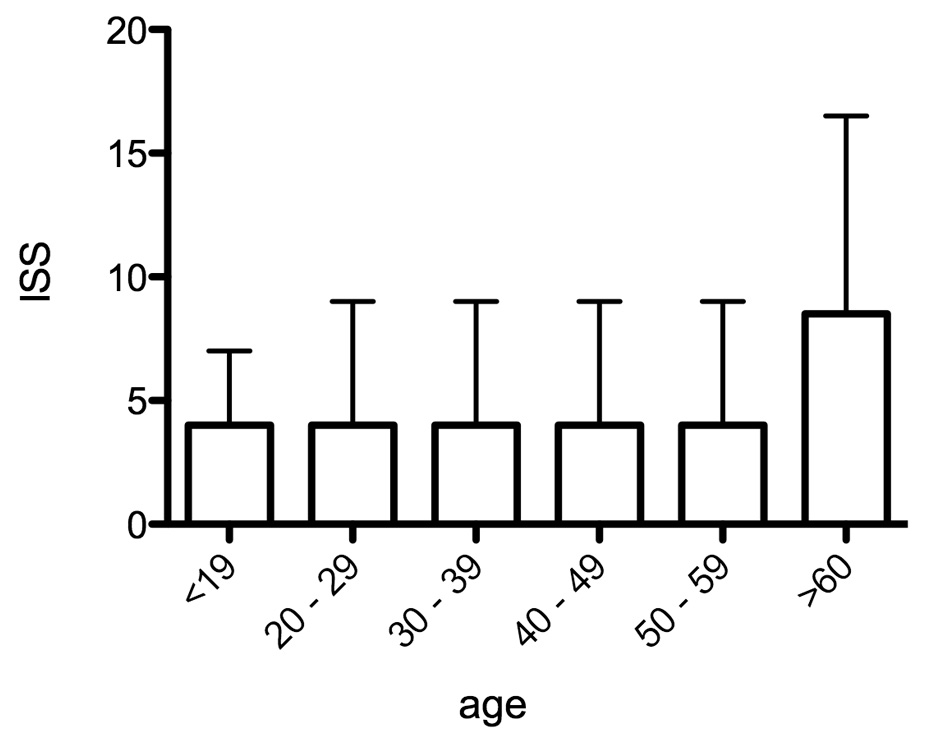
Figure 1
Level and distribution of the ISS by age group. Median, interquartile-range.
DOI: https://doi.org/10.4414/smw.2012.13674
A 10-year analysis from a Swiss university hospital trauma unit
In developed industrial countries, the most frequent causes of morbidity and mortality in construction workers are still falls or injuries from falling objects [1, 2]. Fatal occupational accidents are 50% more frequent at night (24:00–06:00 hours) than during the day [2]. In 2005, 141 Million working days were lost in the European Union due to occupational accidents, corresponding to 35 lost days for each accident [2]. In Switzerland, there are about 45 fatal occupational accidents per year. The rate of non-fatal occupational accidents has been calculated to be 1,133 per 100,000 inhabitants [3].
The types, circumstances and causes of injuries have been investigated and described in detail before by several authors [2–10]. The results of these studies have led to extensive health and safety measures and have greatly reduced morbidity and mortality in developed countries [3]. Thus, according to WHO Health Data, the number of non-fatal occupational accidents in Switzerland was almost halved between 1990 and 2005 [3].
The Swiss accident insurance agency SUVA have analysed their own figures for 2011 and concluded that there is a significant increase in occupational accidents on Monday mornings [5]. However, their analysis was restricted to stumbling and falls – the two most frequent causes of accidents in construction work. Moreover, they only used data from accident insurance companies and did not obtain information directly from hospitals. The same limitations apply to the analysis performed by the General Accident Insurance Agency in Austria on their data from 2004 to 2008 [6].
The present study, used data exclusively from the Department of Emergency Medicine University Hospital Bern/Switzerland and contains a 10-year analysis of accidents, injury patterns and risk factors in the building trade which led to medical treatment. To our knowledge, this is the first systematic long-term analysis of this type in Switzerland.
