Figure 1
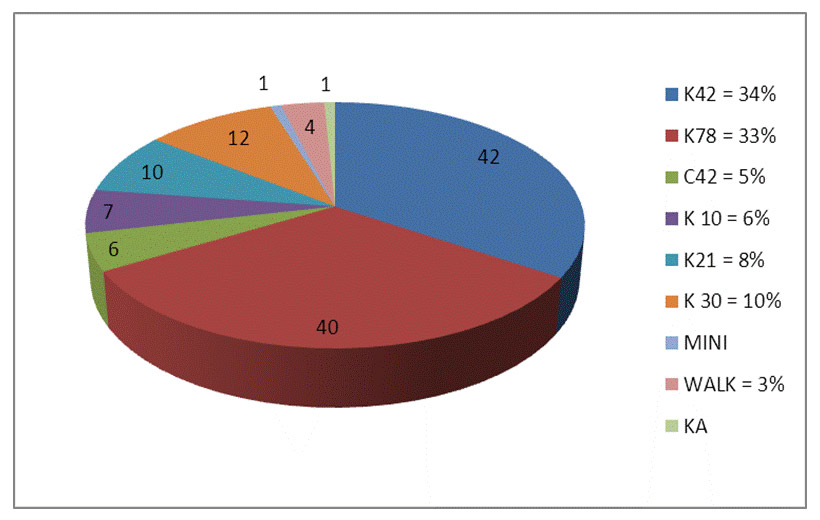
Distribution of the different categories within the group of athletes that completed the questionnaire.
DOI: https://doi.org/10.4414/smw.2013.13785
STUDY/PRINCIPLES: To assess the effects of an “on-site” prevention and education programme to improve the cardiac screening in competitive amateur athletes.
METHODS: We integrated an “on-site prevention and education programme” at the 2012 edition of the Swiss Alpine Marathon in Davos, Switzerland. After a specific lecture, the athletes could visit a “Sports-Cardiology-Section” at the official “medical-park”. On an anonymised questionnaire, they could state their intention for a screening programme in general and after our “on-site” intervention.
RESULTS: Among the 150 athletes who attended the medical day (3.3% of 4,500 finishers) the response rate was 82%. While 39 (31.7%) athletes were aware of “exercise related SCD”, more than twice as many (64.2%) were not. 72.4% of the participants (n = 89) reported that they never had taken part in cardiac screening examinations. 70.7% (n = 87) runners were convinced that they would benefit from such a screening. 65.9% (n = 81) of the runners stated that our “on-site” prevention concept influenced their decision to consider a cardiac screening in the future.
CONCLUSION: An “on-site prevention and education” concept for the prevention of SCD in competitive amateur athletes is feasible and successfully increased the athletes’ awareness of the issue. The vast majority of athletes felt to have benefited from such a programme. The current study confirms that there is an alarming lack of preventive measures in the very large group of ambitious, competitive, amateur athletes that are frequently underprepared for challenging sports events.
The real incidence of fatal cardiac events in athletes remains controversial and is highly dependent on data acquisition, the sort of sport and the individual characteristics of the athletes within a given study. While a yearly incidence of about 1–3 sudden cardiac deaths (SCD) per 100,000 young athletes (age <35 years) is an established estimate in literature [1–5], newer data demonstrates a wider range; while a recent large survey of North-American marathon runners showed an unexpectedly low rate of SCD [6], data from North-American college athletes suggested that the incidence depends highly on the kind of sports and the race of said athletes [7]. As such, the risk of SCD for a black Division I basketball player may be as high as 1:3,000 [7].
It is important to consider that SCD in sports is by far not only an issue in young top-level athletes. Amateur, but nevertheless, competitive athletes should be within the same focus of Sports Cardiology. Indeed, with increasing age, the risk for sports-related SCD accelerates steadily [8–11]. Marjion et al. examined the incidence of sports-related deaths in the general population and reported striking findings: while only 6% of fatal events occurred in young competitive athletes, more than 90% concerned athletes performing “recreational sports” with an average age of 46 years (± 15 years) [10]. Therefore, it should be highlighted that SCD in sports has become an issue of public health and not specifically of young, professional athletes.
