Figure 1
Location of Hochdorf, Canton Lucerne in Switzerland.
DOI: https://doi.org/10.4414/smw.2013.13819
The Hochdorf burial (fig. 1) was found in 1887 during construction work. Apart from a short written description, there is no documentation [1, 2]. According to this text, the individual lay supine with the arms stretched alongside the body. The grave was aligned in south-north direction. The head pointed north, which is typical for the late Iron Age. Alongside the head, there was a large stone. Traces of a coffin or other constructions related to the funeral were not mentioned, but must be expected. The individual in the Hochdorf grave has a skull anomaly (fig. 2).
Figure 1
Location of Hochdorf, Canton Lucerne in Switzerland.

Figure 2
Skull with intensely calcified bone proliferation at the right side of the os frontalis.
The sex and age of the individual were determined using anthropological methods. It was also possible to determine a differential diagnosis by means of radiological and histological examinations. This finding is unique as it is the oldest known case with this kind of pathology. Earlier studies have examined and discussed similar pathologies from archaeological findings, as well as from living patients [3‒12]. Prates et al. [13] examined a male Ptolemaic Egyptian mummy using digital radiography and multidetector computerised tomography (MDCT). They found several dense bone lesions in the spine, pelvis and proximal extremities of the mummy. This is evidence of an osteoblastic metastatic disease. Several paleopathological cases from Switzerland are already well known [7, 14‒20]. Ulrich-Bochsler et al. [21] published a possible case of spondylitis tuberculosa in the Canton of Bern. There is also a possible case of skeletal tuberculosis of the knee in an early medieval young female found in Canton Ticino [22]. Rüttimann and Lösch [15] found several different pathologies in the Bernese burial register (1805–1876). They published cases of, for example, typhus, respiratory diseases, strokes, cramps and cancer. The aim of the study was to reconsider a differential diagnosis and to use different methods of investigation.
The skeleton seems to have been seriously disturbed by construction work. Only the skull, the left half of the pelvis and the left femur are preserved. At least ten brooches were found on the chest. There is no information about how they were arranged. The brooches belong to the archaeological period La Tène B2 and are often found in burials of this time. The large number of brooches was a rather common practice in the late Iron Age, but also indicates a high social rank of the deceased person. Here, a fragmented bronze ring was also discovered and described as an arm ring; though no information is provided about its exact location. Two rings were found on the legs ‒ probably just above the foot, as is usual for Celtic burials. The grave goods are typical for the late Celtic period (La Tène B2) and thus the late 4th and the early 3rd century BC between 320 and 250 BC [23]. Although no other burials are known in the vicinity, it might have been part of a larger cemetery.

Figure 3
Location of sampling for histological analysis (red triangle).

Figure 4
X-ray image of the skull.
The anthropological examination to determine the individual’s sex was performed in accordance with published methods [24‒27], as was estimation of the age at death [24, 27‒30]. Radiological examinations were performed with plain X-ray imaging and a multislice CT-scanner (Somatom 6, Siemens Medical Solutions, Germany). The CT scan was obtained using the following parameters: 150mAs, 130kV, 1.25 mm slice thickness, reconstruction in a bone image kernel (B70). For histological analysis, a fragment of the lesion was taken from the tabula externa and interna of the skull (fig. 3). Pathological processing was routine, with formalin fixation, decalcification and paraffin embedding with subsequent slicing and staining with haematoxylin and eosin, and elastica van Gieson to demonstrate the different components of the matrix [4]. Unstained hard-cut sections were also prepared using bio-epoxide resin (Biodur®) and a microtome (Leica) with an inner diameter saw.