The Emergency Department of the main university hospital in the Canton of Bern is a tertiary trauma centre of super-regional importance. The intake area covers ca. 2 million inhabitants and there are about 35,000 emergency patients seen annually. All emergency patients are recorded and coded with an electronic patient administration programme. For the period 2001–2011, we identified all patients who reported their occupation as “construction worker” (Bauarbeiter) and/or identified the place of accident as a construction site (Baustelle). We used our hospital administration SAP and our digital patient data base “Qualicare”. Qualicare is a fully electronic data bank (3D), storing all personal data as well all patient history and other documents related to the patient’s treatment. Keywords can be searched and complete data sets “extracted” and analysed. All patient records then were searched by hand again and only primary injuries included. We agree that some occupations or sites of accident which could be prone to these types of accidents may have been missed. From this data set, we took information on the variables age, gender, nationality, day of accident, cause of accident, injury pattern and treatment. We also distinguished out-patient from in-patient treatment and conservative from surgical therapy.
Figure 1
Level and distribution of the ISS by age group. Median, interquartile-range.
Because literature on this topic is scarce and in order to be able to compare and discuss our study, we decided to classify according to the U.S. studies [7, 8]. As in these studies, we divided the patients into six age groups. But we chose a different age division within the groups, because the average age of U.S. construction workers is younger [7, 8].
The Injury Severity Score (ISS) was used to describe the severity of the injuries. This established medical score correlates with mortality, morbidity and hospitalisation time after trauma. The ISS differentiate 6 ISS body regions and the score ranges from 1 to 75. ISS define a major trauma or polytrauma if the score is greater than 15.
IBM SPSS 20 was used to perform descriptive analyses, based on the analysis of the frequencies of all variables in the data set. A one factor ANOVA and t-test were used to test whether there were significant differences between the different groups with respect to the means of the ISS values. Where appropriate, a post hoc test was used to establish which means were significantly different and at what level of significance. Correlations were tested between different degrees of injury to body parts. Correlations were also examined between days of the week, body regions, occupation (dichotomised) and country (selection of the most frequent countries).
782 patients were included in the study (778 men, 99.5%; 4 women, 0.5%). The median age was 36 (range 16–74 years).
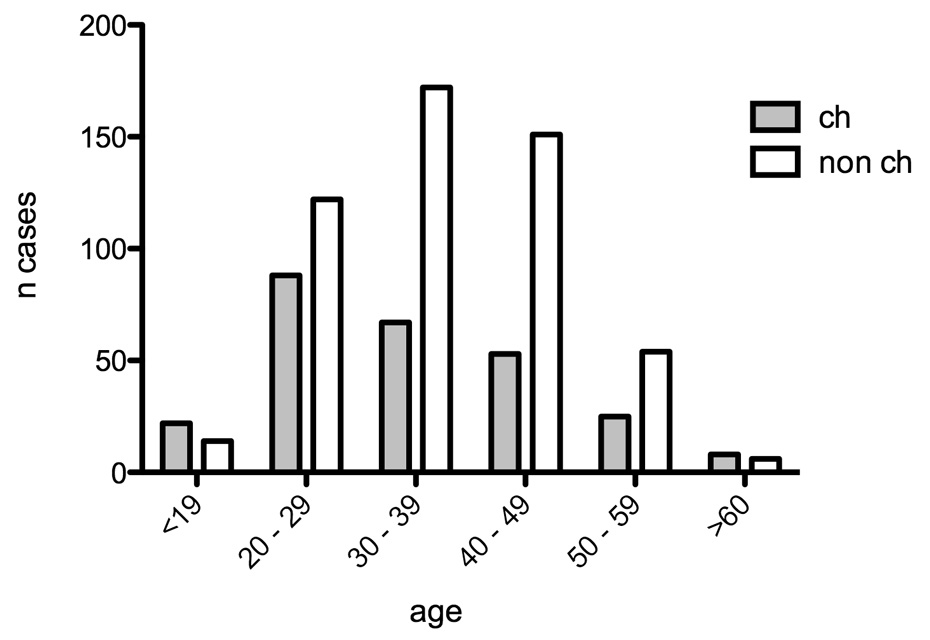
Figure 2
Frequency of accidents categorised by age and nationality. X-square: p <0.0001.
CH = Swiss; non CH = foreign workers.
Most patients were between 30 and 39 years (238, 30.4%), followed by 20‒29 years old (210/26.9%) and 40–49 years (203/26.0%).
Most of the patients were not Swiss citizens (519, 66.4%).
Distribution over the working days of the week was even; fewer patients came to the Emergency Centre on Saturdays and Sundays after an accident (table 1). For each working day, the median age was between 33 and 38 (16–74) (table 1). There was no statistically significant correlation between age and the day of the week (table 1).
