Figure 1
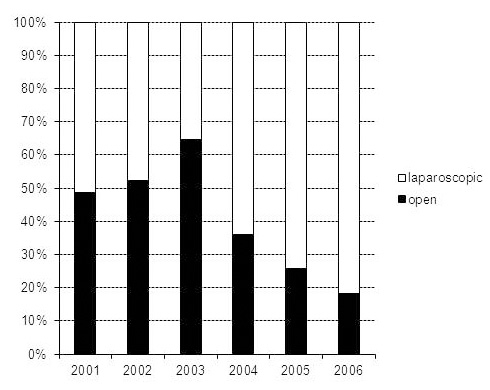
Percentage of open versus laparoscopic appendectomies.
DOI: https://doi.org/10.4414/smw.2012.13617
Quality assurance plays an important role in ensuring high quality of care in surgery. To ensure this high quality of care, many surgical departments in Switzerland are members of the working group for quality assurance in surgery (Arbeitsgemeinschaft für Qualitätssicherung in der Chirurgie [AQC]). The purpose of this working group is to create a database to capture the annual statistics of the clinics, as well as establishing personal procedure lists and assure quality of care [1].
The purpose of this study was to assess the value of the AQC database as a tool for quality assurance and as a source for scientific studies. To meet our goal, we chose to assess acute appendicitis. Acute appendicitis is a classic surgical disease which is frequently diagnosed. Acute appendicitis is predominantly a clinical diagnosis, and most patients present with a typical history and characteristic findings on examination. However, abdominal ultrasound and CT scans are increasingly used to establish the diagnosis and reduce the risk of unnecessary operations. This is especially important as acute appendicitis is a disease of the young. The highest incidence of appendicitis is found in patients between the age of 10 and 19 years [2, 3]. Appendicitis can be cured quickly by appendectomy. Traditionally, appendectomy is performed through a right lower quadrant open incision. Nowadays, however laparoscopy is an established treatment modality and increasingly appendectomies are performed by the laparoscopic approach [4].
In this study, we had two hypotheses. Firstly that the percentage of laparoscopic appendectomies would have increased over time without an increase in the complication rate, and secondly that these procedures would have been primarily performed by residents and junior faculty members according to the teaching concept at our hospital.
All appendectomies performed at the Department of Surgery of the Kantonsspital Olten between 2001 and 2006 were prospectively recorded in the AQC database. Multiple data points were recorded. Among other parameters, demographic data were collected including age and sex, type of procedure (laparoscopic versus open), the intraoperative diagnosis and status of the surgeon (resident, junior staff, senior staff) performing the procedure. Results were obtained by analysis of this database. All data entered in the database was reviewed and approved by one senior faculty member to ensure high quality of data. Some additional data was obtained from the Swiss outcome study for 2005 and 2006 [5]. The society “outcome” was founded in 1999. Its members are hospitals and insurance companies of the canton Zurich as well as the Health Department of Zurich. The purpose of the society is to perform quality assessment studies. Today, twenty different studies have been completed, among them the study for acute appendicitis. In this study, the following parameters were recorded among others: the delay from entry into the emergency department until surgery, length of hospitalisation and histological diagnosis. Our hospital was part of the appendicitis study in 2005 and 2006.
Statistical comparisons were based on Fisher’s exact test.
Overall, 684 appendectomies were performed at our institution between 2001 and 2006. Three hundred procedures were performed in women and 384 procedures were performed in men. Most of the patients were between 10 and 29 years old at the time of the procedure. The mean age of the patients was 33 (SD 19.27) years.
Figure 1
Percentage of open versus laparoscopic appendectomies.
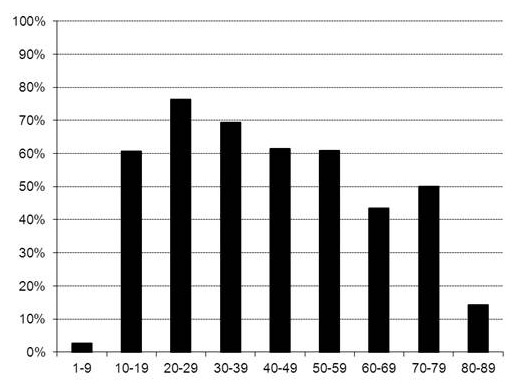
Figure 2
Percentage of laparoscopic procedures by age of the patients.
