Late removal of retrievable caval filters
DOI: https://doi.org/10.4414/smw.2014.14022
Ludwig
von Segesser, Enrico
Ferrari, Piergiorgio
Tozzi, Saad
Abdel-Sayed, Denis
Berdajs
Summary
The advent of retrievable caval filters was a game changer in the sense, that the previously irreversible act of implanting a medical device into the main venous blood stream of the body requiring careful evaluation of the pros and cons prior to execution suddenly became a “reversible“ procedure where potential hazards in the late future of the patient lost most of their weight at the time of decision making. This review was designed to assess the rate of success with late retrieval of so called retrievable caval filters in order to get some indication about reasonable implant duration with respect to relatively “easy“ implant removal with conventional means, i.e., catheters, hooks and lassos. A PubMed search ( http://www.pubmed.gov ) was performed with the search term „cava filter retrieval after 30 days clinical“, and 20 reports between 1994 and 2013 dealing with late retrieval of caval filters were identified, covering approximately 7,000 devices with 600 removed filters. The maximal duration of implant reported is 2,599 days and the maximal implant duration of removed filters is also 2,599 days. The maximal duration reported with standard retrieval techniques, i.e., catheter, hook and/or lasso, is 475 days, whereas for the retrievals after this period more sophisticated techniques including lasers, etc. were required. The maximal implant duration for series with 100% retrieval accounts for 84 days, which is equivalent to 12 weeks or almost 3 months. We conclude that retrievable caval filters often become permanent despite the initial decision of temporary use. However, such “forgotten“ retrievable devices can still be removed with a great chance of success up to three months after implantation. Conventional percutaneous removal techniques may be sufficient up to sixteen months after implantation whereas more sophisticated catheter techniques have been shown to be successful up to 83 months or more than seven years of implant duration. Tilting, migrating, or misplaced devices should be removed early on, and replaced if indicated with a device which is both, efficient and retrievable.
Introduction
The main indications for implantation of a caval filter (fig. 1) in the presence of proven venous thrombo-emboli include A) recurrent pulmonary emboli despite efficient anticoagulation B) contra-indication of anticoagulation in the presence of pulmonary emboli C) complication of anticoagulation D) inability to achieve or maintain adequate anticoagulation [1]. However, the indications are only part of the parameters of the equation about the usefulness of caval filtration in a specific patient. As a matter of fact, and based on our own experience, there are also a number of concerns related to the caval filters themselves including filter dislodgement, filter penetration, filter fracture, venous thrombo-embolic events originating from the caval filter, complete thrombosis of the vena cava related to the caval filter, etc. Hence, the advent of retrievable caval filters in the sixties of the last century [2] was a game changer in the sense, that the previously irreversible act of implanting a medical device into the main venous blood stream of the body requiring careful evaluation of the pros and cons prior to execution suddenly became a “reversible“ procedure where potential hazards in the late future of the patient lost most of their weight at the time of decision making. This does not mean that late problems related to caval filters vanished [3, 4]. As a matter of fact it turned out in our clinical practice that so-called retrievable caval filters typically designed and approved for use for two or three weeks (less than 30 days) were often left in situ and thus became permanent. It is only at the occasion of complications or new health problems that the retrieval of the originally temporary caval filter was reconsidered, and sometimes attempted. The present review was designed to assess the rate of success with late retrieval of so called retrievable caval filters in order to get some indication about reasonable implant duration with respect to relatively “easy“ implant removal with conventional means, i.e., catheters, hooks and lassos.