For 54.9% of the patients, the cause was identified as “hit by a moveable object or piece of equipment” or “contact with a stationary object or piece of equipment” (table 2).
For 56.6% of patients, the diagnosis was contusion/abrasion or fracture (table 3).
The extremities were the most affected region of the body (472/782 patients), followed by purely external injuries (178/782) (table 4).
The median ISS value was 4 (0–75). The median ISS was also 4 for each working day (table 5). For each age group up to 60, the median ISS was 4; for patients above 60, it had the much higher value of 9 (table 5, fig. 1). The Kruskal-Wallis test between age groups and ISS gave a p of 0.089, showing a trend for older construction workers (>60 years) to suffer more severe injuries (table 5).
The median age was almost identical for Swiss and non-Swiss: Swiss 38 years (16–74); non-Swiss 37 years (17–61)); the median ISS was 4 (0–75) for both Swiss and non-Swiss. More Swiss than non-Swiss had injuries with ISS >15 (42/263, 16%, Swiss; 41/519, 8%, non-Swiss). The frequency of accidents of Swiss and non-Swiss worker categorised by age is shown in figure 2. Most patients were treated as out-patients (526, 67.3%). Most patients were treated as out-patients (526, 67.5%). Most treatment was conservative. The occupational accident was fatal in 3 cases (0.4%).
ANOVA tests between different categories did not reveal any significant differences; therefore no post test was applied. Correlations were calculated between week days, injury severity, body region, age, etc.; however, no pattern could be detected. These data are not shown.
| Table 1: Distribution of the number of patients and their age by the day of the week. | ||
| Day | N | Median (range) |
| Monday | 146 (18.7%) | 35 (16–61) |
| Tuesday | 123 (15.8%) | 38 (18–74) |
| Wednesday | 142 (18.2%) | 33 (18–70) |
| Thursday | 126 (16.1%) | 35 (17–64) |
| Friday | 114 (14.2%) | 37 (17–71) |
| Saturday | 57 (7.3%) | 36 (19–59) |
| Sunday | 74 (9.5%) | 33 (16–59) |
| The differences are not significant (p = 0.147). | ||
| Table 2: Causes and frequencies of the injuries. | |
| Causes | N |
| Hit by a moveable object or piece of equipment | 218 (27.9%) |
| Contact with a stationary object or piece of equipment | 209 (27%) |
| Squashing or compression by equipment or objects | 102 (13%) |
| Squashing or compression into collapsing material | 62 (7.9%) |
| Non-specific | 28 (3.6%) |
| Abrasions | 17 (2.2%) |
| Abrasions from vibrations | 1 (0.1%) |
| Unclassified | 145 (18.5%) |
| Table 3: Frequencies and distribution of the diagnoses. | |
| Diagnoses | N |
| Contusion/abrasion | 223 (28.5%) |
| Fracture | 220 (28.1%) |
| Sprain/stretching | 146 (18.7%) |
| Cut | 136 (17.4%) |
| Other diagnoses | 57 (7.3%) |
| Table 4: Distribution of the injuries over the regions of the body. | |
| Region | N |
| Extremities | 472 |
| External | 178 |
| Head/neck | 133 |
| Abdomen | 81 |
| Chest | 74 |
| Face | 68 |
| Table 5: Distribution of the median ISS over the age groups. | ||
| Age Group | N | ISS (median) |
| <19 | 36 (4.6%) | 4 (1; 66) |
| 20–29 | 210 (26.9%) | 4 (1; 61) |
| 30–39 | 238 (30.4%) | 4 (1; 75) |
| 40–49 | 203 (26.0%) | 4 (1; 36) |
| 50–59 | 79 (10.1%) | 4 (1; 59) |
| 60+ | 16 (2.0%) | 9 (1; 34) |
| There was a trend to higher ISS values at over 60 (p = 0.089). | ||
In December 2008, the European Commission issued a study on the causes of occupational accidents in the European Union. This showed that the number of occupational accidents decreases with increasing work experience and that the frequency of fatalities decreases with increasing age [2].
In our Swiss study, most injuries were in the 30 to 40 age group. Chau et al. found the same age distribution in their French study [4]. In two much larger American studies, with 1.7 and 0.57 million injuries, most patients were much younger, being 16 to 19 years old or 25 to 34 years old [7, 8]. It is worth noting that in 2011 the mean age in the USA was 36.5, which is about 4 years younger than the mean age in the Swiss population and 6 years younger than the mean in the German population. Interestingly enough, Lipscomb found that the accident rate was 5-fold higher in the 16–19 year old group than in the 55 to 64 year old group [7]. In the European Risk Observatory Report 2006, it was reported that the accident rate for 18- to 24-year olds was higher [12]. In our study, there was no trend for younger construction workers to be injured more frequently. Possibly our population is different from the population of the comparable studies.
