parents. The average number of days per week doing physical activity was lower in the problematic users group than in the average users group. The two groups also differed on the number of devices to connect to the internet, the amount of time spent on the internet and the main activity performed on it, with problematic users using it mostly for leisure. On average, problematic users slept almost one hour less on schooldays than regular users. Finally, prevalence rates of overweight, poor emotional wellbeing and chronic conditions were higher in the problematic use group. In the same line, all health problems also showed higher prevalence rates among problematic users (table 1).
Figure 1
Log-linear model representing the associations between significant variables.
At the multivariate level (table 2), problematic users were more than twice as likely to suffer from sleep problems, 74% more likely to suffer from weight problems and between 30% and 50% more likely to suffer from musculoskeletal and back problems. In the same line, they were 58% more likely to suffer from a chronic condition. After checking for significant variables, headaches and sight problems did not remain statistically associated with problematic internet use. When including all health problems in the same logistic regression, sleep problems were the only health complaint that remained statistically significant (table 3).
The different associations can be seen more clearly in the log-linear model (fig. 1). Problematic internet use was linked both to sleep problems and back problems, and sleep problems were also related to number of devices. Additionally, both gender and emotional wellbeing were connected to most health problems.
| Table 2:Multivariate analysis for each health problem individually using average users as the reference group*. | ||
| Problematic users | p-value | |
| Chronic condition** | 1.58 [1.11:2.23] | 0.011 |
| Back problems | 1.46 [1.04:2.05] | 0.029 |
| Weight problems | 1.74 [1.03:2.93] | 0.037 |
| Headaches | 1.33 [0.96:1.85] | NS |
| Musculoskeletal problems | 1.36 [1.00:1.84] | 0.048 |
| Sleep problems | 2.16 [1.62:2.88] | <0.001 |
| Sight problems | 1.15 [0.80:1.66] | NS |
| *Controlling for age, gender, family status, physical activity, main internet use pattern, number of devices to access Internet, daily time on Internet, wellbeing, having a chronic illness, being overweight and average hours of sleep on schooldays. **Controlling for age, gender, family status, physical activity, main internet use pattern, number of devices to access internet, daily time on internet, wellbeing, being overweight and average hours of sleep on schooldays. | ||
| Table 3: Multivariate analysis including all the health problems at the same time using average users as the reference group*. | ||
| Problematic users | p-value | |
| Back problems | 1.23 [0.85:1.77] | NS |
| Weight problems | 1.48 [0.86:2.53] | NS |
| Headaches | 1.07 [0.75:1.51] | NS |
| Musculoskeletal problems | 1.09 [0.79:1.51] | NS |
| Sleep problems | 2.03 [1.50:2.74] | <0.001 |
| Sight problems | 0.97 [0.66:1.42] | NS |
| *Controlling for age, gender, family status, physical activity, main internet use pattern, number of devices to access internet, daily time on internet, wellbeing, having a chronic illness, being overweight and average hours of sleep on schooldays. | ||
Overall, 11.2% of our sample was moderately and 0.6% severely addicted to the internet. These prevalence rates are similar to [34] or slightly higher than [35] those reported in the literature using the same instrument. It is however, worth noting that contrary to what has been mainly described by other researchers [22, 34, 36], the prevalence of problematic internet use in our study was higher among females. Park [37] also found a higher prevalence among females and hypothesised that it could be related to Internet activities mostly used by females such as social networks. The fact that we included school-related internet activities could explain this finding, as the literature indicates that heavy internet female users favouring information seeking and chatting report a better academic performance than non-heavy users and males [38]. Another hypothesis could be that, as it has been observed with risk behaviours such as smoking [39], there may be a changing trend with adolescent girls becoming more internet-addicted than males. Further studies are needed to investigate this result more in-depth.
Problematic internet use is also associated with suffering from a chronic condition and this is independent of gender. Previous studies carried out in Switzerland [14, 28] reported similar results but for females only. However, to date this relationship has been seldom studied and deserves a more in-depth analysis.
