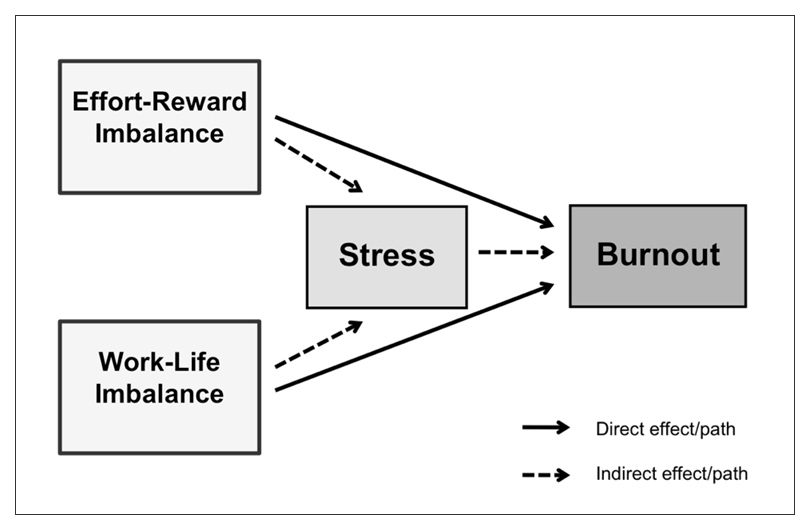
Figure 1
Conceptual path model.
DOI: https://doi.org/10.4414/smw.2012.13577
Burnout is a commonly used and well studied concept in work-related psychosocial health research. It is considered to be a job stress phenomenon, conceptualised as a response to permanent or chronic stressors on the job [1, 2], a lagged affective reaction to prolonged exposure to stress at work [3] or a consequence of long-term involvement in adverse and emotionally demanding work situations [4–7]. Burnout describes a form of mental distress or a persistent negative state of mind that is associated with depression, sleep disorders, hypertension, headaches and many others health disorders [2, 4]. While some researchers have defined burnout as a psychological syndrome with distinct symptoms or components such as exhaustion, cynicism and inefficiency [1], others have characterised it primarily by emotional exhaustion and fatigue [5].
Over the past years, many studies have tried to identify the primary causes and early predictors of burnout and “high risk” people in this regard [2]. As already noted, work stress in general and work stressors in particular, such as high workload, lack of social support, direct patient or client contact, and many more, have been identified as correlates or antecedents of burnout [2, 8]. Thus, all long-lasting and work-related stressors are basically potential predictors or risk factors of burnout.
Two work-related stress models have received special attention in previous occupational stress research, the job demand-control model of Karasek and Theorell [9] and the model of effort-reward imbalance (ERI) of Siegrist [10]. These models conceptualise job stress as a result of a discrepancy between high job demands and low job control [9] or an imbalance between high effort spent and low reward received at work [10].
In addition to these established stress models, another concept related to job stress has been well explored, at least in occupational health psychology: the concept of work-family conflict (WFC) or work-home interference [11, 12]. This concept is situated at the interface between work and family life and was developed and conceptualised as a multidimensional, bidirectional construct [13, 14]. In contrast to the other mentioned concepts that localise stress in an imbalance within work, the concept of WFC is about an imbalance or conflict in between the work and the family domain. A negative spillover from one domain to the other and vice versa in the form of inter-role conflicts affecting at least one domain indicates an imbalance between these two life domains.
In contrast to the traditionally narrow focus on role conflicts between work and family, which largely restricts WFC research to employees who live with a partner or spouse and with underage and dependent children [15], we use the more comprehensive term of work-life conflict (WLC) or rather work-life imbalance (WLI) and a measure somewhat distinct from the commonly used WFC scale (see Measures section). This term not only expresses our broader scope and extended study population but also highlights the conceptual similarity to the ERI model.
Both concepts of imbalance, the ERI model and the WLI concept, have been studied in relation to burnout. Conditions of high efforts put into the job combined with low rewards received from the job have been found to be stressful and detrimental to health as expected [10, 16–18]. Such experiences of lacking reciprocity or perceptions of inequity at work go along with depression [19–22] and in particular with emotional exhaustion and burnout as has been shown by some studies [8, 17, 23–26]. Negative spillover effects and role conflicts between work and family or private lives indicating WLI also have repeatedly been shown to be quite strongly associated with job stress or general psychological or emotional distress [12, 27–29] and/or with burnout [3, 27, 30–32] or fatigue as a single burnout symptom [15, 33–35].
The studies on the association of ERI and burnout (or exhaustion) are small in number and, with the exception of a large-scale cross-sectional study by de Jonge et al. [17], restricted largely to “people work” and so-called helping professions such as nursing or teaching. Although studies on WFC and burnout are quite numerous, they are restricted mostly to small and homogeneous samples and specific professional categories.
In summary, it can be said that both ERI and WFC are recognised risk factors of work stress and as such have been identified as predictors of burnout. Although few studies have investigated ERI in the context of the work-home interface or in combination with WFC respectively [36–38], such combined research is completely lacking in relation to stress or burnout as common outcomes. No such study has been done or published so far, neither in Switzerland nor in other countries. The main aim of the present study, therefore, was to explore to what extent these two forms of imbalance are associated with general psychological stress and burnout independent of each other and to compare them in this regard.
Figure 1
Conceptual path model.
Another aim was to study this relationship in a hospital setting with many health care professionals such as physicians, therapists and nurses who do physically and/or emotionally demanding “people work” and often have irregular and/or long working hours and therefore experience most likely effort-reward and work-life imbalance and, thus, are at comparably high risk of stress and burnout.
The basic assumptions underlying the study are to be tested as pictured in the conceptual path model (see fig. 1). ERI and WLI as recognised work-related stressors are both expected to be positively but possibly unequally associated with general psychological stress and burnout symptoms. Whereas WLI is regarded as an overarching concept of conflict and is thus assumed to be a source of general stress, ERI is described as an entirely work-related phenomenon and is conceptualised as a predictor of job stress. WLI, thus, is expected to be a stronger predictor of general stress than ERI. In contrast, ERI as a work-specific stressor is expected to be a stronger predictor of burnout than WLI, since burnout as a job stress phenomenon is considered to be a reaction or response to prolonged stress at work [2, 3]. Also, general psychological stress is assumed to be the immediate or intermediate outcome and burnout the final outcome of a failed reciprocity at work and a perceived job-related gratification crisis (referred to as ERI) and of experienced role conflicts at the interface between work and private life (referred to as WLI). In other words, general stress is considered to be a short-term reaction to stressors like ERI or WLI, whereas burnout is considered to be a lagged reaction to such stressors. Therefore, associations of ERI and WLI with burnout are expected to be partly mediated by general psychological stress.