0.5% of our construction workers were female. The comparable figures in 2007 were 1.0% for Western Europe, 2% for North America and even 7.5% for Asia.
We found a surprising result when classifying the injuries by nationality. The proportion of foreigners in the injured in our study was 66.4% – a very high value. This is more than twice the proportion of foreigners in the general labour market in Switzerland. According to the Swiss Accident Insurance Agency SUVA, this was only 30% in 2010, corresponding to the 26.4% of foreigners in the overall population [14]. The SUVA statistics for 2010 show that, for all of Switzerland, 40.7% of accidents were to foreigners [14]. We can see three reasons for the high proportion of foreigners in our study. First, there is the high proportion of foreigners in Switzerland (26.4%) compared to an average of 6.5% per country in the EU. Second, since 1960 the proportion of foreigners in the construction industry has been consistently high (about 60%). Third, there is also an above average proportion of temporary and part-time employees, including a relatively high proportion of foreigners and younger workers [15]. It is known that foreign employees have a greater risk of injury than the local population; in Europe, the USA and in other countries [7, 8, 13, 16, 17]. The reasons for this include the lower average level of education and the relatively high proportion of unskilled workers – which doubles the risk of an accident [15]. In 2009, a scientific analysis of the Swiss accident insurer SUVA for the optimisation of accident prevention showed two major influencing factors [15]. The better the training was, the lower was the risk of accidents. Unskilled workers have more than twice the risk of accidents [15]. At the beginning of a new job, the accident risk is greatest [15].
Well proven methods to improve occupational safety may be inadequate for temporary and part-time workers, who are often less well paid, must accept more dangerous work and who often speak the local language less well [15–17].
We have measured, the accidents were evenly distributed over the working days of the week. In contrast, the accident insurance agencies in Switzerland and Austria found that the risk was higher on Monday mornings [5, 6]. We failed to find this.
In our study, the two most frequently recorded causes were “hit by a moveable object or piece of equipment” or “contact with a stationary object or piece of equipment”. These were followed by “squashing” and “falling into collapsing material”. Comparable results have been found for the whole of Switzerland, Austria, Germany and the USA [5–8].
As described, the frequencies of the causes for occupational accidents in the building trade are almost identical in Europe and the USA. As expected, the results of the diagnoses of our patients do not differ from the analyses in comparable studies [4, 7, 8].
As regards the severity of the injuries, our results do not differ from those of Chau, Lipscomb or Shishlov [4, 7, 8]. We found a trend that older workers (above 60) were injured more rarely, but more severely. In general, we assume that older construction workers are at special risk due to prior diseases.
Our most striking result is that there is a very high proportion of foreigners among injured construction workers.
Contrary to expectations, we found that the distribution of accidents over the working week was even. Thus, we failed to confirm the conclusion of the Swiss (SUVA) and Austrian (AUVA) accident insurance agencies that Mondays are particularly dangerous.
If we consider our results and bear in mind that both foreigners and temporary and part-time employees are at particular risk, we can conclude that health and safety measures are relatively unsuccessful in these groups – for a variety of known reasons. To achieve a further reduction in the number of accidents suffered by construction workers, current successful health and safety measures must be established in the groups at risk and specific prevention campaigns must be carried out. There are therefore currently three new concepts for accident prevention [18]. First, “zero-accident-vision”: convincing people that accidents are preventable. Second, “integration”: extensive security measures across work, household work and leisure. Third, “globalisation”, increasing standards in large international companies. In our opinion the “zero-accident-vision” is suited to increase the insight of the employer’s responsibility for health and safety of the workers. This approach has the greatest potential to prevent accidents.
1. Morbidity and mortality most frequently caused by falls or injuries from falling objects.
2. Foreigners, temporary and part-time employees are at particular risk.
3. There is a trend for older construction workers to suffer more severe injuries.
4. Contrary to expectations, we found that the distribution of accidents over the working week was even.
5. Currently successful health and safety measures must be established in the groups at risk.
Acknowledgments:We particularly wish to thank Prof. Heinz Zimmermann, MD, Senior Consultant and Director of the Emergency Centre in Bern University Hospital, who made this study possible through his organisation of the Emergency Department. We also wish to thank the staff of the Emergency Department, who have recorded these data during the last 10 years and entered this into the database.