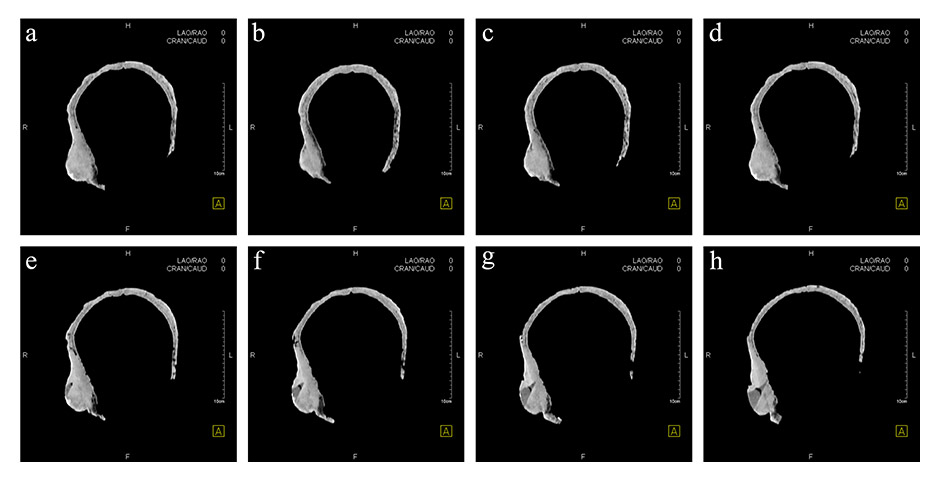
Figure 5
Horizontal computed tomography cross-sections of the skull. Selected representative slices.
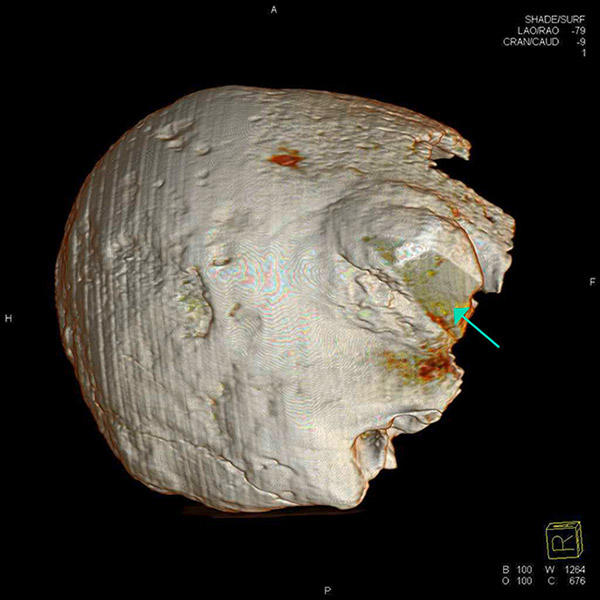
Figure 6
Computed tomography three-dimensional reconstruction of the skull. Wedge-shaped area in the centre of the lesion filled with material of lower X-ray density than the adjacent bone (green arrow).

Figure 7
Hard-cut section 1.25x. Sample taken out of the lesion.
The remains are well preserved. Morphological examination of skull and pelvis clearly classify the individual as female. The age at death was between 30 and 50 years. There is an intensely calcified bone proliferation at the right side of the os frontalis (fig. 2). Plain X-ray and CT imaging show a large (5.3 x 3 x 8.7 cm) sclerotic lesion in the area of the right temple with a partly bulging appearance (fig. 4). Figure 5 shows representative slices of the admission CT. A differentiation between tabula interna, diploë and tabula externa is not possible in major parts of the lesion. The inner boundary of the lesion shows multiple smooth-edged irregularities. There is a diffuse thickening of the right skull vault (right 7 mm, left 4 mm). The left skull vault presents a mix of sclerotic areas and areas with normal appearance with a clear differentiation between tabula interna, diploë and tabula externa. CT imaging and plain X-ray show a wedge-shaped area in the centre of the lesion that is filled with material of lower X-ray density than the adjacent bone (figs 5 and 6). Histology shows mature organised lamellar bone tissue with ordered formation of trabeculae (figs 7–9). No pathological alterations were found in the postcranial bones.