In addition to these assumptions medical care professionals such as physicians, nurses and therapists are hypothesised to be highly exposed to ERI and WLI and therefore to be “high risk” people with regard to stress and burnout and in comparison with other hospital employees. The assumption of helping professions being more than average exposed to ERI and WLI and therefore more affected by psychosocial and stress-related health risks is partly based on existing evidence from Switzerland and from a comparison of physicians with other academics and the general working population in this regard [39].
This cross-sectional study is based on survey data from a sample of employees of a large public hospital in the canton of Zurich that covers nurses and physicians and also people in non care giving professions. The survey was carried out among the workforce of the Cantonal Hospital of Winterthur. The study sample also included persons not living with a partner and/or children who are usually excluded from WFC research.
The data were collected in 2007 by a postal survey using a self-developed fully standardised and comprehensive questionnaire with well-established and validated multiple- and single-item measures for all relevant study variables. Out of a total staff of around 2,160 employees (at the time of survey) a stratified random sample was drawn. From these 960 randomly selected employees (gross sample) that were asked by letter to participate in the survey 502 members of staff finally completed and returned the questionnaire (net sample). The study sample consists of physicians (10.9%), nursing staff (47.6%), technical care personnel and emergency staff (10.5%), medical technical personnel and therapists (12.9%), administrative personnel (10.5%) and logistic personnel (7.6%). Consisting to a large proportion of women (77.8%), Swiss citizens (85.3%), part-time employees (85.1%) and highly educated persons (43.7%), the study sample differs significantly from the general working population. While the overall response rate was 52%, the response rates among the different occupational groups ranged between 29% (technical care personnel and emergency staff) and 77% (medical technical personnel and therapists). The response rate of the physicians was 43% and that of the nursing staff 63%.
Effort-reward imbalance (ERI): A short version of the original ERI questionnaire of Siegrist and Peter [40] was used to measure the model of ERI. The ERI questionnaire originally consisted of two scales measuring its extrinsic components of “effort” and “reward”, and a third scale assessing its intrinsic component of “overcommitment”. In this study as in many other prior studies, “overcommitment” was not included.
Of the originally used two-stage Likert scale items, 10 out of 17 were selected in order to measure the two extrinsic components of “effort” and “reward”. More precisely, five items from the original 6-item effort scale (e.g., “Due to the heavy workload, there is often a lot of time pressure”), and five items from the 11-item reward scale were used. The reduced 5-item reward scale covers all three components of occupational gratifications, namely money (1 item on appropriate salary), esteem (1 item each on sufficient respect and recognition from colleagues and from supervisors) and career opportunities (1 item each on adequate promotion prospects and on status consistency).
Traditionally, ERI has been analysed by calculating the ratio between the effort score (nominator) and the reward score (denominator), multiplied by a correction factor to adjust for the unequal number of items in both scales. With a cut-off at one, a ratio above one is considered to be indicative of an imbalance between effort and reward. Nevertheless, some studies have applied the ratio as a continuous and not a dichotomous variable, following Niedhammer et al. [41], who suggested that a continuous score may be more useful, particularly in samples where few individuals score higher than one. This study took the same approach and applied the ERI ratio as a continuous variable (or in its recoded version as an ordinal scale) for most statistical analyses. However, for stratified logistic regression analyses the ERI ratio was dichotomized in order to avoid too large confidence intervalls due to small numbers of cases. For more differentiated linear regression analyses, the two scales with their sum scores ranging from 5 to 25 (effort scale; α = 0.79) and from 8 to 25 (reward scale; α = 0.62) were used in place of the ERI ratio.
Work-life imbalance (WLI): WLI was assessed by an adapted and shortened version of the well-established and validated 18-item WFC scale of Carlson et al. [13]. The 10-item measure used in this study incorporates four of the six recognised dimensions of the WFC construct, namely the time- and strain-based forms of both directions (work conflicting with family, family conflicting with work). In accordance with Netemeyer et al. [12] and in line with most other studies in this field since then, the behavioural-based forms of both directions were not covered in the questionnaire and therefore not considered in this study. At least two or all three items of each of the remaining four 3-item subscales used in the original and consolidated 18-item WFC scale of Carlson et al. [13] were selected, translated into German and slightly reformulated by replacing or complementing the term “family” with “private life” or other expressions comprising the whole non-work domain.
Participants were asked to what extent they agreed or disagreed with ten statements, each with five suggested responses ranging from ‘Completely disagree’ (score 0) to ‘Completely agree’ (4). Two or three items were used for each of the measured dimensions and subscales.
We constructed an accumulated 10-item scale with a total score (WLI score) ranging from 0 (‘No conflict’) to 40 (‘Very strong conflict’), and alternatively four 2- and 3-item subscales indicating all four conceptual dimensions of the construct. A reliability analysis resulted in acceptable up to very good Cronbach’s alpha coefficients as measures of internal consistency for the consolidated WLI score (α = 0.74) as well as for the subscales measuring the time-based work-to-life conflict (α = 0.75; 3 items, e.g., “I regularly miss private events or family activities because of my work.”), the strain-based work-to-life conflict (α = 0.90; 2 items, e.g., “When I come home from work, I feel often too drained to take part in family or private activities.”), the time-based life-to-work conflict (α = 0.57; 2 items, e.g., “My family and personal obligations often keep me from participating in work events which are important for my career.”) and the strain-based life-to-work conflict (α = 0.77; 3 items, e.g., “Family tensions or personal worries often lower my performance at work”).
