Sport climbing from a medical point of view
DOI: https://doi.org/10.4414/smw.2012.13688
Summary
Rock climbing, sport climbing and bouldering are highly popular new sport disciplines. An increasing number of indoor climbing gyms throughout the country offer the possibility to perform the sport regularly independently from the weather. As a result a variety of new pathologies like the closed flexor tendon pulley rupture of the finger and syndromes caused by overuse mainly in the upper extremity have appeared and should be familiar to physicians and therapists working in the field of sports medicine. An overview of the most common and most specific climbing related injuries as well as their diagnosis and treatment options with a focus on the upper extremity are presented.
Introduction
During the last 25 years rock-climbing, sport climbing and particularly bouldering (climbing at low heights but still up to several meters) has become increasingly popular. Initially rock and sport climbing were used by ambitious alpinists to train and prepare for longer alpine routes or expeditions. In the meantime it has become an independent discipline with its own world-cup. In Switzerland the first climbing gyms opened in the late eighties and their numbers increased to 53 in 2011. Parallel to the fact that climbing is nowadays a popular sport, the level of climbing performances has increased continuously from the seventies onwards. In 1983 Jerry Moffat climbed “The Face” which was the first route rated grade 10 in the UIAA (Union Internationale des Associations d'Alpinisme) scale until Wolfgang Güllich pushed the limits again with “Action Direct”, at that time (1991) the first route rated UIAA grade 11. Chris Sharma finally hit the 12th grade with “Jumbolove” in 2008.
Following this increase in performance new climbing-specific injuries such as closed flexor tendon pulley disruption [1, 2] or lumbrical muscle strain [3] where described. Many injuries in climbers are rather due to overload than acute trauma particularly concerning the shoulder. Since the introduction of bolted routes (safe protection points with bolts every 2–3 meters) and the development of dedicated ropes allowing for dynamic and soft deceleration of falls, heavy injuries due to ground-drops became very rare. Nevertheless alpine climbing and classic alpinism remain a dangerous sport due to objective dangers like rock fall, sudden weather changes and poor protection in case of a fall. In contrast sport climbing and bouldering usually performed on solid rock at low height (sport climbing routes usually have a length of 20–30 meters) is not as dangerous a sport as perceived in public opinion. The injury rates per 1,000 hours of sport are quite low compared with other popular sports. Schöffl [4] rated it at 0.079 per 1,000 hours for indoor-climbing, Neuhof [5] at 0.2 injuries per 1,000 hours of sport climbing, Schussman [6] at 0.6 injuries per 1,000 hours of mountaineering and Backe [7] at 4.2 injuries per 1,000 hours of rock-climbing of all sub-disciplines. These injury rates are lower compared to those of motor-cycling with 13.5 per 1,000 hours of sport [8], playing football with 31 per 1,000 hours [9], handball with 50 injuries per 1,000 hours [10] or even ice-hockey with 83 injuries per 1,000 hours [11] or rugby with 286 injuries per 1,000 hours of sport [12].
The injury patterns and locations changed considerably during the development of the sport. In classical mountaineering injuries are mostly due to falls and rock-falls with only limited or low-quality protection, the injuries being fractures and sprains of the lower extremity or the head and trunk [6]. In contrast a fall in sport climbing is very common and inevitable when an athlete tries to complete a route at the limit of his performance. Because difficult routes often take place on steep or overhanging rock formations with small holds, this has led to a completely different injury pattern. Schöffl [13] mentioned that 67% of 604 injuries concerned the upper extremity and shoulder whereas poly-traumas or fatal events accounted for less than 1%. Bouldering injuries have shifted even more to the upper extremity [14] where more than 80% of the injuries are of the upper extremity. Of these, the finger and the shoulders were the most frequently affected. In comparison, in traditional climbing, where the protection is not as good and the sport is usually performed with removable protection such as nuts or cam-devices, injuries are more likely to affect the lower extremity caused by falls [15]. Comparing outdoor with indoor climbing it has been shown that the risk of injury in the former is a little bit higher, particularly for injuries to the knee, ankle and foot caused by down-jumps while bouldering.
This article gives an overview of the most specific but also the most common injuries related to sport climbing and bouldering with emphasis on those of the hand. Guidelines for the different treatment options are also given according to the current literature. Controversial issues are discussed and current different points of view are highlighted.