There are already several known cases of benign tumours in ancient populations. Brothwell and Sandison [10], for example, described a case of ivory osteomata in a Roman Egyptian skull. Our study presents a very unusual case of multiple osteosclerotic lesions in an Iron Age skull from Switzerland. It is the oldest known case with this kind of pathology worldwide. Analysis with various investigative methods leads to a differential diagnosis. The CT image showed that a piece of bone had been removed from the lesion earlier (fig. 5e‒h). The sampling point was then carefully reconstructed so that there was no visible trace left. It is not clear when this reconstruction of the earlier sample was done and the person who took the sample is also unknown. This work was never published or presented. In the 1950s and 1960s, one of the anthropologists in Switzerland was Erik Hug [31, 32]. His work on bone material included reconstructions just like the one in the Hochdorf skull. This could indicate that the earlier bone biopsy was performed by Erik Hug.
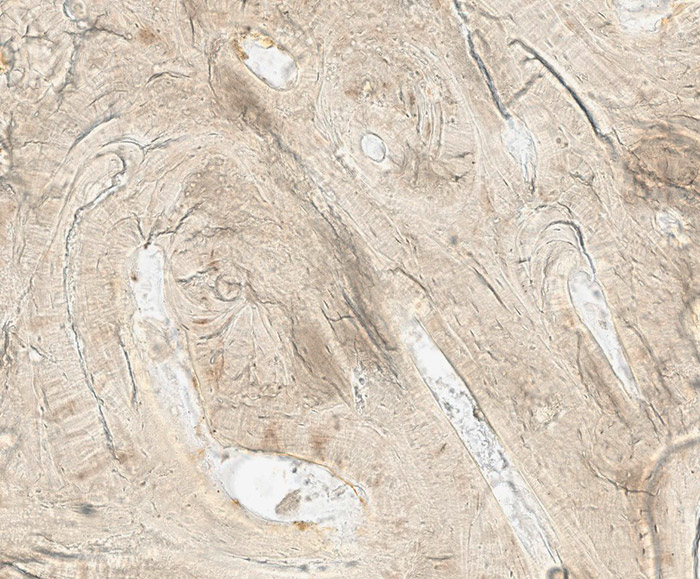
Figure 8
Hard-cut section 40x. Sample taken out of the lesion.

Figure 9
Paraffin embedding, haematoxylin and eosin, 40x. Sample taken out of the lesion.
The radiological images show no osteolysis. The tumour is clearly defined and appears to be a benign tumour. The differential diagnosis leads to the following conclusions: the radiological examinations imply hyperostosis, for example exostoses. The diagnostic findings could also be a callus formation as a result of trauma or osteomyelitis. Various benign tumours must also be considered.
Histomorphological analysis revealed mature, structured lamellar bone without indication of an associated immature or fibrous component. The bone lesion is dense and without evidence of lytic areas. Although viable cellular components, which could have shown signs of nuclear atypia, could not be demonstrated, the mature architecture of the remnant bone structures do not raise the suspicion of malignancy.
Moreover, a reactive lesion like a callus formation as a result of trauma or osteomyelitis seems to be unlikely because of the orderly architecture and the purely lamellar matrix formation. The histological findings also exclude Paget’s disease or hyperparathyroidism [33, 34], since both conditions involve signs of heavy bone remodelling. Primary malignant conditions can be excluded owing to the macroscopic and microscopic findings. However, the macroscopic appearance could be consistent with osteoblastic metastases as well. Rather, the systematic arrangement of the lesions, their absence on the other bones (pelvis, femur) and the histology findings exclude this differential diagnosis.
Given that the carefully taken bone sample is representative of the large and also the smaller lesions, the presence of multiple osteomas is considered as the first differential diagnosis on the basis of the macroscopic, radiological and histological findings.