General psychological stress: Psychological stress or distress was assessed by a general indicator of stress symptoms developed in the early 1970s, a single-item measure that has been validated and suggested for use in survey research in place of longer measurement scales by Elo et al. [42]. This single item refers to the general experience of stress and not specifically to job stress. First, the following definition of stress was given: “Stress means a situation in which a person feels tense, restless, nervous and anxious and/or is unable to sleep at night because his/her mind is troubled all the time”. Second, after this definition respondents were asked to report on how often they felt stressed in such a way in the last 12 months. The response was recorded on a 4-point scale varying from ‘Never’ (score 0) to ‘Very often’ (3).
Burnout: Burnout was measured using the Copenhagen Burnout Inventory (CBI) [5]. The CBI was developed as an alternative to the most widely used Maslach Burnout Inventory (MBI) [1, 43]. Its use is not restricted to “people work” but is basically applicable to all work domains, settings and professions. The CBI consists of three different dimensions or subscales measuring personal, work-related and client-related burnout. Given the restrictions on the length of the questionnaire, we used a shortened version of the original 21-item scale covering all three dimensions of the CBI. Three items for personal burnout (e.g., “How often do you think: ‘I can’t take it anymore’?”), three for work-related burnout (e.g., “Are you exhausted in the morning at the thought of another day at work?”) and two for client-related burnout (e.g., “Are you tired of working with clients or patients?”) were selected. Respondents were required to indicate how frequently these burnout symptoms were experienced with given response categories from ‘Never’ (score 0) to ‘Seldom’ (25), ‘Sometimes’ (50), ‘Often’ (75) and ‘Always’ (100).
Due to the small number of selected items for each dimension (reliability analyses resulted accordingly in rather low alpha coefficients between 0.59 and 0.75) and for other practical and statistical reasons (a factor analysis reproduced only two instead of three factors merging the personal and work-related burnout items to one factor), we created and used a combined single measure with one total score instead of three independent measures or subscales. This CBI score was calculated as the average of the scores on the items. The resulting 8-item measure with scores ranging from 0 to 78 showed a right-skewed distribution and a fairly good Cronbach’s Alpha of 0.79. A CBI score of 50 and above was considered to be indicative of an elevated number of burnout symptoms and, thus, an increased risk of having or developing burnout syndrome.
Confounding factors and control variables: Age and gender were used as control variables. Work-related factors such as time commitment to work, job status and job autonomy were used as potential confounding variables. Time commitment to work was measured by the weekly number of long hours with already consolidated response categories from 1 ‘No overtime’ to 5 ‘11 or more long hours per week’. Job autonomy as the only latent variable and multiple-item measure among these covariates was assessed by a selection of six questions (each with a response scale ranging from 0 ‘Never’ to 4 ‘Always’) about having influence over the amount of work to be done and especially about the freedom to decide if and when to take a break without permission, single days off at short notice or vacations. The 6-item measure consists of five items that were taken from two well-validated multiple-item scales of influence and the degree of freedom at work (e.g. “Do you have any influence on the amount of work assigned to you?”) of the Copenhagen Psychosocial Questionnaire (COPSOQ) [44], supplemented by an own formulated item (“Can you take days off at short notice?”). Cronbach’s alpha-coefficient of the 6-item scale was .66.
First, high risk groups with regard to frequent stress feelings and numerous burnout symptoms were explored by calculating the prevalence rates differentiated by divisions or rather professional groups as well as by levels of ERI and WLI and stratified by gender.
Then, bivariate correlation coefficients (Pearson’s r) between all relevant study variables (predictors, confounders, outcomes) were estimated in order to test the preconditions for confounding and mediation.
Subsequently, according to Baron and Kenny’s three step approach [45] for testing mediation with cross-sectional data several linear regression analyses were performed and multiple adjusted beta coefficients (β) were calculated in order to test the assumptions implied by the conceptual path model. At step one, the ERI and WLI measures as the two independent variables were initially included in the regression model for the prediction of stress and associations were additionally adjusted for the confounding and control variables. At step two, exactly the same was done for the burnout measure as the dependent or outcome variable. At step three, the stress indicator as the formerly dependent variable was first included as the only and then as an additional independent variable and a potential mediator in the regression model for the prediction of burnout. All three steps or regression models were first done with the overall measures (ERI ratio, WLI score) as independent variables and then replaced by their components or subscales (effort and reward scales, time- and strain-based work-to-life and life-to-work conflict subscales) in order to obtain more differentiated results.
Finally, stratified logistic regression analyses were done to explore possible differential associations of ERI and WLI with burnout between the different professional categories.
Preliminary analyses were conducted to shed some light on potential risk groups regarding ERI and WLI and especially regarding general stress perceptions and burnout symptoms. Nurses and particularly physicians were found to be “high risk” people with regard to burnout and compared to other hospital staffs, which is hardly surprising (see table 1). Physicians (not so nurses) also showed ERI and especially WLI at a frequency above or even far above average. The same applied to the technical care and emergency staff. Pronounced or frequent stress feelings were slightly more prevalent among physicians, nurses and medical-technical staff including therapists than among other hospital staffs.
