Figure 1
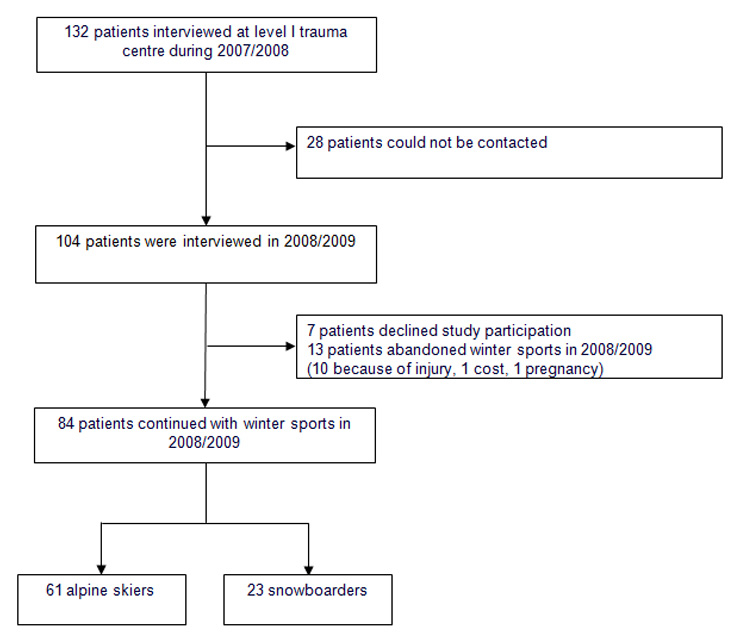
Flow chart of study patients.
DOI: https://doi.org/10.4414/smw.2011.13283
During a single skiing season throughout Switzerland, around 1000 alpine skiers and snowboarders per day present with injuries serious enough to require medical treatment [1]. Some are minor, but others are associated with increased morbidity and mortality [2–5]. Head and spinal trauma are among the most devastating injuries and can cause costs for the individual and the community [2, 7, 8]. Insurance companies therefore regularly launch large injury prevention campaigns [1, 6].
Our prior research has focused on risk factors in alpine skiing and snowboarding, and found a trend towards lower helmet wearing rates in injured snowboarders [3–5]. Very little is known, however, about the way injuries influence subsequent behaviour. For example, do these patients continue skiing or snowboarding in the next season, and are they more likely to wear protective clothing? Such findings may provide important information for prevention and intervention campaigns.
We therefore investigated the association between ski and snowboard injuries and changes in the use of protective equipment in the subsequent season.
This study compared protective clothing wearing rates amongst injured alpine skiers and snowboarders in the 2007/2008 and 2008/2009 seasons. All injured adult (≥16 years) alpine skiers and snowboarders who were admitted to a level I trauma centre during the 2007/2008 skiing season were eligible to participate and were interviewed about wearing protective equipment (e.g., helmet and back protectors) on the slopes [3, 4]. Patients were excluded who were not able to be contacted by phone in 2008/2009 after three attempts or who did not agree to take part in the study.
During the 2007/2008 season, patients injured when alpine skiing or snowboarding had been interviewed on admission to the emergency department or during their hospital stay, using a standardised questionnaire about behaviour on the slopes [3, 4]. Patients were excluded if they were severely intoxicated or had suffered intracranial bleeding, skull fractures, or persistent retrograde amnesia, or exhibited a Glasgow Coma Score (GCS) <14. Patients with concussion were included if their GCS was 15 and they were able to fully and coherently understand and answer the questions. The questionnaire was available in English, French and German.
The same patients were contacted by phone by a trained medical student at the end of April 2008/2009 and were re-interviewed about wearing protective equipment. Participation in the study was voluntary and anonymous, and confidentiality was guaranteed. Data were collected, stored, analysed and shared according to the ethics committee standards of the Inselspital Bern. The injury severity score (ISS) was calculated for all patients, using the 2008 Abbreviated Injury Scale [9]. The primary outcome was the difference in protective equipment wearing rates between the two seasons.