In line with previous results, both backache [12, 13, 15] and musculoskeletal pain [12, 13, 15, 40] were associated with problematic internet use in our study, even though other studies [14] found no such associations. Similarly, the association between internet use and headaches is not conclusive, with some authors reporting a relationship [13] and others none [14]. In our case, although the difference was clear in the bivariate analysis, it did not remain significant when allowing for confounding variables. Similarly, eyesight deterioration has been described as one of the main negative impacts of excessive internet use [13, 15] but our results did not support it. As is the case for headaches, the multivariate analysis does not confirm the bivariate findings. One explanation to these inconsistent findings reported in the literature could be the diverse instruments and cut-off points used in the different studies.
Our results show that problematic internet use is related to some somatic complaints even after controlling for potential confounders. This is in agreement with previous research [1, 9, 40] reporting that increasing time on internet is related to poorer perceived health overall and to health complaints [40]. Our results also confirm our hypothesis that the association between internet use and poor perceived health is more important when adolescents mostly devote their time online to leisure activities.
Problematic internet users are over twice more likely to report sleep problems. Internet overuse has been associated with less hours of sleep [9, 11, 15, 36] and excessive daytime sleepiness [4, 36] or insomnia [3]. A previous Swiss study [14] also found that high internet users did not sleep enough, but only for adolescent girls. The fact that problematic users have access to the internet through numerous devices could be associated with a higher probability of internet access at any time and any place (even when in bed) without parental control and less hours of sleep. Several authors [33, 41] have also found that having devices in the bedroom was associated with sleep-related problems. As sleep problems are directly related to all other health problems in the log-linear model and are the only health problem that remains significant when all others problems are included in the multivariate analysis, it could be assumed, as described by Punamäki et al. [40], that poor perceived health and health complaints could be mediated by poor sleeping habits.
The main strengths of our study are that it is based on a large representative sample, the use of a widely recognised tool to measure problematic internet use and the control for potential confounders in the analyses. However, some limitations need to be mentioned. First, the cross-sectional nature of the study does not allow drawing conclusions about causal relationships. Second, a response bias cannot be precluded as the questionnaire was self-reported. Third, as adolescents are media multitaskers, it may be difficult for them to differentiate between school and leisure internet time. However, the fact that we controlled for the number of devices to connect to the internet (as a proxy for multitasking) and that we did not ask them what they spent their time on but rather most of their time, should minimise this bias.
Our results confirm that problematic internet users more frequently report health problems, even after controlling for confounding factors. Among those, lack of sleep is the most strongly associated and seems to influence the other ones.
Clinicians dealing with adolescents should remember to screen any patient complaining of sleep-related problems, back or musculoskeletal pain or weight problems for excessive internet use. Clinicians can also play an important role in parental guidance regarding the limitation of time their adolescent children can spend online for leisure activities. Furthermore, advising parents to limit the number of devices used to connect to the internet, mainly those that can be kept in their adolescent’s room could help warrant enough sleeping time.
1 Kim JY. The nonlinear association between Internet using time for non-educational purposes and adolescent health. Journal of preventive medicine and public health = Yebang Uihakhoe chi. 2012;45(1):37–46.
2 Cao F, Su L. Internet addiction among Chinese adolescents: prevalence and psychological features. Child Care Health Dev. 2007;33(3):275–81.
3 Cheung LM, Wong WS. The effects of insomnia and internet addiction on depression in Hong Kong Chinese adolescents: an exploratory cross-sectional analysis. J Sleep Res. 2011;20(2):311–7.
4 Kim JH, Lau CH, Cheuk KK, Kan P, Hui HL, Griffiths SM. Brief report: Predictors of heavy Internet use and associations with health-promoting and health risk behaviors among Hong Kong university students. J Adolesc. 2010;33(1):215–20.
5 Liu TC, Desai RA, Krishnan-Sarin S, Cavallo DA, Potenza MN. Problematic Internet use and health in adolescents: data from a high school survey in Connecticut. J Clin Psychiatry. 2011;72(6):836–45.