| Table 1: Numbers and proportions of different levels of ERI, WLI, stress and burnout by professions/divisions. | ||||||||||||||
| Medical care | Nursing | Care technics / emergency service | Medical technics / therapy | Administration | Logistics | Total study population | ||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| Effort-reward imbalance (ERI ratio) | ||||||||||||||
| (Very) low (≤0.5) | 8 | 15.7 | 31 | 14.5 | 4 | 8.3 | 15 | 24.6 | 15 | 30.6 | 5 | 18.5 | 78 | 17.3 |
| Moderate (>0.5, ≤1.0) | 32 | 62.7 | 143 | 66.8 | 31 | 64.6 | 37 | 60.7 | 31 | 63.3 | 17 | 63.0 | 291 | 64.7 |
| (Very) high (>1.0) | 11 | 21.6 | 40 | 18.7 | 13 | 27.1 | 9 | 14.8 | 3 | 6.1 | 5 | 18.5 | 81 | 18.0 |
| Total | 51 | 214 | 48 | 61 | 49 | 27 | 450 | 100.0 | ||||||
| Work-life imbalance (WLI score) | ||||||||||||||
| (Very) low (0–7) | 8 | 15.1 | 47 | 20.7 | 10 | 19.6 | 24 | 38.7 | 19 | 37.3 | 8 | 21.6 | 116 | 24.1 |
| Moderate (8–15) | 25 | 47.2 | 136 | 59.9 | 30 | 58.8 | 24 | 38.7 | 28 | 54.9 | 21 | 56.8 | 264 | 54.9 |
| (Very) high (16–28) | 20 | 37.7 | 44 | 19.4 | 11 | 21.6 | 14 | 22.6 | 4 | 7.8 | 8 | 21.6 | 101 | 21.0 |
| Total | 53 | 227 | 51 | 62 | 51 | 37 | 481 | 100.0 | ||||||
| Stress feelings (frequency scale) | ||||||||||||||
| Never | 10 | 18.9 | 41 | 17.7 | 5 | 9.8 | 15 | 23.8 | 8 | 15.7 | 9 | 25.0 | 88 | 18.1 |
| Sometimes | 32 | 60.4 | 140 | 60.6 | 36 | 70.6 | 33 | 52.4 | 36 | 70.6 | 21 | 58.3 | 298 | 61.4 |
| (Very) often | 11 | 20.8 | 50 | 21.6 | 10 | 19.6 | 15 | 23.8 | 7 | 13.7 | 6 | 16.7 | 99 | 20.4 |
| Total | 53 | 231 | 51 | 63 | 51 | 36 | 485 | 100.0 | ||||||
| Burnout symptoms (CBI score) | ||||||||||||||
| Substandard (0– <25) | 9 | 17.0 | 37 | 16.1 | 6 | 12.0 | 16 | 26.2 | 16 | 45.7 | 13 | 48.1 | 97 | 21.3 |
| Averaged (25– <50) | 27 | 50.9 | 153 | 66.5 | 37 | 74.0 | 36 | 59.0 | 17 | 48.6 | 12 | 44.4 | 282 | 61.8 |
| Increased (50–100) | 17 | 32.1 | 40 | 17.4 | 7 | 14.0 | 9 | 14.8 | 2 | 5.7 | 2 | 7.4 | 77 | 16.9 |
| Total | 53 | 230 | 50 | 61 | 35 | 27 | 456 | 100.0 | ||||||
Further analyses showed a somewhat linear dose-response relationship between exposures and outcomes. The proportion of respondents reporting distinct stress feelings and showing an increased number of burnout symptoms increased gradually and substantially with cumulative degrees of ERI and WLI, thus indicating a clear gradient for both genders (see table 2). This gradient was more accentuated for WLI than for ERI. The same applied to women compared to men. One third to more than half of those men and women who scored relatively high on the consolidated WLI scale and one fifth to two fifths of all respondents with a comparatively high ERI ratio above 1 felt frequently stressed or were at increased risk of developing a burnout syndrome.
The steady increase of the prevalence rates with a cumulative ERI ratio supported the decision to use the ERI ratio as a continuous and not a dichotomous variable.
| Table 2: Gender-specific numbers of cases and prevalence rates of (very) frequent stress feelings and increased burnout symptoms by degree of effort-reward and work-life imbalance. | ||||||||||||
| Total study population | Study participants feeling stressed often to very often | Study participants with increased burnout symptoms (50–100) | ||||||||||
| Men | Women | Men | Women | Men | Women | |||||||
| n | % | n | % | n | %* | n | %* | n | %* | n | %* | |
| Effort-reward imbalance (ERI ratio) | ||||||||||||
| (Very) low (≤0.5) | 20 | 19.8 | 60 | 16.9 | 2 | 9.5 | 2 | 3.3 | 0.0 | 1 | 1.8 | |
| Moderate (>0.5, ≤1.0) | 64 | 63.4 | 231 | 65.3 | 11 | 18.0 | 48 | 20.8 | 11 | 19.0 | 31 | 14.1 |
| (Very) high (>1.0) | 17 | 16.8 | 63 | 17.8 | 4 | 20.0 | 26 | 41.3 | 5 | 29.4 | 26 | 41.9 |
| Total | 101 | 100.0 | 354 | 100.0 | 17 | 16.7 | 76 | 21.5 | 16 | 17.2 | 58 | 17.2 |
| Work-life imbalance (WLI score) | ||||||||||||
| (Very) low (0–7) | 21 | 19.3 | 98 | 25.9 | 2 | 9.5 | 8 | 8.2 | 0.0 | 3 | 3.3 | |
| Moderate (8–15) | 61 | 56.0 | 207 | 54.6 | 6 | 10.0 | 30 | 14.5 | 10 | 18.5 | 22 | 11.2 |
| (Very) high (16–28) | 27 | 24.8 | 74 | 19.5 | 9 | 33.3 | 42 | 56.8 | 6 | 25.0 | 37 | 50.7 |
| Total | 109 | 100.0 | 379 | 100.0 | 17 | 15.7 | 80 | 21.1 | 16 | 16.7 | 62 | 17.1 |
| * Proportion of employees feeling (very) often stressed or being at increased risk of burnout among those with the corresponding level of ERI and WLI. | ||||||||||||
The study variables turned out to be quite strongly correlated with one another, except for job status (see table 3). Strong inter-correlations were especially found between the two independent variables or predictors (ERI ratio, WLI score) on the one hand and the two dependent variables or outcomes (single-item stress scale, multiple-item burnout score) on the other, providing additional supportive evidence for the assumed associations and causal paths (see fig. 1).
Table 3 also confirms two of the three work-related variables (long hours, job autonomy) to be confounders, as they are significantly correlated with both the independent and the dependent variables, long hours being a risk factor and job autonomy being a resource or protective factor in this regard. Unexpectedly, job status did not emerge as a confounding factor and, thus, was not considered in subsequent multiple regression analyses.