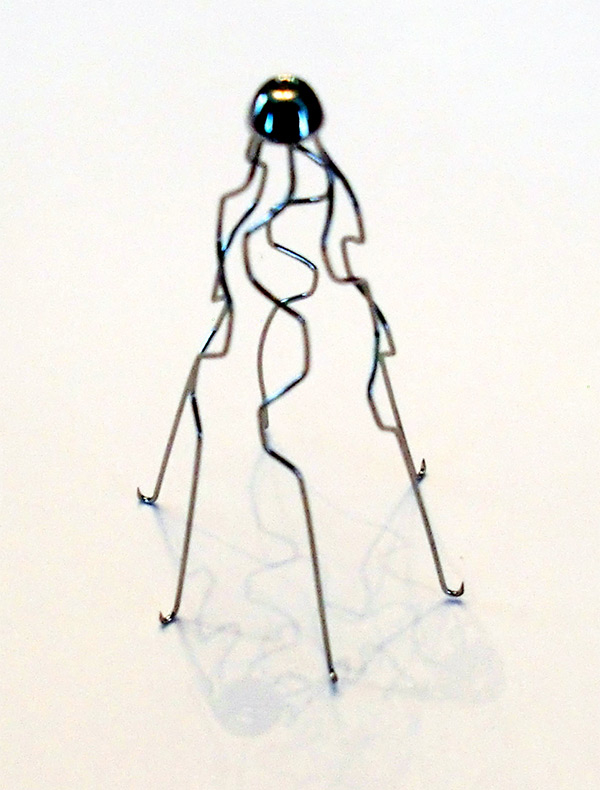
Figure 1
Original Greenfield vena cava filter (catalog no. 2846). This device was designed for permanent implantation including sharp hooks at the bottom to prevent migration. In contrast, retrievable caval filters have a hook or a graspable area at the tip that allows for traction and refolding into a sheath.
Search strategy
In order to assess the rate of success with late retrieval of temporary caval filters, a PubMed search ( http://www.pubmed.gov ) was performed on 13 October 2013, with the search term “cava filter retrieval after 30 days clinical“. This search term was based on the rational that the most frequent venous filter deployment site is the inferior vena cava, that the retrievable caval filters are typically designed for an implant duration of 15 ± 10 days, and that the 30 days implant interval is a regulatory hurdle with less stringent criteria for medical devices designed for less than 30 days implant duration.
Results
The search described above identified 20 reports between 1994 and 2013 dealing with late retrieval of caval filters. The 15 reports providing sufficiently detailed information about the number of implants, the filter position, the mean and/or range of implant duration, the proportion of successfully removed filters, and the number of not removed filters with the reason for failure if available are shown in table 1. This compilation covers approximately 7,000 devices. The total number of removed filters in table 1 accounts for 600 devices. The maximal duration of implant reported is 2,599 days and the maximal implant duration of removed filters is also 2,599 days. The maximal duration reported with standard retrieval techniques, i.e., catheter, hook and/or lasso, is 475 days, whereas for the retrievals after this period more sophisticated techniques including lasers etc. were required. The key problem in failure to remove retrievable caval filters appears to be the position of the filter tip or key filter part designed for re-folding the device. We can tell from our experience, that tips of tilted filters tend to sink into the caval wall and can become overgrown, thus making capture difficult. The maximal implant duration for series with 100% retrieval (fig. 2) accounts for 84 days, which is equivalent to 12 weeks or almost 3 months (table 2).
