Profiles of drug users in Switzerland and effects of early-onset intensive use of alcohol, tobacco and cannabis on other illicit drug use
DOI: https://doi.org/10.4414/smw.2013.13805
Stéphanie
Baggio, Joseph
Studer, Meichun
Mohler-Kuo, Jean-Bernard
Daeppen, Gerhard
Gmel
Summary
QUESTIONS UNDER STUDY / PRINCIPLES: The main aim of this study was to investigate profiles of drug users, with a particular focus on illicit drugs other than cannabis, and to explore the effect of early-onset intensive use (drunkenness, daily smoking, high on cannabis) on profiles of illicit drug use.
METHODS: Baseline data from a representative sample of 5,831 young Swiss men in the ongoing Cohort Study on Substance Use Risk Factors were used. Substance use (alcohol, tobacco, cannabis and 15 types of other illicit drug) and age of onset of intensive use were assessed. The Item Response Theory (IRT) and prevalence rates at different ages of onset were used to reveal different profiles of illicit drug use.
RESULTS: In addition to cannabis, there were two profiles of other illicit drug use: (a) “softer” drug users (uppers, hallucinogens and inhaled drugs), among which ecstasy had the highest discriminatory potential (IRT slope = 4.68, standard error (SE) = 0.48; p <0.001); and (b) “harder” drug users (heroin, ketamine, gamma-hydroxybutyrate/gamma-hydroxylactone, research chemicals, crystal meth and spice), among which ketamine had the highest discriminatory potential (slope = 4.05; SE = 0.63; p <0.001). Onset of intensive use at the age of 12 years or younger also discriminated between these two profiles.
CONCLUSION: Both the IRT model and the effect of onset of intensive use enabled two groups of illicit drugs to be identified. In particular, very early onset (at 12 years or younger) intensive use of any substance was a marker for later use of the second group of drugs.
Introduction
The stages of involvement in drug use are commonly agreed upon [1–5]. The sequence goes from the use of licit drugs (alcohol and tobacco) to cannabis use, and then the use of other illicit drugs [6–13]. However, although there are many studies on the pathway from licit drug use to cannabis use, and finally to other illicit drugs, there is not much detailed information about the potential stages of the use of illicit drugs other than cannabis. Researchers mostly refer to “hard drug use” [1, 14, 15] and aggregate all illicit drugs apart from cannabis into a single class [2], without providing any information on their potential sequential use. Occasionally, studies have reported that heroin use is the final stage of the sequence [8, 16, 17]. The use of cocaine, gamma-hydroxybutyrate/gamma-hydroxylactone (GHB/GBL) and ketamine is more common among people with extensive drug histories and seems to occur late in the sequence of illicit drug use [18]. The most common order appears to be cannabis, pills, cocaine and then heroin [7], but this order is sometimes described as unstable [19, 20]. The present study provides insight into the profiles of the users of illicit drugs other than cannabis. With a large sample size, differences between 15 types of illicit drug besides cannabis were analysed.
The literature also shows that early use of cannabis or alcohol is an important predictor of drug-use trajectories [7, 21–24]. Early alcohol, tobacco and cannabis use are three of the most relevant factors influencing use of other illicit drugs [16]. Studies have tended to look at early-onset use generally, rather than at whether intensive early-onset use (of alcohol, tobacco or cannabis) is associated with later use of illicit drugs other than cannabis. However, early drunkenness poses a greater risk of behavioural problems among adolescents than simple early onset of alcohol use [22].
The present study had two objectives. The principal aim was to identify the profiles of users of the most common drugs. We use “profiles of drug users” instead of “stages of drug use” because of the cross-sectional design of the study. However, even cross-sectional studies enable examination of sequential phenomenon [25]. The gateway theory has been studied from two perspectives: temporal sequences of drug use [26], and the strength of the association between drugs [25, 27, 28] as used in this study. The study also explored the effect of intensive early-onset use of alcohol, tobacco and cannabis on the likelihood of initiating other illicit drug use, that is, the effect of the first experience of being drunk or of being high on cannabis. We also investigated the age of onset of intensive tobacco use (i.e. daily smoking); smoking is less frequently described as a gateway drug, but this study aimed to provide further information on its effect. An additional aim was to provide data on the prevalence of drug use among young Swiss men; indeed, data on drug use are scarce in Switzerland, where no detailed information comparable to that provided by studies in various other European coutries is available (see for example the European Monitoring Centre for Drugs and Drug Addiction [EMCDDA] studies in the European Union, e.g. http://www.emcdda.europa.eu).
|
Table 1: Participants’ characteristics. |
|
Sociodemographic variables
|
|
| Age (years) mean (standard deviation) |
20.0 (1.24) |
| Language |
|
| |
French-speaking |
55.4% |
| |
German-speaking |
44.6% |
| Civil status |
|
| |
Single |
94.9% |
| |
Living with a partner |
4.4% |
| |
Maried |
0.4% |
| Education |
|
| |
Primary (9 years) |
48.2% |
| |
Secondary (12 years) |
26.2% |
| |
Tertiary and higher (>13 years) |
25.6% |
| Family income |
|
| |
Below average |
14.5% |
| |
Average |
41.4% |
| |
Above average |
44.1% |
| Residence |
|
| |
Urban |
41.4% |
| |
Rural |
58.6% |
Methods
The data used in this study were derived from the Cohort Study on Substance Use Risk Factors (C-SURF), a longitudinal study designed to assess substance use patterns and related consequences in young Swiss men. The protocol (Protocol No. 15/07) was approved by the Ethics Committee for Clinical Research of Lausanne University Medical School. Participants were selected at three of six army recruitment centres, in Lausanne (French-speaking) and Windisch and Mels (German-speaking), between August 23, 2010 and November 15, 2011. These three centres cover 21 of the 26 cantons in Switzerland, including all French-speaking cantons. The recruitment centres cover the smaller inner Cantons of Switzerland in the rural region of the Alps, but also large Swiss cities (Basel for the German-speaking region, Geneva and Lausanne for the Francophone region and Bern for the bilingual area). The German-speaking centres were suggested by the army administration because they were the biggest centres with the highest number of people going through the recruitment process. We avoided the Ceneri (the centre for Italophone men), mainly for organisational reasons and to avoid running a study in three different languages (Italophones represent less than 5% of the Swiss population). Thus, the study is largely representative of all Swiss men, although the upper North of Switzerland and particularly the Zurich region was not represented. Army recruitment is mandatory in Switzerland; therefore, all young men around 20 years old were eligible for study inclusion. Briefly, of the 13,245 conscripts informed about the study, 7,563 (57.1%) gave written consent to participate and 5,990 (79.2%) of these filled out the baseline questionnaire. More details about sampling and nonresponse are provided in Studer et al. [29]. Briefly, nonrespondents were more likely to be substance users and used substances more frequently. In general, however, differences between respondents and nonrespondents were small and probably only significant because of the large sample size. Missing values among participants were listwise deleted, so the study ultimately included 5,831 participants (97.4% of the sample).