Flexor tendon pulley injuries of the fingers
Among all problems of the fingers and the hand in climbers those concerning the flexor tendon sheath are the most common. The so-called crimp-grip-position (fig. 1), which is commonly used in climbers up to 90% of the time, [1, 16] is a very specific position of the finger where the proximal interphalangeal (PIP) joint is flexed more than 90° and the distal interphalangeal (DIP) joint is hyper-extended (fig. 2) resulting in very high loads to the pulleys of the flexor tendon sheath, which are three to four times higher than the force acting at the fingertip [17, 18]. The existence of friction between the flexor tendons and the pulleys [3, 19] has added to the understanding of pathological mechanism of pulley disruption. If a sudden load to the finger occurs as a consequence of a foot slipping or, if the climber grasps a hold very quickly during a dynamic move one or more pulleys may disrupt (fig. 2). In this case the climber himself or even the belayer may hear a loud snapping sound. Usually only one finger flexor tendon pulley disrupts, the A2-pulley being one-and-a-half to two times more likely to be involved than the A4-pulley of either the ring or the middle finger. This injury was first described by Bollen and Tropet in 1990 [1, 2] in rock climbers and had not been described in the medical literature before. Only in 2006 Schöffl [20] described a few cases of closed flexor tendon injuries in non-climbing activities. Climbers initially treated the injury by taping their fingers around the proximal phalanx without impairment of function [1].
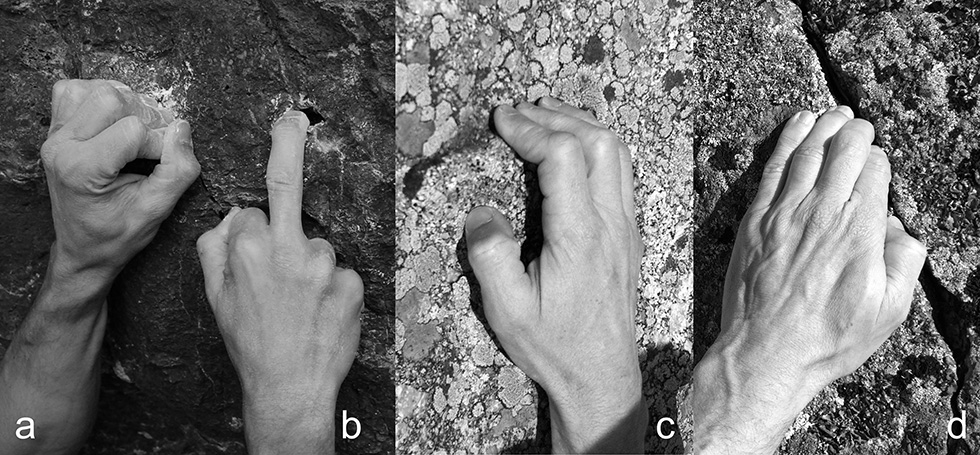
Figure 1
Typical full crimp grip position (A) to hold a small ledge. The PIP joints are flexed more than 90° and the DIP joints are hyper-extended, this way the thumb can also act as a holding force. One finger pocket (B) with typically completely flexed adjacent fingers increases flexion force of a single finger to up to 50%. The half/open crimp position (C) with PIP joints flexed to about 80° thereby generating most flexion torque. Squeezing and distorting the fingertips into a crack (D) is sometimes the only way to hold on.
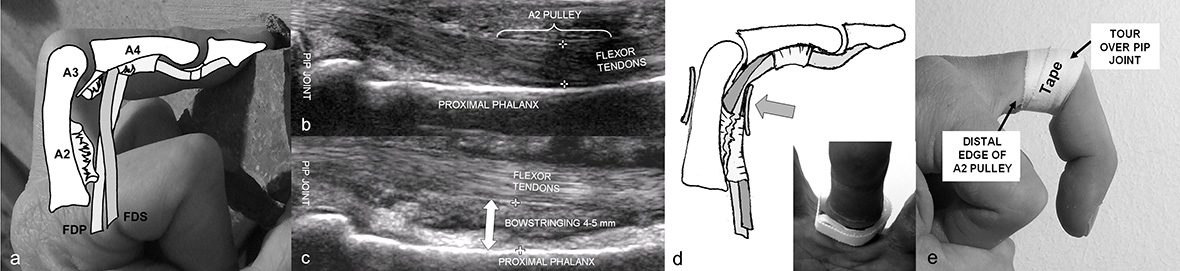
Figure 2
Finger flexor tendon sheath (A) with complete disruption of the A2 and the A3 pulley, partial disruption of the A4 pulley leading to bowstringing of the deep (FDP) and the superficial (FDS) flexor tendons. Ultrasound view of the normal anatomy (B) and of a disrupted A2 pulley (C) with an apparent bowstringing of the flexor tendons. A pulley protection ring (D) brings the flexor tendon back to normal position. Properly applied pulley tape (E) prevents flexion of the PIP joint of more than 80°.
The diagnosis of a pulley disruption is based on the history (pop or snapping sound) and on clinical examination, where a painful flexor tendon bowstringing can be palpated during resisted finger-flexion. The lift-off or bowstringing of the tendon visualised by ultrasound [21, 22] or a magnetic resonance imaging (less accurate) confirms the diagnosis. The treatment recommendations are controversial as some hand surgeons still treat single pulley-disruptions with reconstruction [23]. However, most accept treating single pulley-disruption conservatively eversince Schöffl [24] showed that even with non-operative management no objective or subjective functional loss occurred. Non-operative treatment is generally functional. The healing-time is between 2 to 3 months and full load-bearing can be expected after 4–6 months.