6 Morrison CM, Gore H. The relationship between excessive Internet use and depression: a questionnaire-based study of 1,319 young people and adults. Psychopathology. 2010;43(2):121–6.
7 Berkey CS, Rockett HR, Colditz GA. Weight gain in older adolescent females: the internet, sleep, coffee, and alcohol. J Pediatr. 2008;153(5):635–9, 9 e1.
8 Burke V, Beilin LJ, Durkin K, Stritzke WG, Houghton S, Cameron CA. Television, computer use, physical activity, diet and fatness in Australian adolescents. Int J Pediatr Obes. 2006;1(4):248–55.
9 Do YK, Shin E, Bautista MA, Foo K. The associations between self-reported sleep duration and adolescent health outcomes: what is the role of time spent on Internet use? Sleep medicine. 2013;14(2):195–200.
10 Russ SA, Larson K, Franke TM, Halfon N. Associations between media use and health in US children. Academic pediatrics. 2009;9(5):300–6.
11 Yen CF, Ko CH, Yen JY, Cheng CP. The multidimensional correlates associated with short nocturnal sleep duration and subjective insomnia among Taiwanese adolescents. Sleep. 2008;31(11):1515–25.
12 Hakala PT, Rimpela AH, Saarni LA, Salminen JJ. Frequent computer-related activities increase the risk of neck-shoulder and low back pain in adolescents. Eur J Public Health. 2006;16(5):536–41.
13 Hakala PT, Saarni LA, Punamaki RL, Wallenius MA, Nygard CH, Rimpela AH. Musculoskeletal symptoms and computer use among Finnish adolescents – pain intensity and inconvenience to everyday life: a cross-sectional study. BMC musculoskeletal disorders. 2012;13:41.
14 Belanger RE, Akre C, Berchtold A, Michaud PA. A U-shaped association between intensity of Internet use and adolescent health. Pediatrics. 2011;127(2):e330–5.
15 Chou C. Internet heavy use and addiction among Taiwanese college students: an online interview study. Cyberpsychol Behav. 2001;4(5):573–85.
16 Khazaal Y, Billieux J, Thorens G, Khan R, Louati Y, Scarlatti E, et al. French validation of the internet addiction test. Cyberpsychol Behav. 2008;11(6):703–6.
17 Sinkkonen HM, Puhakka H, Merilainen M. Internet use and addiction among Finnish adolescents (15–19 years). J Adolesc. 2014;37(2):123–31.
18 Lai CM, Mak KK, Watanabe H, Ang RP, Pang JS, Ho RC. Psychometric properties of the internet addiction test in Chinese adolescents. J Pediatr Psychol. 2013;38(7):794–807.
19 Cao H, Sun Y, Wan Y, Hao J, Tao F. Problematic Internet use in Chinese adolescents and its relation to psychosomatic symptoms and life satisfaction. BMC public health. 2011;11:802.
20 Lam LT, Peng Z, Mai J, Jing J. The association between internet addiction and self-injurious behaviour among adolescents. Injury prevention: journal of the International Society for Child and Adolescent Injury Prevention. 2009;15(6):403–8.
21 Mejia D, Berchtold A, Belanger RE, Kuntsche EN, Michaud PA, Suris JC. Frequency and effects of meeting health behaviour guidelines among adolescents. Eur J Public Health. 2013;23(1):8–13.
22 Durkee T, Kaess M, Carli V, Parzer P, Wasserman C, Floderus B, et al. Prevalence of pathological internet use among adolescents in Europe: demographic and social factors. Addiction. 2012 May 23.
23 Yen CF, Ko CH, Yen JY, Chang YP, Cheng CP. Multi-dimensional discriminative factors for Internet addiction among adolescents regarding gender and age. Psychiatry Clin Neurosci. 2009;63(3):357–64.
24 Bonfadelli H, Bucher P, Piga A. Use of old and new media by ethnic minority youth in Europe with a special emphasis on Switzerland. 2007;Communications(32):141–70.