In our clinic, the standard surgical approach for appendicitis today is laparoscopy. After a slight increase of open procedures between 2001 and 2003, we recorded a clear increase in the use of laparoscopic interventions from 51% in 2001 to 81% in 2006 of all procedures performed (fig. 1).
The percentage of laparoscopic procedures was highest in patients between 20 and 39 years of age. In very young patients under 10 years old, just one out of 37 procedures was done by laparoscopy. Furthermore, there was a decrease in the percentage of laparoscopic procedures in the elderly patients (fig. 2). However, there were seven procedures done in patients older than 80 years.
According to the teaching concept at our hospital, appendectomies should be performed by residents or junior faculty members. This was confirmed by our study. Ninety three percent of all appendectomies were performed by the residents or the junior faculty members (fig. 3). Furthermore, we could demonstrate a significant increase in the proportion of laparoscopic procedures performed by residents from 7% in 2001 to 44% in 2006 (from 4/57 to 44/99 procedures, p <0.01), as well as an overall increase in the absolute number of procedures performed by residents (from 18 in 2001 to 52 in 2006).
In this study, special interest was placed on the percentage of negative appendectomies. The percentage of appendices that seemed to be non-inflammatory during the operation by the surgeon could be evaluated by the ICD-10 diagnosis codes in the database. The percentage of negative appendectomies in this study was around 3% (fig. 4). This correlated with data of the outcome study, where the histological diagnosis was evaluated. Histological diagnosis showed no signs of inflammatory changes in 6.1% of appendectomies performed in our clinic in 2005 and 2006.
The main postoperative surgical complications in our study was surgical site infection in 3.6% of the open procedures as compared to no surgical site infections in laparoscopic procedures (p <0.001). Intra-abdominal abscess formation was recorded in 2.7% of laparoscopic procedures as compared to 1.8% in open surgery. There was no significant difference between laparoscopic and open procedures (p = 0.608). The overall postoperative complication rate in the study was 5.4% with no statistical difference between open (6.5%) and laparoscopic (4.7%) surgery (p = 0.305). The re-intervention rate in this study was 3.8%.
From 2005 to 2006, our department took part in the Swiss outcome study for appendicitis. In this study, additional data were collected. Among other parameters, the delay from entry into the emergency department until surgery was determined. The average delay from entry into the emergency department until surgery was 7.6 hours in 2005 and 2006. Furthermore, length of hospitalisation was also recorded. The average hospital stay in these patients was 4.7 days during these two years.
The percentage of histologically perforated appendicitis could also be determined in the outcome study. In our clinic, we had a clear decrease of perforated appendicitis from 29% in 2005 to 15% in 2006 (n = 19, 12 resp.).
This study clearly shows that the AQC database offers a wide variety of possibilities for quality assurance and scientific analyses due to the large amount of data collected, as well as the quality of the data collected.
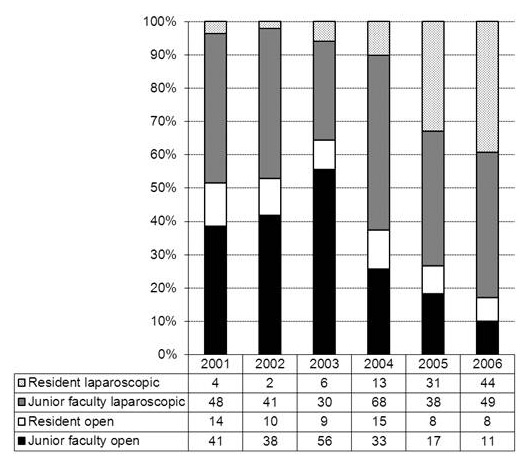
Figure 3
Percentage and absolute numbers of procedures by status of the surgeon (residents / junior faculty members).

Figure 4
Percentage of negative appendectomies by the surgeon during the procedure.
