Alcohol consumption in late adolescence and early adulthood – where is the problem?
DOI: https://doi.org/10.4414/smw.2013.13826
Emmanuel
Kuntsche, Gerhard
Gmel
Summary
Risky single-occasion drinking (RSOD) is more common in late adolescence and early adulthood (approximately between the ages of 16 and 30) than in any other period in life. This is also the age when young people in Switzerland and many other European countries are legally allowed to buy and drink alcohol, but they usually do not yet have adult responsibilities. This paper reviews evidence from the international literature and provides examples of studies conducted in Switzerland demonstrating that (a) RSOD is by far most prevalent on Saturday evenings followed by Friday evenings, usually because young people go out and do not have any work or study responsibilities the next day; (b) RSOD results from drinking in private before going out (“predrinking”) and accelerating the pace of drinking (i.e. increasing the number of drinks consumed per hour); (c) RSOD is often not accidental but purposeful,. to seek excitement, to have fun and to feel the effects of alcohol; (d) RSOD occurs predominantly outside the home, mostly in bars, pubs, discos or at special events and festivals; (e) RSOD often results in intended and unintended injuries and other acute consequences, which are leading risk factors for mortality and morbidity in this age group. Effective prevention strategies should include attempts to reduce opportunities to engage in heavy drinking as well as strategies to reduce its harmful consequences.
Introduction
Much is known about the epidemiology of underage drinking in Europe thanks to large-scale international surveys targeting 11- to 16-year-olds [1, 2]. Less is known about changes in alcohol consumption during the period when adolescents start to become adults, however. This period is shaped by developmental transitions, such as leaving home, embarking upon a professional career, living with a stable partner or even becoming a parent.
Furthermore, this period is interesting from an alcohol policy point of view. Many existing studies of individuals in late adolescence and early adulthood were conducted in the United States, where the minimum legal drinking age is 21 years. In Europe, however, there is different legislation in place as regards on-premises drinking and off-premises purchasing of alcohol, at least for nondistilled beverages, which can often be legally purchased at the age of 16 or 18 years [3]. As explained below, this catches adolescents in a period of neurological and psychosocial immaturity.
To better understand alcohol consumption in late adolescence and early adulthood (covering an approximate age range of 16 to 30 years), this paper first concentrates on the development of risk taking throughout adolescence, including when young people grow out of this behaviour, which usually takes place with the onset of adult roles and responsibilities. Subsequently, we describe the prevalence of daily and risky drinking over the course of life and, more specifically, we provide evidence of the typical drinking patterns of young adults, for example on weekend evenings. We also outline what motivates young adults to drink in this way. We continue by demonstrating where young adults usually drink and the resulting adverse consequences. We conclude by providing recommendations for preventing harm resulting from the specific drinking patterns of young adults.
For each of these topics, we provide a brief overview based on selected studies from the international literature. As examples, we present evidence from studies conducted in Switzerland.
Why focus on older adolescents’ and young adults’ alcohol consumption?
Risk taking in adolescence and beyond
Since the landmark study of Jessor and Jessor [4], it is common knowledge that in adolescence different kinds of risk behaviours are widespread among individuals and tend to co-occur within the same individuals, a phenomenon known as “problem behaviour syndrome” [5]. In Switzerland, results from a repeated cross-sectional survey among 15-year-olds (total n = 4,146) showed that, although the frequency of smoking, drunkenness and cannabis use greatly increased over a 12-year period, the underlying factor structure, that is, clustering as a kind of substance use syndrome, remained the same [6].
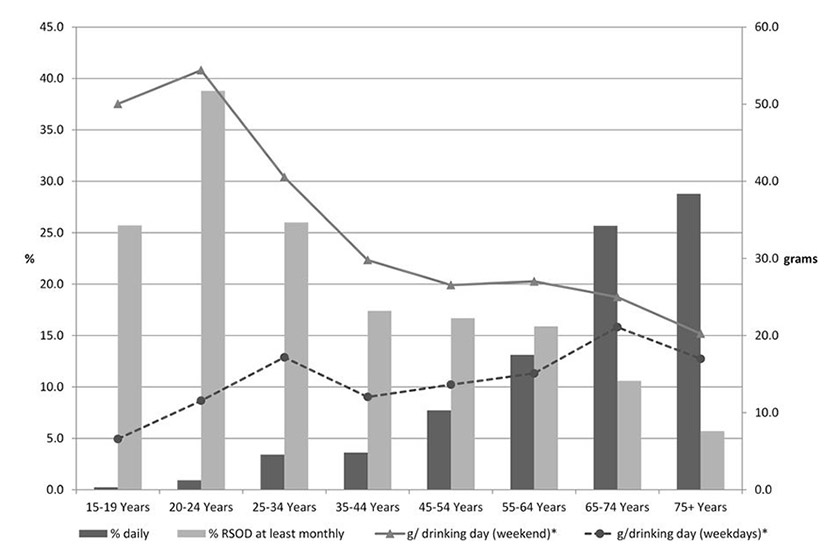
Figure 1
Percentage of daily and risky single occasion drinkers (RSOD) and grams of alcohol consumed on weekend days and weekdays by age group in 2011.