1 Ayers MH, McGarvey S, Stafford E. The construction chartbook. The U.S. construction industry and its workers. Publication. CPWR - Center for Construction Research and Training (2007). 4th ed. Silver Spring. Main findings, Page XV.
2 Europäische Kommission Generaldirektion Beschäftigung, Soziales und Chancengleichheit. Referat F4. Ursachen und Begleitumstände von Arbeitsunfällen in der EU. 2008.
3 WHO Regional Office for Europe. WHO Health Data. Arbeitsunfälle und Berufskrankheiten. Copenhagen Denmark. Indikatoren des Gesundheitswesens. 2012; available at http://www.gbe-bund.de. Last accessed 19 March 2012.
4 Chau N, Gauchard GC, Siegfried C, Benamghar L, Dangelzer JL, Francais M, et al. Relationships of job, age, and life conditions with the cause and severity of occupational injuries in construction workers. Int Arch Occup Environ Health. 2004;77(1):60–6.
5 SUVA Schweizerische Unfallversicherungsanstalt. Medienmitteilung vom 27.09.2010. Unfallstatistik: Achtung vor dem Montagmorgen 2010; available at http://www.suva.ch/startseite-suva/die-suva-suva/medien-suva/medienmitteilungen-suva/2010/unfallstatistik-achtung-vor-dem-montagmorgen/medienmitteilung-detail-suva.htmm. Last accessed 19 March 2012.
6 Allgemeine Unfallversicherungsanstalt Abteilung Statistik in Österreich 2009. Sturz und Fall. Unfallstatistik 2004–2008. Available at http://www.auva.at/mediaDB/MMDB130104_Sturz_und_Fall.pdf. Last accessed 19 March 2012
7 Lipscomb HJ, Schoenfisch AL, Shishlov KS. Non-fatal contact injuries among workers in the construction industry treated in U.S. emergency departments1998-2005. J Safety Res. 2010;41(3):191–5.
8 Shishlov KS, Schoenfisch AL, Myers DJ, Lipscomb HJ. Non-fatal construction industry fall-related injuries treated in US emergency departments, 1998–2005. Am J Ind Med. 2011;54(2):128–35.
9 Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften AWMF 2011. S3-Leitlinie Polytrauma / Schwerverletzten-Behandlung der Deutschen Gesellschaft für Unfallchirurgie. AWMF online (Stand 07/2011). Available at http://www.awmf.org/leitlinien/detail/ll/012-019.html. Last accessed 19 March 2012
10 Lefering R, Nienaber U. Jahresbericht 2010 des Traumaregisters Deutsche Gesellschaft für Unfallchirurgie (DGU), Sektion Intensiv- und Notfallmedizin, Schwerverletztenversorgung (NIS), Köln, 2010;7–9.
11 Bouillon B, Bühren V, Hinz P, Hoffmann R, Kubosch D, Kühne C, et al. Arbeitskreis Weissbuch. Schwerverletzten-Versorgung. Deutsche Gesellschaft für Unfallchirurgie (Hrsg.) Berlin 2006: 10–12.
12 European Agency for Safety and Health at work. Young workers – facts and figures. European Risk Observatory Report 2006. ISSN 1830-5946.
13 Ong VY, Habibah AK, Lee FC. Safety among foreign workers and impact on emergency medicine services in Singapore. Singapore Med J. 2006; 47(2):121–8.
14 Unfallstatistik UVG 2011. Available at http://www.unfallstatistik.ch. Last accessed 19 March 2012.
15 Studer R, Scholz-Obermatt S, Lanfranconi B. Unfallrisiken und Schadenverlauf im Personalverleih, SSUV Sammelstelle für die Statistik der Unfallversicherer, Luzern August 2009: 21, 25–29, 34, 51–52, 59–62.
16 Europäische Agentur für Sicherheit und Gesundheitsschutz am Arbeitsplatz. Available at http://www.osha.europa.eu/de/statistics/index/stm. Last accessed 19 March 2012.
17 Immigrant Workers at Risk 2005; available at http://www.aflcio.org. Last accessed 19 March 2012
18 Magazine of the European Agency for Safety and Health at Work. Preventing accidents at work. Available at http://osha.europa.eu/en/publications/magazine/4. 2002.
Funding / potential competing interests: No financial support and no other potential conflict of interest relevant to this article were reported.