The data were analysed in two steps. Firstly, McNemar tests were used to determine overall differences in protective clothing wearing rates between the two seasons. Secondly, the study attempted to identify participants who had not worn protective clothing before their injury. Multiple logistic regressions, with age, gender and ISS as predictors, were used to compare findings in those who started wearing protective equipment after injury and those who did not [9].
As shown in figure 1, 132 patients (92 alpine skiers, 40 snowboarders) were interviewed during the 2007/2008 season. A total of 28 patients were no longer able to be contacted at the address provided, leaving 104 patients (76 alpine skiers, 28 snowboarders) to be interviewed for the 2008/2009 season, 7 of whom declined. A total of 10 skiers and one snowboarder had abandoned winter sports due to their injury, and 2 snowboarders had quit snowboarding for other reasons (pregnancy, costs of winter sports).
Figure 1
Flow chart of study patients.
We therefore had a sample of 84 patients who had continued with winter sports in the 2008/2009 season, of whom 61 were alpine skiers and 23 were snowboarders. The patients had a median age of 39 years (interquartile range [IQR] 27.00–48.50), and 59 (70.2%) were male. The median ISS was 4 (range 1–29). A breakdown of patients included in the study is shown in table 1. The distribution of injured body regions and the injury severity are shown in table 2.
Table 3 summarises the changes in protective equipment wearing rates between the two seasons. After sustaining an injury, 32 patients (22 alpine skiers and 10 snowboarders) started to wear a helmet and 8 patients (5 alpine skiers and 3 snowboarders) started to wear a back protector (table 3). None of the patients who had worn a helmet or back protector prior to injury abandoned wearing these after the injury. In contrast, total numbers of patients wearing knee and wrist protectors dropped from 6.0% to 4.8% and from 13.1% to 11.9%, respectively, after sustaining an injury (table 3). Overall, helmet and back protector wearing rates increased from 40.5% to 78.6% and 14.3% to 23.8% respectively. The helmet wearing rate more than doubled in snowboarders (from 39.1% to 82.6%, p = 0.002). The back protector wearing rate more than doubled in alpine skiers, although this difference was not statistically significant (from 6.6% to 14.8%, p = 0.063). The changes found for knee or wrist protectors, which were worn by only a minority of patients in the present study, were not statistically significant (table 3).
As shown in table 4, younger injured alpine skiers decided to wear back protectors more often in the subsequent season than older skiers. There was no significant age effect in injured snowboarders. No difference was observed for gender or ISS in injured alpine skiers or snowboarders who started wearing a helmet or back protector in the subsequent season.
| Table 1: Demographics (n = 84). | |||
| Kind of winter sport (n [%]) | Age median (range) | Male n (%) | ISS median (range) |
| Alpine skiers: 61 (72.6) Snowboarders: 23 (27.3) | 44 (18–81) 28 (19–47) | 39 (63.9) 20 (87.0) | 4 (1–24) 4 (1–29) |
| Total | 39 (18–81) | 59 (70.2) | 4 (1–29) |
| Table 2: Injured body regions of included patients (n = 84). | ||||
| Body region* | Alpine skiers (n [%]) | AIS** (median [IQR]) | Snowboarders (n [%]) | AIS (median [IQR]) |
| Head | 10 (16.4) | Concussion only | 5 (21.7) | Concussion only |
| Face | 7 (11.5) | 2 (1.75–2.00) | 4 (17.4) | 2 (2.00–2.00) |
| Chest | 6 (9.8) | 1 (1.00–2.00) | 3 (13.0) | 1 (1.00–2.00) |
| Abdomen | 1 (1.6) | 2 (2.00–2.00) | 0 (0) | |
| Pelvis | 7 (11.5) | 2 (1.50–4.00) | 2 (8.7) | 1 (1.00–1.00) |
| Spine | 8 (13.1) | 2 (1.00–2.00) | 4 (17.4) | 2 (1.00–2.00) |
| Upper extremities | 21 (34.4) | 2 (1.00–2.00) | 7 (30.4) | 2 (1.00–2.00) |