As Pearson’s correlation coefficient equates the beta coefficient in a bivariate linear regression analysis, findings presented in Table 3 also support the three preconditions that have to be fulfilled for mediation according to Baron and Kenny [45].
| Table 3: Descriptive statistics and inter-correlations (r) between relevant study variables. | |||||||||||
| Values | Mean | SD | α | 1 | 2 | 3 | 4 | 5 | 6 | ||
| 1 | ERI ratio | 0.2–2.4 | 0.8 | 0.3 | – | ||||||
| 2 | WLI score | 0–28 (40) | 11.0 | 5.1 | 0.74 | 0.38*** | |||||
| 3 | General stress scale | 0–3 | 1.1 | 0.7 | – | 0.23*** | 0.38*** | ||||
| 4 | CBI score | 0–78 (100) | 35.1 | 14.0 | 0.79 | 0.43*** | 0.58*** | 0.50*** | |||
| 5 | Long hours (frequency) | 1–5 | 2.1 | 0.9 | – | 0.28*** | 0.20*** | 0.11* | 0.17*** | ||
| 6 | Job autonomy score | 0–24 | 9.9 | 4.2 | 0.66 | –0.26*** | –0.32*** | –0.16*** | –0.34*** | n.s. | |
| 7 | Job status (position) | 1–4 | 2.2 | 0.5 | – | n.s. | n.s. | n.s. | n.s. | 0.29*** | 0.25*** |
| *p ≤0.05; **p <0.01; ***p <0.001; n.s. = not significant (p >0.05); bold red framed = preconditions of confounding; grey shaded = preconditions of mediation | |||||||||||
WLI was found to be more strongly associated with stress and burnout than ERI when adjusting for each other and additionally for the confounding and control variables (see table 4). Initially (models 1, 3 and 6), as well as after replacement of the consolidated independent variables by their components or subscales (models 2, 4 and 7), the regression or beta coefficients were clearly higher for the WLI than for the ERI measure(s). These differentiated results suggested that the strain-based forms of WLI were solely responsible for the strong associations found between WLI and stress and burnout. In particular, strain-based work-to-life conflict emerged as the strongest explanatory or risk factor of stress (model 2) and burnout (models 4 and 7) by far. As regards the ERI components, findings also offered the effort scale being a much stronger correlate or predictor of stress and burnout than the reward scale which turned out not to be predictive at all.
Table 4 also shows that all conditions required for mediation are met according to Baron and Kenny [45] and their three-step approach: First, ERI and WLI were found to be significantly and positively associated with general psychological stress (step 1); second, ERI and WLI both turned out to be strongly and positively associated with burnout (step 2), and third (step 3), general psychological stress was also strongly associated with burnout (model 5), and associations or rather beta coefficients found in step 2 were reduced when the stress variable was additionally controlled (models 6 and 7). Since associations of ERI and WLI with burnout not completely disappeared but only partially (WLI) or very slightly (ERI) decreased when stress as the potential mediator variable was included and controlled in step 3, just partial and not perfect mediation was found.
All in all, 15% of the variation of the stress scale and a proportion of 52% of the variance of the burnout score (as the main outcome variable) were explained by the covariates considered and included in the fully adjusted and differentiated regression models (models 2 and 7).
| Table 4: Explaining general stress and burnout – results of stepwise multiple linear regression analyses. | |||||||
| Dependent or outcome variable(s) Stress scale (0–3) CBI score (0–78/100) | Step 1 (stress scale) | Step 2 (CBI score) | Step 3 (CBI score) | ||||
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | |
| β | β | β | β | β | β | β | |
| Independenta and interveningb variables | |||||||
| ERI ratioa (0.2–2.4) | 0.11* | – | 0.24*** | – | – | 0.21*** | – |
| Effort scale (score 5–25) | – | 0.11* | – | 0.21*** | – | – | 0.20*** |
| Reward scale (8–25) | – | n.s. | – | n.s. | – | – | n.s. |
| WLI total scorea (0–28/40) | 0.32*** | – | 0.43*** | – | – | 0.34*** | – |
| Time-based work-to-life conflict (0–12) | – | n.s. | – | n.s. | – | – | n.s. |
| Strain-based work-to-life conflict (0–8) | – | 0.23*** | – | 0.42*** | – | – | 0.36*** |
| Time-based life-to-work conflict (0–8) | – | n.s. | – | n.s. | – | – | n.s. |
| Strain-based life-to-work conflict (0–12) | – | 0.14** | – | 0.09* | – | – | n.s. |
| Stress scaleb (0–3) | – | – | – | – | 0.43*** | 0.30*** | 0.27*** |
| Confoundingc and control variables | |||||||
| Number of long hoursc (0–11+ h/week) | n.s. | n.s. | n.s. | n.s. | 0.11** | n.s. | n.s. |
| Job autonomy scorec (0–24) | n.s. | n.s. | –0.09* | n.s. | –0.23*** | –0.09* | n.s. |
| Sex (female) | n.s. | n.s. | n.s. | n.s. | n.s. | n.s. | n.s. |
| Age | n.s. | n.s. | n.s. | –0.11** | –0.11** | n.s. | –0.11** |
| Adjusted R square | 0.144 | 0.154 | 0.383 | 0.459 | 0.311 | 0.457 | 0.518 |
| Number of cases in model | 425 | 425 | 403 | 403 | 435 | 403 | 403 |
| *p ≤0.05; **p <0.01; ***p <0.001; n.s. = not significant (p >0.05); bold red framed = preconditions of confounding; grey shaded = preconditions of mediation | |||||||
Across the whole study population, the risk of facing an increased burnout symptomatology was more than four times higher in those with an effort-reward imbalance and more than five times higher in those with a (very) high work-life imbalance compared to the less exposed among the hospital staff (see table 5). But stratified logistic regression analyses revealed that odds ratios (as measures of association and proxies for the relative risk) varied quite a lot between the different occupational groups. And WLI, not throughout, turned out as the stronger risk factor of burnout than ERI. In physicians, therapists and medical-technical personnel (among which high WLI was most prevalent) the adjusted odds ratio proved to be much higher for ERI than for WLI, whereas among nursing, technical care and emergency staffs and also among the administrative and logistic personnel the exact opposite was found.
