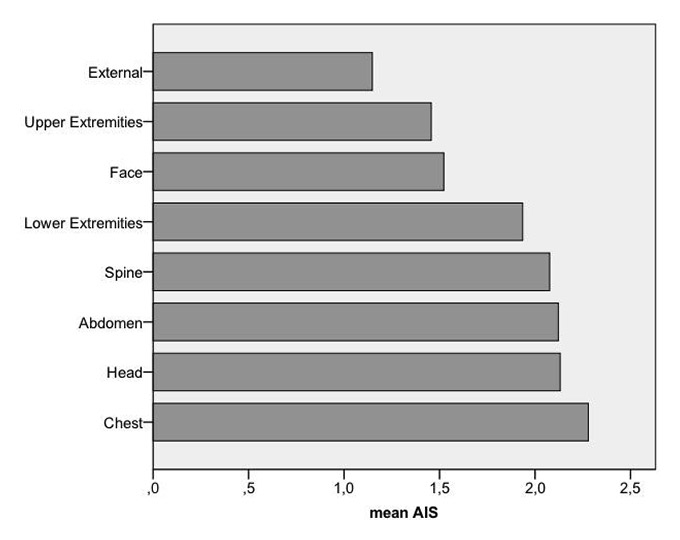
Figure 1
Mean AIS Score.
External injuries include soft tissue injuries and burns.
DOI: https://doi.org/10.4414/smw.2013.13846
Accidents in agriculture are a problem of global importance [1]. Half of the world's labour force, 1.3 billion people, works in agriculture [2]. Agriculture consistently ranks as one of the most dangerous occupations [3–8], along with mining and construction. Traumatic injuries in agriculture are a serious public health problem [9]. Several studies have examined a wide range of potential risk factors for injuries related to agricultural work [1, 4], such as hard physical work, handling machines and animals, and working at heights [1, 3, 10]. All of these mechanisms may lead to trauma [11]. Moreover, agriculture involves multiple seasonal tasks that have to be undertaken quickly to take advantage of favourable weather conditions, leading to long working hours and subsequent sleep deprivation ‒ factors that significantly increase injury risk [11].
Even though several preventive measures have been undertaken [1] – such as safety education of farm workers, installation of fall prevention devices and increased security of agricultural vehicles [1] – fatality rates have remained consistently high [10].
The farming population in Switzerland has decreased in recent years, but 2.1% of Switzerland’s population are still involved in agriculture [12, 13]. According to Swiss Accident Statistics, agriculture is the most dangerous occupational sector in Switzerland, followed by the construction and wood industries [14]. In 2010, a total of 165.7 per 1000 people working in agriculture suffered an injury; 0.03 per 1000 people died [14].
There are few studies on admissions to emergency department (ED) from agricultural injuries. Even though several studies on agriculture and its risks have been published, most of these focused on general risk factors and possible preventive strategies, but not on injury severity [9]. We therefore aimed to assess injury severity and accident mortality in farming at our level I trauma centre.
Our ED (Inselspital, Switzerland) ‒ the only Level I centre in a mainly rural and agricultural catchment area ‒ serves about 1.8 million people and treats more than 35,000 cases per year. Services at our hospital include 24-hour in-house coverage by general surgeons and prompt care from highly trained specialists in different areas, with extensive experience in trauma assessment and treatment. Our centre is also a referral resource for communities in nearby regions.
Figure 1
Mean AIS Score.
External injuries include soft tissue injuries and burns.