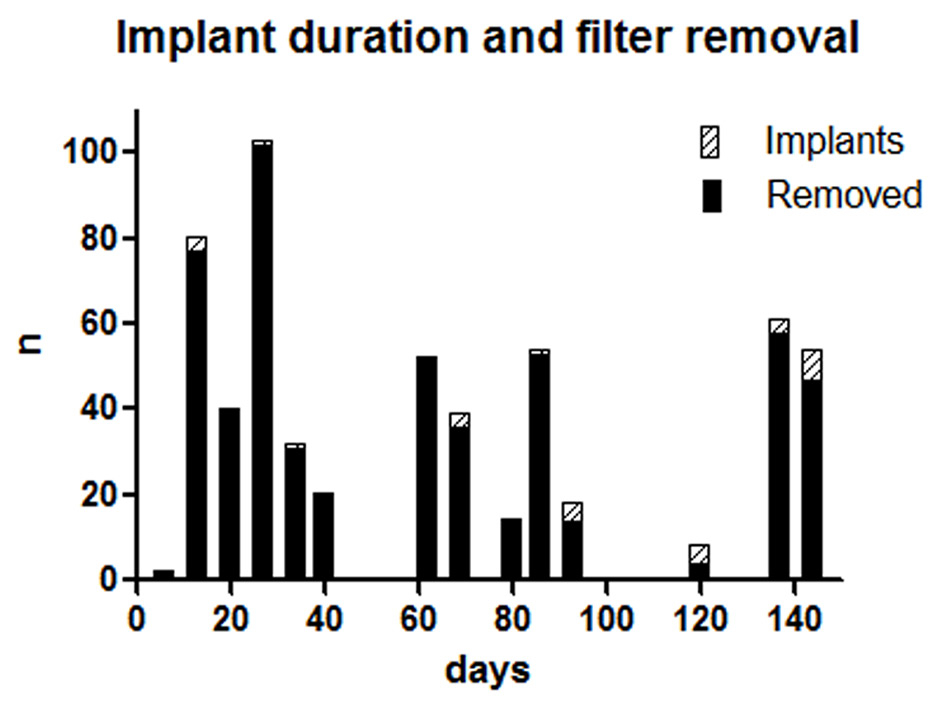
Figure 2
Proportion of filters removed over time. It is interesting to note, that up to 84 days, 100% filter removal can be obtained by conventional means (hooks and lassos).
In our experience, there are many good reasons for postponing early removal of retrievable caval filters including patent foramen ovale and/or other intra-cardiac right to left shunts, presence of clot within the caval filter at the time of planned removal, unresolved deep vein thrombosis, persistent pulmonary hypertension, persistent respiratory insufficiency, unstable anticoagulation and others.
|
Table 1: Main findings for duration and success of removal with various filter types. |
|
Reference
|
Year published
|
Author
|
Filter brand
|
No. devices
|
Position
|
Duration Mean
|
Range
|
Removed
|
Not removed
|
| |
|
|
|
|
|
days |
|
days |
cause |
| 5 |
2013 |
Smouse HB |
Crux |
54 |
Cava |
84.6 ± 57.6 |
6–190 |
53/54 |
1 remained |
| 6 |
2013 |
Kuo WT |
X |
50 |
Cava |
815 |
|
20–2599 50/50 |
fractures > 1y |
| 7 |
2011 |
Van Ha TG |
X |
20 |
Iliac |
40±10 |
30–71 |
all |
none |
| 8 |
2011 |
Angel LF |
X |
6,834 |
Cava |
NA |
|
NA |
no superior design |
| 9 |
2010 |
Johnson MS |
Option |
39 |
Cava |
67 |
1–175 |
36/39 |
3 remained |
| 10 |
2009 |
Binkert CA |
G2 |
61 |
Cava |
140 |
5–300 |
58/61 |
3 tip at wall |
| 11 |
2009 |
Sangwaiya MJ |
Celect |
14 |
Cava |
84 |
6–190 |
14/14 |
none |
| 12 |
2007 |
Yamagami T |
Gunther |
80 |
Cava |
13.4 ± 4.2 |
NA |
77/80 |
3 remained |
| 13 |
2007 |
Piano G |
Bard/Gu |
52 |
Cava |
63 ± 30 |
NA |
52/52 |
8 refused |
| 14 |
2006 |
Bovin G |
Tempo |
103 |
Cava |
29.5 ± 14 |
2–86 |
102/103 |
none <84 d |
| 15 |
2006 |
Stefanidis D |
X |
54 |
Cava |
142 |
17–475 |
47/54 |
1 strut fracture |
| 16 |
2006 |
De Gregorio M |
Gunther |
32 |
Cava |
30 |
NA |
31/32 |
1 force > 9.8N |
| 17 |
2005 |
Rosenthal D |
OptEase |
40 |
Cava |
16.4 ± 7.2 |
3–48 |
40/40 |
none |
| 18 |
2005 |
Imberti D |
ALN |
18 |
Cava |
<3 months |
|
14/18 |
|
| |
|
|
|
8 |
Cava |
>3 months |
|
4/8 |
|
| 19 |
1994 |
Nakagawa |
Nitinol |
2 |
Cava |
6 |
5–7 |
2/2 |
none |
|
Table 2: Main findings. |
| Number of reports |
15 reports |
| Period of reports |
1994 and 2013 |
| Number of devices covered |
7,000 devices |
| Total number of removed filters |
600 devices |
| Maximal implant duration |
2,599 days |
| Maximal implant duration of removed filters |
2,599 days |
| Maximal implant duration with standard retrieval |
475 days |
| Maximal implant duration with 100% retrieval |
84 days = 12 weeks <3 months |
Discussion
The most striking finding of this review is the fact, that retrievable caval filters designed for temporary caval filtration of two or three weeks (less than 30 days) have been successfully removed in all cases where this was attempted, in several series [6, 7, 11, 13, 14] as many as 12 weeks after insertion. This includes Celect, Bard, Gunther, Tempo and other filter brands. Although this does not mean that the caval filters designed for short term use should be implanted routinely for long term use, it is extremely helpful for clinical practice to know, that the regulatory threshold of 30 days for temporary caval filtration by the means of a retrievable caval filter is not written in stone for clinical reasons. There can be no doubt, that temporary caval filtration of three weeks which may be extended to almost three months without compromising the rate of removal reduces the pressure of too early a removal of the intra-caval device, when this may still be required, or the removal process is contra-indicated at a specific moment for some other reason [20], provided that the device considered is designed for longer term use or later conversion to a non-filtering device.