We recommend the use of a special pulley protection ring (fig. 2) designed to protect the neuro-vascular bundles while allowing an adequate reposition of the tendon without compromising circulation within the finger. After two months, the ring is replaced by a pulley protection tape (fig. 2). To take strain off the healing pulley it is applied around the PIP-joint and inhibits flexion of that joint to more than 80° above which pulley load becomes particularly high [17, 19]. With this treatment regimen we were able to reduce the initial bowstringing at the A2-pulley to about 50% and at the A4-pulley to about 40%. If the injury is left untreated or protected only with a tape the amount of bowstringing remains the same. If, however, two or even more pulleys are disrupted (for instance A2 an A3 or A2, A3 and A4-pulley), the amount of bowstringing increases substantially leading to a loss to the active flexion range of motion of the finger and a reconstruction of the ligament has to be considered. This can be performed with a graft from the extensor retinaculum or a free tendon graft. The results of such interventions are generally good and do not differ much between techniques [13, 25, 26]. However, whether all these patients need a reconstruction at all is still being debated. We have seen a series of patients with multiple pulley ruptures who returned to their previous climbing level without restriction except for a small loss of flexion range of motion. It has to be taken into consideration that pulley reconstruction leads to a rehabilitation time of several months.
Many climbers try to protect their flexor tendon pulleys by applying a circular tape around the proximal phalanx. Their intention is to prevent an injury of an otherwise healthy flexor tendon sheath (pulley system). Whereas in the situation of a disrupted pulley a certain amount of bowstringing can be relieved by a tape, any effect of a protective pulley-tape around an intact pulley is very unlikely [27, 28]. The main positive effect may be that the PIP-joint is not flexed more than 80–90° if the tape is applied close or even over the PIP-joint itself. Probably more important to prevent a pulley injury is the correct warming-up procedure and the avoidance of a pronounced crimp grip position. This consists of finger flexion exercises with therapeutic silicon rubber mastic and slowly increasing load to the finger flexors with climbing for 20–30 minutes. It has been shown that over the first 100 to 120 climbing moves the amount of physiological bowstringing of the flexor tendons shows an increase of up to 30%. This effect could only be shown when performing climbing movements and was not observed with other warming-up techniques. Therefore we recommend climbing about 3–4 routes with 40 moves or 8–12 boulder-problems [17] with increasing intensity.
Chronic tenosynovitis of the flexor tendons is the second most common finger problem in rock-climbers. Clinically the A2 or A4 pulleys are painful upon palpation; sonographically synovitis or scar formation and an alteration of the pulley similar to that of a trigger finger can be observed. Besides reduction of training intensity and strict prevention of the crimp-grip-position, local or systemic NSAID medications or steroid-infiltrations into the flexor tendon sheath are possible. The development of this problem can sometimes be very frustrating with recurrent painful periods lasting more than a year. Nevertheless, the prognosis is favourable and operative treatment such as tenolysis or a synovectomy are rarely necessary.
Injuries due one or two finger pockets
In difficult sport climbing routes, particularly in lime-stone crags, very small holes (called one or two-finger pockets) are sometimes only deep enough to provide a hold for the distal phalanges. These often very shallow pockets are blocked with only one or two fingertips. In order to increase the loading of one finger, all other (not loaded) fingers are completely flexed into the palm while the load-bearing finger is nearly extended (fig. 1); this increases the maximum flexion strength of up to 50% due to the cross-bridging fibres in the forearm musculature [17]. A side effect of this manoeuvre is that the flexor digitorum profundus tendons in the hand are shifted in different directions to one another. The common origin of the lumbrical muscle belly III and IV from two adjacent flexor digitorum profundus tendons are moved apart and may suffer a strain or muscle tear. This usually happens when pulling on a one-finger-pocket resulting in a sudden sharp pain in the palm. Clinically, pain in the palm can be provoked when grasping a one or two finger pocket but not when loading all fingers with a similar degree of flexion [3]. To prevent the formation of scar tissue in the lumbrical muscle belly and to prevent further injury, it is very important to start doing stretching exercises immediately following injury. This is done in the same way the injury was provoked but with much less load. A similar injury pattern is observed in the carpal tunnel at the wrist or in the extrinsic finger flexors in the forearm. Similar stretching exercises are recommended.