Importantly, an adequate cardiac screening is able to prevent the majority of cardiac events in athletes [12–18]. Mainly Italian data has shown a decrease of these events by almost 90% in young competitive athletes after implementing a simple screening programme consisting of a questionnaire, a physical examination focused on cardiovascular items as well as a 12-lead resting ECG [13, 14]. The detection of coronary artery disease (CAD), which is the underlying substrate of SCD in the vast majority of athletes aged over 30 to 35 years is obviously not that accurate and alternative strategies for risk estimation and stratification need to be integrated [8].
Although the Swiss Society of Sports Medicine (SGSM) published their recommendations for the prevention of SCD in sports in 1998, these guidelines particularly targeted top-level athletes [19, 20]. Still the vast majority of competitive athletes in Switzerland are currently not covered by a standardised cardiac screening. A recent large survey of competitive Swiss athletes that were not integrated in an Olympic or other top-level squad showed that only 9% underwent a regular cardiac screening, despite their risk of exercise-related SCD [21]. However, only 47% of the assessed athletes were interested in a cardiac screening. Younger age, female gender and a lower extent of weekly training efforts were negative predictors for the acceptance of such a screening [21]. Although this relatively low acceptance rate may express a certain fatalistic attitude of individual athletes, it is of note that the reason why a relevant part of the subgroup that did not accept regular cardiac screening might be due to a lack of awareness and knowledge of the issue. As such, we concluded that comprehensive education is a crucial point to provide a tailored and ultimately voluntary screening.
The aim of the current study was to assess the effects of an “on-site” prevention and education programme to improve the individual knowledge and awareness regarding sports-related SCD.
We introduced and provided the concept of an “on-site” prevention and education programme at one of the most popular running events in Switzerland and Europe – the “Swiss Alpine Marathon”. Established in 1986, the race currently attracts more than 4,500 runners from all over the world, participating in various categories (table 1).
The main races are scheduled on a Saturday at the end of July. Throughout the days before the race the athletes can participate in various events concerning technical running skills, track inspections, etc. One day (usually Friday, the day before the race) is traditionally dedicated to Sports Medicine. On that day, various lectures are given, and the athletes have the possibility to visit a “medical park” that provides basic health checks, like blood pressure and heart rate measurements, estimation of plasma glucose, body composition and ventilatory function. For the purpose of our study, we integrated our “on-site prevention and education programme” in the 2012 edition of the “medical day”. A lecture with the focus on the prevention of SCD in sports was held. After the lecture (30 minutes), the athletes had the possibility to visit a “Sports Cardiology Section” at the official “medical park”. On two movable walls the theoretical background of SCD in sports was highlighted and paper handouts of some crucial studies were available. Furthermore, two experienced physicians in the field were “on-site” to provide additional information.
Every visitor to the lecture and the “medical park” received a specific anonymised questionnaire (see attachment), on which the athletes could state their intention towards a screening programme in general and “on-site”, and if they ever went through a cardiac screening before. Participation was voluntary.
Statistical analysis was performed using standard statistical software (SPSS version 16.0, Inc, Chicago, IL). Data are given as median (range) unless stated otherwise.
Approximately 4,500 runners finished the 2012 edition of the “Swiss Alpine Marathon”. The medical lectures and the sections at the “medical park” were attended by 150 athletes. Of these, 123 athletes returned the questionnaire (response rate 82%). The athletes originated from different countries (i.e. Switzerland: 49, Germany: 52, Belgium: 2, Italy: 1, Denmark: 1, Turkey: 1, not specified: 17) and their average age was 48 years (range: 11–83 years, SD = 15.89). The gender ratio was nearly balanced (56% male, 44% female). However, of the athletes that completed the questionnaire, twice as many men as women had competed in the long distance tracks. Overall, the majority of athletes (72%) registered for a long distance track, either regular marathon “C42” (5%), the mountain marathon “K42” (34%) or mountain ultra-marathon “K78” (33%). Only very few athletes participated in the “WALK” category (n = 4) and these athletes might have had an approach of “leisure activity” rather than “competitive sports”. As such, they should probably be addressed less aggressively regarding the prevention of exercise-related SCD. See table 1 and figure 1 for detailed track information.
Figure 1
Distribution of the different categories within the group of athletes that completed the questionnaire.