| Lower extremities | 15 (24.6) | 2 (1.00–2.00) | 5 (21.7) | 1.5 (1.00–2.00) |
| * Multiple entries possible, ** Abbreviated injury scale | ||||
| Table 3: Comparison of protective equipment wearing rates between the 2007/2008 and 2008/2009 seasons (n = 84). | |||
| Type of protective equipment | 2007/2008 (n [%]) | 2008/2009 (n [%]) | p-value |
| Helmet | 34 (40.5) | 66 (78.6) | <0.001 |
| Alpine skiers Snowboarders | 25 (41.0) 9 (39.1) | 47 (77.0) 19 (82.6) | <0.001 0.002 |
| Back protector | 12 (14.3) | 20 (23.8) | 0.021 |
| Alpine skiers Snowboarders | 4 (6.6) 8 (34.8) | 9 (14.8) 11 (47.8) | 0.063 0.380 |
| Knee protector | 5 (6.0) | 4 (4.8) | 1.000 |
| Alpine skiers Snowboarders | 2 (3.3) 3 (13.0) | 2 (3.3) 2 (8.7) | n.a. 1.000 |
| Wrist protector | 11 (13.1) | 10 (11.9) | 1.000 |
| Alpine skiers Snowboarders | 2 (3.3) 9 (39.1) | 3 (4.9) 7 (30.4) | 1.000 0.690 |
| *not available | |||
| Table 4: Association with age, gender and severity of injury. | |||
| Change 2007/2008 to 2008/2009 | Age (mean group 0 and 1 / p-value) | Gender (OR [female/male] / 95% CI / p-value) | ISS (mean group 0 and 1 / p-value) |
| Wearing a helmet | 43.4, 39.0 / 0.292 | 1.17 / 0.30–4.6 / 0.825 | 6.0, 3.2 / 0.120 |
| Alpine skiers Snowboarders | 48.1, 43.5 / 0.095 27.0, 29.0 / 0.600 | 2.0 / 0.73–5.3/ 0.180 1.17 / 0.30–4.6 / 0.825 | 5.1, 3.1 / 0.370 9.0, 3.3 / 0.280 |
| Wearing a back protector | 41.7, 32.4 / 0.076 | 0.0 / 0-Inf / 0.71 | 5.1, 2.2 / 0.176 |
| Alpine skiers Snowboarders | 44.6, 30.2 / 0.043 27.9, 35.3 / 0.145 | 0.0 / 0-Inf / 0.76 0.0 / 0-Inf / 0.83 | 5.0, 2.0 / 0.239 5.4, 2.5 / 0.556 |
In our study, helmet wearing rates doubled in snowboarders and back protector wearing rates doubled in alpine skiers after injury. Younger alpine skiers decided to wear back protectors more often after sustaining an injury than older alpine skiers. Protective gear was worn more frequently by snowboarders than by alpine skiers.
Participation in interviews for both seasons (2007/2008 and 2008/2009) was voluntary. In the first season, we had excluded patients who were unconscious, heavily intoxicated, or suffered life-threatening injuries, which did introduce a certain selection bias. For practical reasons, for the present study, only patients interviewed at our level I trauma centre in 2007/2008 were re-interviewed about the subsequent season (patients had also been interviewed at two regional hospitals in the 2007/2008 season). Our results are based on self-reported data, and it is possible that some participants use protective equipment less regularly than others, and that some people over-reported protector wearing rates. Small differences between these data at the two time points are possible. Unfortunately, our database did not collect data on the duration of injury-related constraints, which might differ widely between individuals, or multi-morbidity, which is strongly correlated to the patients’ age. The median age of our study population was 39 year, with interquartile ranges from 27.0–48.5, indicating that most of our study population was unlikely to suffer from multi-morbidity.
A population-based survey on non-injured alpine skiers and snowboarders, conducted by the Swiss Council for Accident Prevention (BfU) in the same periods as our study, showed only a small increase in helmet wearing rates from 55% to 63% in alpine skiers and from 70% to 71% in snowboarders [10]. In this survey, the rate of wearing back protectors increased from 6% to 13% in alpine skiers and decreased from 41% to 38% in snowboarders [11]. Further studies on the effect of wearing protective equipment after an injury in winter sports should include case-control studies comparing the attitudes to wearing protective clothing in injured and non-injured alpine skiers and snowboarders over several skiing seasons.