Crack climbing
Granite crack climbing requires its own specific techniques. Jamming and mortising the hand, arm, leg and even the whole body into a crack - depending on the size – is mandatory. Small cracks (1–4 centimetres in width) are climbed by jamming contorted fingers into the crack (fig. 1). If climbers slip off the rock with their feet, sudden high torsional forces are applied to the fingers, which may lead to fractures, ligament tears or even dislocation of the finger joints. These mostly non-climbing-specific injuries can usually be treated by conservative means (taping, small splints) if only ligaments are concerned (be aware of hardly visible impression fractures). However, the ligaments and capsular structures of the finger joints are complex and provide stability not only in the radio-ulnar direction. Therefore, instability has to be assessed by a physician in order to decide which kind of tape or splint is needed. If the treatment is inadequate, a later instability, deformation or contraction may develop. Only the ulnar collateral ligament of the metacarpophalangeal joint of the thumb (skiers-thumb) is an injury, which often has to be treated surgically. The problem in this situation is that the torn ligament may dislocate proximally over the adductor tendon and stay away from the original insertion [29]. Since no healing potential exists, this type of injury has to be excluded by a sonography or a MRI.
The wrist
As bouldering has become more and more popular, falls onto the wrist, even if protected with a crash-pad (portable mattress) have led to wrist injuries. But also falls during rope climbing with a swing against the wall absorbed by the hands are similar to high-energy trauma cases. Distal fractures of the radius are usually quite painful or have an obvious deformity when dislocated so that the climber shows up shortly after injury on an accident and emergency department. In contrast, injuries to ligaments (scapholunate or lunotriquetral ligament disruption), TFCC (triangular fibro cartilage, ulno-carpal disc) and particularly fractures of the scaphoid are very often only slightly painful. Frequently these injuries are seen only several months after the initial trauma. A ligamentous injury is quite difficult to treat at such a late stage and the prognosis is much worse. Scaphoid-fractures almost always turn into a non-union if left untreated and mostly end up in degenerative changes of the wrist (SNAC [scaphoid non-union advanced collapse] [30]). We recommend thoroughly investigating a wrist, which has been painful for more than three weeks to exclude such an injury.
A climbing-specific injury that we have observed is the indirect fracture of the hamate hook during a repeated attempt of an under-cling-grip on a difficult boulder. This climber held his wrist in an ulnar-abduction where the FDP-tendons of the small and ring-finger are deflected by the hamate hook. The high forces at the hamulus finally led to a basal-fracture of the hamate (indirect fracture type). The fracture could be treated successfully with a special splint in ulnar and radial deviation of the wrist [31].
The finger joints of “elderly” climbers and adolescents
Climbing of particularly difficult routes with small holds leads to very high impact-forces on the finger bones and joints with impressive changes of the thickness of the cortices (fig. 3) [32]. Whether rock-climbing leads also to a degenerative arthritis of the finger joint has already been debated and investigated by different authors [33–35]. They described radiographical changes of finger joints of long-term climbers such as osteophytes, subchondral sclerosis and joint space narrowing. Nevertheless, none of those authors could show clear evidence of an increased rate of degenerative arthritis compared to an age-matched group of non-climbers [33–35]. In these studies the radiographs were mostly performed in an anterior-posterior view and the changes of the joints were assessed according to the Kellgren and Lawrence [36] or the Altmann score [37]. We conducted a study [38] where we investigated the anterior-posterior and the lateral views of the fingers in a group of 31 Swiss performance sport climbers. The mean of years of climbing was 20 years and the mean of the highest reached sport climbing level was 8b redpoint (French grade, corresponding to UIAA grade 10). Almost all of the climbers had little or no symptoms in the finger joints but up to 84% showed osteophytes at the PIP-joints and up to 68% in the DIP-joints. According to the Kellgren and Lawrence score 6 climbers (19%) had signs of an osteoarthritis (significant) whereas the age-matched non-climbing-group had practically no signs of radiological changes in the finger joints. We observed that in the lateral views (fig. 3) the climbers showed even more impressive osteophytes in the DIP and PIP joints. However there were almost no other apparent changes such as subchondral cysts, osteolysis or joint space narrowing. Most of the climbers concerned had performed bouldering at a high level and were older than 35 years. These climbers reported rare episodes of slight pain and stiffness on the dorsal side of the joints when hitting hard objects or after climbing intensively with the crimp-grip-position. This can be explained by an irritation of the dorsal side of the joint capsule by the osteopytes [39]. The pain usually disappears after 3–5 weeks, sometimes corticosteroid-injections are necessary and very rarely such an osteophyte has to be removed. Even when calcified parts or osteophytes are broken off and freely move in the joint, they are taken up by the joint capsule and become asymptomatic after several weeks.