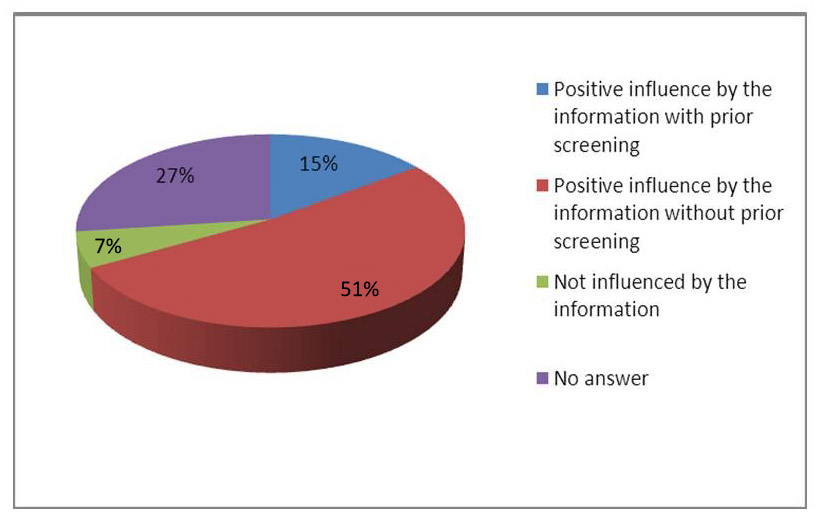
Figure 2
Impact of the “on-site prevention and education” concept regarding the incentive towards a regular cardiac screening”.
Most of the athletes proved to be quite experienced in performing regular endurance sports. The vast majority had trained for more than 24 months (n = 121, overall 98.4%); one (0.8%) athlete had trained regularly for less than 24 months and another athlete (0.8%) for less than 6 months.
The average weekly training effort was 2 to 7 hours in the majority of athletes (n = 78; 63.4%), and 7 to 12 hours in 32 (26.0%) runners. Only a few athletes trained more than 12 hours per week (n = 5; 4.1%), while 6 (4.9%) athletes performed sports less than 2 hours per week prior to the race. These 6 athletes nevertheless competed in the K78 (n = 1), K24 (n = 2), C24 (n= 1), K21 (n = 1) and WALK category (n = 1). Most athletes (111 of 123 or 90.2%) had taken part in a long–distance running event equal to the Swiss Alpine Marathon previously, while 12 (9.8%) participated for the first time in such an event.
While 39 (31.7%) athletes were aware of the problem of “exercise related SCD”, more than twice as many (64.2%) were not. Five athletes did not answer this particular question.
A majority of participants reported that they had never taken part in cardiac screening examinations (n = 89, 72.4%), while 32 (26.0%) athletes had done so in the past. While Swiss athletes had rarely undergone such a medical check-up (17%), German athletes, the largest subgroup of athletes that attended the “medical day”, the screening participation rate was 35%. All athletes who had already participated in a screening programme competed in long distance tracks (marathon or ultra-marathon distance).
Eighty-seven (70.7%) runners were convinced that they would benefit from a cardiac screening, while only 10 thought that they would not (8.1% overall; 11.2% of the athletes had not previously undergone a medical screening). However, it has to be noted that 21% (n = 26) did not answer this particular question.
While 18 (14.6%) athletes were not willing to spend more than 50 Swiss Francs (CHF) for a baseline screening, 57 (46.3%) felt that a cost of 50 to 100 CHF would be acceptable while 28 (22.8%) were even willing to pay more than 100 CHF. However, these results have to be interpreted by taking account of the internationality of the participants as the amounts in the questionnaire were listed in CHF.
The majority of the participating athletes (n = 79, 64.3%) felt that the physician performing cardiac screening should be no more than 10 to 50 kilometres away from their home. Twenty-one runners (17.1%) accepted a distance even greater than that (>50 kilometres) and 13 athletes (10.6%) said that they would not travel more than 10 kilometres to undergo a cardiac screening.