Figure 1
Criterion information curves for drug use.
The criterion information curves represent how each criterion measured the underlying latent trait. The point on the x-axis where the probability of endorsement (y-axis) is 50% determined the severity parameter. The discrimination parameter of each criterion is the slope: the steeper slopes had higher discrimination parameters. Thus, ecstasy and ketamine discriminate very strongly between different drug users (high values on the y-axis), whereby ecstasy is less severe (more left = 1.59) compared with ketamine (more to the right with severity = 2.23) as regards the latent trait (substance use severity). (Detailed values can be found in table 4.)

Figure 2
Prevalence rates of drug use according to age of first getting high with cannabis.
The prevalence rate for each drug is given according to the age of first getting high with cannabis. For example, 14.9% of the participants who first got high with cannabis at age 12 years or earlier used heroin, whereas only 2.4% of the participants who first got high with cannabis at age 13 to 15 used heroin (percentages can be found in table 5).
Illicit drug use
Fifteen questions measured lifetime use of illicit drugs; answers were coded as “used” or “nonused”. The substances were as follows: (1.) hallucinogens, magic mushrooms, psylocibin, peyote, mescalin; (2.) other hallucinogens (lysergide [LSD], phencyclidine [PCP, Angel Dust], 4-bromo-2,5-dimethoxyphenethylamine [2C-B], 2,5-dimethoxy-4-iodophenethylamine [2C-I]); (3.) Salvia divinorum; (4.) speed; (5.) amphetamine, metamphetamine, amphetaminsulfate (e.g. Dexedrine, Benzedrine); (6.) crystal meth (ice); (7.) poppers (amylnitrite, butylnitrite); (8.) solvent sniffing (e.g. glue, solvent and gases such as benzine, ether, toluol, trichloroethylene, nitrous oxide); (9.) ecstasy, 3,4-methylenedioxy-N-methylamphetamine (MDMA); (10.) cocaine, crack, freebase; (11.) heroin; (12.) ketamine (Special K), dextromethorphan (DXM); (13.) GHB / GBL / I-4 Butandiol (BDB); (14.) research chemicals (e.g. mephedrone, butylone and methedrone); and (15.) spices or similar substances. Use of these drugs over the previous 12 months was also assessed.
Cannabis use
Cannabis use was assessed by asking participants if they had ever smoked cannabis (hashish, marijuana or grass) before; the study will refer to cannabis, the most common term, but the principal psychoactive constituent of cannabis is delta-9-tetrahydrocannabinol (THC). Answers were coded as “used” or “nonused”. They were also asked at what age they had got high on cannabis for the first time. Lifetime use was assessed instead of previous 12-month use, because the aim was to analyse the effects of early onset of cannabis use on stages of other lifetime drug use, and not only current consumption. The relevant age of onset of intensive use (first time high) was selected as follows: “age 12 years or earlier”, “age 13 to 15 years”, “age 16 to 18 years”, “age 19 years or older” and “never” (noncannabis users and participants who had never got high with cannabis). Previous studies reported that those who first used cannabis before the age of 12 were twice as likely to have severe mental illness (SMI) as those who first used cannabis at the age of 18 or older ([30], see p. 69 for SMI definition). Early cannabis use (before the age of 16) predicted later dependence [31], and cannabis use at the age of 18 or younger predicted impairment and irreversible harm [32]. These categories were selected to test the effect of early intensive use rather than early initiation.
Tobacco use
Participants were asked if they had ever smoked. They were recorded as users if they had smoked at least 50 cigarettes, or 10 water pipes, or 25 cigars or cigarillos, or 25 pipes. Twelve-month use was similarly assessed. Age of onset of intensive use was assessed using the age at which participants started to smoke daily. The same age categories as those for cannabis were used.
Alcohol use
Alcohol use was assessed by asking participants if they had had a total of at least 12 drinks of any kind of alcohol in their entire life. Answers were coded as “used” or “nonused”, and 12-month use was also assessed. Participants were asked how old they were when they got drunk for the first time. The same age categories as those described above were used.
Statistical analysis
The item-response theory (IRT) was used to define profiles of drug users. The IRT is a latent trait theory, which supposes that an item is a function of an unobservable or latent trait. It assumes that each item does not have the same level of severity, unlike Likert scaling, which assumes that the different items are equivalent. The IRT orders the items according to their severity level across the underlying trait [33]. Different IRT models can be used. We selected the two-parameter logistic model [34, 35] after checking the unidimensionality of the construct (a prerequisite for IRT) with an exploratory factorial analysis for ordinal data (WLSMV: weighted least squares means and variance adjusted estimation). This model defines the relationship between the observed data and an underlying latent construct with two parameters: a severity parameter (threshold) and a discrimination parameter (slope). The severity parameter reveals whether each criterion (each drug in the current study) is endorsed less frequently, for example, is more “severely” reported. This parameter is the point of the latent construct where there is 50% endorsement. The discrimination parameter is represented by the steepness of the slope and shows the ability of a criterion to discriminate between participants who are low or high on the latent construct. These two parameters were plotted graphically on a “criterion information curve.”