Our retrospective cohort study comprised adult (≥16 years) patients admitted to our emergency department (ED) between 1st January 2000 and 31st December 2011 in relation to an accident in agriculture. An accident in agriculture was defined as an accident occurring while working in farming or forestry. All patients presenting to the ED with an accident in agriculture during the study period were initially eligible for study inclusion. Patients were identified using the appropriate search string in the patient demographic field of our computerised patient database (Qualicare Office, Medical Database Software, Qualidoc AG, Bern, Switzerland). Since this medical database allows instantaneous retrieval of past diagnostic reports, discharge summaries, consultations, radiographs and other relevant medical documents, the authors were able to retrospectively analyse the aetiology of the accident, the diagnostic results, and therapeutic procedures initiated in the ED. The following clinical data was extracted from medical records: admission date, aetiology of the accident (machine, animal, fall or unknown), type of machine/animal, fall height, type of injury, count of injuries, hospitalisation and in-hospital mortality. No nursing records were consulted. Demographic data, such as gender and age, were also assessed. All medical records were reviewed by an internal specialist, a surgical specialist and a specialist in emergency medicine. Each diagnosis was coded according to the Abbreviated Injury Scale (AIS) handbook 2008 and the Injury Severity Score (ISS) was calculated for each patient. Severe injuries were defined as ISS >15. According to the AIS, each injury was coded to eight different regions (head/neck, face, spine, thorax, abdomen/pelvic contents, upper extremity, lower extremity, external). Each injury was assigned an AIS severity code, ranging from 1 (minor) to 6 (maximal, unsurvivable) according to the handbook [15]. To calculate ISS, the scores for the three most severely injured body regions were squared and summed to produce the ISS score [16].
Each patient was categorised into only one group of accident aetiology. All specialists had to agree independently on the classification. Hospitalisation and in-hospital mortality was extracted from our hospital's central patient registry (SAP). As this register only stores patient information for 10 years, we were only able to assess hospitalisation and mortality data in 696 patients.
Duplicated records (n = 4) and patients with admissions not related to trauma (n = 88) were excluded from the analysis.
All statistical analyses were performed with the SPSS 20.0 Statistical Analysis programme (SPSS Inc; Chicago, IL). The data were summarised using descriptive statistics (means, standard deviations, percentages and Ns). The differences in patient and injury characteristics were compared between injury types using chi-squared tests for categorical variables, and t-tests and ANOVA for continuous variables. Multivariable logistic regression was used to identify predictors of accident severity (serious or not), hospitalisation and mortality and the models included gender, age, AIS region, injury severity and injury aetiology. All p values were two tailed and at a level of significance of 0.05.
The study was approved by the Ethics Committee of the Canton of Bern, Switzerland.
| Table 1: Patient characteristics. | |||
| n | % | p value | |
| n total | 815 | 100 | |
| Demographics | |||
| Male/female | 785/30 | 96.3/3.7 | 0.0001 |
| Mean age in years (SD) | 47.23 (16.93) | ||
| Machines | 322 | 39.5 | |
| Cutting machine | 78 | 24.2 | |
| Tools | 71 | 22 | |
| Motor vehicle | 110 | 34.2 | |
| Grinding machine | 16 | 5 | |
| Saw | 43 | 13.4 | |
| Others | 4 | 1.2 | |
| Fall | 245 | 30.1 | |
| Median fall height (m) (range) | 2.00 (0.5–30) | ||
| Animal | 131 | 16.1 | |
| Cow | 94 | 71.8 | |
| Bull | 13 | 9.9 | |
| Horse | 24 | 18.3 | |
| Injury mechanism unknown | 117 | 14.4 | |
| Number of diagnoses | 1 (1–14) | ||
| Region of Injury (number of diagnoses) | |||
| Head/neck | 175 | 21.5 | |
| Face | 176 | 21.6 | |
| Chest | 111 | 13.6 | |
| Abdomen | 49 | 6 | |
| Upper extremities | 368 | 45.2 | |
| Lower extremities | 154 | 18.9 | |
| Spine | 91 | 11.2 | |
| External | 54 | 6.6 | |
| Mean ISS (SD) | 5.5 (6.41) | ||
| Hospitalisation | 358 | 43.9 | |
| In-hospital mortality | 13 | 1.6 | |
Out of 390,000 ED visits over twelve year study period, a total of 815 patients were eligible for the study. Table 1 lists the patient characteristics. We found a male predominance of 96.3% versus 3.7% females (p <0.0001). Injury severity did not differ by gender (p <0.23). Injuries to the upper extremities were most common. Overall injuries to the chest (mean 2.28 AIS, SD 1.02) were most severe, followed by injuries to the head (mean 2.13 AIS, SD 1.06) and the abdomen (mean 2.12 AIS, SD 0.94). See figure 1.