The vast majority of runners stated that our “on-site” prevention concept influenced their decision (n = 81, 65.9%) to consider a cardiac screening in the future (fig. 2). Of these athletes, 31 were already aware of SCD occurring during sports activities, while 50 (40.7% overall) heard of the issue for the very first time. Of the 31 athletes that were already aware of the issue, 16 (13.0% overall) nevertheless had never undergone a cardiac screening, but were convinced to do so in the future after having attended the prevention campaign prior to this race. Only a small minority of the participating athletes (6.5%; n = 8) felt that they had not been influenced positively by the information given to them during the “medical day”, while 27% (n = 33) didn’t answer that particular question. Participation in a longer distance race at the “Swiss Alpine Marathon” correlated with a positive acceptance towards a screening programme (ultra-marathon/marathon distance: 47% versus 20%).
| Table 1: Race categories of the “Swiss Alpine Marathon”, 2012 edition. | ||
| Category | Distance and Vertical Height | Characteristics |
| K78 | 79.4 km, ± 2600 m | Biggest mountain marathon worldwide |
| K42 | 42.2 km, + 1720 / –1550 m | Highest-located Marathon in Europe |
| C42 | 42.2 km, +500 / –1150 m | Regular marathon in alpine surroundings |
| K30 | 30.2 km, +380 / –900 m | Mountain half-marathon |
| K21 | 22.9 km, +750/ –260 m | |
| K10 | 10.9 km, +160 m/ –130 m | Beginners track |
| WALK | 10.9 km, +160/ –130 m | Nordic-Walking event |
| MINI | 0.5 km, +0.9 km/ –1.4 km | Fun event for kids |
Although Swiss sports associations as well as the network of the Swiss Olympic Society provide an excellent medical supply for top-level athletes including cardiac screening, there is still a significant lack of adequate prevention strategies for amateur and “non-top‒level” athletes. A recent survey found that only 9% of a large sample of such athletes formerly underwent such a medical screening [21]. This alarming situation requires new strategies for the optimisation of SCD prevention in competitive athletes in Switzerland. The “on-site prevention and education” concept, implemented at one of the biggest running events in Europe proved to be feasible and successful in increasing the awareness of SCD in sports. Although it was a pilot project, the concept perfectly complemented the well-established structures of the event and earned positive feedback from the athletes and the organising committee.
Beside the very low rate of screened athletes, one of our major findings of the former survey [21] was the fact that only about half (47%) of the athletes expressed their interest in such a cardiac screening programme [21]. Although data on the motivation are missing, it can be speculated that the negative attitude towards cardiac screening reflects a fatalistic mind-set of athletes. This attitude should be respected and a mandatory screening, as it is enforced by law in Italy, would not seem to be compatible with the culture in Switzerland. On the other hand, we hypothesised that there has to be a relevant subgroup of athletes that do not have adequate knowledge regarding SCD in sports and the possibilities of its prevention. Thus, when applying an on-site prevention campaign prior to a sports event, two target groups can be reached: athletes that are basically not aware of the problem of sports-related SCD and those who are aware of the issue, but are not yet convinced that it would be worthwhile to undergo such a screening. In addition, a third group of individuals should be mentioned that already underwent a screening, but should be motivated to continue regular follow-ups. As our study impressively demonstrated, these target groups can be reached perfectly by an “on-site” concept. Firstly, and most importantly, there was a large subgroup of runners that had not been aware of the problem of sports-associated SCD (41%) thus far. This is surprising in a sample of athletes competing at an ambitious running event such as the “Swiss Alpine Marathon”. Only one athlete out of this large group stated that the prevention programme did not influence his personal motivation towards a screening in the future – all others felt that their motivation to get screened regularly in the future had increased because of the event. All athletes of the subgroup, being aware of the issue, but not yet being screened, could be motivated by our information to do so in the future.
Of note, there was only a small minority of athletes (n = 8, 6.5%) that stated, that they had not benefited from the campaign. However, recognising that five of them already had undergone a regular screening previously (and thus could not have further benefited from the campaign) there were only three athletes that definitely felt that they will continue to refrain from a cardiac screening programme.
It can therefore be assumed, taking a number of abstentions into account, that at least two thirds of the athletes did benefit from the on-site screening and education concept while only 1 out of 15 runners did not take advantage of the intervention. However, our initiative overall reached only a relatively small number of athletes. This number was limited to the 150 out of 4,500 race finishers (3.3%) that attended the traditional “medical day”. This amount of athletes has been quite stable during the last years. However, to increase the number of participants the athletes should be better informed prior to a race. Particularly the issue of prevention of SCD in sports should be addressed on official application forms, on the homepage and in public media. Focussed mailings to all registered participants of the race could additionally inform about the prevention campaign and events during the official “medical day”. In the current setting of the study, we deliberately abstained from providing a questionnaire to all registered athletes by e-mail or by postal service because we think that the lecture with focus on the prevention of SCD and the possibility to discuss the issue with experts “on-site” is a crucial characteristic of our approach.