Proportion tests (z-tests) were used to explore the effect of the age of onset of intensive use of alcohol, tobacco or cannabis on illicit drug use. Comparisons were made between the proportions of users of each drug who initiated intensive use at 16 to 18 years of age and those who initiated at 13 to 15 years of age. The 13 to 15 onset group was similarly compared with the adjacent 12 years or younger onset group. We also ran logistic regression models separately with each illicit drug as the outcome and onset of intensive use as exposure, while controlling for the actual age of respondents. However, as age at conscription was very homogeneous, we did not report these models separately. Differences between models adjusted for age and models without adjustment were negligible as expected, and did not result in any different findings.
|
Table 2: Lifetime use and use in the previous 12 months. |
|
|
Percentage users (n = 5,831)
|
|
Lifetime
|
Previous 12 months
|
| Total (at least one drug used) |
95.8 (n = 5,586) |
94.2 (n = 5,493) |
| Alcohol |
94.8 |
92.9 |
| Tobacco |
60.4 |
45.7 |
| Cannabis |
47.6 |
30.7 |
| Hallucinogens / magic mushrooms |
5.7 |
2.8 |
| Ecstasy |
5.7 |
3.7 |
| Cocaine |
5.5 |
3.2 |
|
Salvia divinorum
|
5.2 |
2.2 |
| Poppers |
5.2 |
2.4 |
| Solvent sniffing |
4.8 |
2.2 |
| Speed |
4.7 |
2.6 |
| Other hallucinogens |
4.2 |
2.3 |
| Amphetamine/methamphetamine |
3.4 |
2.0 |
| Spice |
1.4 |
0.5 |
| Ketamine |
1.3 |
0.6 |
| GHB/GBL |
1.2 |
0.5 |
| Crystal meth |
1.1 |
0.4 |
| Research chemicals |
1.1 |
0.5 |
| Heroin |
1.0 |
0.4 |
| GBH = gamma-hydroxybutyrate; GBL = gamma-hydroxylactone |
|
Table 3: Intensive use onset: percentage of participants by age categories. |
|
|
Nonusers / No intensive onset
|
≥19 years
|
16–18 years
|
13–15 years
|
≤12 years
|
| High on cannabis |
59.9 |
2.2 |
22.2 |
14.0 |
1.7 |
| Daily smoking |
68.4 |
2.8 |
20.0 |
8.0 |
0.7 |
| Drunkenness |
12.6 |
3.4 |
38.7 |
43.0 |
2.3 |
Results
Prevalence of substance use
The participants’ characteristics are described in table 1. The prevalence rates of substance use are given in table 2. Only 4.2% of participants did not use any drugs, and the most prevalent drugs were licit drugs. Alcohol was the most prevalent (95.8% for lifetime use), followed by tobacco (94.8%), then cannabis (47.6%), and finally the other illicit drugs. Hallucinogens (magic mushrooms 5.7%, other hallucinogens 4.2%, Salvia divinorum 5.2%), uppers (speed 4.7%, ecstasy 5.7%, cocaine 5.5%, amphetamines/methamphetamines 3.4%) and inhaled drugs (poppers 5.2%, solvents, 4.8%) had a prevalence of approximately 4% to 5% (except for amphetamines and methamphetamines). The remaining illicit drugs (ketamine, heroin, GHB/GBL, research chemicals such as mephedrone or butylon, crystal meth and spice) had a lower prevalence of approximately 1%.
Table 3 illustrates the percentages of respondents broken down by age of first drunkenness, first daily smoking and first time being high on cannabis. Between 13 and 18 years of age, a total of 36.2% of participants had got high on cannabis, 28% had smoked daily, and 81.7% had got drunk for the first time. Late or early intensive use was less prevalent. Intensive alcohol use was more prevalent than intensive cannabis use, and intensive tobacco use was the least prevalent.
IRT model parameters and criterion information curves
The unidimensionality of the data was first checked with an exploratory factorial analysis. The first factor explained 71.04% of the variance. The IRT model parameters and associated criterion information curves for each drug are shown in table 4 and figure 1. Severity was lowest for alcohol, tobacco and cannabis, and greatest for spice, ketamine, GHB/GBL, crystal meth, research chemicals, heroin, solvent sniffing and poppers. The other drugs were intermediate in terms of severity. Discrimination was low for alcohol, tobacco, cannabis and inhaled drugs (poppers and solvents), and high for ecstasy and ketamine.
Comparison of drug users by age of onset of intensive use
The results of the proportion comparisons are summarised in tables 5, 6 and 7; figures 2, 3 and 4 give an overview of the prevalence rates for different ages of onset of intensive use. The higher the number of participants who got high on cannabis at an early age, the greater the increase in the proportion of users of each drug within the age classes of onset of intensive use of cannabis (table 5). For example, 33.7% of those who got high at the age of 12 or earlier also used cocaine, whereas only 20.7% of those who got high between 13 and 15 did so. The proportions began to increase at age 13 to 15 for most of the drugs (hallucinogens and uppers, as described in the previous section), but only at an onset of intensive cannabis use at 12 or earlier for ketamine, GHB/GBL, heroin, research chemicals, crystal meth and spice (fig. 2). There were no statistical differences in proportions between cannabis use onset at 16 to 18 compared with 13 to 15 for these drugs.
The patterns were quite similar for onset of intensive use of alcohol (table 6, fig. 3), with a commonly observed steep increase from 13 to 15 to 16 to 18 for first drunkenness. The effects were only significant as a tendency (p <0.10) for solvents (comparison of age 16–18 and 13–15), GHB/GBL and heroin (comparison of age 13–15 and 12 and younger). The differences between 13 to15 and 12 and younger for ketamine, research chemicals, crystal meth and spice were smaller for onset of intensive alcohol use than for onset of intensive cannabis use.