| Table 5: Associations between both imbalance measures and increased burnout symptoms (CBI score ≥50) among different professional categories. | ||||||
| Medical care (physicians) | Nursing | Care technics and emergency service | Medical technics and therapy | Administration and logistics | Total study population | |
| ORa | ORa | ORa | ORa | ORa | ORa | |
| Effort-reward imbalance (ERI ratio) | ||||||
| No (≤1.0) | 1 | 1 | 1 | 1 | 1 | 1 |
| Yes (>1.0) | 22.55** | 3.77** | 1.68 | 39.53* | 2.98 | 4.57*** |
| Work-life imbalance (WLI score) | ||||||
| Very low to moderate (0–15) | 1 | 1 | 1 | 1 | 1 | 1 |
| High to very high (16–28) | 1.80 | 9.64*** | 92.03* | 1.91 | 8.55 | 5.30*** |
| No. of cases in model | 51 | 205 | 47 | 55 | 52 | 417 |
| * p ≤0.05; ** p <0.01; *** p <0.001; aadjusted for one another and additionally for age, gender, and occupational status. | ||||||
The main aim of the present study was to explore in a hospital setting in Switzerland whether ERI or WLI is more strongly associated with general psychological stress and burnout. An additional aim was to examine whether such imbalances and health impairments are more prevalent in medical care and nursing staffs than in other hospital staffs, and whether ERI or WLI are associated with stress and burnout to varying degrees in different professional categories.
Nurses and particularly physicians as expected and assumed for such “helping” professionals who do physically, temporally and/or emotionally demanding “people work”, turned out to be most affected by an increased risk of burnout, and at least physicians were also highly or even most exposed to ERI and WLI. In addition, evidence was found for a clear gradient in the relationships between ERI and WLI on the one hand and stress and burnout on the other, i.e. gradually increasing proportions of hospital staffs who feel (very) frequently stressed and show increased burnout symptoms with increasing degrees of ERI and WLI.
Bi- and multivariate statistical analyses then revealed significant and partly very strong correlations as well as multiple adjusted regression coefficients for the ERI and WLI measures in relation to the outcome measures, namely the single-item stress scale as well as the multiple-item burnout score. The findings supported both the direct and indirect causal paths implied by the underlying conceptual path model. In sum and for the entire study population, WLI was much more strongly associated with general psychological stress (β = 0.32) and, contrary to expectations, also with burnout (β = 0.43) than ERI (β = 0.11 and 0.24), when controlled for one another and additional covariates. However, ERI was also found to be a relevant and independent explanatory or risk factor of general psychological stress and burnout. Replacing the consolidated WLI score by its four subscales and the ERI ratio by its two components revealed differentiated and illuminating results which showed that associations of ERI and WLI with general stress and burnout can be attributed largely to the effort component of the ERI measure and the strain-based forms of both directions of the WLI measure.
Beyond that and according to Baron and Kenny’s three step approach for testing mediation with cross-sectional data, the results suggested that general psychological stress plays a mediating but not very significant role in the relationship between WLI or ERI and burnout, as it emerged as a strong correlate or risk factor by itself, and its inclusion in the regression model slightly to fairly reduced the effects or measures of association (beta coefficients) of the two explanatory or independent variables, ERI and WLI. That means that the relationships between ERI and burnout and particularly between WLI and burnout were found to be only partly and not fully mediated by stress.
Finally, stratified analyses revealed different associations between the two imbalance measures and burnout for different professional categories. In physicians, therapists and medical-technical personnel in contrast to nursing and other hospital staff, ERI turned out to be the much stronger risk factor for burnout than WLI. For physicians, medical-technical professionals and therapists, thus, conditions of high efforts (e.g., much time spent at work) combined with low rewards at work seem to be more stressful and exhausting than a demanding job or work hours that are poorly compatible with one’s personal or family life. Particularly for physicians such work-life imbalance may be better accepted as an integral part of the job unlike an insufficiently rewarded job.
The fact that some of the strong associations or high OR almost consistently found in these stratified analyses and across all occupational groups showed quite large confidence intervals (not shown in Table 5) and either were not significant or turned out to be exceptionally high is most likely caused by small numbers of cases. The fairly strong and highly significant associations and not too large confidence intervals found in the total sample at least point to such conclusion. The results of the stratified analyses therefore have to be interpreted with caution. This needs to be considered but does not necessarily argue against the given and plausible interpretation of this differential finding.
In sum and at least for the study sample, an increased risk of burnout seems to be largely explained (statistically spoken to a proportion of around 50%) by conditions and perceptions of ERI and WLI and, in addition and independent of such imbalances, by general stress feelings that, in turn, are partly resulting from work-related stressors like these.
As noted at the beginning and to our knowledge, no single study has been published that compared and combined the two constructs ERI and WLI (or WFC) with regard to the prediction of general psychological stress and burnout. Consequently, there are no findings from other studies so far to be compared to the main finding of our study. However, at least partial results are comparable and consistent with other studies that found, for example, that the work-to-family conflict was a stronger stress or burnout correlate than the inversely directed family-to-work conflict [12, 28]. In a study performed by Montgomery et al. [32], work-family interference was found to be very strongly associated with emotional exhaustion (β = 0.61), supporting our finding of a similarly strong unadjusted association or bivariate correlation between WLI and burnout (r = 0.58). But like most of all other previous studies that have found strong evidence for an association between WLI or rather WFC and burnout or fatigue [3, 15, 31, 33–35], the study of Montgomery and colleagues did not differentiate between the time- and strain-based forms of WFC and accordingly did not investigate both forms in relation to burnout.
In support of another of our findings Schulz et al. [25] found the effort scale to be more strongly associated with emotional exhaustion as the major component of burnout than the reward scale. But apart from that they also found stronger associations between the effort and reward scales on the one hand and emotional exhaustion on the other (β = 0.32/–0.22) than we did in the present study after or rather due to adjustment for WLI and different work-related confounders (β = 0.21/n.s.). However, not reported results of a corresponding analysis suggest that the effect sizes of the two ERI scales on burnout would have been comparably strong and similarly different in the absence of additional controls such as WLI, job autonomy and number of long hours (β = 0.45/–0.14).
This study provides first and initial evidence for a differential and independent prediction of general psychological stress and burnout by two identified work-related stressors and established concepts of imbalance that have not been investigated conjointly so far, even less differentiated by their subcomponents or dimensions, stratified for and compared among different professional categories in a hospital setting in Switzerland. Besides these strengths, the study has some methodological limitations and shortcomings too.