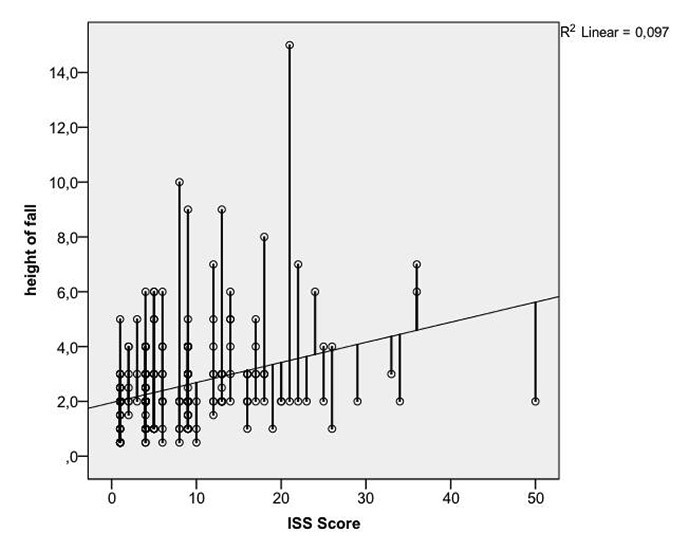
Figure 2
Fall height in correlation to ISS Score.
Table 2 lists a risk analysis. A total of 70 patients (8.6%, 70/815) were severely injured. Patients with injuries to the chest were most likely to suffer from severe injuries (OR 9.45, 95% CI 5.59–16.00, p <0.0001) followed by patients with injuries to the abdomen (OR 7.06, 95% CI 3.22–15.43, p <0.0001) and to the head (OR 5.03, 95% CI 2.99–8.66, p <0.0001). Patients suffering from a fall were significantly more likely to be severely injured (OR 2.54, 95% CI 1.55–4.17, p <0.0001). Hospitalisation was associated with machine- and fall-related injuries (OR 22.39, 95% CI 1.95–4.14, p <0.0001 and OR 2.84, 95% CI 1.68–3.41, p <0.001, respectively). Patients with severe injuries were more likely to be hospitalised (OR 7.19, 95% CI 3.83–13.49, p <0.0001). Patients suffering from a fall and patients with severe injury were more likely to die than others (OR 3.32, 95% CI 1.07–10.29, p <0.037 and OR 9.17, 95% CI 6.20–13.56, p <0.0001, respectively).
Table 3 lists the distribution of injury severity amongst the injury aetiologies. Patients suffering from a fall had a larger number of diagnosis than others (p <0.0001). Patients suffering from a fall had more severe injuries of the head/neck than others (p <0.037), whereas patients with injuries in relation to the use of machines had more severe injuries to the lower extremities than others (p <0.021). For all other AIS regions, no relation to injury aetiology was found. The mean ISS was highest in patients suffering from a fall (7.72, SD 7.56), followed by patients suffering from animal injuries (5.09, SD 6.02) and injuries related to machines (4.7, SD 5.96) (p <0.0001). Hospitalisation rate and in-hospital mortality was highest in patients suffering from a fall (p <0.04 and p <0.031, respectively).
Fall height correlated positively with the ISS Score, hospitalisation and mortality (all p <0.0001). See figure 2.