Interestingly enough, there are other devices, that are left in the vena cava for some time and are therefore designed to be removed sooner or later, like intravascular gas exchangers [21] built for temporary extra-pulmonary gas transfer, which can be removed by simple traction after more than 28 days [22], venous cannulas used for extra-corporeal membrane oxygenation including collapsible designs, which can also be removed by simple traction after as many as 28 days [23–25]. In contrast, permanent implants in the vena cava like catheters connected to valves or ports, pace maker leads, as well as defibrillator leads can become very difficult for late removal in toto and may require special expertise as well as specific instrumentation including lasers, threaded stylets, cutting sheaths, etc.
These more complex removal procedures bring us to the second important finding of this review. As a matter of fact, even caval filters implanted for 2,599 days can be removed without open surgery but with specific trans-luminal techniques after this period of indwelling, whereas standard retrieval techniques may still work after an implant duration of up to 475 days (table 2).
There are a number of additional observations listed in table 1 which deserve to be highlighted. The review of Angel LF covered 6,834 implants of multiple brands, but did not reveal a markedly superior design. Two reports with smaller series mentioned strut fractures [6, 15]. The latter can migrate and may require surgical removal under certain circumstances. One key reason for problems with the removal of retrievable caval filters appears to be the position of the filter tip or key filter part designed for re-folding the device. The latter can be difficult to capture if it adheres to the venous wall [10] a situation which is favoured if the filter is tilted with reference to the caval axis. In such a situation the point of traction designed for capture by the retrieval device (typically a hook) may be flush to the caval wall, or even hidden in intramural fashion. With a tilted device, even the approach with a lasso from the other side, may be difficult or impossible and therefore it may not be possible to be snared and reloaded into a sheath. It is a fact that stent arms and arches driven by excessive expansion force (e.g., due to expansion in tilted position) lead to more media atrophy with intimal overgrowth [25], can penetrate the basal membrane of the endothelium, and the adventitia, and thus it can be impossible to grab the specific point of traction designed for device refolding prior to re-loading into a catheter. Hence, the indication to consider earlier retrieval of tilted retrievable caval filters where overgrowth of the key components designed for device collapsing are risking success with standard retrieval techniques, and to avoid more complex interventions including open surgery.