First, causal inferences and conclusions about the causal directions underlying the results cannot actually be drawn due to the cross-sectional design of the study. Although we tested our mediational path model by estimating a series of linear regression models following Baron and Kenny’s approved three-step approach to test for mediation with cross-sectional data [45], we could only study and conclude association and not causation. This points to the value and need for longitudinal studies.
Second, a common-method bias and/or a measurement artefact due to the use of single-source self-reported survey data or as a result of reciprocal causality cannot be excluded entirely. The differential associations found for the different professional categories argue against the observed strong association between WLI and burnout being a measurement artefact. In addition, this particular finding is fully in line with the research literature (see Allen et al. [27] for a systematic and comprehensive review of the WFC literature) that found the significant and strong relationship between WFC and burnout to be one of the best investigated and most consistent and strongest findings at all – nota bene without raising any doubts with regard to common-method variance, overlap of measures or conceptual redundancy.
Third, with a view to feasibility in a large field study shortened and/or slightly adapted, supplemented or less common versions of the original instruments, or in the case of stress a validated single-item measure in place of a multiple-item measure, were used as measures of the main and mostly multidimensional concepts. However, even though poor measures were assumed, this would result in a non-differential misclassification with regard to exposure and outcome and consequently produce a bias towards an underestimation of the correct or “true” association or effect measure without calling the findings into question.
Fourth, given the rather poor return or response rates and the small number of cases in some of the studied occupational groups, we must be cautious in generalising the findings. Although there is no indication of a selection bias among the randomly selected study participants, findings relating to certain professional categories or to prevalence rates of ERI, WLI, stress, and burnout cannot be transferred to others beyond the study sample.
This is the first study (not only for Switzerland) to have examined the ERI model in conjunction with the WLI or WLC construct and used to explain or predict general psychological stress and burnout. Among hospital staffs WLI was found to make a remarkable contribution to the prediction of both general psychological stress and burnout, in excess of the ERI model, which nevertheless also turned out to be predictive in this regard. This indicates at least for some occupational groups like nurses that general psychological stress and burnout cannot be attributed predominantly to making high efforts at work that are inappropriate and disproportional to the low rewards received and therefore to stress at work in a narrow and traditional sense. In fact, general psychological stress and burnout seem to result even more from high but not time-related job demands and work strains that are poorly compatible with family and other life activities and commitments (strain-based work-to-life conflict).
The study results have implications for future research and, if confirmed by other studies, also for business practice, and workplace health promotion. Since no other comparable study has been conducted so far, our main finding that WLI is more strongly associated with general psychological stress and burnout than ERI except for physicians, therapists and medical-technical staff for whom the opposite was found, currently stands alone and has first to be validated and replicated by subsequent cross-sectional and longitudinal studies before it can be generalised and transferred to the entire professions or other populations. In this process, special attention should be given to the study samples and the measures of ERI, WLI, stress, and burnout. Further studies using longitudinal data, larger study samples representing the general working population, and complete or alternative measurement scales are needed in order to provide additional evidence in support of our main finding. In addition, future research should distinct consistently between the time- and strain-based forms and both directions of work-life conflict or imbalance and take their differential associations with burnout into consideration.
Beyond that, both ERI and WLI seem to play an important and complementary role for general psychological stress and burnout and do so independently of one another. However, strain-based role conflicts, particularly those affecting the non-work domain and interfering with private life activities and commitments (work-to-life conflict), turned out to be even more stressful and exhausting than insufficiently rewarded high efforts put into work. Thus, companies and health promoters are well advised to take both sources or risk factors of stress and burnout into account when planning intervention strategies in order to ameliorate conditions at work for the prevention of stress and burnout.
1 Maslach C, Jackson SE. The measurement of experienced burnout. J Occup Behav. 1981;2:99–113.
2 Maslach C, Leiter MP. Early predictors of job burnout and engagement. J Appl Psychol. 2008;93(3):498–512.
3 Innstrand ST, Langballe EM, Espens GA, Falkum E, Aasland OG. Positive and negative work-family interaction and burnout: A longitudinal study of reciprocal relations. Work & Stress. 2008;22(1):1–15.
4 Ahola K, Toppinen-Tanner S, Huuhtanen P, A. K, Väänänen A. Occupational burnout and chronic work disability: An eight-year cohort study on pensioning among Finnish forest industry workers. J Affect Disorders. 2008;115(1–2):150–9.
5 Kristensen TS, Borritz M, Villadsen E, Christensen KB. The Copenhagen burnout inventory: A new tool for the assessment of burnout. Work & Stress. 2005;19(3):192–207.
6 Shirom A. Burnout in work organizations. In: Cooper CL, Robertson IT, eds. International Review of Industrial and Organizational Psychology. New York: John Wiley & Sons; 1989: 25–48.
7 Schaufeli WB, Greenglass ER. Introduction to special issue on burnout and health. Psychol Health. 2001;16(5):501–10.
8 Peltzer K, Mashego T-A, Mabeba M. Short Communication: Occupational stress and burnout among South African medical practitioners. Stress Health. 2003;19:275–80.
9 Karasek R, Theorell T. Healthy work: stress, productivity, and the reconstruction of working life. New York: Basic Books, 1990.
10 Siegrist J. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol. 1996;1:27–41.
11 Greenhaus JH, Beutell NJ. Sources of conflict between work and family roles. Acad Manage Rev. 1985;10(1):76–88.
12 Netemeyer RG, Boles JS, McMurrian R. Development and validation of work-family conflict and family-work conflict scales. J Appl Psychol. 1996;81(4):400–10.
13 Carlson DS, Kacmar KM, Williams LJ. Construction and initial validation of a multidimensional measure of work-family conflict. J Vocat Behav. 2000;56(2):249–76.
14 Gutek B, Searle S, Klepa L. Rational versus gender role explanations for work-family conflict. J Appl Psychol. 1991;76(4):560–8.
15 Hämmig O, Gutzwiller F, Bauer GF. Work-life conflict and associations with work- and nonwork-related factors and physical and mental health outcomes: a nationally representative cross-sectional study in Switzerland. BMC Public Health. 2009;9:435.
16 Calnan M, Wadsworth E, May M, Smith A, Wainwright D. Job strain, effort-reward imbalance, and stress at work: competing or complementary models? Scand J Public Health. 2004;32(2):84–93.