Note: *among drinkers only (n = 5,840); data from Addiction Monitoring in Switzerland financed by the Federal Office of Public Health
More recent research has demonstrated that, besides genetic factors [7–10], the acquisition of risk behaviours including risky drinking and other substance use patterns originates in neurological and psychosocial changes which occur during the transition from childhood to adulthood. Neurologically, asynchronous maturation of prefrontal and limbic systems and the remodelling of dopaminergic pathways are assumed to make risk taking appear more rewarding for adolescents than is the case among children and adults [11]. Psychosocially, risk taking can be functional in dealing with developmental tasks in this life stage, such as experiencing one’s own limits, demonstrating autonomy from parents, seeking acceptance or increasing social status among peers [12].
Later in adulthood, risk-taking behaviours (including risky drinking) tend to decrease or disappear. Again, this can be explained from neurological and psychosocial perspectives. Fostered neural connections between the prefrontal cortex and the limbic system lead to better emotion-cognition coordination and self-regulation, which allow individuals to refrain from impulsive behaviour in favour of a more reflective behaviour by the time they reach their mid-20s [11]. Psychosocially, risk-taking behaviours become less functional or even detrimental when adult roles and responsibilities are taken on. Studies have demonstrated that, when entering stable employment, living in a stable partnership or marriage, or becoming a parent, young adults reduce risky single-occasion drinking (RSOD) frequency to more moderate levels of alcohol use [13]. The protective effect of adult roles and responsibilities was also demonstrated in a national representative study in Switzerland, showing that the higher the family responsibilities (having small children to care for, doing the majority of the childcare and the household chores, etc.) among mothers, the lower the level of their alcohol use [14]. Although some protective effects were found for fathers too, the effect was much stronger among mothers, indicating a differentiation between male and female gender roles among parents living in Switzerland.
Conclusion: often co-occurring with other risk behaviours, RSOD is particularly common in late adolescence and early adulthood and tends to decrease later in adulthood when new roles and responsibilities emerge.
Development of daily and risky drinking over an individual’s life
Alcohol consumption usually starts in adolescence. Across 38 European and North American countries and regions, for example, the prevalence of weekly drinking was 2% among 11-year-olds, 4% among 13-year-olds and 21% among 15-year-olds [1]. For repeated drunkenness, these figures were 2%, 9%, and 32%, respectively. The volume of drinking usually increases until early adulthood and then remains relatively stable until retirement age, with some slight increases in some countries (including Switzerland) and slight decreases in other countries [15, 16]. With risky single-occasion drinking (RSOD, also called “binge drinking” or “heavy episodic drinking”, often defined as consuming five or more drinks on one occasion [usually defined as 2 hours] or by the subjective feeling of drunkenness), a different picture emerges. Here, in most countries, prevalence and average frequency increase sharply across the adolescent years, peak in young adulthood and subsequently decrease until retirement age [17, 18].
The “Addiction Monitoring in Switzerland” (AMIS) [19] project has been providing up-to-date evidence about alcohol and other substance use in the Swiss population since 2011. AMIS combines available data from routine reporting systems such as hospital statistics with data from a continuous rolling survey (i.e. representative subsurveys every 3 months) to provide comprehensive information on a large variety of addictive behaviours. In figure 1, which is based on almost 11,000 individuals, the bars represent the percentage of those who drink daily and those who consumed five or more drinks on a single occasion for men, and four or more for women (RSOD) at least once a month according to 10-year age categories (5-year for the two youngest age groups). These results confirm the general trend mentioned above. The percentage of daily drinkers is very small (below 2%) up to the age of 24 and increases steadily thereafter until age 75 and beyond. In contrast, with a prevalence of almost 40%, RSOD drinking peaks among 20- to 24-year-olds and steadily decreases over the age groups until age 75 and older. These results are consistent with a study among more than 3,500 19-year-old men in French-speaking Switzerland, which showed that 75.5% of drinkers had an RSOD day at least monthly and that 69.3% of the total weekly alcohol volume was consumed in the form of RSOD days in this group of young males [20].
Conclusion: RSOD prevalence and frequency increase sharply across the adolescent years, peak in young adulthood and subsequently decrease until retirement age.
When and why do young adults usually engage in risky drinking?
Day of the week
The lines in figure 1 represent the usual amounts consumed by drinkers on weekdays and weekend days when drinking occurred over the past 12 months. Whereas the amount consumed on weekend drinking days peaks among 20- to 24-year-olds and steadily decreases over the age groups until age 75 and beyond, the amount consumed on drinking days during the week increases almost steadily across the age groups and reaches its highest level among 65- to 74-year-olds. This also means that the discrepancy between drinking during the week and at weekends diminishes with age; thus a RSOD style often occurring at weekends changes into a more regular (e.g. daily), moderate drinking style when people grow older.