Finally, for the age of onset of intensive tobacco use, the results showed similar tendencies, except for solvents, for which proportions did not differ between the 16 to18 and 13 to 15 age groups (table 7). Salvia divinorum and poppers showed differences only at borderline significance levels (p <0.10) between 16 to 18 and 13 to 15. The patterns were a little less clear than for onset of intensive cannabis and alcohol use (see fig. 5), but the prevalence for very early onset of daily smoking was similar to that for cannabis onset and inferior to that for early alcohol onset.
|
Table 4: Criterion response model parameters. |
|
|
Severity =threshold
|
Discrimination = slope
|
| Alcohol |
–3.35 (0.06)*** |
0.59 (0.00) |
| Tobacco |
–0.32 (0.02)*** |
1.39 (0.08)*** |
| Cannabis |
0.08 (0.02)*** |
1.41 (0.08)*** |
| Hallucinogens / magic mushrooms |
1.78 (0.05)*** |
1.93 (0.12)*** |
| Ecstasy |
1.59 (0.03)*** |
4.68 (0.48)*** |
| Cocaine |
1.68 (0.04)*** |
2.95 (0.22)*** |
|
Salvia divinorum
|
1.93 (0.05)*** |
1.62 (0.09)*** |
| Poppers |
2.22 (0.08)*** |
1.13 (0.07)*** |
| Solvent sniffing |
2.49 (0.11)*** |
0.94 (0.06)*** |
| Speed |
1.72 (0.04)*** |
3.38 (0.30)*** |
| Other hallucinogens |
1.76 (0.04)*** |
3.63 (0.36)*** |
| Amphetamine/methamphetamine |
1.85 (0.04)*** |
3.55 (0.35)*** |
| Spice |
2.46 (0.09)*** |
1.99 (0.20)*** |
| Ketamine |
2.23 (0.06)*** |
4.05 (0.63)*** |
| GHB/GBL |
2.36 (0.08)*** |
2.85 (0.34)*** |
| Crystal meth |
2.43 (0.09)*** |
2.52 (0.28)*** |
| Research chemicals |
2.42 (0.09)*** |
2.64 (0.38)*** |
| Heroin |
2.42 (0.08)*** |
2.86 (0.39)*** |
| Standard errors are given in parentheses.
*** p <0.001;
GBH = gamma-hydroxybutyrate; GBL = gamma-hydroxylactone |
|
Table 5: Proportion of users of each drug within age categories of onset of intensive use of cannabis. |
|
|
First cannabis high
|
z-tests
|
|
Nonuser
n = 3,484
|
≥19
n = 129
|
16–18
n = 1,299
|
13–15
n = 819
|
≤12
n = 100
|
16–18/
13–15
|
13–15/
≤12
|
| Hallucinogens / magic mushrooms |
0.009 |
0.047 |
0.071 |
0.207 |
0.337 |
–5.189*** |
–3.822*** |
| Ecstasy |
0.009 |
0.031 |
0.069 |
0.211 |
0.366 |
–5.427*** |
–4.507*** |
| Cocaine |
0.008 |
0.031 |
0.069 |
0.207 |
0.337 |
–5.198*** |
–3.759*** |
|
Salvia divinorum
|
0.020 |
0.039 |
0.064 |
0.182 |
0.347 |
–4.495*** |
–4.687*** |
| Poppers |
0.025 |
0.070 |
0.080 |
0.120 |
0.188 |
–1.650* |
–2.337*** |
| Solvent sniffing |
0.007 |
0.062 |
0.060 |
0.099 |
0.257 |
–1.713* |
–5.004*** |
| Speed |
0.007 |
0.047 |
0.052 |
0.172 |
0.317 |
–4.537*** |
–4.006*** |
| Other hallucinogens |
0.007 |
0.016 |
0.050 |
0.143 |
0.327 |
–3.523*** |
–4.910*** |
| Amphetamine/methamphetamine |
0.006 |
0.023 |
0.037 |
0.118 |
0.267 |
–3.057** |
–3.839*** |
| Spice |
0.005 |
0.008 |
0.009 |
0.036 |
0.168 |
–1.171 |
–2.862** |
| Ketamine |
0.005 |
0.008 |
0.011 |
0.032 |
0.168 |
–0.889 |
–2.850** |
| GHB/GBL |
0.005 |
0.008 |
0.008 |
0.032 |
0.119 |
–1.003 |
–1.947* |
| Crystal meth |
0.005 |
0.008 |
0.007 |
0.028 |
0.158 |
–0.923 |
–2.638** |
| Research chemicals |
0.006 |
0.008 |
0.005 |
0.029 |
0.109 |
–1.055 |
–1.808* |
| Heroin |
0.005 |
0.008 |
0.005 |
0.024 |
0.149 |
–0.873 |
–2.498** |
| Z-tests for difference in use proportions between age 16–18 and 13–15, and between 13–15 and 12 or younger. Example of proportions: 0.366 for ecstasy means that 36.6 of those respondents who started getting high on cannabis at age 12 or younger also used ecstasy at least once in their lives.
*** p <0.001, ** p0< .01, * p <0.05, # p <0.10
GBH = gamma-hydroxybutyrate; GBL = gamma-hydroxylactone |
Discussion
Principal findings and implications
The results of the IRT model were in accordance with the results of previous studies: the profiles of drug users went from licit drug users (first alcohol users, then alcohol and tobacco users), to cannabis users and then to users of harder illicit drugs. However, there was not one but two profiles for the other illicit drug users. Hallucinogens such as magic mushrooms, LSD and Salvia divinorum, uppers like speed, ecstasy, cocaine, amphetamines and methamphetamines, and inhaled drugs (known as recreational drugs) such as poppers or solvents constituted the first profile of other illicit drug users, with ecstasy having the strongest discriminatory potential. A second profile was formed for the other users of other “hard” drugs, like ketamine, heroin, GHB/GBL, research chemicals, crystal meth and spice. The results showed that use of these drugs was less prevalent among participants, and that their severity parameters were higher than for the earlier drugs in the IRT model. Thus, the profiles of drug users included a distinction between “soft” illicit drug users and “hard” illicit drug users. Interestingly, cocaine resembled a “soft drug”, despite commonly being regarded as a “hard drug” in terms of potential for dependence or harm. These results may indicate different stages of drug use, from middle-stage drugs to final-stage drugs, which come later, as the prevalence rates suggested. However, this result needs to be tested in a study of longitudinal design, or using data on self-reported onset for each drug [25].