We conclude that retrievable caval filters often become permanent. However, such ”forgotten“ retrievable devices can still be removed by conventional catheter techniques with a great chance of success up to three months after implantation. Conventional percutaneous removal techniques may be sufficient up to sixteen months after implantation whereas more sophisticated catheter techniques have been shown to be successful up to 83 months or more than seven years of implant duration. Tilting, migrating, or misplaced devices should be removed early on, and replaced if indicated with a device which is both, efficient and retrievable. Our preference goes for retrievable or convertible temporary caval filters designed for optional permanent implantation.
References
1 Kaufman JA, MD, Kinney TB, MD, Streiff MB, MD, Sing RF, DO, Proctor MC, MS, Becker D, MD, MPH, et al. Guidelines for the Use of Retrievable and Convertible Vena Cava Filters: Report from the Society of Interventional Radiology Multidisciplinary Consensus Conference. J Vasc Interv Radiol. 2006;17:449–59
2 Williams R, Schenk W. A removable intracaval filter for prevention of pulmonary embolism: early experience with the use of the Eichelter catheter in patients. Surgery. 1970;68:999–1008.
3 Angel LF, Tapson V, Galgon RE, Restrepo MI, Kaufman J. Systematic review of the use of retrievable inferior vena cava filters. J Vasc Interv Radiol. 2011;22(11):1522–30.e3. doi: 10.1016/j.jvir.2011.08.024. Review.
4 Kuo WT, Robertson SW, Odegaard JI, Hofmann LV. Complex retrieval of fractured, embedded, and penetrating inferior vena cava filters: a prospective study with histologic and electron microscopic analysis. J Vasc Interv Radiol. 2013;24(5):622–30.e1; quiz 631. doi: 10.1016/j.jvir.2013.01.008. Epub 2013 Mar 21.
5 Smouse HB, Mendes R, Bosiers M, Van Ha TG, Crabtree T. The RETRIEVE trial: safety and effectiveness of the retrievable crux vena cava filter. RETRIEVE Investigators. J Vasc Interv Radiol. 2013;24(5):609–21. doi: 10.1016/j.jvir.2013.01.489.
6 Kuo WT, Odegaard JI, Rosenberg JK, Hofmann LV. Excimer Laser-Assisted Removal of Embedded Inferior Vena Cava Filters: A Single-Center Prospective Study. Circ Cardiovasc Interv. 2013;24. [Epub ahead of print]
7 Van Ha TG, Dillon P, Funaki B, Zangan S, Lorenz J, Piano G, et al. Use of retrievable filters in alternative common iliac vein location in high-risk surgical patients. J Vasc Interv Radiol. 2011;22(3):325–9. doi: 10.1016/j.jvir.2010.09.033. Epub 2011 Feb 1.
8 Angel LF, Tapson V, Galgon RE, Restrepo MI, Kaufman J. Systematic review of the use of retrievable inferior vena cava filters. J Vasc Interv Radiol. 2011;22(11):1522–30.e3. doi: 10.1016/j.jvir.2011.08.024.
9 Johnson MS, Nemcek AA Jr, Benenati JF, Baumann DS, Dolmatch BL, Kaufman JA, et al. The safety and effectiveness of the retrievable option inferior vena cava filter: a United States prospective multicenter clinical study. J Vasc Interv Radiol. 2010;21(8):1173–84. doi: 10.1016/j.jvir.2010.04.004. Epub 2010 Jul 3.
10 Binkert CA, Drooz AT, Caridi JG, Sands MJ, Bjarnason H, Lynch FC, et al. Technical success and safety of retrieval of the G2 filter in a prospective, multicenter study. J Vasc Interv Radiol. 2009;20(11):1449–53. doi:10.1016/j.jvir.2009.08.007.
11 Sangwaiya MJ, Marentis TC, Walker TG, Stecker M, Wicky ST, Kalva SP. Safety and effectiveness of the celect inferior vena cava filter: preliminary results. J Vasc Interv Radiol. 2009;20(9):1188–92. doi: 10.1016/j.jvir.2009.05.033. Epub 2009 Jul 23.