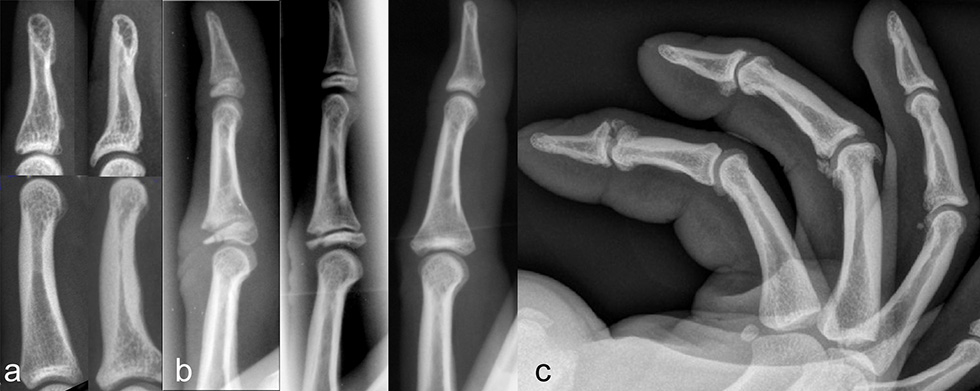
Figure 3
Osseous adaptations of climber’s distal and middle phalanx compared with a non-climbers bones (A); epiphyseal thinning (B, left), epiphyseal fracture (B, middle) in an adolescent climber, strict avoidance of crimp grip let the fracture heal without a joint surface incongruity or axial deviation (B, right); lateral view of the fingers of a 38-year-old world class boulderer, almost every joint shows osteophytes and calcifications of the capsule, joint space narrowing, a main sign of osteoarthritis however is not apparent.
We still do not know the long-term effects of sport climbing to the finger joints. The oldest climbers performing the sport at such a high level are generally not older than early fifties. However, it seems that the changes observed have arisen through adaptation and do not show the same pattern of the common inherited degenerative arthritis (poly-arthrosis).
In order to prevent the development of these changes, we recommend not using a pronounced crimp-grip-position with a flexion of the PIP-joints to more than 80–90° and trying to keep the DIP-joint always flexed to about 5–15°. This is the position (85° flexion) where the PIP joint generates maximal flexion torque [40, 41]. By doing so, the joints are loaded in a midway-position whereas the joint contact area remains as large as possible. The full crimp-grip where the thumb overlays the index finger should therefore be avoided wherever possible.
Particularly in young adolescent climbers or in children, the full crimp-grip-position has to be avoided. The growth plates of the finger bones are not closed until the age of 17–19 years, are the weakest structures of the finger, and are most susceptible to injuries [42, 43]. In the full crimp-grip-position a shift of the middle phalanx results in a very high load proximal to the dorsal part of the base of the middle-phalanx. This may lead to growth-plate overload, consolidation and partial necrosis and finally to growth plate fracture (Salter-Harris II fracture, fig. 3). Premature partial or complete closure of the growth-plate with uneven or interrupted further growth of the finger bone ending up in a considerable axial-deviation or foreshortened finger may follow. Even complete destruction of the joints and early degenerative changes are possible. As soon as pain without obvious trauma in the PIP-joints is apparent in an adolescent, the crimp-grip-position should not be tolerated at all until the pain disappears or the growth-plates have closed at the age of 17–19 years. Regular radiographic controls are mandatory.
Neurological and other soft tissue problems of the upper extremity
Carpal tunnel syndrome, the most common nerve compression syndrome [44] is also the most common reason for surgical nerve decompression in climbers and is managed in the same manner as in non-climbers without disadvantage (possible tendon bowstringing at the wrist). But also the radial nerve at the elbow and proximal forearm may be an origin of pain (supinator tunnel syndrome). Since this is purely a motor nerve, only weakness of the wrist and finger extensors and a dull pain are perceived. Stretching exercises and deep friction massage of the supinator muscle are usually helpful and surgery is rarely necessary. Rarely affected is the median nerve at its passage through the pronator teres and the ulnar nerve at the elbow (cubital tunnel syndrome) and at the hypothenar. Digital nerves may also be compressed [45] but rather acutely (neuropraxia) when squeezed into cracks or holes activating a sharp electrifying pain directly over the nerve with a hyposensitivity and numbness distal to the injury. Symptoms usually disappear after a few weeks.
In contrast to the commonly observed trigger finger of the A1 pulley, climbers mostly suffer from finger flexor tendosynovitis as mentioned above, usually at the A2 pulley, which is not associated with triggering. Ganglion cysts are found in climbers around the A1 and the A2 pulley, are usually only a few millimetres in size but rock-hard and may provoke pain under direct pressure during climbing. Again, digital nerves may come under pressure of such a cyst, which occasionally requires excision.
Besides the nerve compression syndromes around the elbow, the most commonly disturbing pain in climbers is the epicondylitis or epitrochleitis. These insertion tendinopathies can be very annoying but are usually self-limiting and rarely require surgery. Infiltrations of any medication [46] had no effect in a recent study and steroids in particular should be avoided. An effective treatment option is active strengthening [47] of the elbow flexors. The exercises are initially performed with shoulder abduction and pronation for golfer’s elbow and with adduction and supination for tennis elbow. The stronger the elbow flexors get, the more the arm can be pushed into the opposite shoulder position and forearm rotation until the symptoms are relieved. Apart from that, strengthening exercises for the antagonists of all flexor and internal rotators of the upper extremity are recommended to prevent muscular imbalance and overuse syndromes.