The occurrence of multiple osteomas is a very rare condition. It can be observed, for example, in the setting of hereditary adenomatous polyposis coli (APC) related to Gardner syndrome [4, 8, 35‒39], where patients are affected by an autosomal dominant disorder linked to the chromosome band 5q21 in the APC gene, the adenomatous polyposis coli locus [40, 41]. Usually, the mandibles are the most common location for osteomas, but they also occur in the skull and long bones [41]. Three different characteristics of Gardner syndrome are described [8, 38, 39]: multiple osteomas, cutaneous tumours and familial polyposis coli (FPC). The incidence of Gardner syndrome is about 1 per 14,025 [42]. The hallmark of this disease is the development of hundreds to thousands of intestinal adenomas (familial adenomatous polyposis) which eventually leads to the development of colon or intestinal cancer [41]. We have no evidence of any visceral or organ pathology in this case, so the diagnosis of Gardner syndrome – although not unlikely – cannot be finally confirmed. Ancient deoxyribonucleic acid (aDNA) analysis could provide more information about genetic disorders. However, aDNA is highly fragmented, so any contamination during excavation, sampling and storage of the bone material must be avoided [43, 44]. The bones here were found in 1887 and then exhibited in a museum in Lucerne. There is a high probability that they are contaminated with modern DNA, for example by the excavators or the museum staff. Furthermore, there is hardly any aDNA preserved owing to the storage conditions. For these reasons, no aDNA analysis was performed.
To improve the understanding of cancer pathogenesis, there is ongoing research in ancient bones [45]. Due to the industrial revolution, carcinogens and the risk of cancer are continuously rising. However, findings like the unique single Hochdorf burial show that osteogenic tumourous lesions were already present in ancient populations such as the late Celtic period. Findings from osseous pathologies may contribute to differential diagnostic considerations about diseases which extend beyond the skeleton: in the case presented here, a genetic disorder may be the underlying cause for the findings in this skull.
Acknowledgements:We thank Sandra Mathier and Lorenzo Campana (Forensic Medicine and Imaging, Bern University) for the CT-measurements. We would also like to thank Petra Nirmaier (Achaeological Survey Lucerne) for assistance during the sampling procedure, Matthias Dömötör (Aye-Aye Productions GmbH) for image editing assistance, Domenic Rüttimann (Physical Anthropology, Bern University) for documentation and photographs, Korbinian Seitz (Bern University) for editing and Christoph Rogalla von Bieberstein (Archaeological Service Bern) for support with the X-ray. We thank the reviewer for the constructive comments.
Funding / potential competing interests: No financial support and no other potential conflict of interest relevant to this article was reported.
1 Brandstetter JL. 1887. Der Grabfund zu Hochdorf. Der Geschichtsfreund XLII. 261–265 + Tafel II.
2 Tanner A. without date of print. Die Latènegräber der nordalpinen Schweiz, Heft 4/9. Kantone Luzern und Solothurn: Zürich.
3 Craig E, Craig G. 2011. The Diagnosis and Context of a Facial Deformity from an Anglo-Saxon Cemetery at Spofforth, North Yorkshire. International Journal of Osteoarchaeology. DOI: 10.1002/oa.1288
4 Bullough PG. 2010. Orthopaedic Pathology. 5thedition. Mosby Elsevier: Missouri.
5 Pinhasi R, Mays S. 2008. Advances In Human Palaeopathology. John Wiley & Sons Ltd: West Sussex.
6 Zink A, Panzer S, Fesq-Martin M, Burger-Heinrich E, Wahl J, Nerlich AG. Evidence for a 7000-Year-Old Case of Primary Hyperparathyroidism. American Medical Association 2005;293:40–2.
7 Ortner DJ. 2003. Identification of Pathological Conditions in Human Skeletal Remains. Academic Press: London.
8 Noterman J, Massager N, Vloeberghs M, Brotchi J. Monstrous Skull Ostemeomas in a Probable Gardner’s Syndrome: Case Report. Surgical Neurology 1998;49:302–5.