| Table 2:Risk analysis. | |||
| Odds ratio | Confidence interval | p value | |
| Severe injury: | |||
| Gender | |||
| Male | 10.64 | 7.7–15.3 | 0.0001 |
| Female | Reference | ||
| Injury aetiology | |||
| Machine | 2.21 | 0.34–2.35 | 0.137 |
| Fall | 2.54 | 1.55–4.17 | 0.0001 |
| Animal | Reference | ||
| AIS region | |||
| Head/neck | 5.03 | 2.99–8.66 | 0.0001 |
| Face | 1.45 | 0.88–2.37 | 0.17 |
| Chest | 9.45 | 5.59–16.00 | 0.0001 |
| Abdomen | 7.06 | 3.22–15.43 | 0.0001 |
| Upper extremities | 4.1 | 0.27–7.54 | 0.0.42 |
| Lower extremities | 1.94 | 1.03–3.73 | 0.04 |
| Spine | 3.20 | 1.67–6.13 | 0.0001 |
| External | Reference | ||
| Hospitalisation | |||
| Gender | |||
| Male | 0.99 | 0.96–1.02 | 0.70 |
| Female | Reference | ||
| Injury aetiology | |||
| Machine | 2.39 | 1.95–4.14 | 0.0001 |
| Fall | 2.84 | 1.68–3.41 | 0.001 |
| Animal | 0.93 | 0.74–1.17 | Reference |
| Severe injury | |||
| Yes | 7.19 | 3.83–13.49 | 0.0001 |
| No | Reference | ||
| Mortality | |||
| Gender | |||
| Male | 1.04 | 1.02-10.6 | 0.049 |
| Female | Reference | ||
| Injury aetiology | |||
| Machine | 0.52 | 0.19–1.43 | 0.16 |
| Fall | 3.32 | 1.07–10.29 | 0.037 |
| Animal | Reference | ||
| Severe injury | |||
| Yes | 9.17 | 6.20–13.56 | 0.0001 |
| No | Reference | ||
| Table 3:Distribution of injury severity amongst the injury aetiologies. | ||||
| Machine | Fall | Animal | p value | |
| Gender (m/f) | 313/9 | 236/9 | 123/8 | 0.41 |
| Mean Age (SD) | 46.65 (14.34) | 44.3 (14.79) | 46.69 (13.19) | 0.11 |
| Mean number of diagnosis (SD) | 1.85 (1,86) | 2.78 (2.46) | 1.91 (1.38) | 0.0001 |
| Injury severity (mean AIS score, SD) | ||||
| Head/neck | 1.73 (0.90) | 2.29 (1.08) | 2.0 (1.17) | 0.037 |
| Face | 1.46 (0.58) | 1.66 (0.59) | 1.46 (0.53) | 0.133 |
| Thorax | 2.56 (0.26) | 2.19 (1.00) | 2.26 (0.84) | 0.26 |
| Abdomen | 2.40 (1.18) | 2.36 (0.84) | 1.8 (0.77) | 0.17 |
| Upper extremity | 1.45 (0.63) | 1.56 (0.64) | 1.5 (0.68) | 0.44 |
| Lower extremity | 2.16 (0.93) | 1.8 (0.72) | 1.68 (0.74) | 0.021 |
| Spine | 2.05 (0.52) | 2.15 (0.94) | 1.83 (0.40) | 0.65 |
| External | 1.19 (0.40) | 1.19 (0.40) | 1 (0) | 0.41 |
| Mean ISS (SD) | 4.7 (5.96) | 7.72 (7.56) | 5.09 (6.02) | 0.0001 |
| Hospitalisation (n) | 153 | 127 | 53 | 0.04 |
| In-hospital mortality (n) | 3 | 9 | 1 | 0.031 |
We aimed to characterise injury severity and mortality in patients following agricultural accidents investigated in an academic teaching hospital ED over a 12-year period. To the best of our knowledge, this is one of the first studies that targets injury severity and mortality in agricultural accidents.
Our study showed that the male gender is predominantly at risk, with more than 95% of our sample being male. This finding is concomitant with the current literature [1, 3, 4]. There are several reasons for these findings. One possible explanation may be that – even though farming usually involves the whole family – it is likely that male farmers mainly perform specific tasks, such as operating heavy machines or driving large motor vehicles such as tractors [17], which places them at greater risk of suffering an injury.
Our study showed a median ISS of four. This is clearly higher than the ISS of two found in a study by Day et al. on risk factors for work-related injury among male farmers in Australia [10]. Moreover, in the same study, the ISS range was 1‒5, whereas in our study it was 1‒50. One possible explanation could be that the study by Day et al. involved fourteen regional hospitals and five metropolitan hospitals [10]. In contrast, our single centre study was conducted at the only level I trauma centre in a large rural area. Therefore most of the more severe and complex injuries are treated at our facility.
The published percentage of patients admitted to hospital varies from 7.3% in a Polish study [9] to 82% in an Australian study [10]. Our figure of 42% is in the intermediate range. The differences from the Australian study are especially striking, as our patients were more severely injured (see above). One possible explanation may be that in Australia – with its extensive rural areas and lower density of medical facilities – patients with minor injuries are more likely to be admitted to hospital than in Switzerland, as access to medical care is more difficult should complications develop. In contrast to other studies, we also found that admission to hospital was not associated with age [1].