The shoulder
The extraordinarily high mobility and range of motion of the shoulder is possible only due to its very small joint surface of the glenoid on the one side and only a minimal bony contact (clavicle) to the axial skeleton on the other side. Stability is provided therefore mostly by active muscular control and a very lax joint capsule. The requirement of a shoulder joint during rock climbing is a large range of motion to reach holds positioned at some distance on the one side, and high force transmission often supporting the whole body weight in overhanging passages on the other. If this system gets out of balance with pain and limited range of motion or force transmission rock climbing becomes impossible.
Although acute injuries of the shoulder in the sense of contusion, acromio-clavicular ligament sprains or dislocation caused by a fall or during a hard climbing move in an abducted and externally rotated shoulder may happen [48], the majority of shoulder pathologies are due to repetitive overload injuries and micro-traumas and are probably the most common reason for a surgical intervention in climbers.
Younger climbers often report a deep antero-superior shoulder pain which is mostly due to proximal biceps tendonitis in the sulcus bicipitis with a possible coexisting biceps tendon pulley lesion, a SLAP lesion (superior labrum antero-posterior lesion of the glenoid) or bursitis subacromialis. MRI is diagnostic and initial treatment is conservative with improvement of active stability and centring of the gleno-humeral joint with physiotherapy and infiltration with corticosteroids. If intractable pain persists for months, biceps tenodesis and SLAP repair procedures need to be discussed. These are the most commonly performed procedures in younger climbers [49, 50] with satisfactory results. Most climbers return to their former climbing level.
Middle-aged climbers suffer in addition from outlet impingement with rotator cuff tears, acromio-clavicular and less frequently from glenohumeral degenerative changes. The pain appears also frequently at rest and during the night finally requiring surgery. In a retrospective survey Bircher et al. [50] reviewed 20 climbers with 21 operated shoulders rotator cuff pathologies. In addition an acromioplasty was performed in 17 shoulders and a biceps tenodesis of the long head of biceps in 15 cases. Rehabilitation was considerably time intensive but the same climbing level was eventually regained in almost all cases after an average of 12 months.
By way of prevention, regular exercises of the antagonists of the shoulder internal-rotators and flexors should be performed. Younger climbers should be advised to avoid dangling their whole body weight (during recovery positions) with completely relaxed shoulder muscles. Completely extended and relaxed joint positions should be avoided also during the so called dynamic moves, jump like movements between distant holds.
The lower extremity
Besides strength and mobility of the upper extremity sport climbing requires also a good mobility of the hip and knee joints with associated problems like antero-superior labral impingement with pre-arthrosis of the hip joint. Particularly in overhanging areas dedicated techniques like the “egyptian / drop knee (maximally internal rotated hip joint), foot hooks, heel hooks and toe hooks assume that strength and mobility of the lower extremity has to be optimal. These techniques stress particularly the hamstrings where often painful and protracted muscle strains are observed. In the knee joint common problems are degenerative or traumatic lesions of menisci or ligament lesion (ACL or MCL) for example caused by sudden falls from the egyptian position.
In sport-climbing high velocity injuries and ground falls have become very rare due to the improved protection devices (bolts, cams, friends) and ropes. But sport climbing even in gyms remains potentially dangerous. Handling errors of the belaying techniques still can lead to falls with several fractures (ankle fracture, open tibia fractures, pelvic fractures, spine fractures). A further common cause of ankle distortion and fractures is bouldering where down jumps from up to several metres are possible although the landing areas are protected by specialised crash-pads.
Several problems around the forefoot are due to the highly dedicated footwear. The climbing shoes are usually worn very tight which improves the ability to stand on small steps of only a few millimetres. The toes are in a hyperextend position in the MTP joints and flexed in the PIP and DIP joints. In addition newer shoe-designs have a flexed and internally rotated forefoot (down turn), which accentuates the former described positions of the toes. The consequences of such footwear are distinct callus formations on the top of the toe joints but also degenerative changes like ganglions, onychomykosis and ingrown painful toenails. The shoes may provoke hallux valgus deformation and very difficult to treat sesamoiditis of the MTP-joint.
The back and the neck
Moderate rock-climbing has a healthy impact for the back musculature which is also used by physiotherapists to treat lower back pain and to improve position and strengthen the trunk musculature. Nevertheless difficult climbing routes require sometimes holding on to so-called under-cling grips where the force vector of the hand is directed cranially. In such situations high compressive forces to the lumbar spine of up to 200 Nm may occur [51] and therefore many performance rock-climbers suffer from lumbar back pain. Treatment options are initially conservative means (physiotherapy, strengthening of antagonists / abdominal musculature). Symptoms around the cervical spine are often caused by the permanent hyperextended position of the belayer in very steep or overhanging routes. This problem can easily be solved with the now available prism glasses allowing for a vertical view direction.