However, despite the relatively low attendance, the current results were confirmed by our former survey among Swiss athletes in many parts [21]. The relatively high average age of the athletes reflected the generally known high percentage of athletes older than 35 to 40 years participating in endurance sports and particularly long-distance events [6, 22]. An advanced age has already been identified as a positive predictor for the acceptance of a cardiac screening and health awareness by athletes in general [21]. In line with our previous survey, we could confirm that in addition to an increased age, male gender as well as higher training efforts, physical capacity and high athletic aims positively predicted the acceptance of a cardiac screening programme [21].
Particularly in the context of such an ambitious mountain running event and considering the fact that the majority of the participants appreciated the value of a screening, the number of athletes that already had undergone a cardiac screening (about a quarter) is still low, although higher than previously reported. Indeed, the low percentage (17%) of previously screened Swiss athletes is closer to the formerly reported range in Switzerland and compares unfavourably with the screening rate of German athletes (35%). This difference regarding screening rates is remarkable. While a medical check-up of competitive amateur athletes is mandatory particularly in Italy or Luxembourg, many other European countries, such as Germany or Switzerland, mandate a screening only for professional and/or elite athletes [14, 17, 19].
According to the questionnaire, most of the participants seemed to be quite experienced endurance athletes. Indeed, more than 90% had competed in a mountain race previously. Nevertheless, an average weekly training effort of 2 to 7 hours performed by the majority of athletes seems barely sufficient, particularly prior to efforts such as a 78 kilometre mountain race with more than 1,600 meters vertical height. Six athletes trained less than 2 hours per week prior to the race, which definitely appears to be inadequate.
In summary, an “on-site prevention and education” concept to increase the incentive towards a regular cardiac screening proved to be feasible and, as our findings demonstrate, also successful to increase the athletes` awareness of the issue. Although probably only a minority of participants attended the medical framework programme, we suggest regularly establishing such programmes at similar events (e.g. running-, cross-country-skiing-events, among others). As the “on-site” information and discussion of the issue is a crucial factor of our approach future research and studies should aim to reach increase the number of included athletes and to provide follow-up and outcome data to finally assess the prognostic impact of this strategy.
Of course, for those athletes that express their willingness to undergo a screening it is crucial to get an easy “first port of call”. As such, the professional network of Swiss Olympic or other skilled physicians and cardiologists can provide adequate information and education “on-site” and serve as a first contact for screening programmes. As previously reported, the majority of the athletes would be willing to pay between 50 to 100 Swiss Francs to cover the cost of a SCD screening and found a distance of 10 to 50 kilometres to reach an assessing physician acceptable.
The fact that the questionnaire was only delivered to athletes that attended the “medical day” reflects a selection bias, as these athletes are supposed to have a particular “health awareness”. However, one major aim of the study was to test a lifelike approach of an “on site” prevention and education concept.
An “on-site prevention and education” concept for the prevention of SCD in competitive amateur athletes is feasible and successful to increase the athletes’ awareness of the issue. The vast majority of athletes felt to benefit from such an intervention. The current study confirms that there is an alarming lack of preventive measures in the very large group of ambitious, competitive amateur athletes. Although exposed to a particularly increased risk for cardiac events during sports, this subgroup is currently not covered by the official screening recommendations of the SGSM and frequently underprepared for challenging sports events.
1 Corrado D, Basso C, Thiene G. Assay Sudden death in young athletes. Lancet. 2005;47–8.
2 Maron BJ. Sudden death in young athletes. N Engl J Med. 2003;349:1064–75.
3 Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980–2006. Circulation. 2009;119:1085–92.
4 Siscovick DS, Weiss NS, Fletcher RH, Lasky T. The incidence of primary cardiac arrest during vigorous exercise. N Engl J Med. 1984;311:874–7.
5 Scoville SL, Campbell CL, Shry EA, Stajduhar KC, Potter RN, Pearse LA, et al. Sudden death in young adults: a 25-year review of autopsies in military recruits. Ann Intern Med. 2004;141(11):829–34.
6 Kim JH, Malhotra R, Chiampas G, d’Hemecourt P, Troyanos C, Cianca J, et al. Race Associated Cardiac Arrest Event Registry (RACER) Study Group. Cardiac arrest during long-distance running races. N Engl J Med. 2012;366(2):130–40.