Figure 3
Prevalence rates for drug use according to age at first drunkenness.The prevalence rate for each drug is given according to the age of onset of being drunk. For example, 7.0% of the participants who first got drunk at age 12 years or earlier used heroin, whereas only 1.3% of the participants who first got drunk at age 13 to 15 used heroin (percentages can be found in table 6).
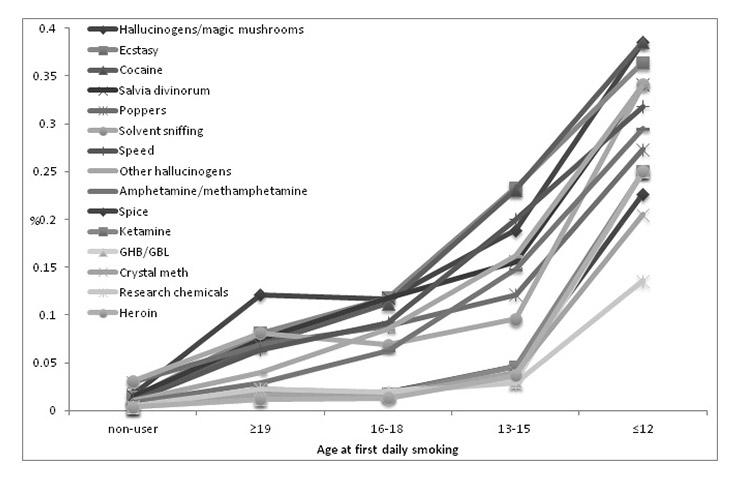
Figure 4
Prevalence rate of drug use according to age at first daily smoking.
The prevalence rate for each drug is given according to the age of onset of daily smoking. For example, 25.0% of the participants who smoked daily at age 12 years or earlier used heroin, whereas only 3.7% of the participants who smoked daily at age 13 to 15 used heroin (percentages can be found in table 7).
The results of the proportion comparisons showed the importance of an early age of onset of intensive use of cannabis, tobacco and alcohol in predicting an increased risk of drug use. The earlier the age of onset of intensive use of these drugs, the greater the risk of going on to use other illicit drugs. A difference was identified between drugs in the “soft” drug users profile (hallucinogens: magic mushrooms, other hallucinogens, Salvia divinorum; uppers: ecstasy, cocaine, speed, amphetamines/methamphetamines; and inhaled drugs: poppers, solvents) and those in the “hard” drug users profile (ketamine, GHB/GBL, heroin, research chemicals, crystal meth and spice). The risk of using the “soft” drugs substantially increased when participants first got high with cannabis, smoked daily or were drunk at 13 to 15 years of age, while the risk of using the “hard” drugs started to increase when participants first got high with cannabis, smoked daily or were drunk at the age of 12 or younger. Therefore, onset of intensive use at an early age (15 or younger) particularly increased the risk of using “soft” drugs, whereas onset of intensive use at a very early age (12 or younger) particularly increased the risk of using “hard” drugs. We identified two groups of illicit drugs, one where the prevalence rate increased with an onset at age 15 or younger and one with an onset of 12 or younger, as we found these two groups of illicit drugs in the IRT model. This pattern was more evident for onset of intensive use of cannabis, and less clear for onset of intensive use of tobacco and alcohol. Cannabis seemed to be a more important precursor for other drug use (heroin, ketamine, GHB/GBL, crystal meth, research chemicals and spice) than these two other licit drugs. Similar conclusions regarding alcohol were also reached by Golub and Johnson [36] in the United States.
Daily smoking onset showed a less clear picture than cannabis. However, very early onset of daily smoking (at 12 years of age or younger) resulted in a high prevalence of drug use similar that of to cannabis, and a higher prevalence rate than alcohol use. Tobacco is described as a gateway drug less frequently than alcohol and cannabis [22–24], but it appears that very early onset of daily smoking may be as predictive for later illicit drug use as very early cannabis onset. Smoking nowadays is likely to be regarded as deviant behaviour or predictive of later deviant behaviours such as cannabis use, particularly at young ages [37, 38], whereas alcohol use is a more accepted norm [39, 40]. In general, however, very early onset of any of these three substances was associated with use of even the less common, “soft” drugs. This may mean that early onset of intensive use of any drug is an expression of a common general liability, a general syndrome of deviance or a problematic behavioural syndrome [41, 42], rather than an expression of a causal drug use sequence in terms of gateway drugs. However, any early intense substance use should be taken as a clear warning sign and marker of the need for early treatment and intervention.
The third aim of the study was to provide data on the prevalence rates of drug use in Switzerland. The results showed that cannabis was the most prevalent illicit drug, with 47.6% of this sample of young men being lifetime users. In the European Union, the lifetime prevalence rate of cannabis use is around 32% (2.9%‒45.5%) for ages 15 to 34 [43]. However, men use cannabis more often than woman and the present sample was composed exclusively of men. Hallucinogens (magic mushrooms, other hallucinogens, Salvia divinorum) and uppers (ecstasy, cocaine, speed, amphetamines/methamphetamines) had a prevalence rate between 3.4% and 5.7%. The prevalence rate of amphetamines, ecstasy and cocaine was congruent with European results (5% [0.1–14.3], 5.5% [0.6–12.7] and 5.9% [0.1–13.6], respectively). Cocaine is the second most experimented-with drug after cannabis in the Europe Union (EMCDDA, 2011). Some other more uncommon drugs such as Salvia divinorum and spice, which often have a high media profile, still have a relatively low prevalence in Switzerland.
Strengths and limitations
The likelihood of drug use depends on several factors, including family structure, peer influence, availability, school factors, neighbourhood, social norms, personality and interactions between biological, psychological and social factors [44, 45]. In other words, the stages of drug use and the profiles of drug users depend on context and culture [46], as well as the frequency of use of each drug. For example, cocaine was easily available in Switzerland when the study took place and could be described as a “fashionable” drug. In contrast, heroin was less available and more expensive in 2011 than now (e.g. http://www.bag.admin.ch).