Sport climbing has become quite a safe activity provided the belaying technique is preformed properly. Nevertheless the load to the upper extremity and particularly to the fingers is very high and has created new pathologies. As long as warming up is conducted regularly and particular finger positions (crimp grip) are kept to a minimum, rock climbing in moderate grades can be performed with minimal risk of damage to the locomotor system.
References
1 Bollen SR. Injury to the A2 pulley in rock climbers. J Hand Surg. [Br] 1990;15:268–70.
2 Tropet Y, Menez D, Balmat P, Pem R, Vichard P. Closed traumatic rupture of the ring finger flexor tendon pulley. J Hand Surg Am. 1990;15:745–7.
3 Schweizer A. Lumbrical tears in rock climbers. J Hand Surg. [Br] 2003;28:187–9.
4 Schoffl V, Winkelmann HP. Accident statistics at “indoor climbing walls”. Sportverletz Sportschaden. 1999;13:14–6.
5 Neuhof A, Hennig FF, Schoffl I, Schoffl V. Injury risk evaluation in sport climbing. Int J Sports Med. 2011;32:794–800.
6 Schussman LC, Lutz LJ, Shaw RR, Bohnn CR. The epidemiology of mountaineering and rock climbing accidents. Journal of Wilderness Medicine. 1990;1:235–48.
7 Backe S, Ericson L, Janson S, Timpka T. Rock climbing injury rates and associated risk factors in a general climbing population. Scand J Med Sci Sports. 2009;19:850–6.
8 Mannering FL, Grodsky LL. Statistical analysis of motorcyclist’ perceived accident risk. Accid Anal Prev. 1995;27:21–31.
9 Junge A, Dvorak J. Soccer injuries: a review on incidence and prevention. Sports Med. 2004;34:929–38.
10 Wedderkopp N, Kaltoft M, Lundgaard B, Rosendahl M, Froberg K. Injuries in young female players in European team handball. Scand J Med Sci Sports. 1997;7:342–7.
11 Molsa J, Kujala U, Nasman O, Lehtipuu TP, Airaksinen O. Injury profile in ice hockey from the 1970s through the 1990s in Finland. Am J Sports Med. 2000;28:322–7.
12 Gabbett TJ. Incidence of injury in amateur rugby league sevens. Br J Sports Med. 2002;36:23–6.
13 Schoffl V, Hochholzer T, Winkelmann HP, Strecker W. Pulley injuries in rock climbers. Wilderness Environ Med. 2003;14:94–100.
14 Josephsen G, Shinneman S, Tamayo-Sarver J, Josephsen K, Boulware D, Hunt M, et al. Injuries in bouldering: a prospective study. Wilderness Environ Med. 2007;18:271–80.
15 Paige TE, Fiore DC, Houston JD. Injury in traditional and sport rock climbing. Wilderness Environ Med. 1998;9:2–7.
16 Marco RA, Sharkey NA, Smith TS, Zissimos AG. Pathomechanics of closed rupture of the flexor tendon pulleys in rock climbers. J Bone Joint Surg Am. 1998;80:1012–9.
17 Schweizer A. Biomechanical properties of the crimp grip position in rock climbers. J Biomech. 2001;34:217–23.
18 Tan MA, Fuss FK, Niegl G. Dynamics of A2 finger pulley rupture. Journal of Mechanics in Biology and Medicine. 2007;7:75–87.
19 Schoffl I, Oppelt K, Jungert J, Schweizer A, Bayer T, Neuhuber W, et al. The influence of concentric and eccentric loading on the finger pulley system. J Biomech. 2009;42:2124–8.
20 Schoffl VR, Jungert J. Closed flexor pulley injuries in nonclimbing activities. J Hand Surg Am. 2006;31:806–10.
21 Klauser A, Frauscher F, Bodner G, Cihak C, Gabl M, Schocke M, et al. Value of high-resolution ultrasound in the evaluation of finger injuries in extreme sport climbers. Ultraschall Med. 2000;21:73–8.
22 Klauser A, Frauscher F, Bodner G, Halpern EJ, Schocke MF, Springer P, et al. Finger pulley injuries in extreme rock climbers: depiction with dynamic US. Radiology. 2002;222:755–61.
23 Moutet F, Forli A, Voulliaume D. Pulley rupture and reconstruction in rock climbers. Tech Hand Up Extrem Surg. 2004;8:149–55.
24 Schoffl VR, Einwag F, Strecker W, Schoffl I. Strength measurement and clinical outcome after pulley ruptures in climbers. Med Sci Sports Exerc. 2006;38:637–43.
25 Arora R, Fritz D, Zimmermann R, Lutz M, Kamelger F, Klauser AS, et al. Reconstruction of the digital flexor pulley system: a retrospective comparison of two methods of treatment. J Hand Surg Eur Vol. 2007;32:60–6.