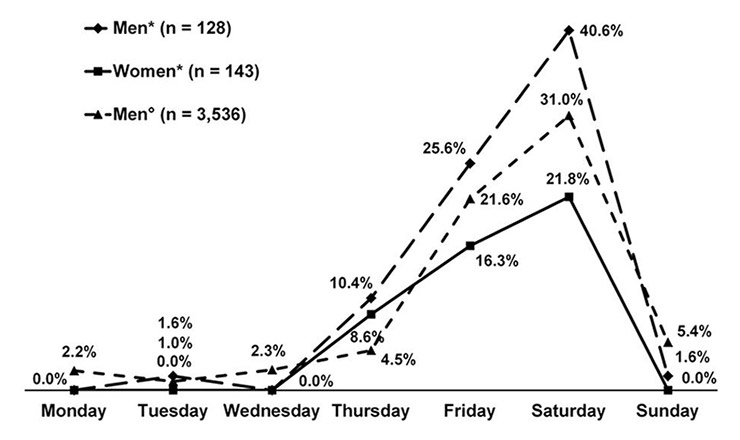
Figure 2
Percentage of individuals regularly consuming more than four drinks on a single occasion in the last 30 days by gender and day of the week.
Note: *mean age = 23.1 years, standard deviation = 3.1 years, data taken from Kuntsche and Labhart [23]; °19-year-olds, data taken from Gmel et al. [20]
Various international studies have reported that, over the course of the week, alcohol consumption peaks on Friday and Saturday when young people go out and do not have any work or study responsibilities the next day [21, 22]. Figure 2 summarises the results from two studies recently conducted in Switzerland [20, 23]. It is clearly visible that the percentage of RSO drinkers was very low from Sunday until Wednesday, increases from Thursday and peaks on Saturday. In fact, the percentage of RSO drinkers increased 14- to 40-fold on Saturdays compared with the beginning of the week. Overall, striking similarities in the shape of the graphs were found irrespective of gender, age, survey year and study design.
Although authors have argued that RSOD is particularly likely when young people go out in the evening on weekends [21, 22], there is surprisingly little epidemiological research documenting RSOD and amounts consumed according to the day of the week and the time of day. The results of one of the rare studies conducted among 747 current drinkers in Switzerland who were asked to complete a drinking diary six times a day covering 24 hours on seven consecutive days shows clearly that both the number of RSO drinkers and the consumed amounts peaked each day in the evening, that is, between 8 p.m. and midnight [24]. However, both peaks were highest on Saturday evenings, followed by Friday evenings.
Conclusion: over the course of the week, RSOD is most prevalent by far on Saturday evenings, followed by Friday evenings, usually because young people go out and do not have any work or study responsibilities the next day.
Weekend drinking patterns
Although it is clear from the literature that RSOD usually occurs on Fridays and Saturday evenings, less is known about how this happens, that is, how consumption progresses throughout the course of the evening to result in (very) high amounts in a relatively short timeframe. For this purpose, Kuntsche and Labhart [23] asked 183 young adult participants in Switzerland to complete five short questionnaires sent to their mobile phones each weekend evening, in order to be able to map the drinking progression from 6 p.m. until midnight. The results revealed that the later in the evening, the more young adults started to drink and also the more those who had already started drinking consumed. The authors concluded that young adults tend to increase the pace of drinking (“accelerate” the number of drinks consumed per hour), and this is particularly the case on Saturday evenings.
However, the increase in consumption throughout the course of the evening at weekends does not have to be linear or occur in the final locations of the evening alone. Recent evidence from North America and the United Kingdom suggests that young people’s heavy drinking occasions in public settings are often preceded by “predrinking” (also known as “prepartying” or “frontloading”), that is, alcohol is consumed in a private place (e.g. at home) or public place (e.g. a park) before going to a party or drinking establishment where more alcohol may or may not be consumed [25, 26]. A recent study among young adults in Switzerland revealed a significantly higher average number of drinks on evenings with predrinking (7.1 drinks) compared with on-premises only (4.2 drinks) and off-premises only (4.3 drinks) evenings [27]. Consistent with previous research, these results demonstrate that, rather than substituting for or reducing the amount subsequently consumed on-premises, predrinking adds to the amount of alcohol consumed on a given evening [26, 28]. Hence, although young people may engage in predrinking with the intention of saving money, they may end up spending and consuming more than planned.
Conclusion: drinking in private before going out (“predrinking”) and accelerating the pace of drinking (i.e. increasing the number of drinks per hour) was shown to play an important role in young adults’ RSOD on weekend evenings.
Motivation to engage in risky drinking
Most adolescents start drinking out of curiosity about the effects and to toast with others, whereas only very few do so to cope with negative feelings and problems [29]. Despite being few in number, this group is particularly problematic because coping motives were found to interact with genetic factors predisposing individuals to engage in frequent RSOD and to suffer alcohol-related problems in early adolescence and beyond [8–10], whereas for example, enhancement motives (i.e. drinking to seek excitement, to have fun and to feel the effects of alcohol) were not. Authors conclude that hereditary influences and biological pathways predispose individuals to drink to cope with negative affect and may explain vulnerability to stress-related drinking [9, 10].