For this study, we had two hypotheses. Firstly that the percentage of laparoscopic appendectomies would have increased over time without an increase of the complication rate, and secondly that these procedures would have been performed primarily by residents and junior faculty members according to the teaching concept at our hospital. We could demonstrate that the percentage of laparoscopic procedures increased clearly from 2001 to 2006, and that these appendectomies were mainly performed by residents and junior faculty members at our hospital according to our teaching concept. Both the proportion of laparoscopic procedures performed by residents and the absolute number of procedures performed by residents increased during that time.
Acute appendicitis is a disease of the young. The highest incidence of appendicitis is found in patients between the age of 10 and 19 years [2, 3]. This correlates with the data found in our study. Accordingly, appendectomy was performed most in younger patients. In our study, younger adult patients were more likely to undergo laparoscopic appendectomy than elderly patients. The open approach was more often considered in elderly patients because of previous abdominal surgery.
However, in children, laparoscopic appendectomy was rarely used. In small children, there is often not enough space in the abdomen for the standard laparoscopic approach. Therefore, an open procedure with a little 2 to 3 cm incision in the right lower abdomen was performed.
Acute appendicitis is predominantly a clinical diagnosis, and most patients present with a typical history and characteristic findings on examination [4]. In our department, the diagnosis algorithm consists of the clinical examination and history of the patient. White blood count (WBC) and C-reactive protein (CRP) are measured. Serial clinical and laboratory examinations are performed as necessary. Ultrasound examinations are not routinely used, but are ordered if the clinical picture is unclear. Especially in younger female patients ultrasound examinations can be used to confirm the clinical diagnosis or to rule out other inflammatory pelvic diseases. CT scans are rarely used in our clinic. They are ordered if the clinical picture and ultrasound examinations are inconclusive. Fifty-six percent of our patients did not have any ultrasound or CT studies for the diagnosis of appendicitis, as opposed to 16% in the other hospitals participating in a recent outcome study. Ultrasound was applied in 26% of the cases, and CT scans in 20% (72 and 20% in the other hospitals, resp.), with few patients having both.
In this study, the percentage of appendectomies that were thought to be negative by the surgeon during the procedure was around 3%. In contrast, histological diagnosis showed no signs of inflammatory changes in 6.1% of appendectomies performed, consistent with the literature [6, 7]. Our diagnosis algorithm, explained above, was able to reliably establish the diagnosis in most of the cases. It is also important to note that most of the indications for appendectomy are confirmed by a senior staff member at our hospital. Besides the use of ultrasound examinations, this could also explain the relatively low rate of perforated appendicitis in the study. Furthermore, there was little delay from admission to the hospital until surgery.
The laparoscopic appendectomy itself is a safe procedure with a low complication rate [8, 9]. In 2011, Brügger et al. published the results of the Swiss Association of Laparoscopic and Thoracoscopic Surgery (SALTS) database. The overall postoperative surgical complication rate in this study of laparoscopic appendectomies was 4.24%, correlating nicely with the complication rate of the present study [10].
In the literature, discussion of the laparoscopic approach for appendectomy remains somewhat controversial. Some authors claim laparoscopic appendectomy shows fewer wound infections, less postoperative pain and shorter hospital stay but more intra-abdominal abscess formation than open surgery [11, 12]. On the other hand, other authors found no significant differences between the open and the laparoscopic procedure [13]. In addition, a recent meta-analysis that reported on overall postoperative complications found only non-significant differences between the open and laparoscopic procedures [14]. These studies correlate with the results of our study where we found more wound infections in open surgery, whereas there were more intra-abdominal abscess formations in the laparoscopic group. However, there was no significant difference in overall complication rates between the open vs. the laparoscopic group.
Laparoscopic appendectomy is sometimes technically more demanding and requires special equipment as well as special training of the operation room staff. From a teaching standpoint, we found that laparoscopic appendectomy is a good introduction to laparoscopy and can be performed as a laparoscopic teaching operation in a safe manner as demonstrated by the low complication rate [15]. This is of special importance in regard to the 50 hour working week limitation in Switzerland. It has previously been shown that limitations in working hours may jeopardise resident education and patient care by worsening surgical training [16]. In addition, a recent study showed a significantly higher postoperative surgical complication and in-hospital mortality rate after the reform, but no increase in intraoperative complication rates [17]. Therefore, early introduction and training in laparoscopy is very important for the surgical training and can be initiated by laparoscopic appendectomy.