26 Gabl M, Reinhart C, Lutz M, Bodner G, Angermann P, Pechlaner S. The use of a graft from the second extensor compartment to reconstruct the A2 flexor pulley in the long finger. J Hand Surg Br. 2000;25:98–101.
27 Schweizer A. Biomechanical effectiveness of taping the A2 pulley in rock climbers. J Hand Surg. [Br] 2000;25:102–7.
28 Warme WJ, Brooks D. The effect of circumferential taping on flexor tendon pulley failure in rock climbers. Am J Sports Med. 2000;28:674–8.
29 Stener B. Displacement of the ruptured ulnar collateral ligamnet of the metacarpo-phalangal joint of the thumb. J Bone Joint Surg. 1962;44B:869–79.
30 Watson HK, Ryu J. Evolution of arthritis of the wrist. Clin Orthop Relat Res. 1986:57–67.
31 Bayer T, Schweizer A. Stress fracture of the hook of the hamate as a result of intensive climbing. J Hand Surg Eur Vol. 2009;34:276–7.
32 Hahn F, Erschbaumer M, Allenspach P, Rufibach K, Schweizer A. Physiological Bone Responses in the Fingers After More Than 10 Years of High-Level Sport Climbing: Analysis of Cortical Parameters. Wilderness & Environtal Medicine 2012:in press.
33 Bollen SR, Wright V. Radiographic changes in the hands of rock climbers. Br J Sports Med. 1994;28:185–6.
34 Rohrbough JT, Mudge MK, Schilling RC, Jansen C. Radiographic osteoarthritis in the hands of rock climbers. Am J Orthop. 1998;27:734–8.
35 Sylvester AD, Christensen AM, Kramer PA. Factors influencing osteological changes in the hands and fingers of rock climbers. J Anat. 2006;209:597–609.
36 Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16:494–502.
37 Altman RD, Hochberg M, Murphy WA, Jr., Wolfe F, Lequesne M. Atlas of individual radiographic features in osteoarthritis. Osteoarthritis Cartilage. 1995;(3 Suppl A):3–70.
38 Allenspach P, Saupe N, Rufibach K, Schweizer A. Radiological changes and signs of osteoarthritis in the fingers of male performance sport climbers. J Sports Med Phys Fitness. 2011;51:497–505.
39 Schoffl V, Hochholzer T, Schoffl I. Extensor hood syndrome – osteophytic irritation of digital extensor tendons in rock climbers. Wilderness Environ Med. 2010;21:253–6.
40 Moor BK, Nagy L, Snedeker JG, Schweizer A. Friction between finger flexor tendons and the pulley system in the crimp grip position. Clin Biomech. (Bristol, Avon) 2009;24:20–5.
41 Schweizer A, Moor BK, Nagy L, Snedeker JG. Static and dynamic human flexor tendon-pulley interaction. J Biomech. 2009;42:1856–61.
42 Hochholzer T, Schoffl VR. Epiphyseal fractures of the finger middle joints in young sport climbers. Wilderness Environ Med. 2005;16:139–42.
43 Pfeifer C, Messner K, Scherer R, Hochholzer T. Injury pattern and overuse stress syndrome in young sport climbers. Wien Klin Wochenschr. 2000;112:965–72.
44 Peters P. Nerve compression syndromes in sport climbers. Int J Sports Med. 2001;22:611–7.
45 Ghiggio P, Nobile G, Cogola L, Testoni R. Wrist and hand nervous distress syndromes in sports. J Sports Traumatol. 1991;13:54–2.
46 Wolf JM, Ozer K, Scott F, Gordon MJ, Williams AE. Comparison of autologous blood, corticosteroid, and saline injection in the treatment of lateral epicondylitis: a prospective, randomized, controlled multicenter study. J Hand Surg Am. 2011;36:1269–72.
47 Peterson M, Butler S, Eriksson M, Svardsudd K. A randomized controlled trial of exercise versus wait-list in chronic tennis elbow (lateral epicondylosis). Ups J Med Sci. 2011;116:269–79.
48 Schweizer A, Bircher HP. Reposition of a dislocated shoulder under use of cannabis. Wilderness Environ Med. 2009;20:301–2.
49 Schoffl V, Popp D, Dickschass J, Kupper T. Superior labral anterior-posterior lesions in rock climbers-primary double tenodesis? Clin J Sport Med. 2011;21:261–3.
50 Bircher H-P, Thuer C, Schweizer A, Bereiter H. Shoulder injuries in sportclimbers, presentation at the Congress of Swiss Orthopaedic and Trauma Society. 2007.
51 Burtscher M, Jenny E. Häufigste trainingsbdingte Beschwerden und Verletzungen bei Sportkletterern. Praktische Sport- und Traumatologie und Sportmedizin 1987;2/87:15–21.