While coping-motivated drinking stays on a relatively small scale throughout adolescence, the endorsement of enhancement motives in particular increases considerably [30]. Research on personality has shown that those who drink for enhancement motives tend to like and actively seek the sensation of feeling drunk as well as other extreme sensations owing to their extraverted, risk-seeking personality which is particularly common among males [31]. This argumentation and corresponding evidence is consistent with the development of a more general risk behaviour syndrome from early to late adolescence, as described above.
Accordingly, a longitudinal study among young adults in Switzerland revealed that enhancement motives assessed at baseline predicted the consumption of high amounts on Friday and Saturday evenings over and above usual consumption [32]. Another longitudinal study demonstrated that enhancement motives predicted RSOD and related consequences on Friday and Saturday evenings among young adults in Switzerland even when predrinking as an important situational factor was taken into account [33]. In this study, however, the effect was only found among men. Among women, only coping motives predicted RSOD and related consequences over time. Women may use alcohol to become more self-confident and to alleviate social anxiety and stress on a night out, for example when meeting new people.
Conclusion: in late adolescence and early adulthood, men in particular drink heavily at weekends to seek excitement, to have fun and to feel the effects of alcohol, which can be an expression of their extraverted, risk-seeking personality and embedded in a more general risk behaviour syndrome.
Where do young people engage in risky drinking and what are the particular problems associated with RSOD?
Drinking location
Research in the United States has shown that bars are frequented most often by young adults (aged 21‒30), whereas those under 21 mostly drink at friends’ and relatives’ homes, parties and special events, but rarely at home [34]. This was confirmed by Clapp and colleagues [35] showing that 87.1% of the last drinking occasions of college students below 21 years of age were at parties as opposed to 12.9% in bars. Particularly those with highly volatile drinking patterns (e.g. heavy drinking at weekends with low drinking during the week, which is typical for young people as described above) drink anywhere but home [34]. In Europe, the minimum purchase age is lower than in the United States. Consequently, results from the European School Survey Project on Alcohol and Other Drugs (ESPAD) [2] show that the majority of 15-year-olds in countries such as Belgium, Croatia, the Czech Republic, Greece, Hungary, Italy, Malta, Monaco, Romania, Serbia, Slovakia, Slovenia, and Ukraine had consumed alcoholic beverages on-premises during the last 30 days, in bars, discos, and so on. Later, between the ages of 16 and 25, about 80% of young people's alcohol use occurs in public settings, as shown by a Dutch study [36].
The recently conducted Cohort Study on Substance Use Risk Factors ( http://www.C-Surf.ch ) provides evidence on alcohol use at different drinking locations among 20-year-old men in Switzerland by means of a location-specific quantity-frequency instrument (table 1). These results show that in the past 12 months, about 20% of alcohol is consumed at home or at someone else's home, whereas about 80% of alcohol consumption occurs in public with bars/pubs, discos / night clubs, and festivals / special events being most frequently cited. These are also the locations where the highest quantities per occasion are consumed, the frequency of use in the past 12 months is highest, and where the highest proportion of alcohol users show the usual drinking pattern of RSOD (e.g. 40% of those who drink in bars and pubs show RSOD every time; 45% do so at festivals and 41% in discos or nightclubs). The proportion of those occasionally having episodes of RSOD will largely exceed these percentages.
In another Swiss study, Labhart and colleagues [27] used the cell phones of 183 young adults to assess their alcohol consumption and drinking location six times (from 5 p.m. until midnight) on Thursdays, Fridays, and Saturdays over five consecutive weeks (7,828 assessments in total). The results revealed that on 74.3% of all evenings with on-premises attendance, alcohol was consumed but only on 46.4% of evenings without on-premises attendance.
Conclusion: older adolescents and young adults predominantly drink outside the home, mostly in bars, pubs, discos, or at special events or festivals, often resulting in heavy-drinking occasions.
Adverse physical consequences
Alcohol is the number one risk factor for mortality and morbidity among young people in established market economies [37], particularly on account of intended injuries (violence, suicide) and unintended injuries (traffic casualties, falls and other injuries). The alcohol-related mortality and morbidity at this age is overwhelmingly related to acute consequences resulting from RSOD; mortality and morbidity due to chronic heavy intake such as liver cirrhosis is rare [38]. The particular drinking style among young people, that is, heavy drinking on weekends with abstinence or rather low intake on most days of the week (see details above), constitutes a particular risk for injuries.
Unfortunately, there are few studies on injuries in the field, which separate consequences related to heavy chronic intake from those of RSOD. Mostly, only acute alcohol intake prior to injury is measured. A high acute intake, however, may occur in chronic heavy drinkers as well as in occasional RSO drinkers. Borkenstein and colleagues [39] demonstrated that the same blood alcohol concentration (BAC) was associated with a 10-fold risk for traffic injury in very infrequent drinkers (e.g. those drinking only once a year or less) compared with the risk in daily drinkers [40]. In fact, given similar BAC, the relative risks increased as the frequency of drinking decreased.