7 Harmon KG, Asif IM, Klossner D, Drezner JA. Incidence of sudden cardiac death in national collegiate athletic association athletes. Circulation. 2011;123(15):1594–600. Epub 2011 Apr 4.
8 Corrado D, Schmied C, Basso C, Borjesson M, Schiavon M, Pelliccia A, et al. Risk of sports: do we need a pre-participation screening for competitive and leisure athletes? Eur Heart J. 2011;32(8):934–44.
9 Thompson PD, Funk EJ, Carleton RA, Sturner WQ. Incidence of death during jogging in Rhode Island from 1975 through 1980. JAMA. 1982;247:2535–8.
10 Marijon E, Tafflet M, Celermajer DS, Dumas F, Perier MC, Mustafic H, et al. Sports-related sudden death in the general population. Circulation. 2011;124(6):672–81. Epub 2011 Jul 25.
11 Borjesson M, Urhausen A, Kouidi E, Dugmore D, Sharma S, Halle M, et al. Cardiovascular evaluation of middle-aged/senior individuals engaged in leisure-time sport activities: position stand from the sections of exercise physiology and sports cardiology of the European Association of Cardiovascular Prevention and Rehabilitation. Eur J Cardiovasc Prev Rehabil. 2010 Jun 19.
12 Corrado D, Pelliccia A, Bjornstad HH, Vanhees L, Biffi A, Borjesson M, et al. Cardiovascular pre-participation screening of young competitive athletes for prevention of sudden death: proposal for a common European protocol. Consensus Statement of the Study Group of Sport Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J. 2005;26:516–24.
13 Dvorak J, Grimm K, Schmied C, Junge A. Development and implementation of a standardized precompetition medical assessment of international elite football players. Clin J Sport Med. 2009;19(4):316–21.
14 Corrado D, Basso C, Pavei A, Michieli P, Schiavon M, Thiene G. Trends in sudden cardiovascular death in young competitive athletes after implementation of a preparticipation screening program. JAMA. 2006;296:1593–601.
15 Pelliccia A, Di Paolo FM, Corrado D, Buccolieri C, Quattrini FM, Pisicchio C, et al. Evidence for efficacy of the Italian national pre-participation screening programme for identification of hypertrophic cardiomyopathy in competitive athletes. Eur Heart J. 2006;27:2196–200.
16 Keller, DI, Kardiale Screening-Untersuchungen beim Kompetitiv- und Gelegenheits-Athleten. Schweizerische Zeitschrift für Sportmedizin und Sporttraumatologie. 2011;59:79–82.
17 Corrado D, Basso C, Schiavon M, Pelliccia A, Thiene G. Pre-participation screening of young competitive athletes for prevention of sudden cardiac death. J Am Coll Cardiol. 2008;52:1981–9.
18 Bille K, Fiquiras D, Schamasch P. Sudden cardiac death in athletes: the Lausanne recommendations. Eur J Cardiovasc Prev Rehabil. 2006;13:859–75.
19 Villiger B, Hintermann M, Goerre S, Kriemler S, Schmied C. Task Force “Prevention of Sudden Death in Elite Sport” SGSM/SSMS 2010;The sudden cardiac death of a young athlete: Recommendations for a sensible and effective preventive exam. Schweizerische Zeitschrift für «Sportmedizin und Sporttraumatologie» (2)/2011;59:108–9.
20 Michaud K, Fellmann F, Abriel H, Beckmann JS, Mangin P, Elger BS. Molecular autopsy in sudden cardiac death and its implication for families:discussion of the practical, legal and ethical aspects of the multidisciplinary collaboration. Swiss Med Wkly. 2009;139(49-50):712–8.
21 Schmied C, Notz S, Cribari M, Gähwiler R, Keller DI, Lüscher TF. Cardiac pre-competiton screening in Swiss athletes. Current situation in competitive athletes and short-time assessment of an exemplary local screening program. Swiss Med Wkly. 2012;142:w13575
22 Haeusler KG, Herm J, Kunze C, Krüll M, Brechtel L, Lock J, et al. Rate of cardiac arrhythmias and silent brain lesions in experienced marathon runners: rationale, design and baseline data of the Berlin Beat of Running study. BMC Cardiovasc Disord. 2012;12:69.
Funding / potential competing interests: No financial support and no other potential conflict of interest relevant to this article was reported.