9 Liakos GM, Walker CB, Carruth JAS. Ocular complications in craniofacial fibrous dysplasia. Br J Ophthalmol 1979;63:611–6.
10 Brothwell D, Sandison AT. 1967. Diseases in Antiquity; A Survey of the Diseases Injuries and Surgery of Early Populations. Charles C. Thomas, Springfield: Illinois.
11 Jaffé H, Lichtenstein L. Solitary unicameral bone cyst: with emphasis on the roentgen picture, the pathologic appearance, and the pathogenesis. Arch Surg. 1942;44:1004–25.
12 Albright F, Butler AM, Hampton AO, Smith P. Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction, with precocious puberty in females: report of 5 cases. N Engl J Med. 1937;216:727–46.
13 Prates C, Sousa S, Oliveira C, Ikram S. Prostate metastatic bone cancer in an Egyptian Ptolemaic mummy, a proposed radiological diagnosis. International Journal of Paleopathology. 2011;1:98–103.
14 Lösch S, Moghaddam N, Ross S, Müller F, Langer R. 2012. A Case Of A Malign Tumour In Iron Age Switzerland. The 19th european meeting of the paleopathology association.
15 Rüttimann D, Lösch S. Mortality and morbidity in the city of Bern, Switzerland, 1805-1815 with special emphasis on infant, child and maternal deaths. HOMO - Journal of Comparative Human Biology. 2012;63:55–66.
16 Papageorgopoulou C, Suter SK, Rühli FJ, Siegmund F. Harris Lines Revisited: Prevalence, Comorbidities, and Possible Etiologies. American Journal of Human Biology 2011;23:381–91.
17 Hofmann MI, Papageorgopoulou C, Böni T, Rühli FJ. Two case examples of pelvic fractures in medieval populations from central Europe. J Anthropol Sci. 2010;88:179–88.
18 Papageorgopoulou C, Rühli FJ, Siegmund F, Woitek U. Assessing dental health predictors in a Swiss medieval population by a spatial probit model. Am J Phys Anthropol. 2010;50:184–184.
19 Haak W, Gruber P, Rühli FJ, Böni T, Ulrich-Bochsler S, Frauendorf E, et al. Molecular evidence of HLA-B27 in a historical case of ankylosing spondylitis. ARTHRITIS AND RHEUMATISM 2005;52:3318–9.
20 Rühli FJ, Hotz G, Böni T. Brief communication: The Galler Collection: A little-known historic Swiss bone pathology reference series. Am J Phys Anthropol. 2003;121:15–8.
21 Ulrich-Bochsler S, Schäublin E, Zeltner THB, Glowatzki G. Invalidisierende Wirbelsäulenverkrümmung an einem Skelettfund aus dem Frühmittelalter (7./8. Bis Anfang 9. Jh.). Ein Fall einer wahrscheinlichen Spondylitis tuberculosa. Schweiz Med Wochenschr. 1982;112:1318–23.
22 Andreetta A, Lösch S. 2012. Lesions of skeletal tuberculosis on young woman’s knee, buried in S. Giovanni Battista curch in Leontica (Ticino, Switzerland). The 19th european meeting of the paleopathology association.
23 Müller F, Kaenel G, Lüscher G. 1999. Die Schweiz vom Paläolithikum bis zum frühen Mittelalter. SPM IV. Eisenzeit: Basel.
24 Ferembach D, Schwidetzky I, Stloukal M. Empfehlungen für die Alters- und Geschlechtsdiagnose am Skelett. Homo – Journal of comparative human biology 1979;30:1–32.
25 Rösing FW, Graw M, Marre B, Ritz-Timme S, Rothschikd MA, Rötzscher K, et al. Recommendations for the forensic diagnosis of sex and age from skeletons. Homo – Journal of comparative human biology. 2007;58:75–89.
26 Sjøvold T. 1988. Geschlechtsdiagnose am Skelett. In: Knußmann R (ed) Anthropologie. Handbuch der vergleichenden Biologie des Menschen, vol 1. Gustav Fischer Verlag: Stuttgart; 444.