In a Swiss diary study, Gmel and colleagues [24] compared drinking patterns by time of day and day of the week with police statistics relating to road traffic accidents. Traffic crash data were matched with alcohol use data from the diary as regards corresponding time of day and day of the week. The study provided strong support for a causal link between RSOD and road traffic accidents. The number of traffic casualties was disproportionately higher on Friday and Saturday nights in Switzerland, when commonly most of the RSOD drinking takes place. With regards to other injuries, not only traffic injuries, Gmel and colleagues [41] conducted a study in an emergency department to analyse the annual volume of drinking and annual frequency of RSOD, together with the acute alcohol intake 6 hours prior to coming to the hospital. Given the same amount of alcohol ingested 6 hours prior to injury, those who normally drank lightly (but with RSOD) were at higher risk compared with chronic heavy drinkers. An explanation for this is that frequent or chronic heavy drinkers may have a higher tolerance of the effects of alcohol, or may have learned to deal with situations under the influence of alcohol. Young people are often more “inexperienced” drinkers. In the case of traffic casualties, being an inexperienced drinker is exacerbated when combined with the unhappy mix of also being an inexperienced driver.
Another important aspect for experiencing alcohol-related harm is the drinking location. Drinking outside the home is generally considered riskier, for example because of the potential for drunk-driving [42]. The risk of involvement in aggressive acts is also higher in bars than in other locations even at the same level of intoxication [43].
In their cell phone-based diary study, Labhart and colleagues [27] asked 183 young adults in Switzerland on 1,441 evenings whether any of the following had occurred during the previous evening: hangover, injured self or someone else, black-out (not remember what happened), unplanned use of other substances, unintended or unprotected sexual intercourse, and property damage or vandalism. The results confirmed that participants were more likely to experience any of the six consequences and also the average number was higher after on-premises drinking evenings (in bars, pubs, discos, restaurants, etc.) than after off-premises evenings (e.g. at home). Labhart et al. [27] also compared evenings with off-premises-only consumption, on-premises-only consumption and the combination of both, so-called “predrinking” (see details above). Interestingly, the results revealed that neither the likelihood nor the number of consequences significantly differed between off-premises-only and on-premises-only evenings. Both types of evening drinking had a significantly lower level of adverse consequences than predrinking evenings, however. Thus, predrinking, which is particularly popular among young adults, constitutes an especially problematic drinking pattern, not only because of the accumulation of two different (heavy) drinking occasions but also because of the double risk of being involved in road traffic accidents and sustaining injuries when traveling to the on-premises locations already inebriated [25, 27].
Conclusion: intended and unintended injuries and other acute consequences due to RSOD are the main risk factors for mortality and morbidity in late adolescence and early adulthood. Being relatively inexperienced drinkers and inexperienced drivers, as well as drinking before even going out, is a particularly dangerous combination.
|
Table 1: Alcohol consumption of those drinking at a given location. |
|
|
Share of total consumption
|
n
|
Proportion of drinkers
|
Quantity1
|
Frequency1
|
Proportion of RSOD
|
| Bars, pubs |
26.7% |
5,091 |
94.9% |
4.6 |
47.3 |
40.3% |
| Discos, night clubs |
18.8% |
4,444 |
82.9% |
4.6 |
38.3 |
41.3% |
| At others’ homes |
12.3% |
4,882 |
91.0% |
3.9 |
25.4 |
28.7% |
| Festivals, special events |
12.1% |
4,528 |
84.4% |
5.0 |
29.2 |
45.3% |
| At home |
9.5% |
4,258 |
79.4% |
3.0 |
29.0 |
16.4% |
| Public places (parks, in the street, etc.) |
5.5% |
3,333 |
62.2% |
3.7 |
22.2 |
27.2% |
| Restaurants |
5.3% |
4,182 |
78.0% |
2.5 |
18.9 |
10.5% |
| Other leisure time locations (orchestra, shooting club, etc.) |
4.5% |
1,964 |
36.6% |
3.1 |
28.4 |
18.7% |
| When doing sports |
2.6% |
2,023 |
37.7% |
2.9 |
23.6 |
15.5% |
| At sport events |
2.1% |
2,415 |
45.0% |
3.1 |
16.0 |
17.2% |
| Cinemas, theatres |
0.7% |
1,363 |
25.4% |
2.3 |
11.6 |
8.1% |
| RSOD = risky single-occasion drinking
Note: Share of total alcohol use is calculated for all alcohol users (n = 5,362) whereas quantity, frequency and proportion of 5+ drinking is calculated for those alcohol users who drink in these locations; 1Mean values |
General conclusion
Consuming large amounts of alcohol in a short period of time (RSOD) is more common in late adolescence and early adulthood than in any other period in life. One of the reasons for this behaviour is a lack of maturity. From age 16 onwards, young people in Switzerland and many other European countries are legally allowed to buy and to drink alcohol as much as they like, they are confronted with ample developmental demands and transitions, such as leaving home, starting to earn a living, or living with a stable partner, but they do not yet have adult responsibilities to contend with, such as a career and family demands.