The mortality rate in our study was comparable to the study by Day et al. [10]. It is widely recognised that injury severity is generally associated with increased mortality [18, 19]. However it is remarkable that we did not find any association between age and mortality, as has been found in other studies [4, 7, 9, 17, 20]. One reason for this may be that our university hospital is relatively far from the farmlands and selects a predominantly young and severely injured clientele. It is also possible that the lack of effect is related to the small sample size. The age range of the patients in our study who died was 26 to 75 years. Falls are the major aetiology of mortality in agricultural accidents [21], as confirmed in the present study. Neither machinery nor animals were associated with mortality in our study. In contrast, a review by Angoules et al. described an association between vehicles and machinery and mortality [21]. It is difficult to explain this difference. One possible explanation could be that our study design – with motor vehicles included in the category “machines” – may have biased our results.
We found that patients with injuries related to falls were more prone to severe injury and hospitalisation. This has also been found in other studies [9, 22, 23]. It is thought that the lack of safety measures (e.g. lack of handrails, guard rails) is related to the risk of severe injury or mortality from falls [22, 23].
Our study showed that machines were the most common cause of injuries. This is consistent with the current literature [1, 3, 4, 9, 10]. Several risk factors have been identified, such as the lack of safety features in the machines, lack of safety education or the neglect of a rollover protective structure in agricultural vehicles [1, 3, 10, 24]. This study showed that injuries to the upper extremities were most common in patients with machine-related injuries, as has also been found by others [3, 21]. However, injuries to the upper extremities were not more severe in patients with machine-related injuries than in patients with other injuries.
Our findings have to be considered with some caution, as our study was conducted retrospectively. As information in our medical history database is presented in a narrative comment, no guarantee of complete or correct reporting can be given and bias is possible. Furthermore, information was often incomplete or unclear and thus had to be excluded. In consequence, underreporting of the aetiologies of agricultural injuries cannot be excluded. As a consequence of the coding according to the AIS handbook, we did not assess the different types of injuries in detail, so that no information on the exact type of injury can be drawn from this study. Additionally we were not able to give any information on the setting of the falls (e.g. house, tree etc.). Furthermore no information on hospitalisation and mortality was available for 146 (17.9%) of our patients. It is therefore possible that hospitalisation and mortality rates are underestimated. Additionally, our study was limited to adults (>16 years of age), as children are treated at a separate emergency department in the same hospital. Therefore no information can be drawn from this study about agricultural accidents to children. This would require additional studies.
Injuries in agriculture are accompanied by substantial morbidity and mortality and range from minor injuries to severe multiple injuries. This study found higher mean ISS scores than in previous studies. Injury severity and mortality from agricultural injuries is predominantly associated with falls. It is therefore essential to improve safety education and to establish preventive measures.
Our study is one of the first studies to assess injury severity in agricultural injuries. Further prospective cohort studies should be conducted on injury severity, but also long-term disability and mortality and the related risk factors.
1 Pickett W, Hartling L, Dimich-Ward H, Guernsey JR, Hagel L, Voaklander DC, et al. Surveillance of hospitalized farm injuries in Canada. Injury prevention: journal of the International Society for Child and Adolescent Injury Prevention. 2001;7(2):123–8. Epub 2001/06/29.
2 Rautiainen RH, Lehtola MM, Day LM, Schonstein E, Suutarinen J, Salminen S, et al. Interventions for preventing injuries in the agricultural industry. Cochrane database of systematic reviews (Online). 2008(1):CD006398. Epub 2008/02/07.
3 Young SK. Agriculture-related injuries in the parkland region of Manitoba. Canadian family physician Medecin de famille canadien. 1995;41:1190–7. Epub 1995/07/01.
4 Crawford JM, Wilkins JR, 3rd, Mitchell GL, Moeschberger ML, Bean TL, Jones LA. A cross-sectional case control study of work-related injuries among Ohio farmers. Am J Ind Med. 1998;34(6):588–99. Epub 1998/11/17.
5 Kachan D, Fleming LE, LeBlanc WG, Goodman E, Arheart KL, Caban-Martinez AJ, et al. Worker populations at risk for work-related injuries across the life course. Am J Ind Med. 2012;55(4):361–6. Epub 2011/12/16.
6 Rivara FP. Fatal and non-fatal farm injuries to children and adolescents in the United States, 1990–3. Injury prevention: journal of the International Society for Child and Adolescent Injury Prevention. 1997;3(3):190–4. Epub 1997/10/27.