There is growing evidence that wearing a helmet protects skiers and snowboarders from head injuries [12, 13]. Despite the inherent risks of not wearing protective equipment, helmets are not mandatory on ski slopes in Switzerland. Many skiers and snowboarders might regard them as an encumbrance. However, some countries, notably Italy, Croatia and Austria, have made helmet use for children compulsory [7]. Empirical studies have so far provided less robust evidence that back protectors prevent spinal injuries [14].
Similarly to prior publications, this study showed that snowboarders wear protective equipment more frequently than alpine skiers [3, 4]. This might be due to the younger median age of snowboarders (28 years vs. 44 years). Furthermore, we observed that younger alpine skiers changed to wearing protective equipment after injury more often than older alpine skiers. Therefore, a possible strategy to encourage helmet wearing and change attitudes towards protective equipment might be via advertisements aimed at young adults, for example by involving persons with a social impact promoting the benefits and ‘coolness’ of protection. Similar approaches have been used successfully for HIV, tobacco and car-injury prevention campaigns [15]. The evidence is even less clear on the human factors which may influence the decision to buy protective devices. In one of the few studies published, Jung et al. observed that neurosurgeons in Austria who have treated patients with head injuries were more likely to wear helmets themselves than a control group of surgeons who had not treated head trauma patients [7].
It is evident that a broad range of psychological processes have to be involved in research into such complex judgement- and decision-making processes as choosing whether to wear protective equipment when skiing [16]. In addition to conscious processes, subconscious processes may play an important part, and affective processes may be just as important as cognitive processes, such as weighing up the risks and benefits of helmet use. A further factor involved is unrealistic optimism, which may be broader and more pronounced in some individuals than the perceived risk of sustaining an injury without protection [17]. Research into long-term behaviour in the use of protective equipment, specifically whether its use is maintained, increases or decreases, will also be necessary for the efficient design of informational programmes to encourage its use.
Injuries could be a trigger for skiers and snowboarders to start wearing protective equipment, such as helmets and back protectors. This might be especially true for young adults. Those who do not yet use protective equipment may be convinced to do so by high-profile media campaigns, including reports from ski or snowboard injury survivors, rather than by ‘textbook advice’. The psychological processes influencing the use of protective equipment require further investigation.
Characteristics of patients with injuries from winter sports in the season 2007/2008 who had abandoned winter sports in the season 2008/2009.
| Snowboarders | |||||
| Age | Gender | Reason | Injured body region | AIS | Type of protection |
| 44 | F | Pregnancy | Head | 1 | Helmet |
| 32 | M | Price of ski ticket | Lower extremity | 1 | Wrist protector |
| 33 | M | Injury | Upper extremity | 2 | Helmet |
| Alpine skiers | |||||
| Age | Gender | Reason | Injured body region | AIS | Type of protection |
| 72 | M | Injury | Lower extremity | 3 | None |
| 44 | F | Injury | Lower extremity | 2 | None |
| 63 | F | Injury | Upper extremity | 2 | None |
| 63 | M | Injury | Lower extremity | 2 | None |
| 54 | F | Injury | Lower extremity | 1 | None |
| 24 | F | Injury | Head, lower extremity | 1 | None |
| 73 | M | Injury | Lower extremity | 1 | None |
| 34 | M | Injury | Lower extremity | 1 | None |
| 31 | M | Injury | Lower extremity | 2 | None |
| 33 | F | Injury | Lower extremity | 1 | None |
Acknowledgments:Mrs Kathrin Dopke MPH, study coordinator, Department of Emergency Medicine, Inselspital, University Hospital Bern, Switzerland. Mr Alistair Reeves, BA (Hons) ELS, for editing the English. Mr Urs Simmen, Msc PhD, Schötzau & Simmen, Statistische Beratung, Basel, Switzerland, for statistical consulting.