Examining young adults’ RSOD more closely revealed that (a) RSOD is by far most prevalent on Saturday evenings followed by Friday evenings, usually because young people go out and do not have any work or study responsibilities the next day; (b) RSOD results from drinking in private before going out (“predrinking”) and accelerating the pace of drinking (i.e. increasing the number of drinks per hour); (c) RSOD is often not accidental but purposeful: to seek excitement, to have fun and to feel the effects of alcohol; (d) RSOD occurs predominantly outside the home, mostly in bars, pubs, discos or at special events or festivals; (e) RSOD often results in intended and unintended injuries and other acute consequences, leading risk factors for mortality and morbidity in this age group.
Conclusion: alcohol consumption in late adolescence and early adulthood is problematic because it often occurs in the evening at weekends in bars, pubs and so on, in combination with predrinking, and often results in intoxication, injuries and other acute consequences, which are leading risk factors for mortality and morbidity.
Implications for preventive action
Although structural measures such as taxation to make alcoholic beverages less affordable have shown undisputed effects on reducing alcohol use in general, and in particular among young people because they are usually on a tighter budget [44], prevention should also take the particular patterns, situations and circumstances of young people's drinking into account. On the one hand, many young people drink heavily intentionally and will therefore continue to do so. On the other, most of them grow out of heavy drinking when they become more mature. Hence, no preventive concept whatsoever will be able to decrease young people's alcohol use to zero, but some preventive action may succeed in helping young drinkers to survive until they decide for themselves to drink more responsibly. This is particularly important because, as described above, young people engage in RSOD on weekend evenings intentionally, to seek excitement, to have fun and to feel the effects of alcohol, rather than by accident [32].
For example, results from the AMIS [19] demonstrate that young people often purchase alcohol on the day they drink it. Buying alcoholic beverages beforehand and stocking them is less common. Therefore, restricting the off-premises sale of alcohol after a certain time (e.g. 10 p.m.), for example, at gas service stations or in 24 hour shops, should prevent RSOD that often occurs on weekend nights in adolescence and young adulthood as described above. In Switzerland, for example, the ban on selling alcohol after 10 p.m. in kiosks and shops has reduced the rate of alcohol intoxication resulting in hospitalisation among young people [45]. Policies aimed at reducing both on-premises and off-premises opening hours have shown beneficial effects in other countries [46, 47].
However, increasing prices through taxation or restricting availability through reduced opening and selling hours may instigate intended predrinking [25, 28], which usually occurs in an unsupervised environment. Drinking (particularly in combination with other drug use) without any kind of formal or informal control or supervision is likely to lead to excess and therefore to particularly harmful consequences (of which Amy Winehouse, Bon Scott or Jimi Hendrix, who died from alcohol intoxication while alone are popular examples). Thus, approaches are needed to encourage young people to make safer choices when predrinking [48]. The Canadian prevention programme “Pre-Thinking While You’re Predrinking” [25], in which transportation is arranged both to and from public drinking venues, is a promising example of this. Moreover, the particular risk associated with inexperienced drivers could be counteracted by a graduated driving license system, for example with stronger restrictions as regards BAC for young drivers.
Despite the higher likelihood of violence and injuries, heavy drinking in bars, pubs, discos, etc. is less problematic because there is some kind of formal and informal control in place. For example, alcohol is served by waiters, and moderate drinkers may be around, creating an atmosphere or social norm in which drunkenness and public disturbance appear inappropriate or not tolerated, and adults and other persons are around who can provide immediate help or call the ambulance if people are badly injured or victims of violence. However, this only works if the persons present actually disapprove of drunkenness and public disturbance and are prepared to help in the event of an emergency, and if existing laws of not serving alcohol to underage or inebriated persons are strictly enforced. Staff training better to detect underage or inebriated patrons and to ensure responsible beverage service might also help prevent intoxication as well as consequences related to the fact that people have to move between places selling alcohol and their homes [49]. There are also many possible ways of designing the physical environment in bars to reduce the consequences of heavy drinking such as violence, for example by means of attractive furniture, avoidance of overcrowding and noise and open and clear access to the bar/waiters and toilets [50].
Conclusion: an effective strategy to prevent excessive drinking in late adolescence and early adulthood and the related harm should include both attempts to reduce heavy drinking occasions and strategies to minimise harm.
References
1 Currie C, Zanotti C, Morgan A, Currie D, De Looze M, Roberts C, et al. Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) study: international report from the 2009/2010 survey. Copenhagen: WHO Regional Office for Europe; 2012 [10.12.12]; Available from: http://www.euro.who.int/en/what-we-publish/abstracts/social-determinants-of-health-and-well-being-among-young-people.-health-behaviour-in-school-aged-children-hbsc-study.
2 Hibell B, Guttormsson U, Ahlström S, Balakireva O, Bjarnason T, Kokkevi AE, et al. The 2011 ESPAD Report – Substance Use Among Students in 36 European Countries. Stockholm: The Swedish Council for Information on Alcohol and Other Drugs (CAN); 2012.
3 International Center for Alcohol Policies (ICAP). Policy Table: Minimum Age Limits Worldwide. Washington, DC ICAP; 2012 [10.12.2012]; Available from: http://www.icap.org/PolicyIssues/YoungPeoplesDrinking/PolicyTableMinimumAgeLimitsWorldwide/tabid/206/Default.aspx.