7 Pickett W, Hartling L, Brison RJ, Guernsey JR. Fatal work-related farm injuries in Canada, 1991–1995. Canadian Agricultural Injury Surveillance Program. CMAJ: Canadian Medical Association journal = journal de l’Association medicale canadienne. 1999;160(13):1843–8. Epub 1999/07/16.
8 Pickett W, Day L, Hagel L, Brison RJ, Marlenga B, Pahwa P, et al. The Saskatchewan Farm Injury Cohort: rationale and methodology. Public health reports (Washington, DC: 1974). 2008;123(5):567–75. Epub 2008/10/03.
9 Nogalski A, Lubek T, Sompor J, Karski J. Agriculture and forestry work-related injuries among farmers admitted to an Emergency Department. Annals of agricultural and environmental medicine: AAEM. 2007;14(2):253–8. Epub 2008/02/06.
10 Day L, Voaklander D, Sim M, Wolfe R, Langley J, Dosman J, et al. Risk factors for work related injury among male farmers. Occup Environ Med. 2009;66(5):312–8. Epub 2008/12/20.
11 Lilley R, Day L, Koehncke N, Dosman J, Hagel L, William P. The relationship between fatigue-related factors and work-related injuries in the Saskatchewan Farm Injury Cohort Study. Am J Ind Med. 2012;55(4):367–75. Epub 2012/01/04.
12 Statistik Bf. Landwirtschaftliche Betriebszählung. 2010 [cited 18.10.2012 18.10.2012]; Available from: http://www.bfs.admin.ch/bfs/portal/de/index/themen/07/03.html.
13 Landwirtschaft Bf. Agrarbericht 2011. Bern: Bundesamt für Landwirtschaft; 2011. 1–284 p.
14 Swiss Accident Statistics. 2011 [18.10.2012]; Available from: http://www.unfallstatistik.ch/d/publik/unfstat/pdf/Ts12.pdf. Last access 26.05.2013
15 Genarelli Thomas W, Elaine. Abbreviated Injury Scale Update 2008. Association for the Advancement of Automotive Medicine. 2008;1(1).
16 Injury Severity Score. 2012; Available from: http://www.trauma.org/archive/scores/iss.html.
17 DeGroot JM, Isaacs C, Pickett W, Brison RJ. Patterns of fatal machine rollovers in Canadian agriculture. Chronic diseases and injuries in Canada. 2011;31(3):97–102. Epub 2011/07/08.
18 Bolorunduro OB, Villegas C, Oyetunji TA, Haut ER, Stevens KA, Chang DC, et al. Validating the Injury Severity Score (ISS) in different populations: ISS predicts mortality better among Hispanics and females. J Surg Res. 2011;166(1):40–4. Epub 2010/09/11.
19 Timmons SD, Bee T, Webb S, Diaz-Arrastia RR, Hesdorffer D. Using the abbreviated injury severity and Glasgow Coma Scale scores to predict 2-week mortality after traumatic brain injury. J Trauma. 2011;71(5):1172–8. Epub 2011/11/11.
20 Voaklander DC, Hartling L, Pickett W, Dimich-Ward H, Brison RJ. Work-related mortality among older farmers in Canada. Canadian family physician Medecin de famille canadien. 1999;45:2903–10. Epub 2000/01/08.
21 Angoules AG, Lindner T, Vrentzos G, Papakostidis C, Giannoudis PV. Prevalence and current concepts of management of farmyard injuries. Injury. 2007;38(Suppl 5):S27–34. Epub 2007/11/30.
22 Solomon C. Accidental injuries in agriculture in the UK. Occupational medicine (Oxford, England). 2002;52(8):461–6. Epub 2002/12/19.
23 Solomon C, Poole J, Palmer KT, Coggon D. Non-fatal occupational injuries in British agriculture. Occup Environ Med. 2007;64(3):150–4. Epub 2006/06/22.
24 Murphy DJ, Myers J, McKenzie EA, Jr., Cavaletto R, May J, Sorensen J. Tractors and rollover protection in the United States. J Agromedicine. 2010;15(3):249–63. Epub 2010/07/29.
Funding / potential competing interests: No financial support and no other potential conflict of interest relevant to this article was reported.