1 bfu. [ http://www.bfu.ch ] Bern: Swiss Council for Accident Prevention. [updated 2011 Jul 4; cited 2011 Jul 4]. Available from: http://www.bfu.ch/German/medien/Seiten/2007_11_22.aspx
2 Franz T, Hasler RM, Benneker L, Zimmermann H, Siebenrock KA, Exadaktylos AK. Severe spinal injuries in alpine skiing and snowboarding: a 6-year review of a tertiary trauma centre for the Bernese Alps ski resorts, Switzerland. Br J Sports Med. 2008;42(1):55–8.
3 Hasler RM, Dubler S, Benneker LM, Berov S, Spycher J, Heim D, et al. Are there risk factors in alpine skiing? A controlled multicentre survey of 1278 skiers. Br J Sports Med. 2009;43(13):1020–5.
4 Hasler RM, Berov S, Benneker L, Dubler S, Spycher J, Heim D, et al. Are there risk factors for snowboard injuries? A case-control multicentre study of 559 snowboarders. Br J Sports Med. 2010;44(11):816–21.
5 bfu. [ http://www.bfu.ch ] Bern: Swiss Council for Accident Prevention. [updated 2011 Jul 4; cited 2011 Jul 4]. Available from: http://www.bfu.ch/English/statistik/Pages/Statistik.aspx
6 http://www.suva.ch/home/suvaliv/kampagnen/check_the_risk_uebersicht.htm (last accessed 14/03/2011)
7 Jung CS, Zweckberger K, Schick U, Unterberg AW. Helmet use in winter sport activities-attitude and opinion of neurosurgeons and non-traumatic-brain-injury-educated persons. Acta Neurochir (Wien). 2011;153(1):101–6.
8 Von Elm E, Osterwalder JJ, Graber C, Schoettker P, Stocker R, Zangger P, et al. Severe traumatic brain injury in Switzerland - feasibility and first results of a cohort study. Swiss Med Wkly. 2008;138(23-24):327–34.
9 Committee on Injury Scaling, Association for the Advancement of Automotive Medicine (AAAM). The abbreviated injury scale 2008 revision. Des Plaines, Chicago: AAAM; 2008.
10 bfu. [ http://www.bfu.ch ] Bern: Swiss Council for Accident Prevention. [updated 2011 Jul 4; cited 2011 Jul 4]. Available from: http://www.bfu.ch/German/Statistikverwaltung%20PDFs/PDF2010/D_VSP_T_10.pdf
11 bfu. [ http://www.bfu.ch ] Bern: Swiss Council for Accident Prevention. [updated 2011 Jul 4; cited 2011 Jul 4]. Available from: http://www.bfu.ch/German/Statistikverwaltung%20PDFs/PDF2010/D_VSP_T_11.pdf
12 Russel K, Christie J, Hagel BE. The effects of helmets on the risk of head and neck injuries among skiers and snowboarders: a meta-analysis. CMAJ. 2010;182:333–40.
13 Cusimano MD, Kwok J. The effectiveness of helmet wear in skiers and snowboarders: a systematic review. Br J Sports Med. 2010;44(11):781–6.
14 Schmitt KU, Liechti B, Michel FI, Stämpfli R, Brühwiler PA. Are current back protectors suitable to prevent spinal injury in recreational snowboarders? Br J Sports Med. 2010;44(11):822–6.
15 Insidesurgery.com. Pennsylvania: Marcucci L, MD. [updated 2009 Mar 20; cited 2011 Jul 4]. Available from: http://www.insidesurgery.com/natasha-richardsons-death-a-helmet-might-have-saved-her/
16 Weber EU, Johnson EJ. Mindful judgment and decision making. Ann Rev Psychol. 2009;60:53–85.
17 Clarke VA, Lovegrove H, Williams A, Macpherson M. Unrealistic optimism and the health belief model. J Behav Med. 2000;23;367–76.
Funding / potential competing interests: No financial support and no other potential conflict of interest relevant to this article were reported.