4 Jessor R, Jessor SL. Problem Behavior and Psychosocial Development: A Longitudinal Study of Youth. New York: Academic Press; 1977.
5 Allen JP, Leadbeater BJ, Aber JL. The development of problem behavior syndromes in at-risk adolescents. Dev Psychopathol. 1994;6(2):323–42.
6 Kuntsche E. Progression of a general substance use pattern among adolescents in Switzerland? Investigating the relationship between alcohol, tobacco, and cannabis use over a 12-year period. Eur Addict Res. 2004;10(3):118–25.
7 Enoch M-A. The influence of gene-environment interactions on the development of alcoholism and drug dependence. Current Psychiatry Reports. 2012;14(2):150–8.
8 van der Zwaluw CS, Kuntsche E, Engels RCME. Risky alcohol use in adolescence: The role of genetics (DRD2, SLC6A4) and coping motives. Alcohol Clin Exp Res. 2011;35(4):756–64.
9 Mackie CJ, Conrod PJ, Rijsdijk F, Eley TC. A systematic evaluation and validation of subtypes of adolescent alcohol use motives: Genetic and environmental contributions. Alcohol Clin Exp Res. 2011;35(3):420–30.
10 Young-Wolff KC, Kendler KS, Prescott CA. Shared genetic contributions to early-onset drinking and drinking to cope motives. Addict Behav. 2012;37(10):1176–80.
11 Steinberg L. A social neuroscience perspective on adolescent risk-taking. Dev Rev. 2008;28(1):78–106.
12 Kuntsche E. Stellenwert der Gesundheit im Jugendalter. In: Kuntsche E, Delgrande Jordan M, editors. Gesundheit und Gesundheitsverhalten Jugendlicher in der Schweiz Ergebnisse einer nationalen Befragung. Bern: Verlag Hans Huber; 2012. p. 11–3.
13 Bachman JG, O'Malley HM, Schulenberg JE, Johnston LD, Bryant AL, Merline AC. The Decline of Substance Use in Young Adulthood: Changes in social Activities, Roles, and Beliefs. Mahwah, NJ: Lawrence Erlbaum; 2002.
14 Kuntsche S, Knibbe RA, Gmel G. Parents’ alcohol use: gender differences in the impact of household and family chores. Eur J Publ Health. 2012;22(6):894–9.
15 Rehm J, Room R, Monteiro MG, Gmel G, Graham K, Rehn N, et al. Alcohol use. In: Ezzati M, Lopez AD, Rodgers A, Murray CJL, editors. Comparative quantification of health Risks Global and regional burden of disease attributable to selected major risk factors. Geneva: World Health Organization (WHO); 2004. p. 959–1108.
16 Rehm J, Arminger G. Alcohol consumption in Switzerland 1987–93: adjusting for differential effect of assessment techniques on the analysis of trends. Addiction. 1996;91(9):1335–44.
17 Kuntsche E, Rehm J, Gmel G. Characteristics of binge drinkers in Europe. Soc Sci Med. 2004;59(1):113–27.
18 Gutjahr E, Gmel G. Defining alcohol-related fatal medical conditions for social-cost studies in Western societies: An update of the epidemiological evidence. J Subst Abuse. 2001;13:239–64.
19 Gmel G, Kuendig H, Maffli E, Notari L, Wicki M, Georges A, et al. Suchtmonitoring Schweiz / Jahresbericht – Daten 2011. Bern: Bundesamt für Gesundheit (BAG); 2012 [13.12.2012]; Available from: http://www.bag.admin.ch/themen/drogen/00042/13457/index.html?lang=de.
20 Gmel G, Gaume J, Faouzi M, Kulling J-P, Daeppen J-B. Who drinks most of the total alcohol in young men – Risky single occasion drinking as normative behaviour. Alcohol Alcohol. 2008;43(6):692–7.
21 Parker H, Williams L. Intoxicated weekends: Young adults’ work hard-play hard lifestyles, public health and public disorder Drugs Educ Prev Pol. 2003;10(4):345–67.
22 Van Wersch A, Walker W. Binge-drinking in Britain as a social and cultural phenomenon: The development of a grounded theoretical model. J Health Psychol. 2009;14(1):124–34.
23 Kuntsche E, Labhart F. Investigating the drinking patterns of young people over the course of the evening at weekends. Drug Alcohol Depend. 2012:319–24.
24 Gmel G, Heeb J-L, Rezny L, Rehm J, Mohler-Kuo M. Drinking patterns and traffic casualties in Switzerland – Matching survey data and police records to design preventive action. Public Health. 2005;119(5):426–36.
25 Wells S, Graham K, Purcell J. Policy implications of the widespread practice of “pre-drinking” or “pre-gaming” before going to public drinking establishments: Are current prevention strategies backfiring? Addiction. 2009;104(1):4–9.
26 Pedersen ER, LaBrie JW. Partying before the party: Examining prepartying behavior among college students. J Am Coll Health. 2007;56(3):237–45.