This investigation was the baseline study of C-SURF and had a cross-sectional design. The order of drug use was inferred on the basis of analyses that reflected hierarchical use and the effect of early intensive use of cannabis or alcohol. The profiles were inferred mainly from use prevalence because age of onset was not recorded for all drugs. To extend this result from profiles (cross-sectional perspective) to stages (longitudinal perspective), longitudinal designs are needed in order to verify the hypothesis of an escalation from “soft” illicit drugs to “hard” illicit drugs. C-SURF is a longitudinal study, and follow-up studies will aim to answer this question. However, cross-sectional data give reliable results, for example with multistate models [25, 47], but age reports are needed (age of onset of each drug).
Another limitation was that the profiles of drug users identified may be “typical,” being valid for most of the “occasional” or “experimental” drug users [48] (90%–95% of users) [49]. Indeed, the prevalence rates were quite low for illicit drugs other than cannabis. However, these profiles are not universal [7] and may differ among serious drug users who can have an “atypical” profile. For example, serious drug users are more likely to use other illicit drugs before cannabis [48], and alcohol is not a prerequisite for cannabis use among them [36]. This population needs a particular focus. It is also important to explore the effect of light and heavy use of a drug (experimentation, regular use, abuse), whereas this study focused on the progression between different drugs. Another shortcoming is that no women could be included. The study is largely representative of men, although it did not include the Italian-speaking canton (Ticino), nor the upper northern region of Switzerland (including Zurich). However, Italophones represent less than 5% of the Swiss population and are similar to Francophones in most patterns of use, so we do not expect our findings to be biased. Not including the Zurich area, which includes the largest city in Switzerland, may have led to the underestimation of some multisubstance use patterns and trajectories. However, the study included four of the five biggest cities in Switzerland and therefore, the omission of the Zurich area may have only marginally affected the findings of the study.
|
Table 6: Proportion of drug users within age categories for onset of intensive use of alcohol. |
|
|
First drunkenness
|
z-tests
|
|
Nonuser
n = 736
|
≥19
n = 135
|
16‒18
n = 2,508
|
13‒15
n = 2,256
|
≤12
n = 196
|
16–18/
13–15
|
13–15/
≤12
|
| Hallucinogens / magic mushrooms |
0.005 |
0.000 |
0.027 |
0.092 |
0.271 |
–3.590*** |
–6.179*** |
| Ecstasy |
0.004 |
0.007 |
0.023 |
0.098 |
0.256 |
–4.135*** |
–5.493*** |
| Cocaine |
0.004 |
0.015 |
0.023 |
0.091 |
0.271 |
–3.774*** |
–6.120*** |
|
Salvia divinorum
|
0.003 |
0.000 |
0.024 |
0.086 |
0.226 |
–3.379*** |
–4.840*** |
| Poppers |
0.005 |
0.022 |
0.031 |
0.084 |
0.141 |
–2.830** |
–2.237* |
| Solvent sniffing |
0.009 |
0.029 |
0.035 |
0.063 |
0.191 |
–1.541#
|
–4.643*** |
| Speed |
0.004 |
0.007 |
0.019 |
0.076 |
0.251 |
–3.165*** |
–5.701*** |
| Other hallucinogens |
0.005 |
0.007 |
0.018 |
0.068 |
0.191 |
–2.743** |
–4.116*** |
| Amphetamine/methamphetamine |
0.007 |
0.007 |
0.014 |
0.052 |
0.201 |
–2.134* |
–4.588*** |
| Spice |
0.004 |
0.007 |
0.009 |
0.016 |
0.095 |
–0.404 |
–2.243* |
| Ketamine |
0.004 |
0.007 |
0.006 |
0.015 |
0.101 |
–0.541 |
–2.292* |
| GHB/GBL |
0.001 |
0.007 |
0.006 |
0.016 |
0.065 |
–0.560 |
–1.461#
|
| Crystal meth |
0.003 |
0.007 |
0.006 |
0.013 |
0.095 |
–0.415 |
–2.119* |
| Research chemicals |
0.003 |
0.000 |
0.007 |
0.013 |
0.070 |
–0.341 |
–1.633* |
| Heroin |
0.003 |
0.000 |
0.006 |
0.013 |
0.070 |
–0.396 |
–1.582#
|
| Z-tests for difference in use proportions between the ages of 16–18 and 13–15, and between 13–15 and 12 or younger. Example of proportions: 0.091for cocaine means that 9.1% of respondents who started getting drunk at age 13–15 also used cocaine at least once in their lives.
*** p <0.001, ** p <0.01, * p <0.05, # p <0.10
GBH = gamma-hydroxybutyrate; GBL = gamma-hydroxylactone |
|
Table 7: Proportion of drug users within age categories for onset of intensive use of tobacco. |
|
|
First daily smoking
|
z-tests
|
|
Nonuser
n = 3,991
|
≥19
n = 166
|
16‒18
n = 1,165
|
13–15
n = 466
|
≤12
n = 43
|
16–18/
13–15
|
13–15/
≤12
|
| Hallucinogens / magic mushrooms |
0.017 |
0.121 |
0.117 |
0.189 |
0.386 |
–2.602** |
–5.772*** |
| Ecstasy |
0.014 |
0.081 |
0.118 |
0.233 |
0.364 |
–3.970*** |
–3.755*** |
| Cocaine |
0.013 |
0.069 |
0.112 |
0.231 |
0.386 |
–4.069*** |
–4.333*** |
|
Salvia divinorum
|
0.015 |
0.075 |
0.118 |
0.156 |
0.341 |
–1.362#
|
–5.394*** |
| Poppers |
0.030 |
0.069 |
0.088 |
0.121 |
0.273 |
–1.332#
|
–4.800*** |
| Solvent sniffing |
0.031 |
0.081 |
0.069 |
0.096 |
0.341 |
–1.165 |
–7.358*** |
| Speed |
0.011 |
0.064 |
0.092 |
0.200 |
0.318 |
–3.623*** |
–3.182*** |
| Other hallucinogens |
0.011 |
0.040 |
0.085 |
0.162 |
0.341 |
–2.603** |
–4.657*** |
| Amphetamine/methamphetamine |
0.009 |
0.029 |
0.063 |
0.148 |
0.295 |
–2.787** |
–3.588*** |
| Spice |
0.006 |
0.017 |
0.019 |
0.046 |
0.227 |
–0.978 |
-3.500*** |
| Ketamine |
0.004 |
0.023 |
0.018 |
0.046 |
0.250 |
–0.977 |
–3.673*** |
| GHB/GBL |
0.004 |
0.012 |
0.020 |
0.031 |
0.250 |
–0.407 |
–3.872*** |
| Crystal meth |
0.004 |
0.017 |
0.016 |
0.040 |
0.205 |
–0.838 |
–2.987** |
| Research chemicals |
0.005 |
0.023 |
0.019 |
0.029 |
0.136 |
–0.370 |
–2.243* |
| Heroin |
0.004 |
0.012 |
0.013 |
0.037 |
0.250 |
–0.844 |
–3.493*** |
| Z-tests for difference in use proportions between the ages of 16–18 and 13–15, and between 13–15 and 12 or younger. Example of proportions: 0.121 for poppers means that 12.1% of those respondents who started daily smoking at age 13–15 also used poppers at least once in their lives.