27 Hermann B, Grupe G, Hummel S, Piepenbrink H, Schutkowski H. 1990. Prähistorische Anthropologie. Leitfaden der Feld- und Labormethoden. Springer-Verlag: Berlin, Heidelberg, New York.
28 Szilvássy J. 1988. Altersdiagnose am Skelett. In: Knußmann R (ed.) Anthropologie. Handbuch der vergleichenden Biologie des Menschen, Band I: Allgemeine Anthropologie, vol 1. Gustav Fischer Verlag: Stuttgart; 421–435.
29 Vallois HV. La durée de la vie chez l’homme fossile. L’Anthropologie. 1937;47:499–532.
30 Acsádi G, Nemeskéri I. 1970. History of human lifespan and mortality. Academiai Kiado: Budapest.
31 Hug E. 1956. Die Anthropologische Sammlung im Naturhistorischen Museum Bern. Sonderabdruck aus den Mitteilungen der Naturforschenden Gesellschaft in Bern. Neue Folge 13. Band.
32 Schoch W, Ulrich-Bochsler S (1987): Die anthropologische Sammlung des Naturhistorischen Museums Bern. Katalog der Neueingänge 1956 bis 1985, in: Jahrbuch des Naturhistorischen Museums Bern 9, Jahrgang 1987, 267–350.
33 Aufderheide A, Rodriguez-Martin C. 2008. The Cambridge encyclopedia of human palaeopathology. 4th Edition. Cambridge University Press: Cambridge
34 Bilezikian JP, Silverberg SJ. Asymptomatic Primary Hyperparathryroidism. N Engl J Med. 2004;350:1746–51.
35 Kerckhaert A, Wolvius E, Van Der Waal K, Oosterhuis W. A giant Osteoma of the mandible: Case report. J Craniomaxillofac Surg. 2005;33:282–5.
36 Bilkay U, Erdem O, Ozek C, Helvaci E, Kilic K, Ertan Y, Gurler T. Benign Osteomas With Gardner Syndrome: Review of the Literature and Report of a Case. J Craniofac Surg. 2004;15:506–9.
37 Davies R, Armstrong JG, Thakker N, Horner K, Guy SP, Clancy T, et al. Severe Gardner Syndrome in Families with Mutations Restricted to a Specific Region of the APC Gene. Am J Hum Genet. 1995;57:1151–8.
38 Gardner EJ, Plenk HP. Hereditary Pattern for Multiple Osteomas in a Family Group. Am J Hum Genet. 1952;4:31–6.
39 Gardner EJ. A Genetic and Clinical Study of Intestinal Polyposis, a Predisposing Factor for Carcinoma of the Colon and Rectum. The American Journal of Human Genetics 1951;3:167–76.
40 Gu GL, Wang SL, Wei XM, Bai L. Diagnosis and treatment of Gardner syndrome with gastric polyposis: A case report and review of the literature. World Journal of Gastroenterology 2008;14:2121–3.
41 Fotiadis C, Tsekouras DK, Antonakis P, Sfiniadakis J, Genetzakis M, Zografos GC. Gardner’s syndrome: A case report and review of the literature. World Journal of Gastroenterology 2005;11:5408–11.
42 Remmele W. 1996. Pathologie 2, Verdauungstrakt. Springer Verlag: Heidelberg; 642–643.
43 Burger J and Bollongino R. Guidelines for the recovery, acquisition and storage of skeletal samples for palaeogenetical analyses. Bulletin der Schweizerischen Gesellschaft für Anthropologie 2010;16:71–8.
44 Burger J, Tresset A and Vigne JD. Environment and excavation: pre-lab impacts on ancient DNA analyses. Comptes Rendus Palevol. 2008;7:91–8.
45 Rehemtulla A. Dinosaurs and Ancient Civilizations: Reflections on the Treatment of Cancer. Neoplasia 2010;12:957–68.