27 Labhart F, Graham K, Wells S, Kuntsche E. Drinking before going to licensed premises: An event-level analysis of predrinking, alcohol consumption, and adverse outcomes. Alcohol Clin Exp Res. 2013;37(2):284–91.
28 Hughes K, Anderson Z, Morleo M, Bellis MA. Alcohol, nightlife and violence: The relative contributions of drinking before and during nights out to negative health and criminal justice outcomes. Addiction. 2008;103(1):60–5.
29 Kuntsche E, Müller S. Why do young people start drinking? Motives for first-time alcohol consumption and links to risky drinking in early adolescence. Eur Addict Res. 2012;18(1):34–9.
30 Cooper ML. Motivations for alcohol use among adolescents: development and validation of a four-factor-model. Psychol Assessm. 1994;6(2):117–28.
31 Kuntsche E, Knibbe RA, Gmel G, Engels RCME. Who drinks and why? A review of socio-demographic, personality, and contextual issues behind the drinking motives in young people. Addict Behav. 2006;31(10):1844–57.
32 Kuntsche E, Cooper ML. Drinking to have fun and to get drunk: motives as predictors of weekend drinking over and above usual drinking habits. Drug Alcohol Depend. 2010;110(3):259–62.
33 Kuntsche E, Labhart F. Drinking motives moderate the impact of pre-drinking on a given evening and related adverse consequences – An event-level study. Addiction 2013 (in press).
34 Treno AJ, Alaniz ML, Gruenewald PJ. The use of drinking places by gender, age and ethnic groups: an analysis of routine drinking activities. Addiction. 2000;95(4):537–51.
35 Clapp JD, Reed MB, Holmes MR, Lange JE, Voas RB. Drunk in public, drunk in private: the relationship between college students, drinking environments and alcohol consumption. Am J Drug Alcohol Abuse. 2006;32(2):275–85.
36 Knibbe RA, Oostveen T, van de Goor I. Young people’s alcohol consumption in public drinking places: Reasoned behaviour or related to the situation? British Jounal of Addiction. 1991;86:1425–33.
37 Rehm J, Taylor B, Room R. Global burden of disease from alcohol, illicit drugs and tobacco. Drug Alcohol Rev. 2006;25(6):503–13.
38 Gmel G, Kuntsche E, Rehm J. Risky single-occasion drinking: bingeing is not bingeing. Addiction. 2011;106(6):1037–45.
39 Borkenstein RF, Crowther FR, Shumate RP, Ziel WB, Zylman R. The role of the drinking driver in traffic accidents (The Grand Rapids Study). Blutalkohol. 1974;11( Suppl. 1):1–131.
40 Hurst PM, Harte D, Frith WJ. The Grand Rapids dip revisited. Accid Anal Prev. 1994;26(5):647–54.
41 Gmel G, Bissery A, Gammeter R, Givel J-C, Calmes J-M, Yersin B, et al. Alcohol-attributable injuries in admissions to a Swiss emergency room – An analysis of the link between volume of drinking, drinking patterns and preattendance drinking. Alcohol Clin Exp Res. 2006;30(3):501–9.
42 Usdan SL, Moore CG, Schumacher JE, Talbott LL. Drinking locations prior to impaired driving among college students: implications for prevention. J Am Coll Health. 2005;54(2):69–75.
43 Graham K, Osgood DW, Wells S, Stockwell T. To what extent is intoxication associated with aggression in bars? A multilevel analysis. J Stud Alcohol Drugs. 2006;67:382–90.
44 Wagenaar AC, Salois MJ, Komro KA. Effects of beverage alcohol price and tax levels on drinking: a meta-analysis of 1003 estimates from 112 studies. Addiction. 2009;104(2):179–90.
45 Wicki M, Gmel G. Hospital admission rates for alcoholic intoxication after policy changes in the canton of Geneva, Switzerland. Drug Alcohol Depend. 2011;118(2-3):209–15.
46 Stockwell T, Gruenewald PJ. Controls on the physical availability of alcohol. In: Heather N, Peters TJ, Stockwell T, editors. The International Handbook of Alcohol Dependence and Problems. Chichester, UK: Wiley; 2004.
47 Popova S, Giesbrecht N, Bekmuradov D, Patra J. Hours and days of sale and density of alcohol outlets: Impacts on alcohol consumption and damage: A systematic review. Alcohol Alcohol. 2009;44(5):500–16.
48 Glindemann KE, Ehrhart IJ, Maynard ML, Geller S. Alcohol front-loading among college students: exploring the need for prevention intervention. J Alcohol Drug Educ. 2006;50:5–13.
49 Graham K, Jelley J, Purcell J. Training bar staff in preventing and managing aggression in licensed premises. J Subst Use. 2005;10(1):48–61.
50 Homel R, McIlwain G, Carvolth R. Creating safer drinking environments. In: Heather N, Peters TJ, Stockwell T, editors. International Handbook of Alcohol Dependence and Problems – Part VI: Prevention of Alcohol Problems. Chichester: John Wiley & Sons Ltd.; 2001. p. 721–40.