25 Sun P, Unger JB, Palmer PH, Gallaher P, Chou CP, Baezconde-Garbanati L, et al. Internet accessibility and usage among urban adolescents in Southern California: implications for web-based health research. Cyberpsychol Behav. 2005;8(5):441–53.
26 Melkevik O, Torsheim T, Iannotti RJ, Wold B. Is spending time in screen-based sedentary behaviors associated with less physical activity: a cross national investigation. Int J Behav Nutr Phys Act. 2010;7:46.
27 Barnett TA, O’Loughlin J, Sabiston CM, Karp I, Belanger M, Van Hulst A, et al. Teens and screens: the influence of screen time on adiposity in adolescents. Am J Epidemiol. 2010;172(3):255–62.
28 Suris JC, Akre C, Berchtold A, Belanger RE, Michaud PA. Chronically connected? Internet use among adolescents with chronic conditions. J Adolesc Health. 2010;46(2):200–2.
29 van der Aa N, Overbeek G, Engels RC, Scholte RH, Meerkerk GJ, Van den Eijnden RJ. Daily and compulsive internet use and well-being in adolescence: a diathesis-stress model based on big five personality traits. J Youth Adolesc. 2009;38(6):765–76.
30 Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320(7244):1240–3.
31 Moller Leimkuhler AM, Heller J, Paulus NC. Subjective well-being and “male depression” in male adolescents. JAffectDisord. 2007;98(1–2):65–72.
32 Pea R, Nass C, Meheula L, Rance M, Kumar A, Bamford H, et al. Media use, face-to-face communication, media multitasking, and social well-being among 8– to 12–year-old girls. Dev Psychol. 2012;48(2):327–36.
33 Chahal H, Fung C, Kuhle S, Veugelers PJ. Availability and night-time use of electronic entertainment and communication devices are associated with short sleep duration and obesity among Canadian children. Pediatric obesity. 2013;8(1):42–51.
34 Lam LT, Peng ZW, Mai JC, Jing J. Factors associated with Internet addiction among adolescents. Cyberpsychology & behavior: the impact of the Internet, multimedia and virtual reality on behavior and society. 2009;12(5):551–5.
35 Lam LT, Peng ZW. Effect of pathological use of the internet on adolescent mental health: a prospective study. Arch Pediatr Adolesc Med. 2010;164(10):901–6.
36 Choi K, Son H, Park M, Han J, Kim K, Lee B, et al. Internet overuse and excessive daytime sleepiness in adolescents. Psychiatry Clin Neurosci. 2009;63(4):455–62.
37 Park S. The association between Internet use and depressive symptoms among South Korean adolescents. Journal for specialists in pediatric nursing: JSPN. 2009;14(4):230–8.
38 Chen SY, Tzeng JY. College female and male heavy internet users’ profiles of practices and their academic grades and psychosocial adjustment. Cyberpsychology, behavior and social networking. 2010;13(3):257–62.
39 Ariza C, Nebot M, Tomas Z, Gimenez E, Valmayor S, Tarilonte V, et al. Longitudinal effects of the European smoking prevention framework approach (ESFA) project in Spanish adolescents. Eur J Public Health. 2008;18(5):491–7.
40 Punamaki RL, Wallenius M, Nygard CH, Saarni L, Rimpela A. Use of information and communication technology (ICT) and perceived health in adolescence: the role of sleeping habits and waking-time tiredness. J Adolesc. 2007;30(4):569–85.
41 Shochat T, Flint-Bretler O, Tzischinsky O. Sleep patterns, electronic media exposure and daytime sleep-related behaviours among Israeli adolescents. Acta Paediatr. 2010;99(9):1396–400.
Funding / potential competing interests: The ado@internet.ch study has been financed by the Service of Public Health of the canton of Vaud and by the Swiss National Science Foundation (FNS 105319_140354). The funding bodies had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript. No other potential conflict of interest relevant to this article was reported.