*** p <0.001, ** p <0.01, * p <0.05, # p <0.10
GBH = gamma-hydroxybutyrate; GBL = gamma-hydroxylactone |
Conclusions
This study provides insight into the profiles of drug users, particularly regarding less common illicit drugs. The profiles differentiated between licit drug use (alcohol and then tobacco), cannabis, and other illicit drugs such as hallucinogens, uppers and inhaled drugs, and finally opiates, crystal meth and spice. These profiles provide information not identified in previous studies, and suggest that there was an order in the use of other illicit drugs, in which “soft” drugs (uppers, hallucinogens and inhaled drugs) precede “hard” drugs (opiates, crystal meth and spice). However, becaus of the cross-sectional study design, these results are preliminary and the findings will be confirmed as future data are gathered. These profiles were also seen in the early age of onset of intensive use of cannabis, tobacco and alcohol: the risk of using “hard” drugs increased for those who began intensive use of alcohol at a very early age, and this was particularly true for cannabis. These results also showed the ages at which interventions may be initiated to prevent drug use. In particular, selective approaches should be used to prevent early onset use of cannabis, tobacco and alcohol.
References
1 Kandel DB. Stages in adolescent involvement in drug use. Science. 1975;190(4217):912–4.
2 Kandel DB, Yamaguchi K. Stages of involvement in the U.S. population. Stages and pathways of drug involvement: Examining the gateway hypothesis. New York: Cambridge University Press; 2002. p. 65–89.
3 Kandel DB, Yamaguchi K, Klein LC. Testing the Gateway Hypothesis. Addiction. 2006;101(4):470–2; discussion 4–6.
4 Scholey AB, Parrott AB, Buchanan T, Heffernan TM, Ling J, Rodgers J. Increased intensity of Ecstasy and polydrug usage in the more experienced recreational Ecstasy/MDMA users: a WWW study. Addictive Behaviors. 2004;(29):743–52.
5 Hamburg BA, Kraemer HC, Jahnke W. A hierarchy of drug use in adolescence: Behavioral and attitudinal correlates of substantial drug use. The American Journal of Psychiatry. 1975;132(11):1155–63.
6 Fergusson DM, Boden JM, Horwood LJ. Cannabis use and other illicit drug use: testing the cannabis gateway hypothesis. Addiction. 2006;101(4):556–69.
7 Kandel DB. Examining the gateway hypothesis stages and pathways of drug involvement. Stages and pathways of drug involvement: Examining the gateway hypothesis. New York: Cambridge University press; 2002. p. 3–15.
8 Wu L-T, Schlenger WE, Galvin DM. Concurrent use of methamphetamine, MDMA, LSD, ketamine, GHB, and flunitrazepam among American youths. Drug Alcohol Depend. 2006;84(1):102–13.
9 Pape H, Rossow I, Storvoll EE. Under double influence: Assessment of simultaneous alcohol and cannabis use in general youth populations. Drug Alcohol Depend. 2009;101(1–2):69–73.
10 Pentz MA, Li C. The gateway theory applied to prevention. Stages and Pathways of Drug Involvement: Examining the Gateway Hypothesis. New York: Cambridge University Press; 2002. p. 139–57.
11 Wagner FA, Anthony JC. Into the world of illegal drug use: Exposure opportunity and other mechanisms linking the use of alcohol, tobacco, marijuana, and cocaine. Am J Epidemiol. 2002;155(10):918–25.
12 Willner P. A view through the gateway: expectancies as a possible pathway from alcohol to cannabis. Addiction. 2001;96(5):691–703.
13 Kokkevi A, Richardson C, Florescu S, Kuzman M, Stergar E. Psychosocial correlates of substance use in adolescence: A cross-national study in six European countries. Drug Alcohol Depend. 2007;86(1):67–74.
14 Goldstein JW, Gleason TC, Korn JH. Whither the Epidemic? Psychoactive Drug-Use Career Patterns of College Students1. Journal of Applied Social Psychology. 1975;5(1):16–33.
15 Kaplan HB, Martin SS, Robbins C. Pathways to Adolescent Drug Use: Self-Derogation, Peer Influence, Weakening of Social Controls, and Early Substance Use. Journal of Health and Social Behavior. 1984;25(3):270–89.
16 Valenzuela E, Fernández M. The sequence of drug use: Testing the Gateway Hypothesis in Latin America. The Journal of International Drug, Alcohol and Tobacco Research. 2011;1(1):1–8.
17 Kandel DB, Yamaguchi K, Klein LC. Testing the Gateway Hypothesis. Addiction. 2006;101(4):470–2.
18 Gross SR, Barrett SP, Shestowsky JS, Pihl RO. Ecstasy and drug consumption patterns: a Canadian rave population study. Canadian Journal of Psychiatry. 2002;47(6):546–51.