17 de Jonge J, Bosma H, Peter R, Siegrist J. Job strain, effort-reward imbalance and employee well-being: a large-scale cross-sectional study. Soc Sci Med. 2000;50:1317–27.
18 Weyers S, Peter R, Boggild H, Jeppesen HJ, Siegrist J. Psychosocial work stress is associated with poor self-rated health in Danish nurses: a test of the effort-reward imbalance model. Scand J Caring Sci. 2006;20:26–34.
19 Buddeberg-Fischer B, Stamm M, Buddeberg C, Bauer G, Hämmig O, Klaghofer R. Work stress, health and satisfaction of life in young doctors: results of a longitudinal study in Switzerland. Deut Med Wochenschr. 2008;133:2441–7.
20 Sakata Y, Wada K, Tsutsumi A, Ishikawa H, Aratake Y, Watanabe M, et al. Effort-Reward Imbalance and Depression in Japanese Medical Residents. J Occup Health. 2008;50:498–504.
21 Tsutsumi A, Kayaba K, Theorell T, Siegrist J. Association between job stress and depression among Japanese employees threatened by job loss in a comparison two complementary job-stress models. Scand J Work Env Hea. 2001;27(2):146–53.
22 Tsutsumi A, Kawanami S, Horie S. Effort-reward imbalance and depression among private practice physicians. Int Arch Occ Env Hea. 2011; Epub ahead of print.
23 Bakker AA, Killmer CH, Siegrist J, Schaufeli WB. Effort-reward imbalance and burnout among nurses. J Adv Nurs. 2000;31:884–91.
24 Klein J, Grosse Frie K, Blum K, Siegrist J, von dem Knesebeck O. Effort-reward imbalance, job strain and burnout among clinicians in surgery. Psychother Psych Med. 2010;60:374–9.
25 Schulz M, Damkröger A, Heins C, Wehlitz L, Löhr M, Driessen M, et al. Effort-reward imbalance and burnout among German nurses in medical compared with psychiatric hospital settings. J Psychiat Ment Hea Nurs. 2009;16:225–33.
26 Unterbrink T, Hack A, Pfeifer R, Buhl-Griesshaber V, Müller U, Wesche H, et al. Burnout and effort – reward-imbalance in a sample of 949 German teachers. Int Arch Occ Env Hea. 2007;80:433–41.
27 Allen TD, Herst DEL, Bruck CS, Sutton M. Consequences associated with work-to-family conflict: A review and agenda for future research. J Occup Health Psychol. 2000;5(2):278–308.
28 Hammer TH, Saksvik PO, Nytro K, Torvatn H, Bayazit M. Expanding the psychosocial work environment: Workplace norms and work-family conflict as correlates of stress and health. J Occup Health Psychol. 2004;9(1):83–97.
29 Smith Major V, Klein KJ, Ehrhart MG. Work time, work interference with family, and psychological distress. J Appl Psychol. 2002;87(3):427–36.
30 Burke RJ, Greenglass ER. Hospital restructuring, work-family conflict and psychological burnout among nursing staff. Psychol Health. 2001;16:583–94.
31 Brauchli R, Bauer GF, Hämmig O. Relationship between time-based work-life conflict and burnout: A cross-sectional study among employees in four large-scale Swiss enterprises. Swiss J Psychol. 2011;70(3):165–73.
32 Montgomery AJ, Panagopolou E, Benos A. Work-family interference as a mediator between job demands and job burnout among doctors. Stress Health. 2006;22:203–12.
33 Demerouti E, Bakker AB, Bulters AJ. The loss spiral of work pressure, work-home interference and exhaustion: Reciprocal relations in a three-wave study. J Vocat Behav. 2004;64(1):131–49.
34 Hämmig O, Bauer GF. Work-life imbalance and mental health among male and female employees in Switzerland. Int J Public Health. 2009;54:88–95.
35 Jansen NWH, Kant I, Kristensen TS, Nijhuis FJN. Antecedents and consequences of work-family conflict: A prospective cohort study. J Occup Environ Med. 2003;45(5):479–91.
36 Franche R-L, Williams A, Ibrahim S, Grace SL, Mustard C, Minore B, et al. Path analysis of work conditions and work-family spillover as modifiable workplace factors associated with depressive symptomatology. Stress Health. 2006;22:91–103.
37 Kinman G, Jones F. Effort-reward imbalance, over-commitment and work-life conflict: testing an expanded model. J Manage Psychol. 2008;23(3):236–51.
38 Willis TA, O’Connor DB, Smith L. Investigating effort-reward imbalance and work-family conflict in relation to morningness-eveningness and shift work. Work & Stress. 2008;22(2):125–37.
39 Knecht M, Bauer GF, Klaghofer R, Buddeberg-Fischer B, Stamm M, Hämmig O. Work-life conflict and health among Swiss physicians – in comparison with other university graduates and with the general Swiss working population. Swiss Med Weekly. 2010;140:w13063.
40 Siegrist J, Peter R. Measuring effort-reward imbalance at work: Guidelines. Düsseldorf: University of Düsseldorf, 1996.
41 Niedhammer I, Tek M-L, Starke D, Siegrist J. Effort-reward imbalance model and self-reported health: cross-sectional and prospective findings from the GAZEL cohort. Soc Sci Med. 2004;58(8):1531–41.
42 Elo A-L, Leppänen A, Jahkola A. Validity of a single-item measure of stress symptoms. Scand J Work Env Hea. 2003;29(6):444–51.
43 Schaufeli WB, Leiter MP, Maslach C, Jackson SE. The Maslach Burnout Inventory – General Survey (MBI-GS). In: Maslach C, Jackson SE, Leiter MP, eds. Maslach burnout inventory manual. Palo Alto: Consulting Psychologists Press; 1996:19–26.
44 Kristensen TS, Hannerz H, Høgh A, Borg V. The Copenhagen Psychosocial Questionnaire – a tool for the assessment and improvement of the psychosocial work environment. Scand J Work Env Hea. 2005;34(6):438–49.
45 Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–82.
Funding / potential competing interests: The study was financially supported by the Progrès Foundation of the Swiss National Accident Insurance Fund (Suva). Grant was given without any conditions. There are no competing interests.