The purpose of this study was to assess the value of the AQC database as a tool for quality assurance and as a source for scientific studies. We could clearly demonstrate that the AQC database itself offers a wide variety for scientific analyses. But as is true for all databases, it is most important to have good data entry to obtain good results. In our experience, one person in a leading faculty position has to be responsible for review and release of the data in this database in order to achieve high standards in quality assurance that can be used for scientific studies and analyses.
Acknowledgements:The authors like to thank Prof. Dr. med. U. Güller for the statistical analysis.
1 AQC Homepage 2007, http://www.aqc.ch
2 Ohmann C, Franke C, Kraemer M, Yang Q. Status report on epidemiology of acute appendicitis. Chirurg. 2002;73(8):769–76.
3 Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132(5):910–25.
4 Humes DJ, Simpson J. Acute appendicitis. BMJ. 2006;333(7567):530–4.
5 Outcome Messung T01- Appendizitis und Verdacht auf Appendizitis, Hauptmessung 2006, Verein Outcome, Josefstrasse 92, CH-8005 Zürich.
6 SCOAP Collaborative, Cuschieri J, Florence M, Flum DR, Jurkovich GJ, Lin P, Steele SR, et al. Negative appendectomy and imaging accuracy in the Washington State Surgical Care and Outcomes Assessment Program. Ann Surg. 2008;248(4):557–63.
7 Güller U, Rosella L, McCall J, Brügger LE, Candinas D. Negative appendicectomy and perforation rates in patients undergoing laparoscopic surgery for suspected appendicitis. Br J Surg. 2011;98(4):589–95. doi: 10.1002/bjs.7395. Epub 2011 Jan 24.
8 Ignacio RC, Burke R, Spencer D, Bissell C, Dorsainvil C, Lucha PA. Laparoscopic versus open appendectomy: what is the real difference? Results of a prospective randomized double-blinded trial. Surg Endosc. 2004;18(2):334–7.
9 Faiz O, Clark J, Brown T, Bottle A, Antoniou A, Farrands P, et al. Traditional and laparoscopic appendectomy in adults: outcomes in English NHS hospitals between 1996 and 2006. Ann Surg. 2008;248(5):800–6.
10 Brügger L, Rosella L, Candinas D, Güller U. Improving outcomes after laparoscopic appendectomy: a population-based, 12-year trend analysis of 7446 patients. Ann Surg. 2011;253(2):309–13.
11 Sauerland S, Lefering R, Neugebauer EA. Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database Syst Rev 2004;(4).
12 Tiwari MM, Reynoso JF, Tsang AW, Oleynikov D. Comparison of outcomes of laparoscopic and open appendectomy in management of uncomplicated and complicated appendicitis. Ann Surg. 2011;254(6):927–32.
13 Katkhouda N, Mason RJ, Towfigh S, Gevorgyan A, Essani R. Laparoscopic versus open appendectomy: a prospective randomized double-blind study. Ann Surg. 2005;242:439–48, discussion 448–50.
14 Sauerland S, Jaschinski T, Neugebauer EA. Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database Syst Rev. 2010;(10):CD001546. Review.
15 Emmanuel A, Byrne J, Wilson I, Balfe P. Is laparoscopic appendicectomy a safe procedure for trainees in the peripheral hospital setting? Ir Med J. 2011;104(9):276–8.
16 Whang EE, Mello MM, Ashley SW, Zinner MJ. Implementing resident work hour limitations: lessons from the New York State experience. Ann Surg. 2003;237(4):449–55.
17 Kaderli R, Businger A, Oesch A, Stefenelli U, Laffer U. Morbidity in surgery: impact of the 50-hour work-week limitation in Switzerland. Swiss Med Wkly. 2012;142:0.
Funding / potential competing interests: No financial support and no other potential conflict of interest relevant to this article were reported.