19 Hays RD, Stacy AW, Widaman KF, Di Matteo MR, Downy R. Multistage path models of adolscent alcohol and drug use: A reanalysis. The Journal of Drug Issues. 1986;16:357–69.
20 Windle M, Barnes GM, Welte J. Causal models of adolescent substance use: An examination of gender differences using distribution-free estimators. Journal of Personality and Social Psychology. 1989;56(1):132–42.
21 Agrawal A, Neale MC, Prescott CA, Kendler KS. Cannabis and Other Illicit Drugs: Comorbid Use and Abuse/Dependence in Males and Females. Behavior Genetics. 2004;34(3):217–28.
22 Kuntsche E, Rossow I, Simons-Morton B, Bogt TT, Kokkevi A, Godeau E. Not Early Drinking but Early Drunkenness Is a Risk Factor for Problem Behaviors Among Adolescents from 38 European and North American Countries. Alcoholism: Clinical and Experimental Research. 2013;37(2):308–14.
23 Lynskey M, Vink J, Boomsma D. Early Onset Cannabis Use and Progression to other Drug Use in a Sample of Dutch Twins. Behavior Genetics. 2006;36(2):195–200.
24 Hall W, Lynskey M. Is cannabis a gateway drug? Testing hypotheses about the relationship between cannabis use and the use of other illicit drugs. Drug and Alcohol Review. 2005;24(1):39–48.
25 Mayet A, Legleye S, Falissard B, Chau N. Cannabis use stages as predictors of subsequent initiation with other illicit drugs among French adolescents: use of a multi-state model. Addict Behav. 2012;37(2):160–6.
26 Guxens M, Nebot M, Ariza C. Age and sex differences in factors associated with the onset of cannabis use: a cohort study. Drug Alcohol Depend. 2007;88(2-3):234–43.
27 Korhonen T, van Leeuwen AP, Reijneveld SA, Ormel J, Verhulst FC, Huizink AC. Externalizing behavior problems and cigarette smoking as predictors of cannabis use: the TRAILS Study. J Am Acad Child Adolesc Psychiatry. 2010;49(1):61–9.
28 Guxens M, Nebot M, Ariza C, Ochoa D. Factors associated with the onset of cannabis use: a systematic review of cohort studies. Gac Sanit. 2007;21(3):252–60.
29 Studer J, Baggio S, Mohler-Kuo M, Dermota P, Gaume J, Bertholet N, et al. Examining non-response bias in substance use research – Are late respondents proxies for non-respondents? Drug Alcohol Depend. Forthcoming 2013.
30 Wright D, Sathe N. State estimates of substance use from the 2002-2003 National Surveys on Drug Use and Health. Rockville, MD: SAMHSA, Offoce of Applied Studies; 2005.
31 Fergusson Dm HL. Early reactions to cannabis predict later dependence. Arch Gen Psychiatry. 2003;60(10):1033–9.
32 Meier MH, Caspi A, Ambler A, Harrington H, Houts R, Keefe RSE, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. PNAS. Forthcoming 2013.
33 Neal DJ, Corbin WR, Fromme K. Measurement of alcohol-related consequences among high school and college students: application of item response models to the Rutgers Alcohol Problem Index. Psychol Assess. 2006;18(4):402–14.
34 Birnbaum A. Some latent trait models. Statistical theories of mental test scores. Reading, MA: Addison-Wesley Publishing company; 1968.
35 Lord FM, Novick MR. Statistical Theories of Mental Test Scores. Reading, MA: Addison-Wesley Publishing Company, ; 1968.
36 Golub A, Johnson BD. The Shifting Importance of Alcohol and Marijuana as Gateway Substances among Serious Drug Abusers. Journal of Studies on Alcohol and Drugs. 1994;55(5):607-14.
37 Clinard MB, Meier RF. Sociology of Deviant Behavior. Fort worth, TX: Harcourt College Publishers; 2001.
38 Kim S-H, Shanahan J. Stigmatizing smokers: public sentiment toward cigarette smoking and its relationship to smoking behaviors. J Health Commun. 2003;8(4):343–67.
39 Grønkjaer M, Curtis T, Crespigny CD, Delmar C. Acceptance and expectance: Cultural norms for alcohol use in Denmark. Int J Qual Stud Health Well-being. 2011;6(4). doi: 10.3402/qhw.v6i4.8461. Epub 2011 Nov 3.
40 NHMRC. Australian guidelines to reduce health risks from drinking alcohol. Canberra: NHMRC; 2009.
41 Dryfoos JG. Adolescents ar risk. New York, BY, USA: Oxford University Press; 1990.
42 Donovan JE, Jessor R. Structure of problem behavior in adolescence and young adulthood. J Consult Clin Psychol. 1985;53(6):890–904.
43 EMCDDA. The state of the drugs problem in Europe. Lisbon: European Monitoring Center for Drugs and Drug Addiction; 2011.
44 Choo T, Roh S, Robinson M. Assessing the “Gateway Hypothesis” among Middle and High School Students in Tennessee. Journal of Drug Issues. 2008;38(2):467–92.
45 Leshner AI. Foreword. Stages and pathways of drug involvement: Examining the gateway hypothesis. New York: Cambridge University Press; 2002. p. xiii-xiv.
46 Hawkins JD, Hill KG, Guo J, Battin-Pearson SR. Substance use norms and transitions in substance use. Stages and pathways of drug involvement: Examining the gateway hypothesis. New York: Cambridge University Press; 2002. p. 42–64.
47 Mayet A, Legleye S, Chau N, Falissard B. Transitions between tobacco and cannabis use among adolescents: a multi-state modeling of progression from onset to daily use. Addict Behav. 2011;36(11):1101–5.
48 Mackesy-Amiti ME, Fendrich M, Goldstein PJ. Sequence of drug use among serious drug users: typical vs atypical progression. Drug Alcohol Depend. 1997;45(3):185–96.
49 Labouvie E, White. Drug sequences, age of onset, and use trajectories as predictors of drug abuse/dependence in young adulthood. Stages and Pathways of Drug Involvement: Examining the Gateway Hypothesis. New York: Cambridge University Press; 2002. p. 19–41.