12 Yamagami T, Kato T, Hirota T, Yoshimatsu R, Matsumoto T, Nishimura T. Evaluation of retrievability of the Gunther tulip vena cava filter. Cardiovasc Intervent Radiol. 2007;30(2):226–31.
13 Piano G, Ketteler ER, Prachand V, Devalk E, Van Ha TG, Gewertz BL, et al. Safety, feasibility, and outcome of retrievable vena cava filters in high-risk surgical patients. J Vasc Surg. 2007;45(4):784–8; discussion 788.
14 Bovyn G, Ricco JB, Reynaud P, Le Blanche AF. Long-duration temporary vena cava filter: a prospective 104–case multicenter study. European Tempofilter II Study Group. J Vasc Surg. 2006;43(6):1222–9.
15 Stefanidis D, Paton BL, Jacobs DG, Taylor DA, Kercher KW, Heniford BT, et al. Extended interval for retrieval of vena cava filters is safe and may maximize protection against pulmonary embolism. Am J Surg. 2006;192(6):789–94.
16 De Gregorio MA, Gamboa P, Bonilla DL, Sanchez M, Higuera MT, Medrano J, et al. Retrieval of Gunther Tulip optional vena cava filters 30 days after implantation: a prospective clinical study. J Vasc Interv Radiol. 2006;17(11 Pt 1):1781–9.
17 Rosenthal D, Swischuk JL, Cohen SA, Wellons ED. OptEase retrievable inferior vena cava filter: initial multicenter experience. Vascular. 2005;13(5):286–9.
18 Imberti D, Bianchi M, Farina A, Siragusa S, Silingardi M, Ageno W. Clinical experience with retrievable vena cava filters: results of a prospective observational multicenter study. J Thromb Haemost. 2005;3(7):1370–5.
19 Nakagawa N, Cragg AH, Smith TP, Castaneda F, Barnhart WH, DeJong SC. A retrievable nitinol vena cava filter: experimental and initial clinical results. J Vasc Interv Radiol. 1994;5(3):507–12.
20 Lee L, Taylor J, Munneke G, Morgan R, Belli AM. Radiology-led follow-up system for IVC filters: effects on retrieval rates and times. Cardiovasc Intervent Radiol. 2012;35(2):309–15. doi: 10.1007/s00270–011–0198–7. Epub 2011 Jun 4.
21 Imai H, Schaap RN, Mortensen JD. Rate of thrombus accumulation on intravenacaval IVOX devices explanted from human clinical trial patients with acute respiratory failure. Artif Organs. 1994;18(11):818–21.
22 von Segesser LK, Schaffner A, Stocker R, Lachat M, Speich R, Baumann PC, et al. Extended (29 days) use of intravascular gas exchanger. Lancet. 1992;339(8808):1536.
23 Li L, Abdel-Sayed S, Berdajs D, Tozzi P, von Segesser LK, Ferrari E. Caval collapse during cardiopulmonary bypass: a reproducible bench model. Eur J Cardiothorac Surg. 2014;46(2):306-12.
24 Berdajs D, Born F, Crosset M, Horisberger J, Künzli A, Ferrari E, et al. Superior venous drainage in the "LifeBox": a portable extracorporeal oxygenator with a self-expanding venous cannula. Perfusion. 2010;25(4):211–5. doi: 10.1177/0267659110375863.
25 Straub A, Schnur W, Rehn E-C, Quinz H, Oertel F, Beyer M. Erfahrungen mit der Smart Canula® zur venosen Drainage im Langzeiteinsatz. Kardiotechnik. 2011;4:111–3.
26 Vorwerk D, Redha F, Neuerburg J, Clerc C, Günther RW. Neointima formation following arterial placement of self-expanding stents of different radial force: experimental results. Cardiovasc Intervent Radiol. 1994;17(1):27–32.